
Abstract
Proximal humerus fractures in pediatric patients are uncommon. This is a case report of a 17-year-old patient with Duchenne muscular dystrophy who sustained an occult proximal humerus fracture. The patient was on chronic steroids and had a history of vertebral and long bone fractures. He was using a wheeled mobility device on public transportation at the time of injury. He had a negative radiograph, but an MRI revealed a right proximal humerus fracture. He had decreased mobilization in the affected extremity, which limited activities of daily living including driving his power wheelchair. After six weeks of conservative management, he returned to his baseline level of activity. It is important to recognize that chronic steroid use adversely affects bone health, and fractures may be missed on initial imaging. To ensure adequate safety, providers, patients, and their families should be educated on the Americans with Disabilities Act guidelines for using wheeled mobility devices on public transportation.
Introduction
Duchenne muscular dystrophy (DMD) is an X-linked recessive disorder caused by a mutation in the dystrophin gene, which affects one in 3500– 5000 males globally [1, 2, 4, 5]. DMD is characterized by progressive muscular weakness, cardiomyopathy, restricted lung disease, skeletal deformities, and cognitive deficits [5]. Chronic steroids are used to preserve function of the musculoskelatal, cardiac, and pulmonary systems, although they do increase the risk for osteoporsis [1–5]. Patients with DMD are at an increased risk of fracture due to chronic steroid use, progressive muscle weakness, and loss of weight bearing activity [1–5]. Fractures in these patients can be missed on x-rays due to bony demineralization and decreased cortical thickness. Therefore, recognizing physical signs and symptoms related to fracture are important when caring for patients with neuromuscular disease as more workup may be required.
Case presentation
The patient was a 17-year-old boy with a history of DMD who was on chronic steroids, had been diagnosed with osteoporosis and was non-ambulatory, who presented to the rehabilitation clinic with a history of right shoulder pain. The patient was on daily deflazacort, which was started at age five, as well as weekly eteplirsen. Six days prior to presentation, he was involved in an incident while riding on an accessible bus to school. He reported that the bus came to an abrupt stop, and his power wheelchair slid forward while his right arm was stationary. His power wheelchair was tied down only in the front with no securement for the back of