
Abstract
PURPOSE:
Restoration of functional mobility including gait and balance are fundamental to prosthetic rehabilitation in children with rotationplasty. The literature to characterize and investigate the correlation between postural balance and gait following rotationplasty are scarce. This study examines the characteristics of balance and prosthetic gait in a subject with rotationplasty and checks whether any association exists between them.
METHODS:
A 14-year-old boy with rotationplasty following Ewing’s sarcoma was fitted with a custom made prosthesis. Center of pressure (COP) measures using the HUMAC® Balance & Tilt System (CSMi, Stoughton, MA), temporal-spatial gait parameters, and energy expenditure measured by a 10 meter walk test were recorded using the new and old prosthesis. A control subject was used for comparison.
RESULTS:
The stability score, path length, and average velocity of COP improved in a new prosthesis for both standing conditions. Gait parameters were improved and energy expenditure was marginally reduced with the new prosthesis. However, overall prosthetic gait was significantly different compared to the control subject.
CONCLUSION:
This subject-centric approach successfully improved balance, gait parameters, and energy expenditure by providing better alignment, fit, and comfort with a custom prosthesis.
Introduction
Rotationplasty is a resection and reconstruction surgery in which the 180 degrees rotated ankle acts as a knee joint to enable consistent functional results [1, 2]. With active knee control supplemented by customized prosthetic rehabilitation, this results in a coordinated gait pattern similar to an able-bodied gait and better than trans-tibial amputation [3, 4]. The altered mechanics and anatomy of the affected lower limb in rotationplasty necessitates state-of-art custom prosthetic design to assist in daily activities [2]. Traditional prosthetic devices hold the vertically oriented residual limb (foot) in a socket which connects to a standard prosthetic foot via a shank extension, and a thigh corset is used for suspension. The prosthetic hinge imitates a knee joint and is aligned in congruence with the ankle axis to accomplish functional ambulation and mobility [5]. Control of the prosthesis is enhanced by the load-carrying capacity of the residual limb (i.e., the foot). The common current approach uses a trial-and-error method to develop a prosthesis customized for each patient’s individual needs.
Earlier studies have used the Short-Form (SF)-36, Faces Pain Scale-Revised, Harris hip score, Oswestry back pain score, Prosthetic Evaluation Questionnaires, timed ‘Up & Go’ testing, gait analysis, and posturography as outcome measures for subjects with rotationplasty [6, 7]. However, these studies are scarce. One study on electromyography and gait analysis has demonstrated good functional restoration of gait following rotationplasty [8]. Moreover, studies on balance and postural assessment in rotationplasty using a prosthesis are lacking. Though few studies have used balance as one of the outcome measures, several have done qualitative assessments. It is important to study how balance and gait parameters are correlated with respect to prosthesis use in rotationplasty, as this has not been investigated so far. It is also necessary to understand the pattern of center of pressure (COP) displacement during a dynamic task while using a prosthesis. To the knowledge of the authors, a quantitative assessment of static and dynamic balance using reliable and valid instruments is not available in the literature. This report describes a case of rotationplasty following Ewing’s sarcoma treatment in which the patient was successfully rehabilitated with a prosthesis and assessed for balance and gait. The objective was to examine several characteristics of balance and prosthetic gait in a subject following rotationplasty and to determine whether any association exists between them. It was hypothesized that his balance and gait would improve with a better prosthetic fit and design.
Method
Case description
A 14-year-old boy with a history of rotationplasty reported to Swami Vivekanand National Institute of Rehabilitation Training and Research (SVNIRTAR) for rehabilitation, and prosthetic restoration in June 2020. His past medical history revealed that he initially presented with a chief complaint of pain, swelling, and tenderness of his left thigh with an accompanying fever during January 2016. He was advised to undergo a full-length femoral radiogram and MRI of his left lower limb. An x-ray showed a lytic lesion with a classic sunburst and moth-eaten appearance as well as a pathologic fracture of the proximal femur shaft (Fig. 1a). MRI report revealed a bone tumor involving the proximal meta-diaphyseal region of the femur with a completely displaced pathologic fracture (Fig. 1b).
