
Abstract
PURPOSE:
To examine language outcomes in the short-term stage (i.e., within three months) of early childhood traumatic brain injury (TBI).
METHODS:
A retrospective chart review over a 10-year period (January 1, 2007 to December 31, 2016) was completed at a single-site inpatient rehabilitation hospital. Inclusion criteria were children aged 15 months to five years 11 months with a diagnosis of closed TBI.
RESULTS:
Twenty-four charts were included in the descriptive analysis of language; there were fewer children with expressive language scores (n = 18) than receptive language scores (n = 24), likely due to word retrieval difficulties as per clinical documentation. Effects of TBI on language performance were more pronounced in receptive than expressive language. For children with scores in both receptive and expressive language areas (n = 18), five children had below average scores. These children were described as having language delays pre-injury (n = 2), lower exposure to English (n = 1), information processing difficulties (n = 1), and difficulties with formulation and organization of language (n = 1).
CONCLUSION:
This study represents an initial step in understanding expressive and receptive language performance shortly after early childhood TBI. Challenges with assessment as well as directions for future research are discussed.
Introduction
Traumatic brain injury (TBI) is a leading cause of death and disability in children [1], with children under four years old the predominant age group visiting the emergency department [2]. Despite these statistics, research on early childhood TBI is less established in comparison to school-aged TBI populations. The need for early childhood TBI research is crucial as earlier age of injury is a critical determinant of long-term outcome; children injured younger are impacted by injury to a greater degree than children injured older, particularly for moderate and severe TBI [3]. Physically, young children are prone to diffuse injury due to their larger heads supported by smaller necks [4] and greater flexibility of cranial bones [5]. A diffuse injury increases the extent of damage to neural networks, impacting the availability of healthy brain networks to support reorganization post-injury [6]. Functionally, young children have not consolidated cognitive and language skills to the extent that older children have due to their stage of development at the time of injury [3, 8]. A TBI occurring when consolidated skills are few is disruptive to development, impacting cognitive-linguistic skill acquisition post-injury. Thus, studying TBI in young children is essential in understanding the unique outcomes of this vulnerable population.
Understanding the effects of early childhood TBI is complex, particularly as it relates to distinguishing developmental concerns from acquired language difficulties. This disruption adds to the already challenging task of preschool language assessment, as variability in rates of language acquisition exists among neurotypically developing populations [9]. Thus, it is not surprising that most early childhood TBI research is conducted years post-injury once language levels have stabilized and pre-injury developmental concerns have been confirmed or ruled out. Further, examination of long-term language outcomes allows for administration of higher-level language tasks such as narrative discourse, reading comprehension, and pragmatic language, tasks which are vulnerable to TBI regardless of injury severity [10–13].
Impairments in higher-level language identified in long-term studies of early childhood TBI demonstrate the persistent impact of injury on scholastic and social success. However, characterizing short-term language outcomes is a necessary first step in understanding the impact of foundational language skills prior to the emergence of higher-level language difficulties. Further, examining language performance in the short-term stage of early childhood TBI recovery is necessary for appropriate parent education and resource allocation. Specifically, describing language performance to parents in a manner that does not preclude the absence of language difficulties in the future, and initiating referrals to appropriate community partners (e.g., preschool or school board speech and language services) that highlight language areas requiring long-term follow-up.
To date, there are limited reports on short-term language outcomes following early childhood TBI. Those that exist focus on measures of semantic knowledge via expressive and receptive vocabulary measures [14–19], an area that is relatively spared in young children sustaining TBI. Describing language performance in early childhood TBI using omnibus language measures provides a comprehensive language profile not found in previous studies. Additionally, examining the effects of TBI via standardized mean difference may assist in understanding the impact of injury to a greater degree than routine statistical analysis (e.g., t-tests) alone. Lastly, exploring individual language scores allows for inclusion of children with demographic (e.g., dual language learning) and pre-injury characteristics (e.g., pre-injury language delays), an exploration that has not been completed in pediatric TBI research.
The primary aim of the study was to describe language performance of young children with TBI (i.e., < 6 years of age) within three months of injury via clinical language measures used by Speech-Language Pathologists (SLPs). The second aim of the study was to examine the effects of TBI on language performance when compared to normative data. The third aim of the study was to explore individual language performance as it relates to demographic (e.g., languages spoken) and pre-injury characteristics (e.g., reported language delays), an exploration overlooked in previous studies. To meet these aims, a retrospective chart review was selected as the study design. Due to the descriptive, exploratory nature of the study, specific hypotheses were not theorized.
Methods
Study population
Charts that were reviewed derived from Holland Bloorview Kids Rehabilitation Hospital’s connect2research registry based on inpatient admission diagnosis and age at admission to Holland Bloorview. This study was approved with waived consent by Holland Bloorview’s Research Ethics Board (REB #17-755).
Inclusion criteria
Charts of children between the ages of 15 months to five years 11 months with an inpatient admission diagnosis of TBI were included. The lower range of 15 months was chosen as this is an age with an identifiable milestone of first word use. The upper range of five years, 11 months was chosen to be consistent with discharge criteria from provincial preschool speech and language programs. All children had been admitted to brain injury rehabilitation services at Holland Bloorview between January 1, 2007, and December 31, 2016, and were within three months of injury. Charts of children with a diagnosis of TBI were identified by Information Systems using the International Classification of Diseases-Tenth Revision [20] of injuries to the head (S00-S09) or sequelae of injuries of head (T90). Identified charts were then pulled by Health Data Records for the study.