the wheelchair. The patient reported hearing a popping noise during this event and had sudden onset of right shoulder pain without numbness, tingling, or radiating pain. He presented to the emergency department the same day, where x-rays of his right upper extremity showed sclerosis of the right proximal humeral physis and diffuse osseous demineralization without acute fracture or dislocation in the shoulder or elbow (Fig. 1).
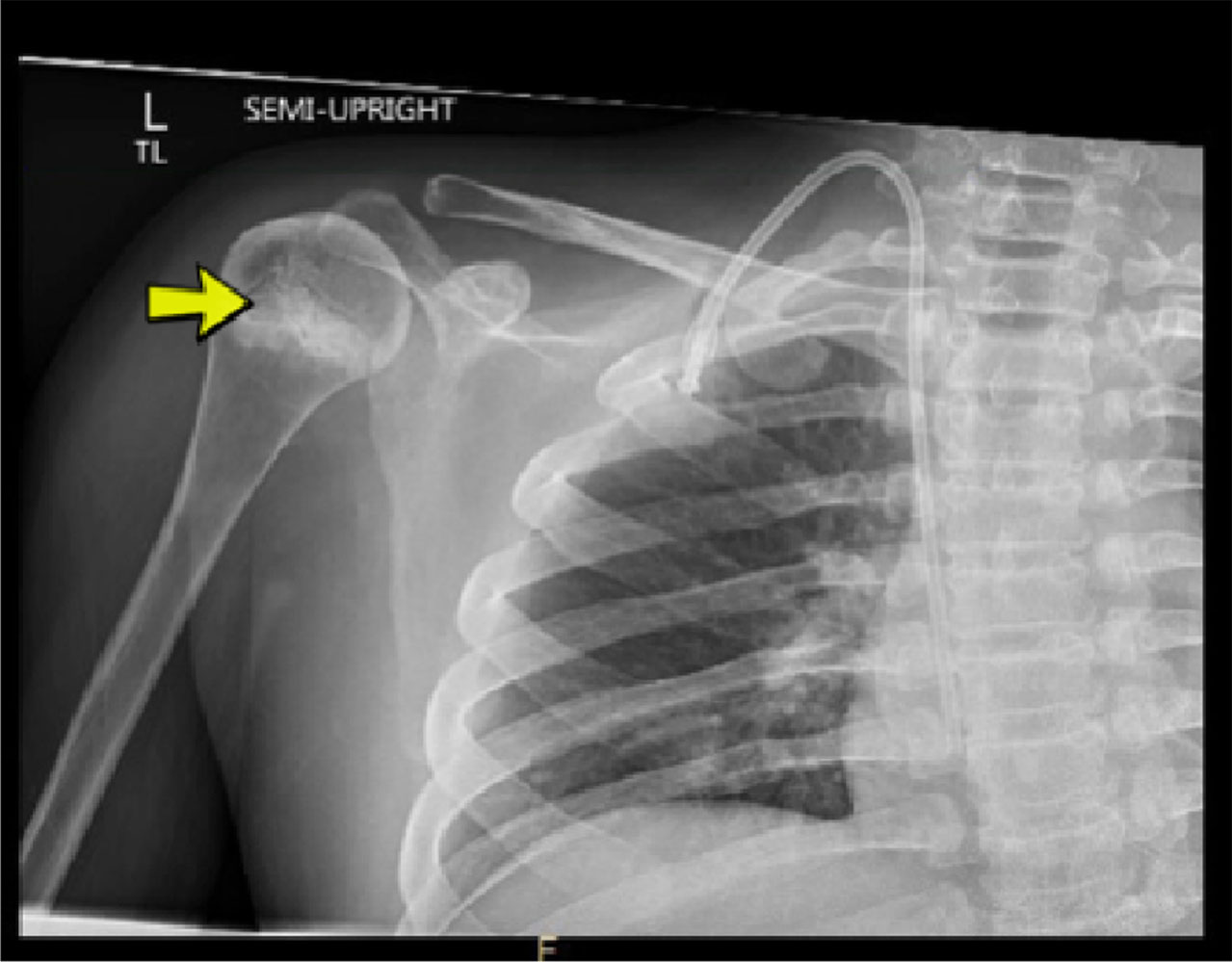
Anteroposterior (AP) view of right shoulder showing diffuse osseous demineralization and sclerosis of the proximal humeral physis (yellow arrow).
During clinic evaluation, the patient reported pain with any active movement of his right arm. He had to use his left arm to prop up his right to use his power wheelchair, as his joystick was located on the right. He also endorsed needing more assistance for activities of daily living. His right upper extremity exam was notable for tenderness on the anterior aspect of the glenohumeral joint and proximal humerus laterally. There was no tenderness along the clavicle, acromioclavicular (AC) joint, or scapular spine. Passive range of motion was restricted to 90 degrees of abduction and 20 degrees of external rotation due to pain. Special tests including Neer’s and Hawkins’s were positive on the right. His strength was at baseline in the left upper extremity, while the right side had decreased strength from his baseline of 2/5 for shoulder abduction, elbow extension, and elbow flexion to 1/5 throughout. Review of past medical history included two femur fractures and multiple vertebral compression fractures, with infusions of bisphosphonate therapy under direction of endocrinology starting 10 years prior to this incident.
Due to his ongoing pain, history of osteoporosis, and physical exam findings, a right shoulder MRI was pursued. The MRI revealed a fracture in the metaphysis of the proximal humerus. The fracture was noted to have mild bony compression with extension to the physis widening of the posterior physis, consistent with a Salter-Harris type II fracture (Fig. 2). Orthopedics was consulted and recommended non-operative management including wearing a sling for at least three weeks for pain control as well as to immobilize the arm to allow for optimal healing. After six weeks in the sling, the patient was nearly pain-free, reporting pain only when caregivers transferred him, which required them to lift from the axillary region. He was back to his baseline level of function and driving his power wheelchair independently; thus, no increase in physical therapy was pursued.