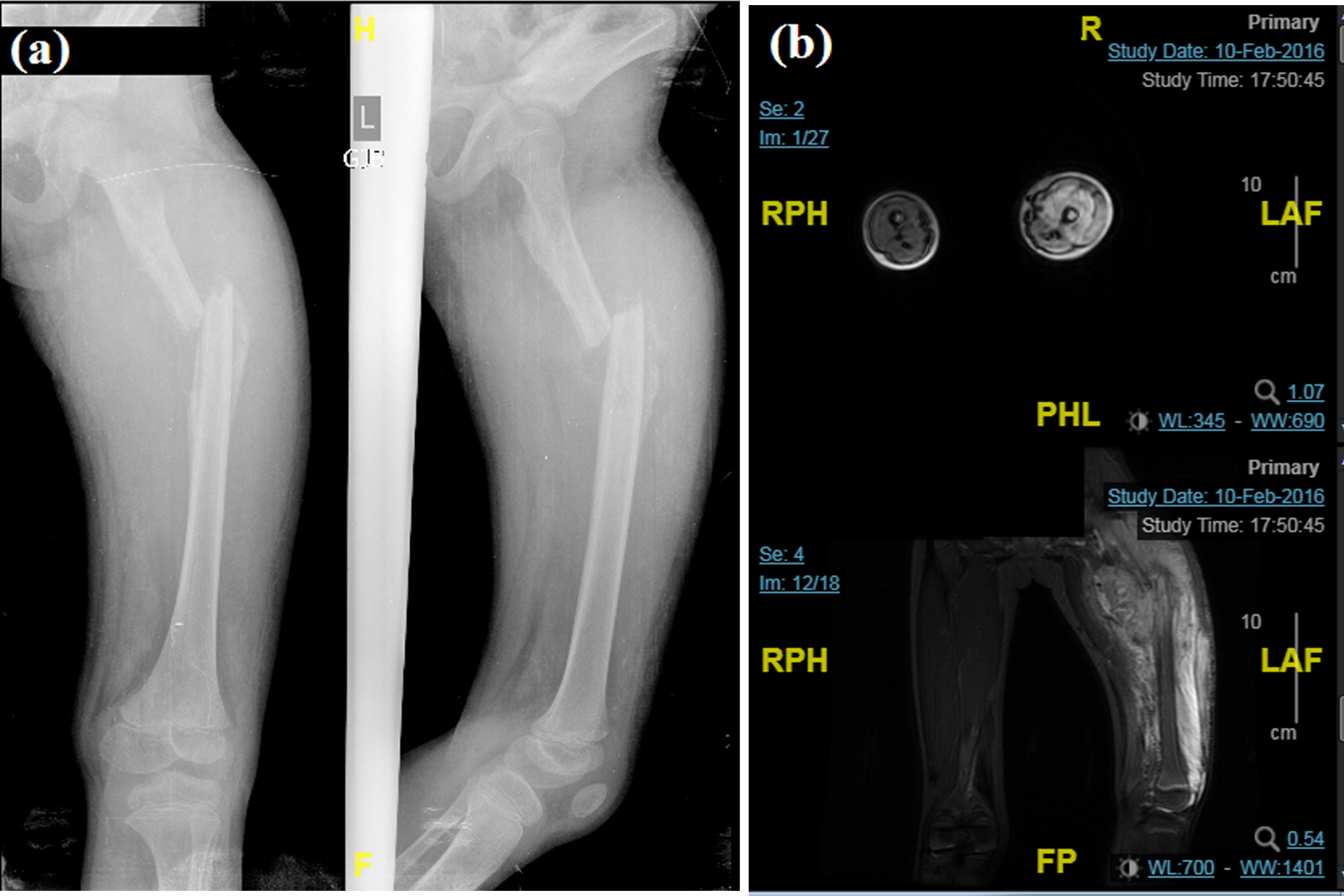
(a) plain x-ray (b) multi-planar MRI images showing complete pathologic fracture with displacement of the proximal diaphysis of left femur, altered marrow signal intensity, and soft tissue mass measuring 8×10×13 cm in its maximum AP, transverse, and CC dimensions.
A Thomas splint was applied inversely to provide effective immobilization for the proximal fragment. He was referred from his district hospital for fine needle aspiration cytology (FNAC), which showed smears of round cell sarcoma. Since a FNAC is a screening test, the subject was referred for an incisional biopsy to confirm either an embryonal rhabdomyosarcoma or Ewing’s sarcoma. The biopsy report confirmed the diagnosis of non-metastatic peripheral primitive neuro-ectodermal tumor (PNET). He was referred to the department of medical oncology in a cancer specialty hospital where he was advised to undergo chemotherapy as per the Intensive Ewing Family Tumor (EFT 2001) protocol from February to May 2016. A rotationplasty was performed in June 2016 without complications (Fig. 2a). The goal of the surgery was to provide him with a functional knee that he could later use for a prosthesis fitting similar to those used by transtibial amputees (Fig. 2b). Post-operative therapy was initiated, and included gait training with a walker. The therapeutic protocol was similar to that of a muscle transfer program which included regaining muscle contraction, flexion, extension, and range of motion of the new knee in addition to balance training and strengthening of several muscle groups, including in the upper limbs. At the end of four weeks, once the wound had healed well and full range of motion of the new knee had been established, prosthetic rehabilitation for ambulation was initiated. Initially, the subject and his family members were not interested in a prosthetic fitting and therefore his first prosthesis (Fig. 4a) was fitted in October 2018 at a regional rehabilitation center.