Exclusion criteria
Charts of children with documentation of previous head injury, an open (i.e., penetrating) TBI, inflicted (i.e., non-accidental) TBI, or an acquired brain injury other than TBI (e.g., tumors, stroke, and encephalitis) were excluded. No exclusion criteria of demographic (e.g., dual-language learners) or pre-injury factors (e.g., parent report of language delay) were applied to this study in order to characterize language performance of a representative, multicultural population.
Data extraction
As per retrospective chart review considerations outlined by Vassar and Holzmann [21], descriptive and numerical data were extracted from each chart to a standardized study-specific data collection table by the first author (C.C.). Extracted data included demographic information (e.g., sex, age at injury, languages spoken), pre-injury factors (e.g., reported language delay, developmental concerns and/or diagnoses), injury-related factors (e.g., Glasgow Coma Scale orthopedic injury comorbidity), standard scores from language measures (e.g., admission assessment), clinical interpretations of language performance (if available), and language measures used. Pre-injury and injury-related characteristics were obtained from physician admission notes. Demographic information and language scores were obtained from SLP assessment notes and assessment record forms (if available). Charts with scores from vocabulary measures only were excluded from the data analysis. Additionally, charts with language scores beyond two weeks of inpatient admission were excluded from the data analysis to mitigate the effects of intervention.
Data analysis
Descriptive statistics were used to summarize demographics, pre-injury factors, and injury-related factors for all charts that met age and diagnostic inclusion criteria. From here, descriptive statistics were used to summarize standard scores from language measures. Means, standard deviations, and sample size were used to calculate the estimated effects of preschool TBI on language performance using RevMan 5.3 software [22]. Language measures were stratified within receptive and expressive language areas. In the absence of a control group, normative data from each language measure was used (M = 100, SD = 15). The sample size of the control group was taken from the total standardization sample of each language measure for conservative estimates of effect. A random effects model [23] was applied to calculate estimated effect sizes based on standardized mean differences of language scores using a 95% confidence interval. Effect