
Abstract
Pediatric patients and their caregivers often experience perioperative anxiety. Interventions reduce caregiver anxiety improve cooperation and contribute to an improved patient experience. This study seeks to evaluate the efficacy of virtual reality (VR)-assisted mindfulness on perioperative caregiver anxiety. Participants were randomized into a standard of care (SOC) group, which included snacks but no technology-based distractions, or a VR group, which included snacks and a VR-guided meditation. Caregiver anxiety was measured before and after the intervention using the Visual Analogue Scale for Anxiety (VAS-A). Secondary aims explored participants’ baseline anxiety with the State-Trait Anxiety Inventory (STAI). VR group participants completed a satisfaction survey. Linear regression models of VAS-A and STAI were used to compare group differences. Satisfaction survey results were reported with descriptive statistics. 26 participants were included, with 12 randomized to the SOC group and 14 to the VR group. VAS-A scores in the VR group were lower than those in the SOC group (p = .002). The STAI found no change in participants’ state of anxiety in the SOC group (p = .7108), compared to a significant reduction (p = .014) in the VR group when controlling for anxiety traits. 12 of 14 caregivers in the VR group expressed satisfaction or strong satisfaction. This study supports the implementation of VR mindfulness as a method to reduce caregiver anxiety. VR use in the pediatric healthcare setting is safe and inexpensive, and the intervention had a high degree of participant satisfaction.
Keywords
Introduction
Caregivers of children experience high anxiety prior to and during anesthesia.1–3 In addition, up to 74% of caregivers experience preoperative anxiety in anticipation of pediatric surgery. 4 Despite this prevalence, interventions that mitigate caregiver anxiety have been implemented in a few hospitals. 5 Caregiver anxiety also influences their children's anxiety and pain perception.6,7 Increased caregiver anxiety is associated with increased distress in pediatric patients, uncooperative anesthetic inductions, prolonged recovery time, increased postoperative pain and delirium, and decreased patient satisfaction.8–10 Caregiver and pediatric anxiety are also mutually reinforcing—the more anxious a child is, the more likely the caregiver will become anxious. 11
Some strategies have been explored to alleviate preoperative caregiver anxiety, including preoperative education, play-based interventions, music therapy, the presence of caregivers at anesthetic induction, and integrative preoperative preparation programs. 11 Audiovisual (AV) distracting technologies for children may also mitigate caregiver anxiety. 12 Even though these treatments have variable results, most caregivers are not offered any anxiolytics.
Mindful meditation reduces anxiety.13,14 However, it would be costly and time-consuming to provide in-person guided relaxation to the volume of patient caregivers in the waiting room at any given time. Technological advances allow digital modalities and immersive technologies to serve as surrogates for in-person guided meditation.15,16 Virtual reality (VR) is another technology available to clinicians with proven success as an effective distraction tool.17–19 VR is an effective anxiolytic for children in pediatric clinical settings and is associated with increased patient cooperation during procedures.20–24 We chose VR over a screen-based solution, such as a tablet or computer, because it is affordable, portable, and allows full immersion, which increases effectiveness by reducing distraction. 25
Given its effectiveness for patient anxiolysis with few side effects, VR-guided meditation may also be an effective tool for treating caregiver anxiety. Improvements across the entire patient and caregiver perioperative experience are associated with improved postoperative outcomes, better treatment adherence patterns, and increased value in healthcare spending. 26 Patient and family experiences improve when providers individually invest and care for patients and their families. 26 Addressing caregiver anxiety aligns with family-centered care, which is an ethos that includes caregivers in the clinical treatment of their family members; 1 example of family-centered care is comforting caregivers when distressed. 26 Reducing caregiver anxiety enhances their capacity to comfort their child and promotes care integration.27,28
This study sought to improve caregiver anxiety in the pediatric perioperative setting by using VR-guided meditation to reduce caregiver anxiety after preoperative separation from their child. We hypothesized that the use of VR-guided meditation as a nonpharmacologic anxiolytic for pediatric patient caregivers would be associated with decreased anxiety. The primary objective was to evaluate the effectiveness of VR-guided meditation in reducing self-reported caregiver anxiety. The secondary objectives explored caregiver anxiety as a function of their personality traits and their satisfaction with the intervention.
Methods
Settings and Context
This study (Clinical Trial 03689868) was conducted from 2018 to 2021 in a 365-bed academic, pediatric hospital in northern California with approximately 1000 operations per month, including level 1 trauma patients. We included pediatric patients who underwent scheduled noninvasive or surgical procedures in the main operating rooms and radiology suites. We excluded caregivers with a history of severe motion sickness, current nausea, seizures, visual problems, or significant cognitive impairment, as per the safety guidelines of the VR headsets.