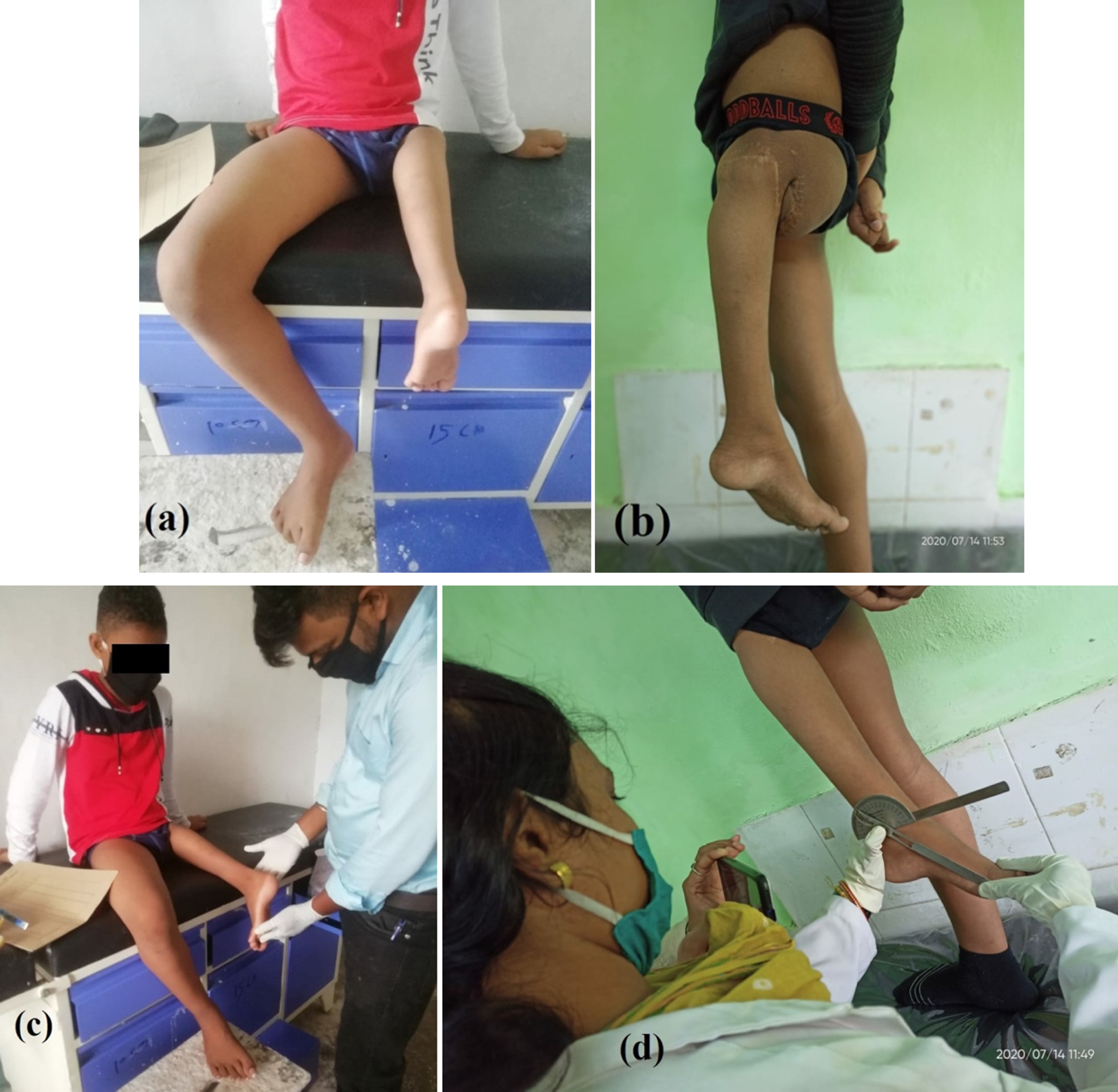
(a) front view (b) side view of rotationplasty (c) examination (d) assessment of functional range of motion.

(a) old prosthesis in anterior and lateral view (b) new prosthesis (c) subject standing with new prosthesis in anterior and lateral view.
The subject was referred to SVNIRTAR and presented with an ill-fitted prosthesis. This prosthesis had gross deformation and malalignment of the joints and bars, improper fit of the thigh shell, insufficient lateral wall support, and shortening of the overall height (Fig. 4a). He had stopped using this prosthesis six months prior to presentation. After careful inspection of the previous prosthesis and extensive assessment and evaluation of the subject’s clinical condition (Fig. 2c, d), a customized prosthesis was designed. A negative cast impression was taken to encase the entire foot in weight-bearing condition, extending up to the level of ischial tuberosity and maintaining a level pelvis. The fabrication, bench (3c, 3d), and static alignment (Fig. 3e, f) of the prosthesis were established according to standard protocols and the subject’s limb posture (Fig. 3a, b).