sizes were characterized using Cohen’s (1988) categorization of small (0.2), medium (0.5), and large (0.8) [24]. A negative effect size (g < 0) indicated worse performance of the TBI group in comparison to normative data, and a positive effect size (g > 0) indicated better performance of the TBI group compared to normative data. A total of three estimated effect size calculations were completed: (i) all language scores, (ii) exclusion of scores from children with pre-injury language delays, and (iii) exclusion of scores from children with pre-injury language delays and children identified as dual-language learners.
For children with scores in both receptive and expressive language areas, individual scores were plotted to illustrate performance differences. A Pearson correlation was used to examine the strength and direction of receptive and expressive language scores.
Results
Charts meeting inclusion criteria
Forty-eight charts were identified after applying diagnostic criteria of age and closed TBI; twenty-one charts did not have extractable language score data. The age of children that did not have language score data (M = 2.80, SD = 1.23) compared to the age of children that had language score data (M = 4.46, SD = 1.04) were significantly younger (t(46) = 5.05, p < 0.00001). A second notable characteristic of charts without language score data included learners of English as a second language. Additional reasons for absent language scores gathered from clinical documentation included short length of stay (n = 2), query of autism spectrum disorder (n = 2), and significant impairment (n = 1). See Table 1 for characteristics of charts with and without language score data.
Demographic, pre-injury, and injury-related characteristics of charts with language score data and charts without language score data
Demographic, pre-injury, and injury-related characteristics of charts with language score data and charts without language score data
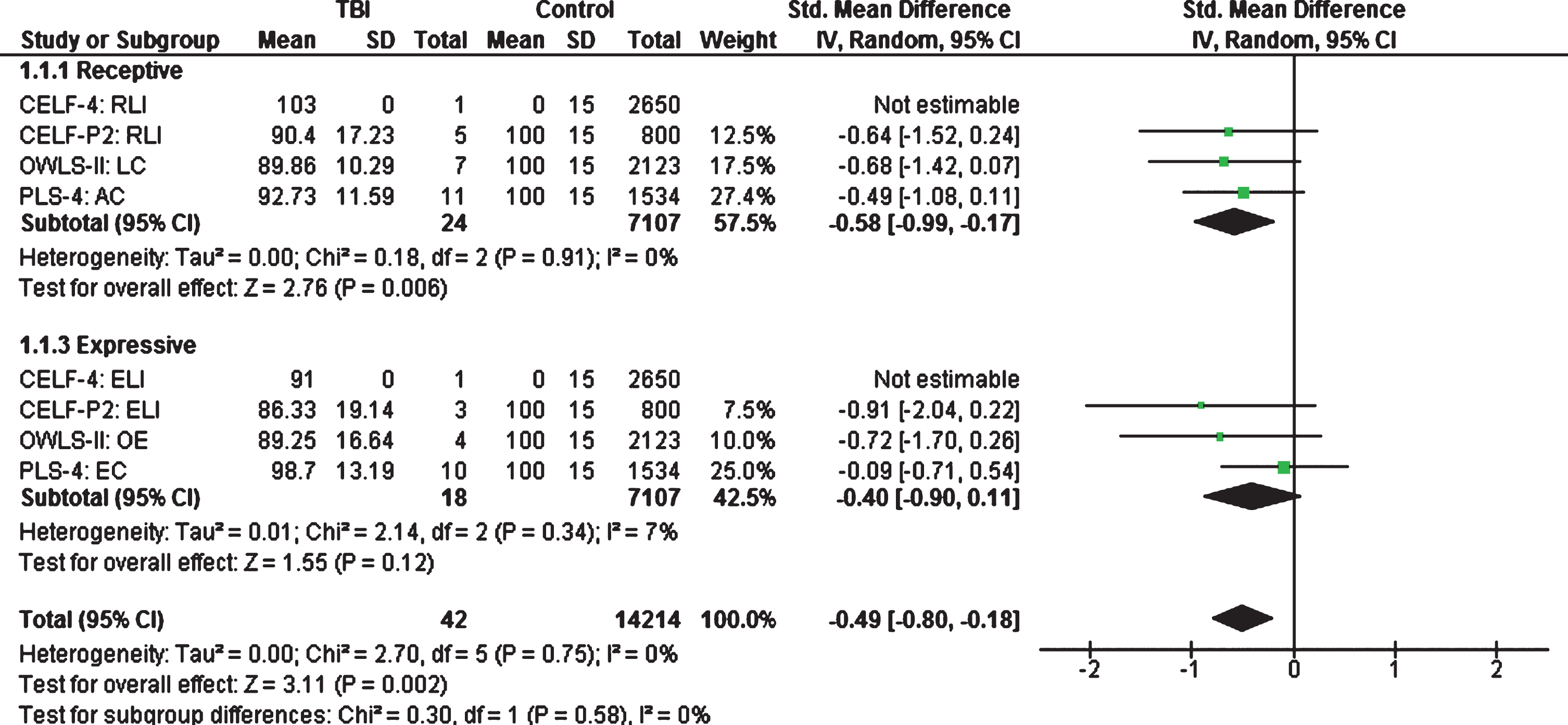
Estimated effect sizes of early childhood TBI on language performance when compared to normative data.
Twenty-seven charts had extractable language score data; three charts were excluded from the descriptive analysis as two children had receptive vocabulary scores only and one child had language scores from discharge assessment only. Therefore, a total of 24 charts were used in the descriptive analysis of receptive and expressive language performance in preschool TBI (Fig. 1).
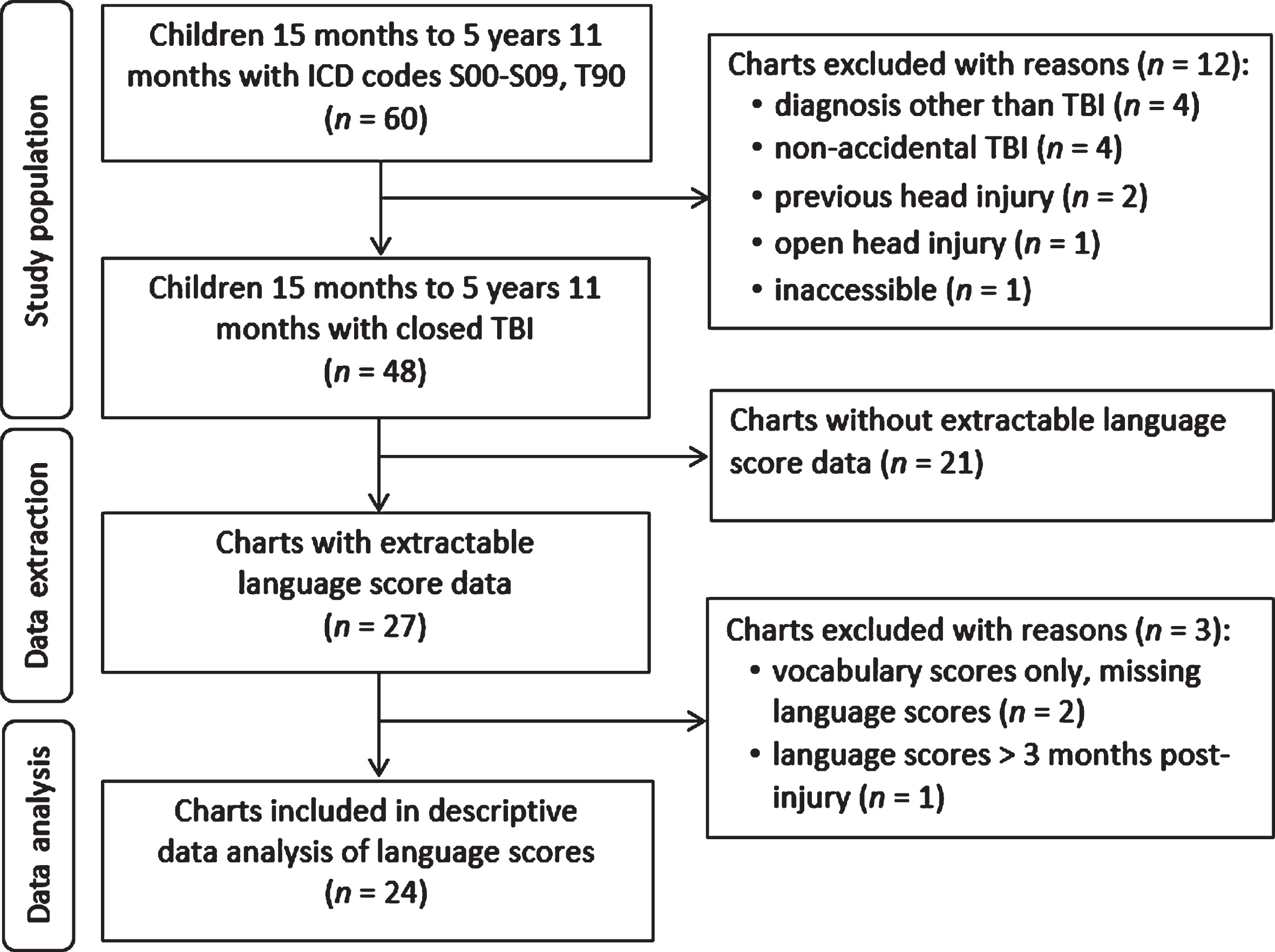
Flow diagram of chart inclusion for descriptive data analysis.
