
Abstract
PURPOSE:
More than 50,000 children are hospitalized yearly in the U.S. for acquired brain injury (ABI) with no established standards or protocols for school re-entry and limited resources for hospital-school communication. While ultimately the school has autonomy over curricula and services, specialty physicians were asked about their participation and perception of barriers in the school re-entry process.
METHODS:
Approximately 545 specialty physicians were sent an electronic survey.
RESULTS:
84 responses (43% neurologists and 37% physiatrists) were obtained with a response rate of ∼15%. Thirty-five percent reported that specialty clinicians currently make the plan for school re-entry. The biggest challenge for school re-entry noted by physicians was cognitive difficulties (63%). The biggest gaps perceived by physicians were a lack of hospital-school liaisons to help design and implement a school re-entry plan (27%), schools’ inability to implement a school re-entry plan (26%), and an evidence-based cognitive rehab curriculum (26%). Forty-seven percent of physicians reported that they did not have adequate medical personnel to support school re-entry. The most commonly used outcome measure was family satisfaction. Ideal outcome measures included satisfaction (33%) and formal assessment of quality of life (26%).
CONCLUSION:
These data suggest that specialty physicians identify a lack of school liaisons in the medical setting as an important gap in hospital-school communication. Satisfaction and formal assessment of quality of life are meaningful outcomes for this provider group.
Keywords
Introduction
After sustaining an acquired brain injury (ABI) such as traumatic brain injury (TBI) or stroke, children have unique challenges to their activities of daily living compared to peers. Moderate-to-severe TBI can result in lifelong impairments in cognition, psychological health, and academic functioning [1, 2]. Longitudinal studies have shown higher usage of school services and lower school competency after TBI, with children injured at a younger age having lower academic skills [2]. Even children with mild TBI (mTBI) have been shown to have emotional and cognitive disturbances [3], despite normal imaging utilizing standard techniques [4]. Research-grade imaging techniques show changes in subcortical grey and white matter in patients with concussion [5], raising the possibility of unrecognized persistent physiologic changes in even mTBI cases. Children with stroke have significantly lower performance in overall intelligence, verbal ability, working memory, and processing speed compared to controls [6]. They struggle with communication disorders including dysarthria and language apraxia regardless of lesion laterality [7, 8] and have impairment in emotional regulation, executive function, and attention [9].
Children and families navigate various support systems after ABI, depending on severity of injury, needs after injury, local resources, family variables, and local legislation. In the early recovery phase after injury, support comes from medical services, with patients with more severe deficits typically participating in inpatient rehabilitation. There, the focus may be on so-called “cognitive rehabilitation,” with therapists from various disciplines working to improve fundamental cognitive skills for daily functioning. After acute recovery, children ideally return to the classroom, where the focus is on education rather than rehabilitation.
In the U.S., the Individuals with Disabilities Education Act (IDEA; originally passed as the Education for All Handicapped Children Act in 1975) provides children with disabilities the same opportunity for education as students who do not have a disability via Individualized Education Programs (IEPs); these are enforced under the Office of Special Education Programs (OSEP). Children may be offered inpatient or outpatient rehabilitation services in the medical setting, with the ultimate goal of returning to the least restrictive schooling environment under IDEA [10]. Medical and school systems have subtle but important differences in their approach to interventions and outcomes. The term “rehabilitation” is used in the medical system and not in the school setting; in the latter, accommodations and modifications to the curriculum are made as a part of an IEP. For schools, academic achievement, learning, and graduation rates are key metrics; these are not traditionally measured in the medical setting.
Within schools, children may qualify for accommodations if their health condition has an impact on their learning. In spite of this, a discrepancy between incidence of TBI and recognition in the school-based setting has been reported, with less than half of eligible students receiving formal or informal supports [11]. Injury severity and the presence of hospital-to-school transition services (including written or verbal communication between the hospital and school) were associated with improved recognition and implementation of school services [11].