(a) checking height (b) establishing load line (c) bench alignment lateral view (d) bench alignment posterior view (e) static alignment lateral view (f) static alignment posterior view.
The custom-made ortho-prosthesis was referred to as an extension prosthesis that utilized a thermoplastic quadrilateral thigh shell, orthotic free knee joints and bars, laminated socket incorporated in an exoskeletal shank extension, and a ranger foot with a pair of shoes (Fig. 4b). The orthotic knee center was kept in congruence to the ankle center (new knee) to reduce shear and avoid relative moments between orthotic and anatomic knee and soft tissues around it (Fig. 4c).
The HUMAC® Balance & Tilt System (CSMi, Stoughton, MA) was used to measure balance parameters (Fig. 5). Observational gait analysis using video recording was performed to detect any gait deviations. Gait parameters were measured using a 10 meter walk test and energy expenditure using the physiological cost index (PCI) were recorded (Fig. 6a, 6b, 6c). All tests were performed with prior written informed consent form the subject.
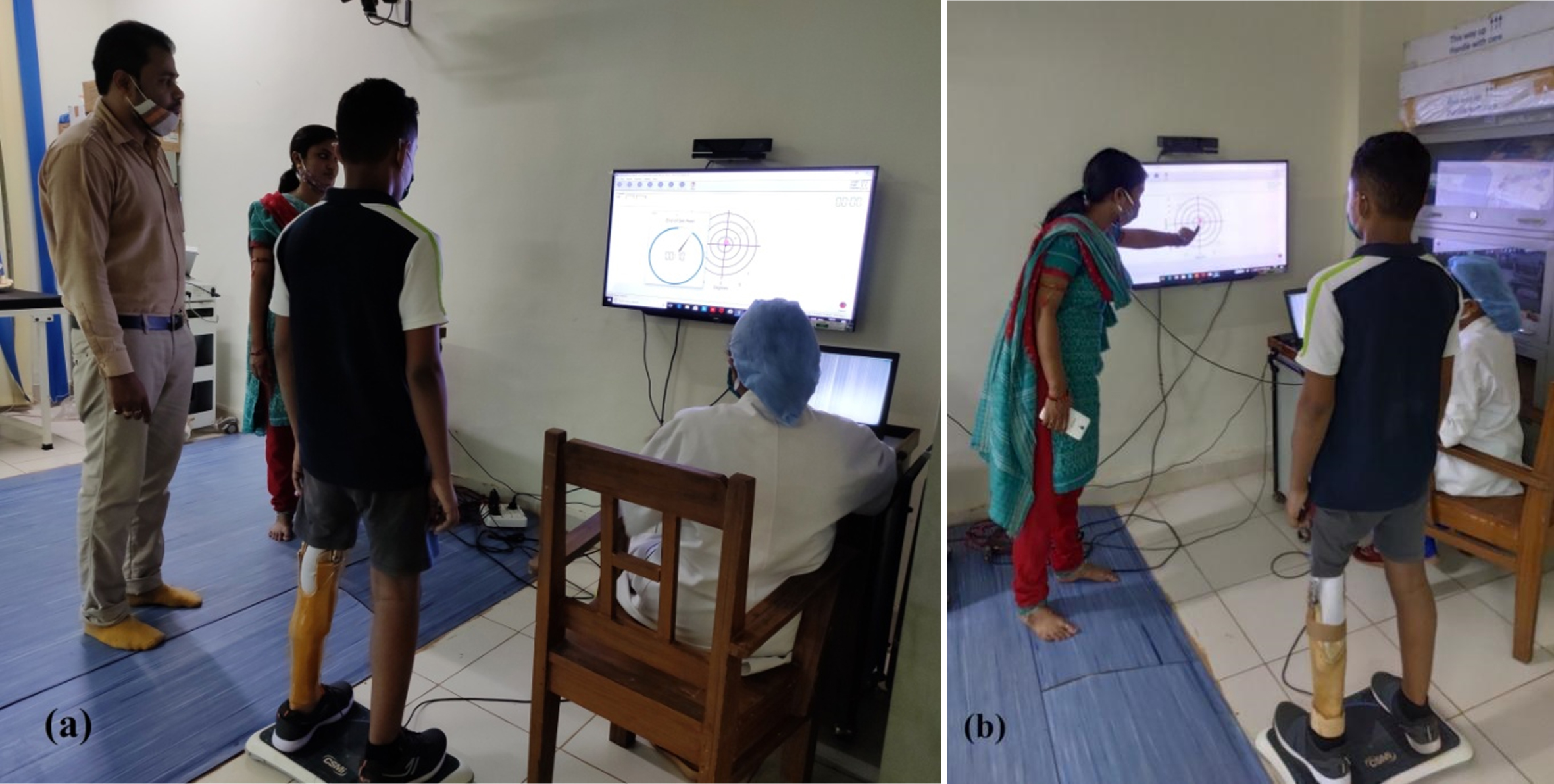
(a) subject standing on HUMAC balance machine (b) instructions provided to the subject for data recording.