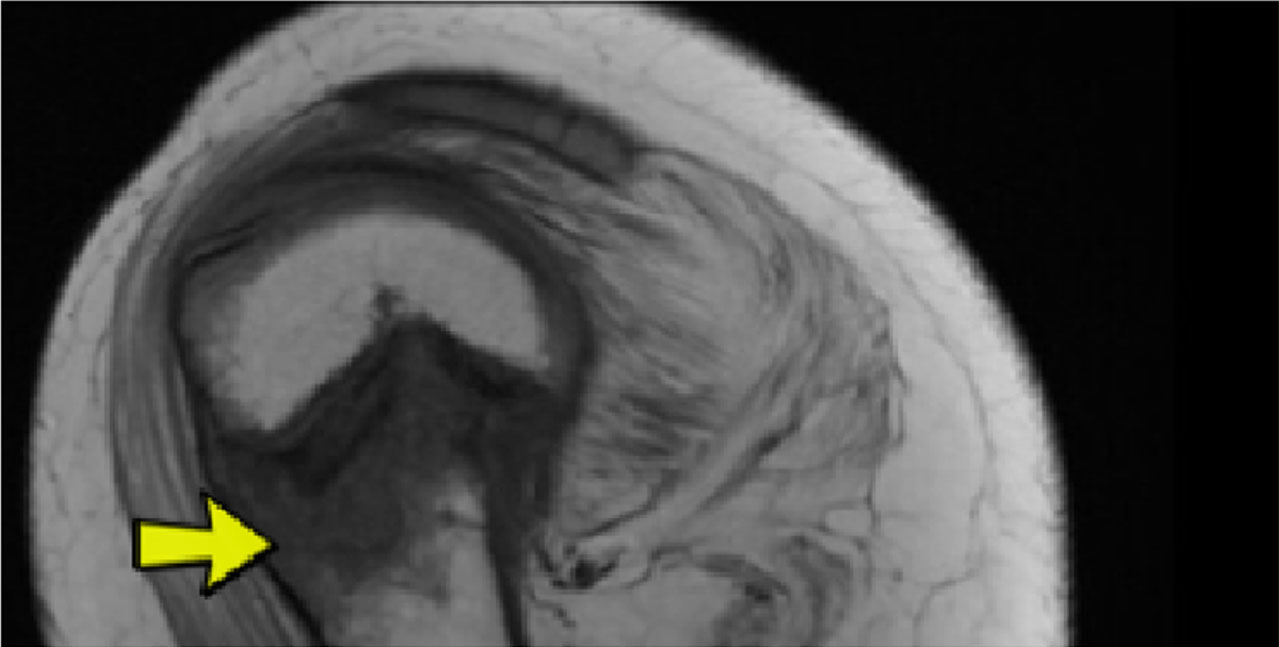
Sagittal T1 view of the right shoulder demonstrating a non-displaced transverse metaphyseal fracture (yellow arrow) extending to the physis (Salter-Harris II).
This is the first reported case of upper extremity fracture in a patient with DMD not related to a fall. Given broad shoulder and humerus pain, the differential diagnosis in this case included fracture, rotator cuff injury, labral pathology, brachial plexus injury, biceps tendinopathy, and AC joint injuries. Although he had an initial x-ray that was negative for fracture, the severity of his functional decline, history of osteoporosis, and physical exam prompted further evaluation. It can be difficult to identify fractures on radiographs when there is underlying demineralization. There are radiographic findings that can be easily overlooked if the reader has less experience with evaluating for subtle impaction lines, trabecular angulations, or sclerotic bands seen in fractures [9]. Fractures represent approximately 80% of missed diagnoses in the emergency department, among all comers [9]. When accessible, MRI is the preferred imaging study to evaluate for occult fracture while also assessing for injury to major soft tissue structures [9]. It has a similar specificity to CT imaging, although it is more sensitive [9]. MRI lends the advantage of identifying other potential soft tissue injuries in the shoulder including labral tear and rotator cuff injury.