Demographic characteristics extracted from the 24 charts with language data included 17 males and seven females; age at injury ranged from 2.17 to 5.92 years (M = 4.56, SD = 1.04). Several children (n = 7) were clinically described as being exposed to two languages in the home, hereafter referred to as dual-language learners. Languages in addition to English included: Cantonese (n = 2), Mandarin (n = 1), Tibetan (n = 1), Punjabi (n = 1), Yoruba (n = 1), and Gujarati (n = 1).
Language score data stemmed from the following measures: the Preschool Language Scale-Fourth Edition (PLS-4 [25]; n = 11), the Oral and Written Language Scales-Second Edition (OWLS-II [26]; n = 7), the Clinical Evaluation of Language Fundamentals-Preschool Second Edition (CELF-P2 [27]; n = 5), and the Clinical Evaluation of Language Fundamentals-Fourth Edition (CELF-4 [28]; n = 1). Receptive language scores were obtained from the indices of Auditory Comprehension (PLS-4; n = 11), Listening Comprehension (OWLS-II; n = 7), and the Receptive Language Index score (CELF-P2; n = 5, CELF-4; n = 1). Expressive language scores were obtained from the indices of Expressive Communication (PLS-4; n = 10), Oral Expression (OWLS-II; n = 4), and the Expressive Language Index score (CELF-P2; n = 3, CELF-4; n = 1).
The average length of time between injury and assessment was 27 days (M = 26.58, SD = 15.89). Age (in years) at assessment was the youngest for the PLS-4 (M = 3.68, SD = 0.76) in comparison to the OWLS-II (M = 5.33, SD = 0.57), the CELF-P2 (M = 5.15, SD = 0.39), and the CELF-4 (M = 5.92, SD = 0). A frequency count of scores by language area revealed more receptive language scores (n = 24) than expressive language scores (n = 18). Reasons for missing expressive language scores may have been due to word retrieval difficulties as described in clinical documentation.