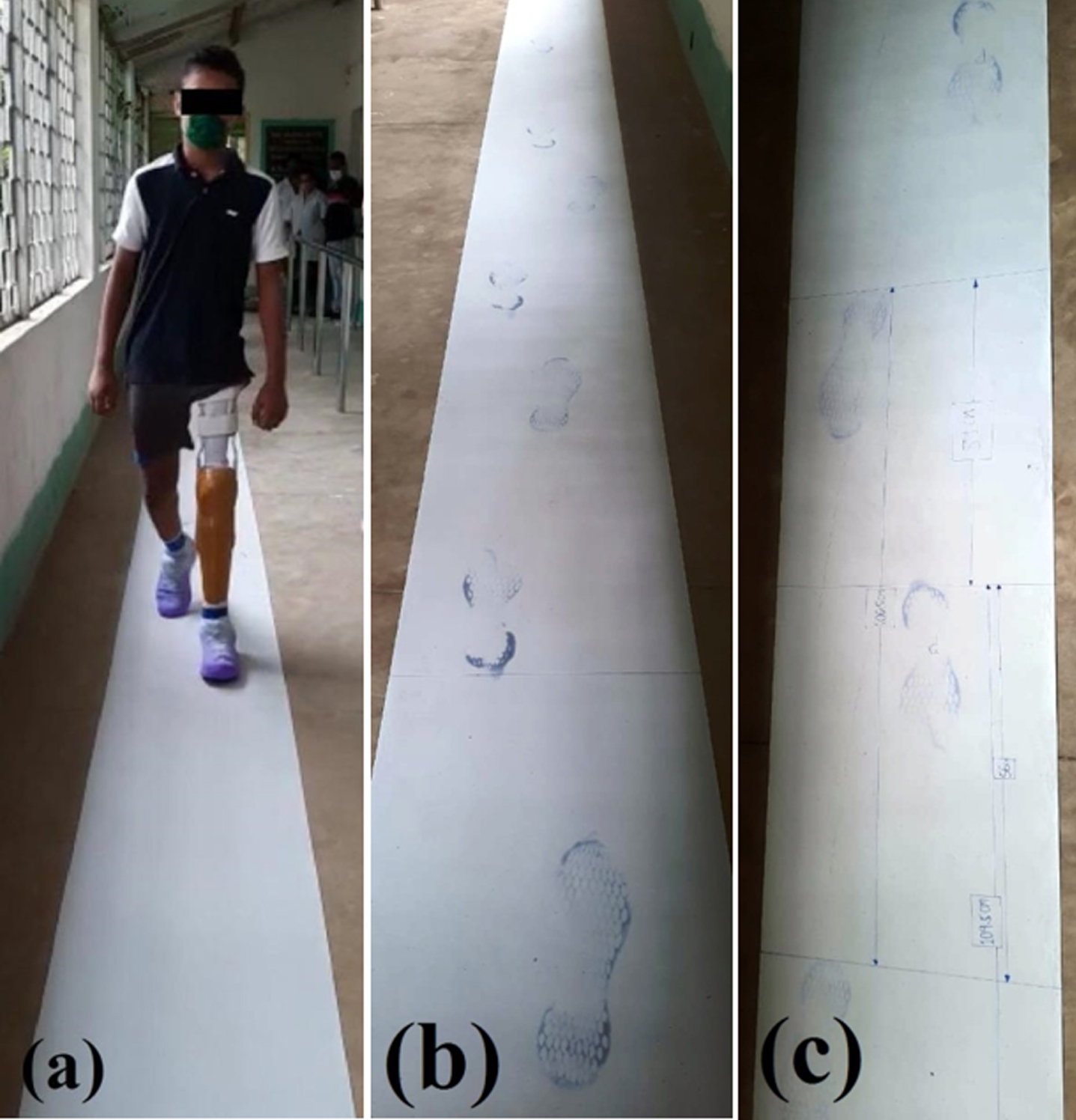
(a) 10 meter walk test (b) foot prints of walk (c) measurement of gait parameters.
Data was recorded after 3 months of using new prosthesis to allow for an acclimation period. It was hoped that this would also reduce the habitual effects of the old prosthesis and reduce bias for the clinical trial. Balance parameters were assessed for the unilateral prosthetic in the standing and bilateral weight-bearing conditions with shoes on and eyes open. The testing order was randomized for prosthetic (old and new) and test condition (static, dynamic, single prosthetic limb, and double limb). The subject was instructed (Fig. 5b) to use the prosthesis while wearing shoes and the balance test was performed in three sessions using the HUMAC® Balance & Tilt System (CSMi, Stoughton, MA). The sessions were conducted consecutively on the same day. The average of the three sessions was considered for analysis.