Medical systems have utilized educational liaisons to communicate with school personnel since the 1970 s. The concept of a hospital-school link emerged in pediatric oncology as survival from cancers improved. It was recognized that the “child with cancer faces an increased potential for problems in social adjustment and rehabilitation” [12]. As the field has grown, the Hospital Educator and Academic Liaison (HEAL) organization was created in 2018 and today represents the premier medical liaison professional organization. Roles include facilitating hospital classrooms and communicating with the home school program. While liaisons have been proposed as a key facilitator of communication between hospitals and schools, evidence demonstrating the contribution of this service to medical outcomes is lacking.
Unmet needs for cognitive and mental health services and the gap in hospital-to-educational systems to support recovery have been well-documented for the pediatric TBI population [13, 14]. A 2015 meta-analysis of 10 papers looking at medical and educational professionals’ experiences identified six main themes: 1) lack of training and knowledge among educators, 2) lack of communication between educators, clinicians, schools, families and students, 3) lack of preparation for the transition, 4) supports available (educators reported a lack of supports available to learn about the consequences of ABI), 5) linking agents (helpful in facilitating the transition), and 6) inadequate policies and procedures that guide transitions, specifically due to “not enough students with ABI to necessitate specialized programmes” [15]. To date, initiatives have focused on improving community supports and teacher education [16]. Educators and clinicians differ in their perceived needs when working with ABI students, with the former group citing a need for more education and the latter citing availability and access to services as a key priority [17].
What is the role of the medical system in helping to bridge the communication and rehabilitation gap between the hospital and schools? Half of patients with TBI report seeing a doctor a year after injury, with a third of families reporting that cognitive rehabilitation was not recommended by the doctor [13]. Despite attempts at physician education about IEPs [18] and physicians’ belief that it is within their scope of practice, physicians are often uncomfortable with making education recommendations and engaging with the special education process [19]. Primary care providers have reported uncertainty about requirements for special education and how to identify patients in need of special education [20].
The purpose of this study was to understand the attitudes of specialty clinicians that saw patients with ABI in a concentrated fashion in follow-up (i.e., primarily neurologists and physiatrists) via a brief survey. Research questions included: Do these clinicians engage with the process of school re-entry, and, if so, how? In terms of supports, what are the biggest gaps and barriers to services as perceived by specialty physicians? Regarding the return to school, what is the primary outcome measure of importance for specialty physicians?
Methods
A 20-question electronic survey was designed by the authors and then pilot tested with feedback incorporated from 15 physicians, including neurologists and physiatrists, at multiple institutions. The survey can be found in Appendix I. The survey was framed by asking respondents to reflect on their return-to-school practices for patients hospitalized with acquired structural brain injury, highlighting TBI and stroke, and excluding concussion, encephalitis, multiple sclerosis, and brain tumors. Pediatric neurologists and physiatrists were surveyed via convenience sampling and included members of the International Pediatric Stroke Organization (IPSO) and the Child Neurology Society TBI Special Interest Group. Participants were asked to further distribute to colleagues, with a final total of 84 respondents. Not all respondents answered all questions, and that is reflected in the sample size counts. Of the approximately 545 invited responses, an estimated one-third of those were neurologists and two-thirds were physiatrists.
In this study, the term “educational liaison” was used to refer to educators employed by the medical system to communicate with outside educational systems. Respondents were allowed to self-identify their primary work setting and practice based on the key words “inpatient,” “outpatient,” “academic,” and “community;” for brevity these terms were not specifically defined in the survey. Results from the survey were tabulated in terms of frequency of responses in Stata. This research protocol was submitted to the University of California San Francisco Institutional Review Board (IRB) for approval and was found to be exempt (IRB #19-28457).