Intervention
After obtaining written caregiver consent, participants were randomized into either the standard of care (SOC) or VR groups. After both groups completed demographic and preintervention surveys, those in the VR group were escorted into a room where they used VR headsets (Oculus Go, Meta, Inc., Menlo Park, CA) to engage in MedMindfulness (Stanford Chariot Program, Palo Alto, CA), a guided 6 min meditation experience. Caregivers were fitted with the VR headsets via a ratchet-based strap that twisted to enlarge or reduce size, creating a comfortable fit. Participants chose the meditation application using a remote controller at the direction of research staff. Between participants, the headsets were cleaned by research staff using infection-prevention-approved cleaning products containing antimicrobial agents (Sani-Cloth, PDI Healthcare, Woodcliff Lake, NJ, USA).
The application provided AV cues for controlled breathing exercises. These consisted of relaxing scenery (such as waterfall landscapes and polar lights) paired with descriptive, meditative audio instructions. They were provided an option of snacks after their VR-guided meditation experience. Those in the SOC group were escorted back to the waiting area and provided snacks if desired, but no technology-based intervention.
Outcomes
The primary outcome was the anxiolytic effect of the VR-guided meditation on caregiver anxiety. The first secondary outcome was the association of caregiver personality traits with anxiety, along with any dependency of the intervention efficacy on these traits. Caregiver satisfaction was also explored as a secondary outcome.
Measures
To measure caregiver anxiety, we used the visual analog scale-anxiety (VAS-A) assessment, a previously validated measure for overall anxiety that provides a 0–100 score. 29 The VAS-A scale has also been validated specifically as a measure for anxiety in preanesthesia evaluation situations. 30 Initially, a pilot analysis of 20 caregivers was conducted to perform a power calculation for sample size. The average anxiety score was 70.55 ± 26.3 (on a scale of 0–100). An anxiety score of ≤40 is considered to be mild anxiety. 29 Thus, we powered this study to show a clinically relevant difference. Given a power of 80, an alpha of 0.05, and a mean decrease in anxiety from 70.5 to 40, we found that 24 patients (12 in each group) were required.
To measure caregiver personality traits and their effects on anxiolysis, we used a standardized method to evaluate anxiety among adults called the State-Trait Anxiety Inventory (STAI). This evaluation allows for a comparison between the caregiver’s state of anxiety and baseline anxiety trait.31,32 The STAI has been used specifically to measure caregiver anxiety.33–36 All participants completed both VAS-A and STAI before and after the intervention.
To measure caregiver satisfaction, participants in the VR group received a survey following their VR-guided meditation experience.
Analysis
We created linear regression models of VAS-A and STAI scores before and after the intervention for both study groups. Additionally, we controlled for STAI trait scores in the secondary outcome that analyzed anxiety states. Satisfaction survey results were reported as calculated descriptive statistics.
Results
In total, 26 caregivers were included (Table 1). The mean age of caregivers who completed the surveys was 44.0 years. Precisely, 53.8% of participants were randomized to the VR group. There was no attrition, and all participants were included in the final analysis of the primary outcome. There were 2 participants in the SOC group and 1 participant in the VR group who had incomplete data for the secondary outcome exploring STAI.
Patient Demographics.

Abbreviations: SOC, standard of care; VR, virtual reality.
Participants in the SOC group (n = 12) had a preintervention VAS-A mean of 50.3 (95% CI: 30.9, 69.7) and a postintervention mean of 51.4 (95% CI: 44.0, 58.9) (Figure 1). Participants in the VR group (n = 14) had a preintervention VAS-A group mean of 56.5 (95% CI: 45.7, 67.3) and a postintervention mean of 33.1 (95% CI: 26.4, 39.8). Results from the linear model demonstrated that the postintervention VAS-A scores in the VR group were different from those in the SOC group (p = .002).