The set level is defined as the distance (degrees) to the center of the farthest target, with higher levels indicating greater perturbation. The hold time is the time in seconds the patient should remain on the target. For static stability, the subject needs to maintain his COP on the centrally placed target. Static balance parameters were assessed with a hold time of 60 seconds. Dynamic stability was tested by assessing a patient’s ability to hold his COP on moving target that circled around their neutral balance point. Perturbation was graded in levels, with level III indicating a moderate level of perturbation. Level III perturbation and a time period of 30 seconds were maintained for all dynamic balance parameters during single leg stance according to the standard protocol of the HUMAC® instrument. To assess dynamic balance, the subject was asked to reach each of eight targets located 45 degrees away from the center, covering a total of 360 degrees. At each target point, the subject was instructed to maintain his balance with a hold time of 30 seconds. A unilateral standing test was performed with gentle upper limb support as the subject was feeling less stable during the test. At least 5 minutes of rest were allowed between each trial set to avoid fatigue. The static and dynamic stability were recorded from a mean of three trials. The static stability variables were path length (cm) and average velocity (cm/sec) of COP. The stability score (%) is a dynamic stability variable and is the ratio of the percent of time the subject was on a target to the time he was active (Fig. 5a).
Temporal-spatial gait parameters were measured on a 10 meter paper walkway test. PCI is a simple index used to estimate energy expenditure during walking. It is based on a ratio between heart rate and self-selected walking speed (PCI = working heart rate –resting heart rate / walking speed). The subject was instructed to walk at a self-selected walking velocity. The gait parameters were also compared with respect to a control subject with a similar body mass index. The mean of three walking trials were used to derive step length, stride length, cadence, velocity, and PCI. A comparison of balance and gait parameters and energy expenditure was made between data using the new and old prostheses.
Results
The results of balance and temporal-spatial gait parameters are presented in Tables 1 2 respectively. The subject demonstrated an improved stability score, reduced path length, and reduced average velocity of COP using new prosthesis for both unilateral prosthetic stance and bipedal standing during balance test evaluation.
Comparison of balance parameters
Comparison of balance parameters
Results of temporal-spatial gait parameters and energy expenditure
There was minimal excursion of COP path, indicating improved balance and maintenance of posture while standing on the new prosthesis. The same trend was observed for both bipedal and unilateral prosthetic stance (Fig. 7).
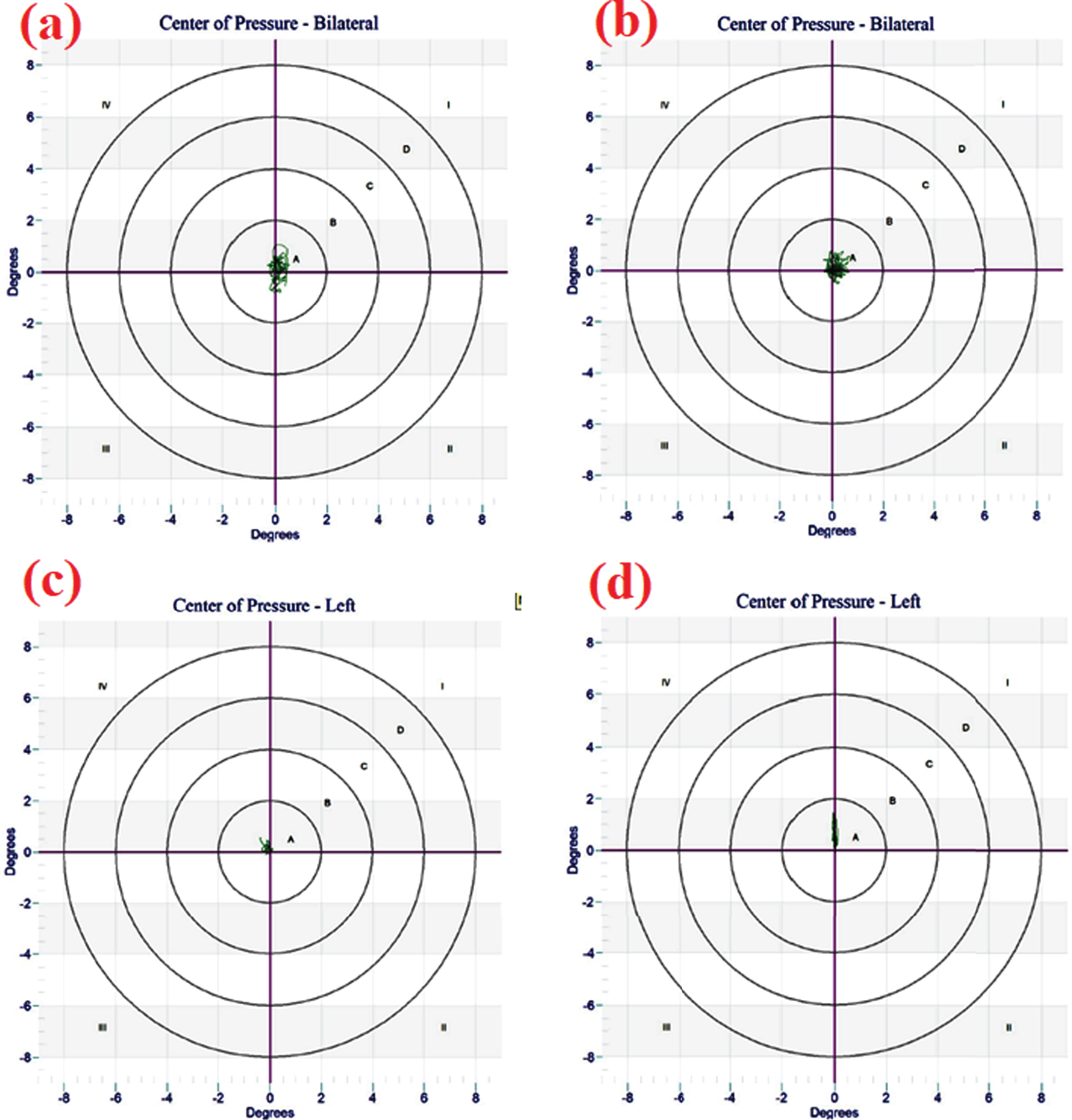
COP trajectory (a) bilateral standing with old prosthesis (b) bilateral standing with new prosthesis (c) standing on old prosthesis unilaterally (d) standing on new prosthesis unilaterally.
