
Abstract
Determining when a child returns to school after an acquired brain injury is difficult to assess. Many factors affect a successful hospital-to-school reintegration. The hospital school simulation allowed the Acute Pediatric Inpatient Rehabilitation Unit (IRU) interdisciplinary team to assess how the patient was functioning at specific stages of the patient healing process to target goals that explicitly helped the patient safely reintegrate into school. A patient with an acquired brain injury (ABI) participated in a hospital school simulation where a novel school simulation rubric (SSR) tool was used to evaluate completion of specific activities the patient would experience in a traditional classroom. Results were shared with the IRU team so accommodations and modifications could be made to the IRU school recommendations letter based on the results of the final SSR. Preliminary results were found to benefit the patient as they reintegrated back to school. This study highlights the need for ongoing communication between hospital providers and educational personnel to provide patients with academic supports for school reintegration.
List of Abbreviations
(ABI) (IRU) (SSR)
Introduction
Because acquired brain injury (ABI) is the leading cause of disability among children, a successful hospital-to-school reintegration is essential to the rehabilitative process [1]. Given ABI incidence among school-age populations, many educators are likely to encounter a child with a brain injury [1]. “Following ABI, children are required to transition back to school and adapt to the physical, cognitive, behavioral, social, and emotional demands of the school environment” [2]. Students must deal with the cognitive and developmental demands placed on their changing brains as they grow following an ABI [2]. During this time of change, students return to school with the expectation of completing the same educational load as they did prior to an ABI. As the brain continues to develop well into early adulthood, the age at the time of injury can impact the developing brain [3]. Having a poor transition back to school can only negatively impact these outcomes. It is essential to understand and identify which interventions are essential to develop educational supports. The school’s role is two-fold in helping students re-enter successfully, not only is their role to help students reintegrate into the school setting efficiently, but also determine which accommodations/modifications will help the student within the guidelines of the Individuals with Disabilities Education Act and Section 504 of the Rehabilitations Act. “When parents and school professionals know what behaviors and characteristics they will be faced with and how to accommodate students returning to school following an ABI, it lessens frustrations for all concerned” [4].
To increase interdisciplinary communication between the medical and educational personnel, a rubric designed to guide educational planning would be helpful to assist with school reintegration following an ABI. Rubrics are commonly used in the education field to evaluate students’ assignments and one that teachers are familiar using. A student’s ABI related needs and abilities should be considered during their educational planning, therefore, attention, mobility, processing information, problem solving, reception and expressive language were evaluated. See Table 1. These areas were specifically chosen due to the impact they have on the educational learning environment. Vanclooster [5] states the importance of increasing the medical teams’ knowledge of the educational field to improve interdisciplinary communication. The medical team uses specific language to communicate effectively and express the needs of the patients they serve. The same is true for the educational staff, who communicate using educational language to express the support needed to service students. Both groups have languages that parallel each other, however, neither language has a cross reference specifically for the benefits of school reintegration. The School Simulation Rubric (SSR) was designed to help each specialty communicate with each other in a common language.
Rubric evaluation tool with higher number indicating less accommodations required in school setting
Rubric evaluation tool with higher number indicating less accommodations required in school setting
Canto [6] stated that there were many barriers in helping students transition back to school following a brain injury. The main difficulties discovered in their research included the lack of communication regarding the injury shared with school personnel [6]. Additionally, there were lack of resources to assist students returning to school following brain injury [7]. Lack of perceived importance by the school personnel was another concern, because brain injuries may not be readily apparent [6, 7]. This highlights the importance of communication between the medical staff and school personnel prior to discharge and having a clear discharge plan and school reintegration plan in place [6, 7].
Rubric development
Each criterion of the SSR was created by this author with the input of physical, occupational, and speech language therapists. The SSR instrument was designed so when the school simulation was completed the hospital school coordinator would be able to share the results with the medical team in terms that would be understood by all, thus merging the interdisciplinary languages. The SSR evaluates and assesses the following: attention, mobility, problem solving, processing information, receptive language (listening), and expressive language (speaking). Please see Table 1. The SSR provides descriptive examples in each category to help guide scoring along a continuum. The evaluator is encouraged to score each domain holistically, to consider all observed, expressed, and written data to determine each categorical score [9].