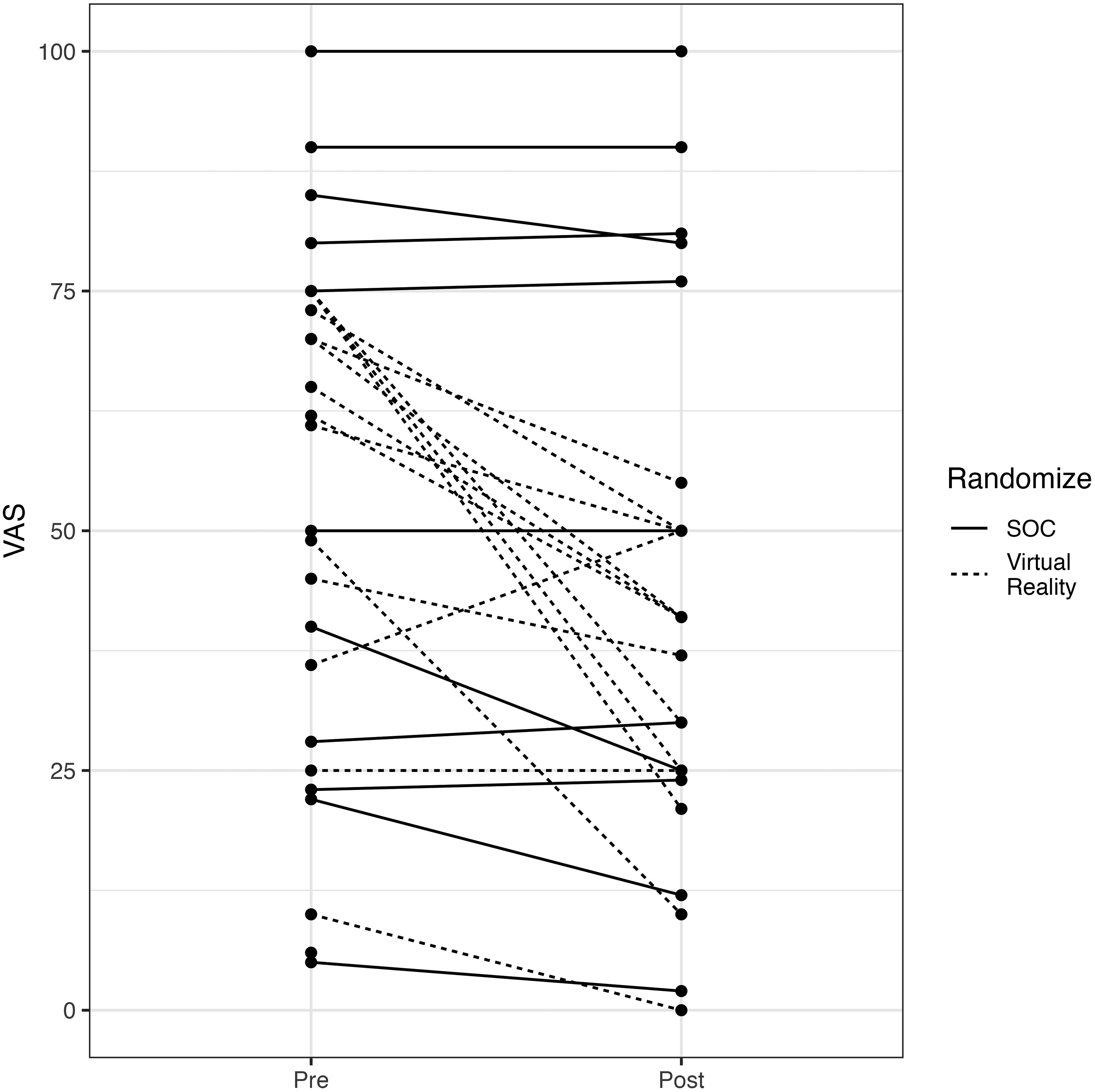
Preprocedure and postprocedure VAS scores, SOC versus VR.
When comparing the preintervention traits between the SOC (n = 10) and VR groups (n = 13), there were no significant differences in anxiety traits (p = .7070). The SOC group had an STAI trait mean of 41.40 (95% CI: 35.85, 46.95). The VR group had a trait mean of 42.77 (95% CI: 38.30, 47.24). Postintervention trait scores were also not significantly different between groups (p = .1590). The SOC group had a postintervention trait mean of 40.40 (95% CI: 35.09, 45.71). The VR group had a postintervention trait mean of 34.69 (95% CI: 29.36, 40.02). A linear regression controlling for preintervention traits was performed. Normality checks on the residuals were carried out and the assumptions were met. There was no change in participants’ state of anxiety after the intervention in the SOC group (p = .7108; Figure 2). In the VR group, there was a reduction in anxiety (p = .014; Figure 2). The mean preintervention state score in the VR group was 49.31 (95% CI: 44.48, 54.14), which decreased to a postintervention mean score of 35.92 (95% CI: 31.44, 40.41). For the SOC group, the mean preintervention state mean of 44.30 (95% CI: 37.66, 50.94), which decreased to only 42.50 (95% CI: 35.89, 49.11).