Observational gait analysis showed decreased knee flexion during swing for both prosthetic limbs. Moreover, the subject walked with increased lateral trunk bending, lateral whips at the heel, and more lumbar lordosis while using the old prosthesis. These parameters were improved with use of the new prosthetic limb. Objective evaluation using the 10 meter walk test revealed improved temporal-spatial gait parameters with the new prosthesis. However, compared to the control subject, this patient demonstrated a significant worsening of all parameters, especially walking velocity and cadence. The prosthetic gait was more energy-consuming compared to the control, but there was marginal difference in PCI observed between the old and new prostheses.
This case study was aimed to analyze prosthetic balance and gait in a subject with a history of rotationplasty due to Ewing’s sarcoma. Comparison was made between two prostheses used by the same subject regarding balance and gait. Additionally, temporal-spatial parameters of gait were compared with a control subject with similar body mass index.
Balance and stability
Static stability is defined as the ability to minimize movement of the center of gravity within a base of support under a given condition. COP has been used to characterize static stability [11]. However, earlier studies commonly assessed balance performance via qualitative measures like the Berg Balance Scale (BBS), Activities-Specific Balance Confidence (ABC) Scale, Star Excursion Balance Test (SEBT), and Balance Error Scoring System (BESS) for various populations, including rotationplasty. To the authors’ knowledge, assessment of balance parameters using reliable and valid instrumentation in subjects with a prosthesis post-rotationplasty is previously unstudied.
In this study, stability score improved in both unilateral prosthetic loading and bipedal standing conditions while using a new prosthesis. The subject scored 77% and 90% for unilateral prosthetic loading with the old and new prostheses respectively. Similarly, he scored 89% and 92% for bipedal standing.
Path length and sway area are different measures of COP displacement. Path length is the distance of COP displacement and is independent of direction. It is based on the principle that the human control system is independent of the direction of the COP trajectory and is used as a basic parameter to analyze balance [12]. In this study, the measured path length was significantly reduced while using a new prosthesis in both standing conditions. The score improved from 43.33 cm to 20.19 cm with a new prosthesis for unilateral prosthetic loading. Similarly, an improved score of 39.6 cm compared to 64.67 cm was observed during bilateral standing. This result indicates that the subject was more balanced while using the new prosthesis with less body sway and reduced path length of COP. The COP trajectory (Fig. 7) shows a larger sway area in bipedal standing with the old prosthesis, which was reduced when using the new one. Instead of being independent in direction, the subject demonstrated larger antero-posterior sway compared to the medio-lateral direction (Fig. 7a, b). Normally, the root mean square value for anterior-posterior sway is larger than for medio-lateral components during standing. However, it may be that the use of a prosthesis encourages a wider standing support to enhance stability and thereby reduces the postural sway in medio-lateral direction. A similar trend was noticed for prosthetic unilateral standing. The new prosthesis demonstrated increased medio-lateral stability with reduced sway. However, minimal centered postural sway in antero-posterior direction was observed. This may be explained by a postural modification adopted by the subject of anterior stooping to normalize the COP position. This was possibly due to the alignment and socket fit of the new prosthesis.