Pediatric proximal humerus fractures are not common (up to 2% of all pediatric fractures), but fortunately, the complication rate after fracture management in this location is rare [8]. The most common causes of this injury in children and adolescents are from direct posterior shoulder trauma or fall onto an outstretched hand with arm abducted and externally rotated. Sports related injuries (such as in hockey, football, and horseback riding) are also reported, as well as overuse injuries such as Little League Shoulder. In the reported case, the patient’s lower body was moving forward while the seat belt held his upper body in a stationary position, exerting anterior force on the shoulder. The proximal humeral physis is responsible for most of the longitudinal growth of the humerus, which means there is great remodeling potential [8]. Most of these fractures are managed conservatively, with a sling or hanging arm casts for 3– 4 weeks. This patient had limited use of his affected upper extremity due to his underlying diagnosis, and even so, fully immobilizing him in a sling and pausing his range of motion regimen helped relieve his pain and aid his healing process.
Currently, standard care for patients with DMD includes chronic steroid use; current options include prednisone and deflazacort. Steroids are proven to prolong time to loss of ambulation, decrease severity of scoliosis, and better preserve lung function [1, 2, 4, 5]. However, steroids have side effects including irritability and increased risk of cataracts, diabetes, weight gain, and osteoporosis. Corticosteroids can also adversely affect bone health by impairing osteoblast activity for bone formation and mineralization, as well as decreasing calcium absorption in the intestine [1]. Patients with DMD are at an increased risk of fracture due to chronic steroid use and progressive myopathy. It is known that 20– 60% of patients with DMD have low trauma extremity fractures (most typically in the distal femur, tibia, or fibula) and up to 30% develop symptomatic compression fractures [11].
This patient had a history of multiple fractures and a diagnosis of osteoporosis. The International Society for Clinical Densitometry’s official position on pediatric osteoporosis states that the diagnosis of osteoporosis should not be made on the basis of densitometric criteria alone. Rather, the finding of one or more vertebral fractures in the absence of local disease or high-energy trauma or the presence of both a clinically significant fracture history and bone mineral density Z-score of less than or equal to – 2.0 is indicative of osteoporosis [12]. The care guidelines for patients with DMD include baseline followed by regular assessment of spine x-rays to monitor for compression fractures in order to initiate treatment when indicated [11]. Though bone mineral density (BMD) alone does not determine diagnosis of osteoporosis, spine BMD by dual energy x-ray absorptiometry can be considered on an annual basis to help monitor bone health and, eventually, guide treatment options [11]. Further, care guidelines for patients with DMD suggest routine surveillance of vitamin D levels to ensure these are adequate [11].
Although there were multiple contributory factors that put this patient at increased fracture risk, another factor in this case was the mechanism of injury in the setting of improper wheelchair tie down. Per Americans with Disabilities Act (ADA) guidelines, wheeled mobility devices should have four straps to tie down the wheelchair in addition to a lap belt and shoulder strap [6, 7]. If a child requires a wheelchair for transportation, they must be secured facing forward [10]. DMD can affect cognition and social skills; therefore, it is important for caregivers and transit operators to be knowledgeable about how to properly secure mobility devices.
Physicians caring for patients with DMD on chronic steroid therapy should be aware of increased fracture risk in both the upper and lower extremities. Bone health should be addressed at all clinical visits for patients with DMD, and endocrinology involvement in the multidisciplinary team is important [3]. Patients should be counseled regarding steroid side effects, including increased risk of fracture and osteoporosis. Fracture should be ruled out with more advanced imaging if there is high clinical suspicion despite a negative x-ray. Physicians, patients, caregivers, and transit operators should all be aware of the ADA guidelines for proper wheelchair securement on public transit. Incorporation of transportation needs in the individualized education program for school should also be considered [10]. Adequate support must be ensured for patients, and it is necessary to provide essential education about school transportation safety guidelines for injury prevention.
Footnotes
Acknowledgments
None.
The topic of this manuscript was previously presented as a poster presentation at the Association of Academic Physiatrists Annual Meeting in 2021 by these authors.
Conflict of interest
None. All authors have agreed to the contents of this submission.
Ethical considerations
Consent was obtained from the patient and parent in this case.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.