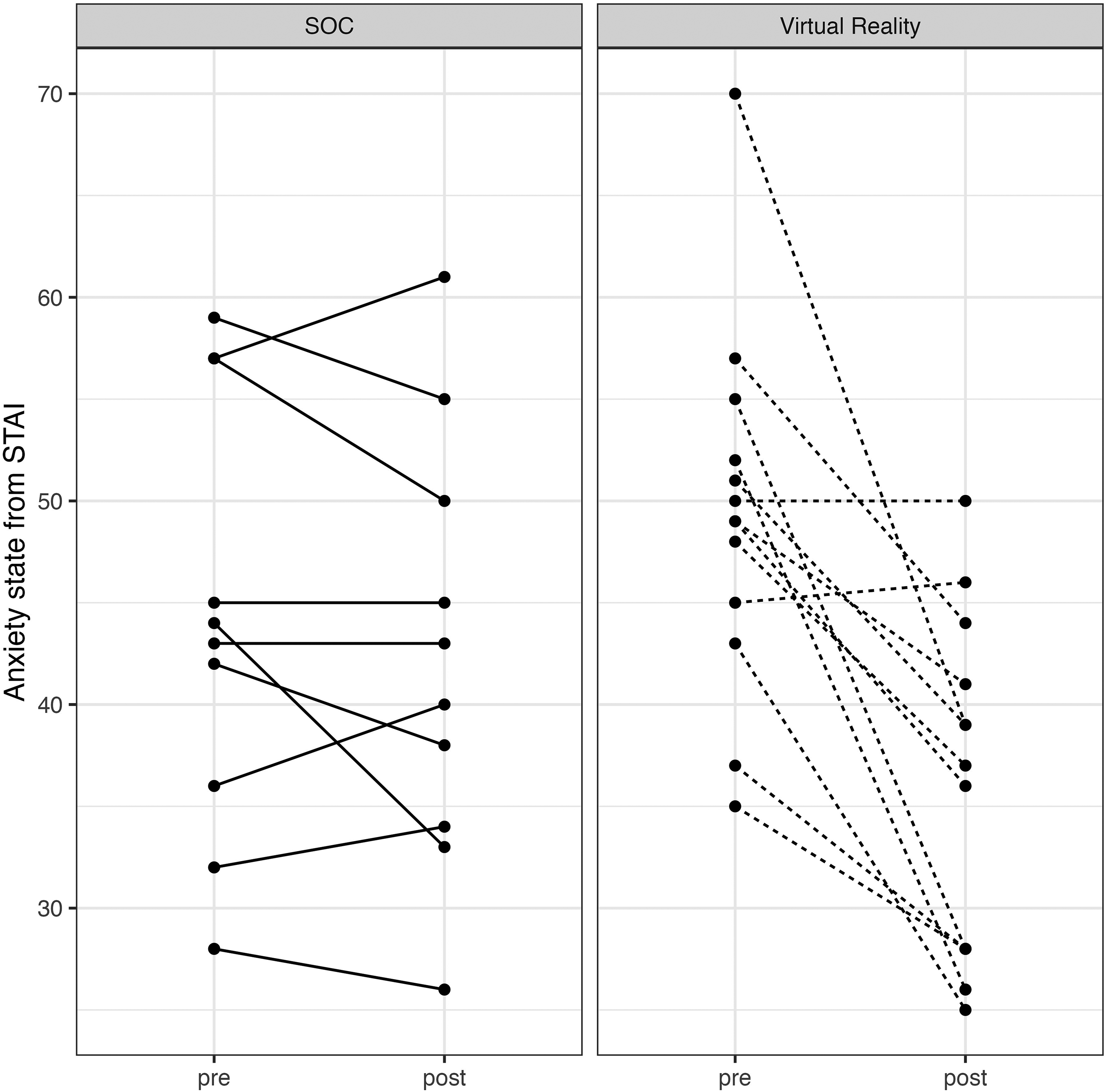
Comparison of change in anxiety between SOC and VR groups.
Satisfaction was high in the VR group (Figure 3). Overall, 12 of 14 caregivers expressed satisfaction or strong satisfaction (4 or 5 on a 5-point scale) across all satisfaction metrics.

Results of caregiver satisfaction survey.
Discussion
To increase generalizability and present an intervention that is feasible, we chose a VR-facilitated meditation compared to SOC. Given the lowering cost of VR headsets and the widely available meditative VR software, a VR-guided meditative treatment is both feasible and effective compared to the typical SOC that patients receive. Caregiver anxiety in the VR group decreased compared to those in the SOC group. In the STAI analysis, we confirmed that despite a heterogeneous group of participants with various baseline anxiety traits, the caregivers in the VR group had decreased states of anxiety compared to SOC. Furthermore, caregivers in the VR group expressed high levels of satisfaction with the intervention. This is indicative of the VR-guided meditation intervention's significant effect on reducing caregiver anxiety relative to the existing SOC. This trend holds even when results are adjusted for participants’ baseline anxiety levels. High user satisfaction ratings also suggest good acceptability and usability for patients.