It is well understood that COP speed is an indicator of the extent of sway during a task and it has been suggested as the most sensitive COP variable for detecting the extent of sway [13]. The average velocity of COP was reduced from 2.87 to 1.35 cm/s when using the new prosthesis for unilateral prosthetic standing, and decreased from 2.16 to 1.32 cm/s during bipedal weight bearing. This reduced postural sway with the new prosthesis indicates adequate prosthetic height and alignment, as well as improved symmetrical weight bearing on both feet. Moreover, the subject had asymmetrical weight-bearing and a reduced ability to accept weight through the prosthetic side which is consistent with the findings of Ackman et al. [6].
Temporal–spatial parameters and energy expenditure
The temporal–spatial parameters of step length, stride length, velocity, and cadence showed marginal improvement while using the new prosthesis compared to the old one. The prosthetic step length and stride length were increased in new prosthesis. However, compared to the normal limb, the prosthetic limb achieved greater step and stride length. This may be due to his ability to bear weight on the intact limb and progress his prosthetic limb with more stability and comfort. Similarly, cadence and walking velocity were both improved in the new prosthesis compared to the old one. This may be attributed to the fact that the subject was well accustomed to both prostheses and there is not a significant difference in design or components used. However, there was a marked alteration observed in the alignment of the old prosthesis at the time of reporting due to its prolonged use.
In addition, there was a marked difference in all gait parameters compared to the control subject. It was observed that the subject walked with reduced step length, stride length, velocity, and cadence compared to the control (Table 2). These findings are consistent with a propulsive phase occurring on the prosthetic side and an acceptance phase taking place on the sound side. Similar results have been observed by previous investigators. Ackman et al. [6] examined differences in gait characteristics of 12 subjects with rotationplasty due to congenital proximal focal femoral deficiency (PFFD) and compared them to a control group. They observed that the PFFD group had a significantly reduced walking speed (p = 0.0049) and cadence (p = 0.0024) compared with the control group. In another study, Catani et al. [9] analyzed the gait of children after Van Nes rotationplasty using a force plate and motion analysis. They observed significant differences in stride length, cadence, and velocity (1.29 vs. 0.90 m/s) compared to the normal children. The subject in this study walked with a self-selected velocity of 46.1 m/min with his new prosthesis compared to 65 m/min for the able-bodied individual. Therefore, he walked at 70.9% of the speed adopted by the control subject.
The energy parameter PCI showed only a marginal difference in favor of the new prosthesis. PCI was measured as 0.57 and 0.59 m/min for the new and old prostheses respectively. However, the subject walked with more energy consumption compared to the control (0.42 m/min). These results are in accordance with the work of Sakkers and Wijk [10] who observed higher energy expenditure in subjects with rotationplasty after limb deficiencies during walking and other activities. However, earlier studies have revealed that creating a new functional “knee joint” in rotationplasty results in a higher functional outcome level and less energy expenditure while ambulating versus an above-knee amputation [7].
A strong correlation was observed for the subject in terms of balance and gait parameters for all tested conditions, which is also supported by earlier published works of Eshraghi et al. [14]. The individual is leading a normal life with full independence in functional daily living activities using the new prosthesis. In addition, the prosthesis restores the cosmetic appearance which had been lost due to his rotationplasty. As reported by the subject, walking with the prosthesis is contributing to improved mobility and strength, especially of the ankle joint. However, careful inspection and follow up is required to compensate for his leg length discrepancy and any associated prosthetic adjustments or replacements until he reaches skeletal maturity. Though rotationplasty is a rare complex limb salvage surgery [15], a long term follow-up study involving large samples is warranted to improve the generalizability of these results.
Conclusion
A well-fitted customized prosthesis following proper rehabilitation protocol completely satisfies the surgical rationale of the rotationplasty procedure. A properly fitted socket design, resetting and optimizing alignment, incorporating adequate suspension, and maintenance of adequate prosthetic height in the new prosthesis resulted in improved balance and gait, as well as reduced compensatory movements. The results also indicate that balance and gait parameters are correlated with respect to the use of a prosthesis in rotationplasty. Though gait and energy parameters were significantly altered compared to the control, the subject achieved full independence in functional daily living activities with maximum restoration of cosmesis with prosthetic rehabilitation.
Footnotes
Acknowledgments
The authors would like to thank the subject and his parents for their sincere cooperation throughout this case study.
Conflict of interest
The authors declare that there is no conflict of interest.
Ethical considerations
Parental informed consent and informed assent from the child was obtained and approved by the authors’ Institutional Review Board.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.