Results
84 survey responses were collected. Of those, 76 met inclusion criteria to continue the survey; specifically, they saw patients hospitalized for brain injury as a part of their practice and they asked patients and families about school. Of those 76 responses, 65 surveys were fully completed (77%) and 11 were partially completed (13%). Since 11 of the 76 respondents that satisfied the inclusion criteria didn’t fully complete the survey, there is variability in the sample sizes for some questions which reflects this missing data. The response rate was 15%, with an estimated 545 specialty physicians contacted. The study cohort required an average of 24.5 minutes for full completion of the survey.
For those respondents who reported that they did not ask patients and families about school and were not eligible to continue with the survey (8%; 7/84; one respondent completed the survey after reporting that they did not see patients with ABI), they cited that this issue was handled by another team member (e.g., social work), they were unsure what to ask, there was insufficient time in the visit, or it was not a concern in their treatment setting.
Experience and specialty of survey respondents
The respondents’ discipline and specialty were collected (Table 1). They were primarily pediatric neurologists (43%; 36/84) and physiatrists (37%; 31/84). Seven additional participants included a psychologist, two hematologists, a neuropsychologist, a radiologist and two critical care physicians. Ten respondents (12%; 10/84) did not answer this question.
Survey respondent demographics
Survey respondent demographics
Eighty-four survey responses were collected, primarily from pediatric neurologists and physiatrists. Seven additional participants included a psychologist, two hematologists, a neuropsychologist, a radiologist and two critical care physicians. The response rate was 15% with an estimated 545 specialty physicians contacted via email. Percentages were rounded to the nearest integer. ABI = acquired brain injury.
The location and practice setting were tabulated for the respondents (Table 1). Seventy-one percent practiced in the U.S. (60/84), while 14% practiced outside the U.S. (12/84); 12 participants did not respond. The most common practice setting was inpatient academic (52%; 44/84), followed by outpatient academic (29%; 24/84). The depth of experience working with patients with ABI was collected by tabulating both years of practice post-training as well as volume of patients with brain injury seen per week. The largest group of respondents had more than 10 years of experience (35%; 29/84), with 27% having 1–5 years of experience (23/84) and 25% having 5–10 years (21/84). Most respondents saw less than 10 patients with brain injury each week (49%; 41/84), with 36% seeing 10–20 (30/84) and 4% seeing more than 20 patients per week (3/84).
This study sought to understand who typically prepared a letter about return-to-school recommendations for the family to discuss with the school. For clarity, while these recommendations, which were referred to as a “plan” in the survey, are certainly not prescriptive for the school, they are often a starting point for discussion, to provide the school with context for new educational needs for a student returning to school after ABI [11]. Respondents were asked who currently made the plan for school re-entry as well as, in their opinion, who should make the plan (Fig. 1). Of the 71 responses recorded for this question, 35% (25/71) of specialty clinicians currently made the plan for school re-entry, followed by school liaisons. Nearly half of respondents (49%; 35/71) replied that school liaisons should make the plan for school re-entry, followed by 32% (23/71) reporting that specialty clinicians should make the plan for school re-entry. One percent (1/71) felt that the family should make the plan, in contrast to the 11% that did so currently (8/71). When asked “who helps” with the return-to-school plan (with multiple choices allowed), the most common responses included “I do” (n = 58), a neuropsychologist (n = 52), school liaison/educators (n = 45), therapist (n = 42), and student’s home school district (n = 41).