Each criterion of the SSR was created by this author. Physical, occupational, speech language therapists, and educator reviewed the SSR for face validity and validity of content to ensure congruence with the rehabilitation department philosophy, mission, and patient outcomes. Revisions were recommended and made based on their knowledge.
Rubric scoring
The scoring method used with the SSR follows a continuum where 4 for “Advanced High”, 3 for “Advanced”, 2 for “Intermediate”, and 1 for “Beginner”. To score each of the six domains by obtaining a sum of scores for each circled cell in each of the domains, a sum score ranges from advanced high of 24 to beginner of 6. Scoring for Advanced High is 20–24, Advanced 15–19, Intermediate 10–14, and Beginner 6–9. For example, a student who received one 4, one 3, three 2s, and one 1 on the SSR equaling 14 points which gives a score of Intermediate. Beginner level score indicates more difficulty in completing tasks. Intermediate level score indicates less support needed and more ability to complete the task but with difficulty, thus indicating the student may require a recommendation for support through special education or Section 504. Advanced score indicates less difficulty with completing the task and less support needed by the teacher and therefore a recommendation through Section 504 would be enough to support the student. Advanced High score indicates that the student would be able to complete all tasks independently with little or no supports by the teacher and either a recommendation to return to school to with no supports would be made or to Section 504. The final score of the rubric evaluation tool with a higher number indicates fewer accommodations required in the school setting. Each criterion of the SSR was created by this author with the help of physical, occupational, and speech therapists. This was designed when the school simulation was completed using the SSR so that the educational staff would be able to share the results with the medical team in terms understood by all, thus merging the interdisciplinary languages.
Methods
A 5-year, 5-month-old female with herpes simplex virus encephalitis participated in the intervention consisting of two 45-minute sessions involving a school simulation in 2018. The initial SSR was administered at the beginning of admission and the second prior to the IRU discharge. There were 24 days of intervention consisting of daily inpatient rehabilitation which included physical, occupational, and speech language therapies that lasted an hour per session each day. A school simulation can be described as a student in a hospital classroom, asked to perform tasks similar to those in a classroom. The SSR is an instrument that scores performance in a simulated school environment such as taking notes, sharpening a pencil, and managing the cafeteria and restrooms. The student was asked to spell word families, add single digits, and sequence picture tasks of ‘what comes next’ activities. While performing these tasks, the evaluator used the SSR as shown in Table 1 to rate the student. The main purpose of the SSR was to assess school performance. The SSR provides descriptive examples in each category to help guide scoring along a continuum. The evaluator is encouraged to score each domain holistically and consider all observed, expressed, and written data to determine each categorical score [9]. As in this case study, the evaluator observed the participant perform specific classroom tasks and chose which descriptive level she matched for each criteria measured.
Discussion of findings
From the initial school simulation to the final one, the participant improved performance in all areas assessed. Her initial SSR the participant scored 8 out of 24 (Beginner) and the final SSR total was 21 out of 24 (Advanced High) (Fig. 1). Through the school simulation the author was able to determine if the participant had the ability to problem-solve scenarios typically experienced in a classroom setting such as: where to turn in papers, what to do if your pencil lead breaks, and how to manage the cafeteria and restrooms. Other areas assessed included whether she had the mobility, attention and expressive language to navigate her surroundings. The student was asked to perform grade-level appropriate tasks involving math problems that involved basic math functions with single digits. The student was also asked to spell word families which she was able to do successfully: cat, hat, sat, fat, bat and hot, pot, lot. Sequencing was a task the student was able to accomplish successfully when presented with wooden pictures of ‘what comes next’ activities. In the areas of attention and mobility, the student increased from a score of 2 to 4 between the first and last SSR. Based on her final simulation and SSR score classroom accommodations were provided to the school to help her successfully reintegrate into the classroom setting. Success was measured by a follow-up phone conversation with the participant’s parents to determine if the school recommendations provided by the IRU medical team were helpful for the student when she returned to school.