Estimated effect sizes of TBI on language performance
Estimated effect sizes of early childhood TBI on language performance in comparison to normative data was medium for receptive language (g = –0.58, CI 95% [–0.99, –0.17], n = 24) and expressive language (g = –0.40, CI 95% [–0.90, 0.11], n = 18). Estimated effects of injury were statistically significant for receptive language (p = 0.006) only (Fig. 2).
Removal of language data from children with pre-injury language delays (n = 5) maintained a medium effect size for receptive language (g = –0.46, CI 95% [–0.93, 0.00], n = 19) and reduced the effect size to small for expressive language (g = –0.36, CI 95% [–1.15, 0.44], n = 15). Estimated effects of injury were not statistically significant in receptive or expressive language (Fig. 3).
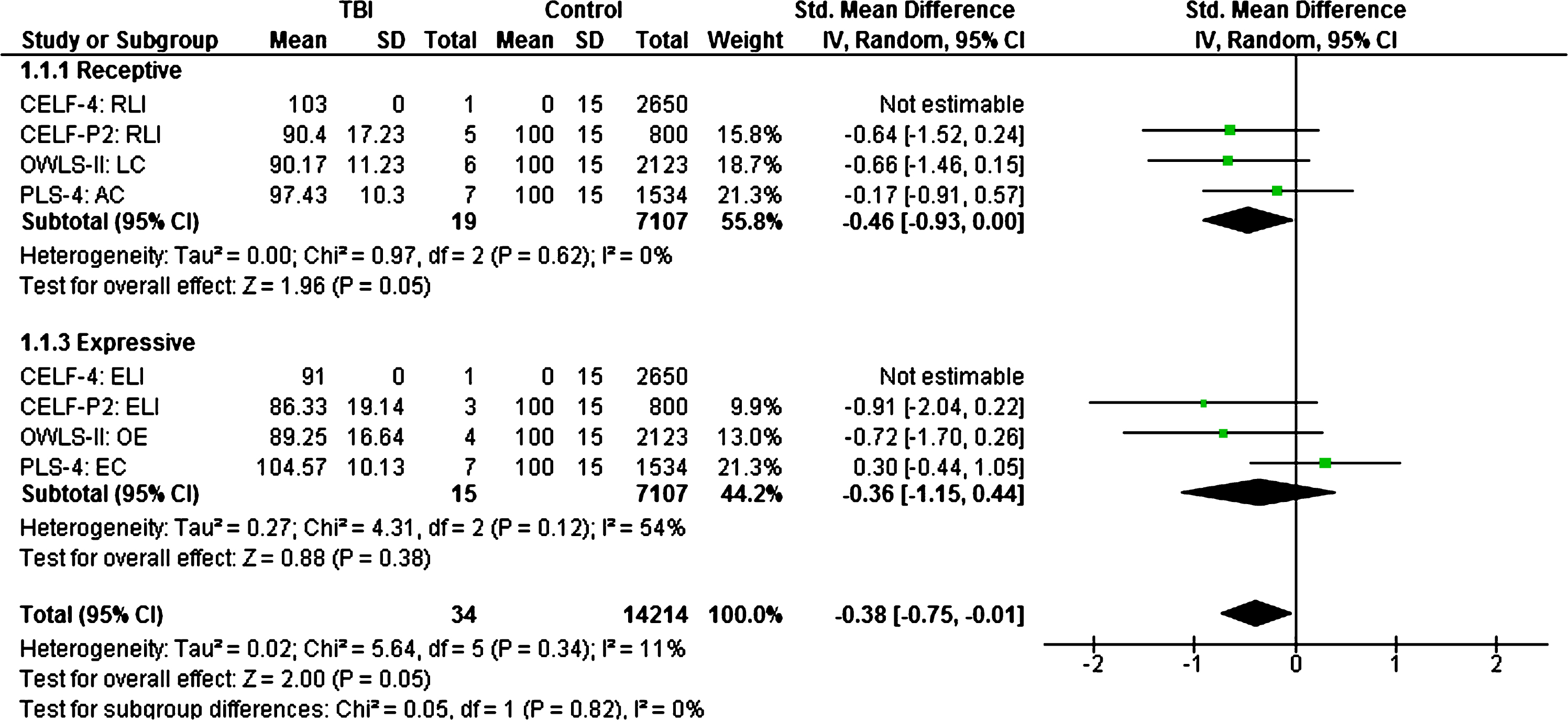
Estimated effect sizes of early childhood TBI on language performance when compared to normative data (children with pre-injury language delays excluded).
Additional removal of language data from children described as dual-language learners (n = 4) maintained a medium effect size for receptive language (g = –0.49, CI 95% [–1.01, 0.04], n = 15) and eliminated the effect of injury on expressive language (g = –0.13, CI 95% [–0.93, 0.67], n = 12). Estimated effects of injury were not statistically significant in receptive or expressive language (Fig. 4).
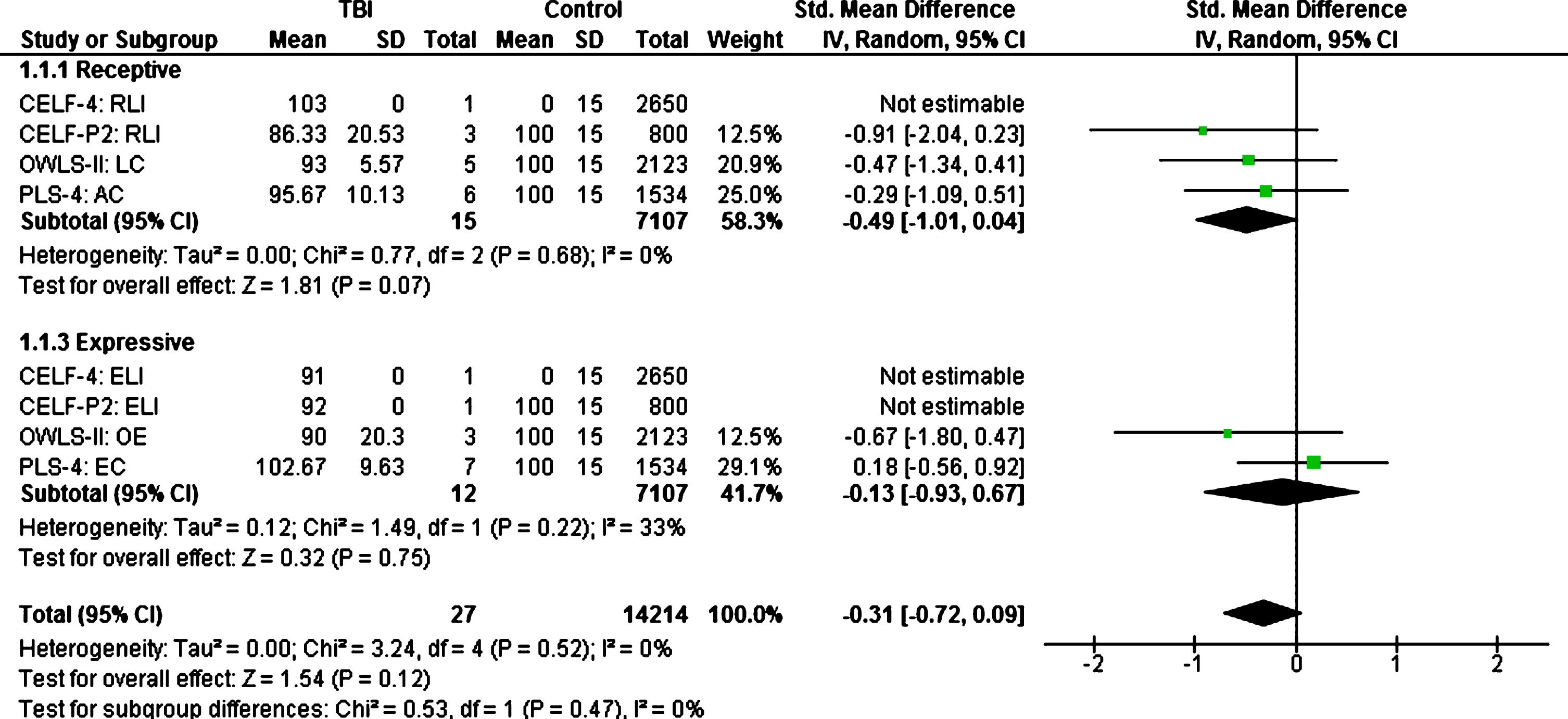
Estimated effect sizes of early childhood TBI on language performance when compared to normative data (children with pre-injury language delays and dual-language learners excluded).