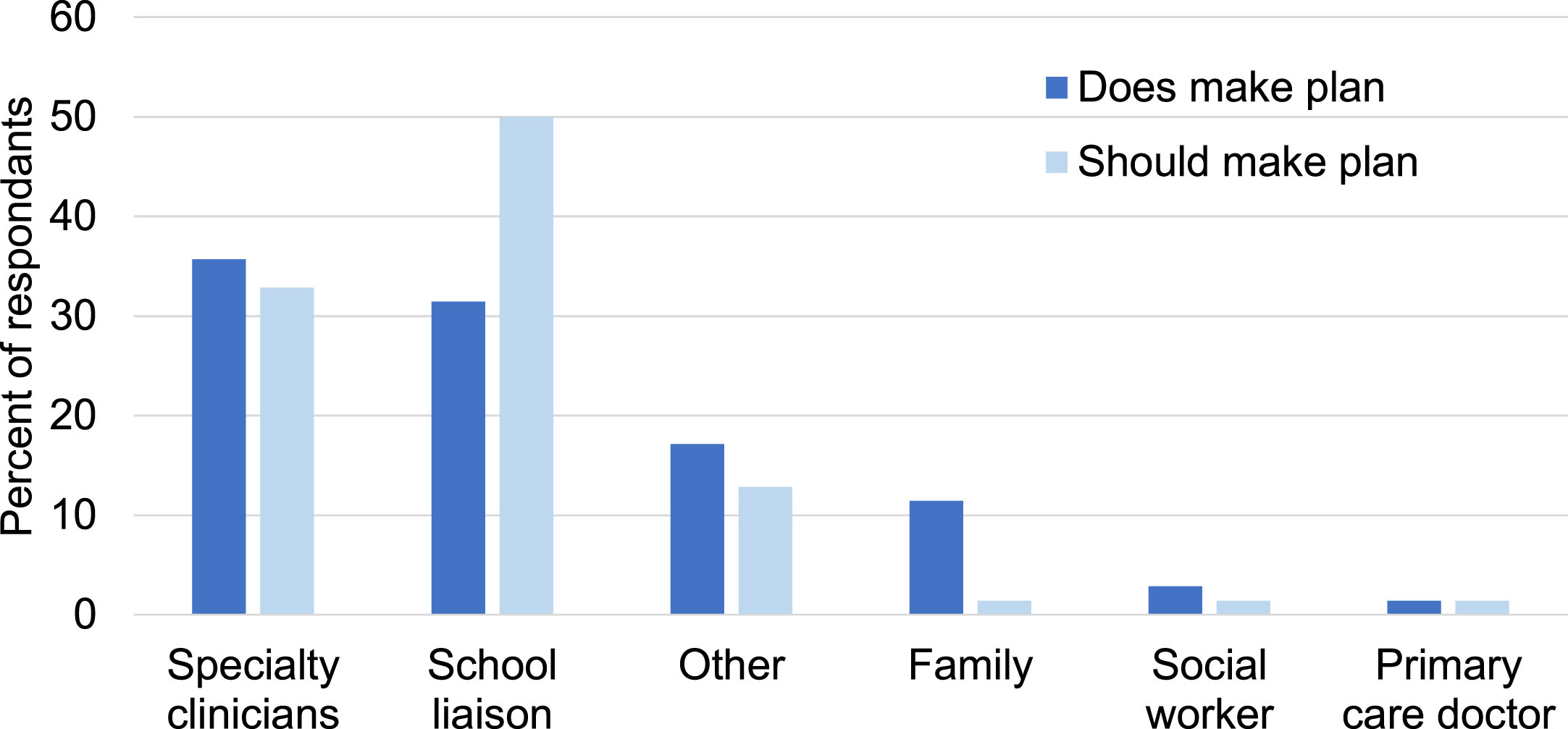
Who “does” vs “should” make the return to school plan? “Other” included respondents who declined to choose one option, preferring to write in multiple options from the above categories. n = 70 respondents.
Respondents were asked about the biggest challenges they saw for their patients for school re-entry as well as the biggest gaps in services. The biggest challenge for school re-entry identified was cognitive difficulties (64%; 44/68), followed by behavioral problems (22%; 15/68), symptom control (12%; 8/68), and lastly, physical challenges (3%; 2/68). The biggest gap in services identified by providers (Table 2) was almost evenly split among the 70 respondents to this question between school liaisons (27%; 19/70), the school’s inability to implement the plan (26%; 18/70), and an evidence-based cognitive rehabilitation curriculum (26%; 18/70).