AV stimulation has improved anxiety scores in both caregiver and pediatric populations. 12 VR is a more advanced technological extension of these prior AV interventions, and the novelty and immersion of VR-guided meditation likely contribute to improved effectiveness. 12 One study directed toward evaluating caregiver anxiety showed a significant reduction in anxiety in caregivers who viewed an educational video about anesthesia in comparison to the group who viewed a video about penguins. 37 An additional study showed similar reductions in caregiver anxiety for those who viewed an educational video on perioperative procedures, as opposed to the SOC group who read an educational booklet instead. 38 However, specific videos for individual sites are costly and lose relevance with procedural modifications over time. Given the effectiveness of the anxiety-relieving VR-guided meditation application in this study, VR-guided meditation may be a reasonable alternative to educational content for caregiver anxiolysis.
The STAI scale is widely used in anxiety studies, and AV interventions are associated with improved anxiety scores. 12 VR was previously investigated as a potential benefit to caregivers for perioperative education when utilizing a VR hospital tour that depicted their child's experience. 11 Our study utilizing a VR-guided meditation application is a cost-effective, novel approach to addressing preoperative anxiety in caregivers compared to traditional SOC. Satisfaction with the intervention was very high, indicating that VR's acceptability is growing. It may further indicate that VR-guided meditation experiences are a sought-after novelty for some patients.
The amount of commercially available VR applications, coupled with the reduced costs of VR headsets, should encourage hospitals to explore VR when seeking to improve the patient experience. Unlike other technologies, VR headsets allow for complete immersion in the visual field. 25 This prevents visual distractions from waiting room commotion. Although not perfect, the visual immersion offered by VR is 1 step closer to improving the possibility of restorative relaxation. The participants in this study benefited quite significantly from this medium for meditation.
This study was motivated by recent attention to family-centered care in pediatric healthcare. 27 Caregiver emotional management is a core tenet of family-centered care. 28 VR-guided meditation is a comparatively cost-effective option for anxiolysis, especially as commercial equipment costs continue to decrease.39,40 Furthermore, VR applications, particularly those designed for mindfulness, are becoming more readily available.40,41 Unsurprisingly, the benefits borne by VR in the pediatric healthcare setting seem to also apply to caregiver anxiolysis. Solutions that singularly address both types of anxiety—caregiver and child—are less resource-intensive than disparate interventions. VR is a safe therapeutic adjunct, 20 with few reported side effects, further enhancing its anxiolytic benefits for both pediatric patients and their families.
Limitations
There were several limitations. This study may be limited in its generalizability, as it was conducted at a single academic institution. Another limitation is that even though we satisfied power calculations, the overall sample size is small. Furthermore, it was difficult to control for all demographic factors. Unlike patients, the past medical histories of the caregivers were not solicited, which may have biased the results in an unpredictable direction despite the randomization. However, the heterogeneous caregiver population whose family members underwent a range of pediatric surgical operations may also improve generalizability across different populations. Finally, there was no measurement of transitional anxiolytic effects on children, as the intervention and measurements began after separation. Future research may investigate caregiver anxiety upon immediate arrival to the hospital to determine differential effects on their children. Given the popularity of tablet-based applications, future studies may also compare anxiolytic effects between tablet- and VR-guided meditations.
Conclusion
VR-guided meditation was an effective, reliable, and safe tool for preoperative caregiver anxiolysis in the context of pediatric surgical procedures. This study demonstrates that VR-guided meditation should be considered for those seeking to reduce caregiver anxiety. Additional studies will investigate the type of VR application (eg, active vs passive media) that provides optimal anxiolysis to provide the most reliable experience to caregivers. Future studies will also examine the corresponding reduction in patient anxiety as a consequence of reducing parental anxiety. They will also examine patient factors that confound and modify the observed effects on caregivers, including the effectiveness of VR-guided meditation anxiolysis for caregivers with limited English proficiency.
Footnotes
Authors Note
This study was approved by the Stanford University Institutional Review Board. All procedures in this study were conducted in accordance with the Stanford University Institutional Review Board's approved protocols. Written informed consent was obtained from the participants for their anonymized information to be published in this article.
Declaration of Competing Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The Stanford Chariot Program has received philanthropic donations from Meta, Inc. and Magic Leap, Inc. SR and TC are on the board of a nonprofit organization, Invincikids, and receive no financial payments for their positions. SR received consultative fees from Apple, Inc.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.