Eighteen charts had extractable language data in both receptive and expressive areas; these scores were plotted to show individual language performance (Fig. 5). An examination of scores revealed that 72% of the sample (n = 13) performed within the average range (85 to 115) in both language areas. The remaining 28% of the sample (n = 5) performed below the average range (i.e., < 85) in one or both language areas. Two children with below-average scores in both expressive and receptive language were identified as delayed in language pre-injury. Two children with below-average scores in expressive language were clinically described as having limited exposure to English syntax (n = 1) and difficulties with formulation and organization of expressive language (n = 1). One child with a below-average score in receptive language was clinically described as having difficulties processing information (n = 1).
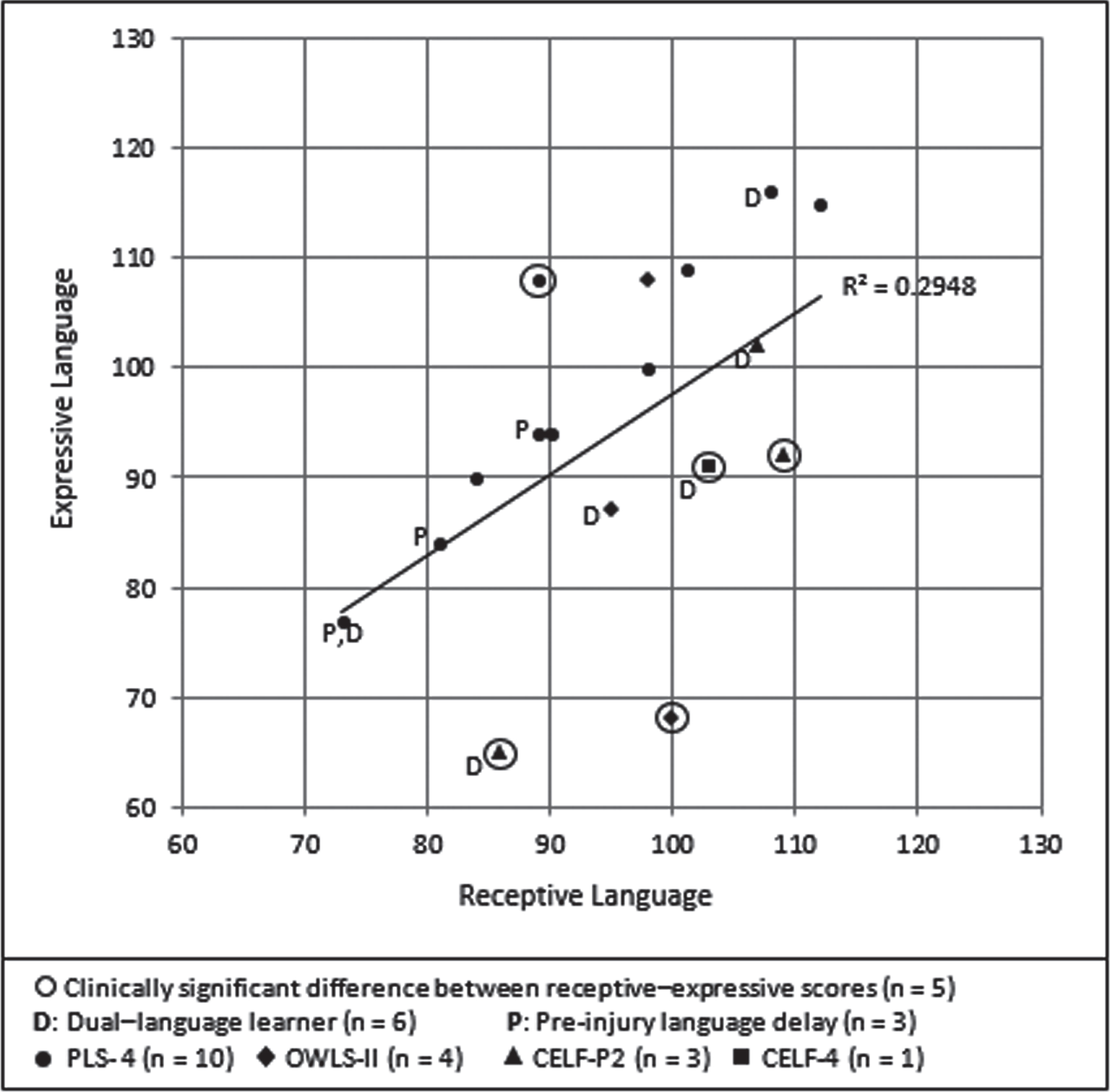
Scatterplot of receptive and expressive language scores for children with scores in both areas. Note: Each data point represents one child’s receptive and expressive language score. Two children have the same data points (90, 94); one data point is from the PLS-4 and one data point is from the OWLS-II.