Gaps in services identified by respondents
Gaps in services identified by respondents
Participants were asked to identify the largest gap in services that they perceived for their patients. For specific groups of professionals, they were asked to classify if their patients had satisfactory or unsatisfactory access. *“Other” responses included multiple gaps (three respondents reported lack of liaisons was an important gap), family unwilling to return to school or not important to family (n = 2), and no comment (n = 1). Percentages were rounded to the nearest integer.
Respondents were asked if their patients had adequate access to support personnel commonly utilized after brain injury, and when access was unsatisfactory, if this was due to limited supply, poor insurance coverage, or both (Table 2). Fifty-two percent of respondents reported that they had adequate personnel to communicate with the school (36/68); forty-seven percent (32/68) replied that they did not have adequate personnel. With regard to access to speech therapists, 60% of respondents reported satisfactory access for most patients (41/68). Within the group that reported unsatisfactory access, the majority (15/68) attributed this to both limited supply and insurance coverage. A minority of respondents (38%; 26/68) reported satisfactory access to neuropsychologists, citing issues with both limited supply and insurance coverage. Similarly, a small group (15%) reported satisfactory access to mental health providers for therapeutic services, with both limited supply and insurance coverage cited as barriers.
Respondents were asked to select outcome measures that they currently used as well as their opinion on ideal outcome measures to use. The most commonly used outcome measures (participants were able to select multiple) were family satisfaction (100%; 61/61), followed by school attendance (75%; 46/61), informally measured quality of life (72%; 44/61), academic achievement (52%; 32/61) and neuropsychological testing (44%; 27/61). Ideal outcome measures (participants were asked to select one) included satisfaction (33%; 20/61), formal assessment of quality of life (26%; 16/61), neuropsychological testing (15%; 9/61), attendance (8%; 5/61), informal quality of life (7%; 4/61), academic achievement (5%; 3/61), and other (5%; 3/61 participants selected this, declining to choose one metric).
Discussion
This study aimed to characterize the attitudes, practices, and experiences of specialty physicians with the return-to-school process for children hospitalized for ABI. Eighty-four pediatric specialists, identified by convenience sampling of providers who cared for children with ABI, responded to an electronic survey. Respondents were first asked if school re-entry was a part of physician-led medical care. The vast majority (90%) of specialty physicians who responded to this survey did ask about the return to school, but only about one-third made recommendations for a school re-entry plan. Regarding who should make the plan for school re-entry, nearly half (49%) responded that a school liaison (assumed for the purposes of this survey to be a medical staff member) should make the plan.
Strikingly, the biggest challenge for school re-entry perceived by specialty physicians was cognitive difficulties, which was a much more common response than behavioral or physical challenges. This is similar to reported family perspectives about needs after TBI [13]. As far as identifying gaps in cognitive rehabilitation (a term used exclusively in the medical setting), respondents identified three primary issues. First, availability of medical school liaisons (educators employed in the medical setting to communicate with schools) was a challenge for nearly half of clinicians (47%). Given limited time in medical appointments as well as limited physician knowledge about school accommodations and vocabulary to make recommendations, this is an important barrier. Second, clinicians perceived an inability on the part of the school to implement a reasonable support plan. This is not to suggest that the schools were falling short and not following IDEA guidelines, but rather indicates that physicians perceived that schools might provide more or different services. This may not be an issue with the school; it may be a misperception on the part of clinicians, recognizing that that the qualifications and roles of special education are an area of relative weakness for physicians [19]. Third, clinicians noted the lack of an evidence-based cognitive rehabilitation curriculum. It is important to note that the activities associated with the term “rehabilitation” are a task for the medical environment and may not be an appropriate curricular expectation. Clinicians also noted limited access to neuropsychologists and mental health providers in the community as barriers to school re-entry. These services are, again, not directly provided by schools, but were pertinent barriers for the clinician.