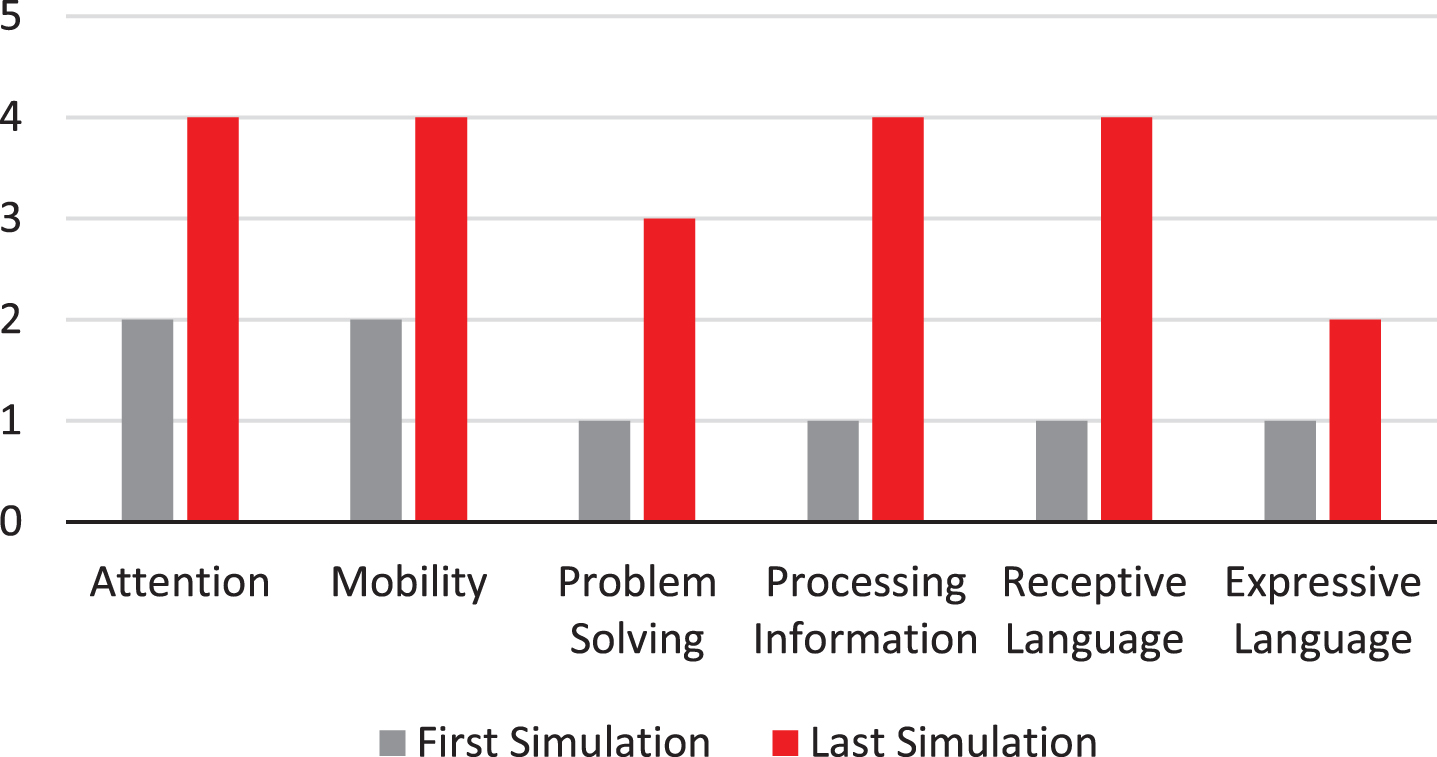
School simulation results.
There were limitations to the simulation in the hospital school setting. Providing the typical distractions of a classroom that the student would normally encounter is difficult in a hospital environment. Moreover, the SSR does not allow for certain personality characteristics that could explain the reason for certain scores: shyness, etc. The patient was extremely shy and would not verbally respond to certain answers therefore, her expressive language score was lower due to this behavior. Students with dysarthria or other speech difficulties would be limited in the expressive category. Subjectivity on the part of the evaluator is always open to interpretation when using rubrics as is the potential for unconscious bias.
Conclusions and future directions
The SSR provided valuable information to the medical disciplinary team which has led to improved communication with school educators and personnel giving them the knowledge needed to provide accommodations to students reintegrating back to school following acquired brain injuries. This was the first SSR tool found in the literature that focused on pediatric hospital-to-school reintegration with ABI. This tool allowed the medical disciplinary team to make appropriate educational accommodations for school reintegration. The usage of the SSR with children who have sustained an ABI is continuing to expand.
Conflict of interest
The author has no conflicts of interest or funding to report.
Ethical considerations
This study, as a case study, is exempt from Institutional Review Board approval.