Results of the Pearson correlation showed a significant, positive, linear association between receptive and expressive language scores (r(16) = 0.54, p = 0.02). This suggests that most children had generally ‘balanced’ scores between language areas. However, upon inspection of individual scores, there were five children that had clinically significant differences between receptive and expressive language scores (i.e., an expressive and receptive point difference that is present in less than 10% of the standardized sample). Children with significantly lower scores in expressive language than receptive language were described in clinical documentation as having poor formulation and non-specific vocabulary (n = 2), poor planning and organization of language (n = 1), and poor syntax influenced by dual-language learning (n = 1); interpretation of significantly lower scores in receptive language than expressive language (n = 1) was not found in clinical documentation. Removal of data from children with clinically significant language discrepancies increased the strength of association between receptive and expressive scores (r(11) = 0.91, p = <0.0001).
Short-term language outcomes (i.e., within three months) of early childhood TBI were examined via a retrospective chart review. Broad inclusion criteria were applied to ensure representation of this site’s multicultural population. Individual language performance was explored as it related to demographic (e.g., languages spoken) and pre-injury characteristics (e.g., reported language delays) not otherwise described in early childhood TBI literature [14–18]. Findings from the study revealed that children with language score data were significantly older on average (4.5 years) than children without language score data (2.8 years). Group analysis of language scores in comparison to normative data revealed statistically significant effects of injury on receptive language only. Upon removal of language data from children identified as having pre-injury language delays, effects of injury on receptive language were no longer significant. Individual analysis of language scores revealed clinically significant differences in receptive and expressive language scores for five children. Interpretation of study findings and challenges with language assessment in early childhood TBI are discussed.
Children without language score data were significantly younger than children with language score data. This finding was not surprising as young age is one challenge of early childhood TBI language assessment [9]. Infants and toddlers were included in the study sample to capture language performance in children under the age of three years via PLS-4 scores; however, only two children under the age of three years had language score data. Raising the inclusion criteria to three years of age, as seen in other outcome studies of early childhood TBI [14–16], would have reduced the number of charts without score data, yet not eliminated them; several children (n = 8) in the study that were over the age of three years did not have language scores likely due to English as a second language, short length of stay, severe impairment from injury, and developmental concerns (e.g., autism spectrum disorder) as described in clinical documentation. For these children, language was captured via unstructured, play-based assessment.
An interesting finding in the statistical analysis of effect sizes of TBI on language performance was that the effects of injury were more pronounced in receptive language than expressive language. Reduced effects in expressive language may have been due to sample size, with less children completing expressive language testing in comparison to receptive language. Reduced effects in expressive language may have also been due to language measure; children with PLS-4 scores had a notably small effect size for expressive language compared to children with OWLS-II and CELF-P2 scores. This may be due to the different construct of the PLS; the PLS-4 provides a broad overview of developmental language skills [25] whereas the CELF-P2 and OWLS-II examines discrete language skills required for academic success [26–28]. Further, the PLS-4 provides more visual supports than the OWLS-II or the CELF-P2 [29], an advantage for a clinical population that excels when cognitive load is minimized [30, 31]. Lastly, the PLS-4 has been found to have a core language score mean that is five points higher than the CELF-P2 for children in the standardization sample who completed both tests [27]. Taken together, the estimated effect sizes for expressive language may have been an underestimate of the true effect of injury due to sample size and language measure.
Not surprisingly, removal of language score data from children reported as having pre-injury language delays (n = 5) increased group mean language scores; this reduced the estimated effects of injury, particularly for expressive language. This finding supports literature that has found pre-injury functioning as a predictor of post-injury language outcomes [15] and suggests that language scores within three months of early childhood TBI may be a greater reflection of pre-language ability than post-injury effects. However, without pre-injury language data we cannot confirm these associations. Obtaining reliable, pre-injury language data is one of the greatest challenges of assessment in young children with TBI compared to children injured older. For children injured older, pre-injury language data can be obtained from parent report, teacher report, and school records; however, for children injured young, parent report is the driver behind pre-injury communication data [9, 30]. A minimum age of inclusion of 15 months was used in this study with the assumption that pre-injury language delays would have been identified in clinical documentation via parent report (e.g., delayed first word use); however, whether pre-injury language delays were accurately reported cannot be confirmed due to the retrospective chart review study design.
In contrast to the trends observed upon removal of language data from children identified as having pre-injury language delays, the removal of language score data from dual-language learners had minimal impact on group mean scores and estimated effects. This may be due to the variability in language performance that accompanied dual-language learners; four of six dual-language learners had relatively higher receptive than expressive language scores, consistent with literature that describes expressive versus receptive language profiles of healthy young bilingual children [32]. However, two children had the opposite language profile with relatively higher receptive than expressive language scores. Variability in language profiles may stem from age of language exposure, as the acquisition of grammatical morphemes [33] and overall proficiency of language differs over time [34–36]. Although data on timing of language acquisition (e.g., sequential versus simultaneous) was not available in clinical documentation, this finding brings awareness to the complexities of including dual-language learners in the short-term stage of preschool TBI. In other words, the variability of language acquisition of dual-language learners may be too great to fully delineate the short-term effects of TBI versus the effects of dual-language learning.
For children with scores in both language areas (n = 18), inspection of individual scores revealed five children with clinically significant differences between their receptive and expressive language scores (i.e., a raw score difference present in less than 10% of the standardization sample). Small sample size precluded statistical analysis of variables of interest, such as if languages spoken or pre-injury language delays contributed to score discrepancies between expressive and receptive language. Additionally, lack of neuroimaging data prevented exploration of neural profiles, such as if lesion location contributed to word retrieval difficulties.
Conclusion
The retrospective chart review examined short-term receptive and expressive language performance in early childhood TBI via clinical language measures used by SLPs. This was completed by extracting language scores documented within two weeks of inpatient admission, before the commencement of intervention. Children who participated in standardized language assessment generally performed within the average range (e.g., 85 to 115 standard score). Estimated effects of early childhood TBI were larger in receptive language than expressive language; however, this finding is cautionary at best as more children completed receptive than expressive language testing. Further, estimated effects of injury in expressive language were nearly absent in children who completed the PLS-4 in comparison to children who completed the CELF-P2 or OWLS-II, reducing the overall effect of injury. Children who had scores in both receptive and expressive language had relatively similar scores across language areas, however a handful of children had clinically significant differences between receptive and expressive language scores. Factors that may have influenced performance included pre-injury language delays and dual-language learning, although associations could not be confirmed due to small sample size.
To address research questions that arose from the retrospective chart review, a larger prospective longitudinal study commencing at the time of injury (e.g., acute care) is needed to track the evolution of injury on language over time and examine predictors of outcome such as dual-language learning, pre-injury language levels, and neural profiles. A longitudinal study that uses consistent language measures may assist in measurement continuity and may also permit exploration of associations between lower-level and higher-level language skills. Examples of outcome measures that could be used include the Vineland Adaptive Behavior Scales [37] to capture pre-injury functioning when administered shortly after injury, and the use of the CELF-P3 [38], the CELF-5 [39], and CELF-5 Metalinguistics [40] to capture language skills over time.
One unique contribution of the study revealed the value of qualitative data provided in clinical documentation, particularly interpretations of language performance (e.g., difficulties with word retrieval, formulation and planning, and information processing). Future research studies in early childhood TBI are encouraged to incorporate qualitative data (e.g., clinical interpretation) as this may provide a more accurate way to capture the subtle effects of injury evidenced in the early stages of recovery. Further, capturing qualitative data in a standardized manner may assist in providing informative language data for children that may not be able to participate in formal language testing. A second unique contribution of the study was the use of effect sizes and descriptive analysis of individual language scores. Effect sizes allowed for more meaningful interpretation of the impact of injury, especially as most children scored within the average range on clinical language assessment. Descriptive analysis of individual language scores allowed for a depiction of the variability in expressive and receptive language scores, generating further questions as to what factors contributed to discrepancies between language areas. Taken together, future studies are encouraged to incorporate a qualitative and quantitative approach when examining language outcomes in early childhood TBI, as this may assist in understanding the subtle effects of TBI as it relates to individual performance on clinical language measures.
Overall, it is important for clinicians to recognize that performance on standardized language assessment in early childhood TBI is only one piece in understanding the long-term higher-level language difficulties experienced in this population. Further, the language area identified as a relative strength in the early stages of TBI recovery does not preclude the absence of long-term impairment in that area, as expression and comprehension of language can never be completely separated [38]. While standardized language assessment may be a necessary first step for children who may not have had a comprehensive language assessment after discharge from acute care settings, effects of injury may be minimized when cognitive processes are still in development [41]. Therefore, it is essential that young children with TBI receive long-term follow up when higher-level language tasks can be administered and assessment of communication competency outside of a testing environment can be completed [42]. Lastly, an interdisciplinary approach to TBI management is essential to fully grasp the complex cognitive-linguistic challenges that emerge in the long-term stages of early childhood TBI [43].
Footnotes
Acknowledgments
This work was supported by an Ontario Graduate Scholarship and the Holland Bloorview Kids Rehabilitation Hospital Foundation via a Kimel Graduate Student Scholarship in Pediatric Rehabilitation awarded to the first author (CC). The authors would like to thank Dr. Peter Rumney for his contribution to this work.
Conflict of interest
In the past two years, Dr. Shannon Scratch has been employed as a Clinician Scientist at Holland Bloorview Kids Rehabilitation Hospital. Dr. Scratch holds research grants that provide money to the institution to support the conduction and dissemination of research from the Social Sciences and Humanities Research Council and Holland Bloorview Kids Rehabilitation Hospital Foundation.
In the past two years, Dr. Nick Reed has been employed as a Senior Clinician Scientist at Holland Bloorview Kids Rehabilitation Hospital and an Associate Professor at the University of Toronto. Dr. Reed holds research grants that provide money to the institutions to support the conduction and dissemination of research from the following entities: Canadian Institutes of Health Research, Public Health Agency of Canada, Special Olympics Canada, Ontario Neurotrauma Foundation, and Greater Toronto Hockey League.
In the past two years, Dr. Deryk Beal has been employed as a Clinician Scientist at Holland Bloorview Kids Rehabilitation Hospital and an Assistant Professor at the University of Toronto. Dr. Beal holds research grants that provide money to Holland Bloorview and the University of Toronto to support the conduction and dissemination of research from the following entities: Natural Sciences and Engineering Research Council of Canada, Canadian Institutes of Health Research, Canada Foundation for Innovation and the Holland Bloorview Kids Rehabilitation Hospital Foundation.
Dr. Carly A. Cermak has no conflicts of interest to report.