In the medical setting, emerging protocols for cognitive rehabilitation [21] are not yet broadly available. While there will never be a “one size fits all” curriculum, there are no quality standards or checklists widely in use [22]. Cognitive rehabilitation is currently provided by a limited and heterogenous patchwork of providers that varies by location across the country and can include neuropsychologists, speech therapists, occupational therapists, and educational therapists [23]. This survey highlighted a perceived shortage of therapists by specialty physicians, particularly within neuropsychology and speech therapy. Patients may have access to additional community or school resources, but physicians may not have the training, language, confidence, or time to ask about these resources within the constraints of their medical encounter. Prior studies have suggested a shortage of therapists to assist with cognitive rehabilitation in the medical and school settings [13, 24]. Limited guidelines for cognitive rehabilitation lead to wide variations in practice [25].
This study also aimed to identify the primary outcome measures of importance for specialty physicians in measuring the success of the return to school. For their current practice, physicians were allowed to select multiple measures, but for the “ideal state,” respondents were asked to select one “best” answer. Family satisfaction, both in the current and ideal state, was the most common response. Notably, formal quality of life measures were not typically used in the current state but were the second most popular response in the ideal state. A very small number of physicians chose “academic achievement,” arguably a key outcome measure for educational systems, as the ideal outcome measure. This may be due to physicians expecting a slower degree of academic progress if there are new deficits present, but it further serves to emphasize divergent priorities in the medical and school systems after brain injury.
Gaps in outcome tracking in the medical setting likely perpetuate cycles of unknowns and heterogenous treatments. There are recommendations for common data elements for pediatric TBI research [26]; however, these are not universally implemented, making comparisons across studies more difficult. The American Academy of Neurology and the Child Neurology Society Quality Measurement Set notes that the “lack of implementation of screening guidelines into clinical practice . . . results in a gap in high quality care” [27]. Facilitators of uptake for outcome measures among clinicians include known validity and reliability, outcome measures learned in professional training, and recommendations in clinical practice guidelines [28]. Barriers include lack of time, relying on judgement for clinical decisions, and unavailability of assessment tools [28]. Lack of key stakeholder engagement in the creation of outcome measures has also been cited as an important barrier to adaptation [29]. iPad-based surveys have been utilized to collect patient-reported outcome measures (PROMs) in adult neurology patients, but participating patients were notably more often privately insured and more likely to report English as their preferred language compared to nonparticipating patients [30]. Barriers to outcomes tracking from both the patient and clinician perspective need to be better understood to monitor and manage outcomes.
Limitations of this study included a low response rate, comparable to other studies using unpaid surveys [31]. The survey format and layout posed limitations; providing set responses to improve standardization provides less flexibility in responses and may even influence responses. For brevity, the survey instrument did not define all query terms, (e.g., liaison, plan); this may have led to misunderstanding about the intent of the questions. Investigators attempted to mitigate survey-related miscommunication by pre-testing 15 physicians and refining the text based on their feedback. Time to complete the survey was also a burden (an average of 24.5 minutes was recorded as the survey open time), which may have contributed to incomplete responses including demographics, which were included at the end of the survey while participants may have opted to terminate the survey early.
The knowledge base of specialty physicians regarding the special education process was not addressed in this survey. This poses a real limitation for interpretation of a survey of a multifaceted collaborative process. Physicians may have unrealistic or misguided perceptions about what the school system can and cannot offer, and how to navigate the special education process has been reported as a relative weakness for pediatricians [19]. It was assumed that this knowledge gap was similar for most specialty clinicians, with formal education about the IEP process not typically provided for physicians. However, specialty physicians may have more experience in this area by necessity of their practice, but respondents’ factual knowledge about the IEP process was not assessed, which is a weakness of this study.
In addition, utilization of a convenience sample of respondents decreased the generalizability of the results. Based on the distribution plan, the survey was sent to an estimated 180 neurologists and 360 physiatrists, with a higher response rate among neurologists. This may have been due to the method of contact, with neurologists being primarily contacted by personal email and physiatrists being contacted primarily via listserv. Participants who completed the survey may have been more interested in the issue of the return-to-school process, skewing the results towards practitioners who were more engaged in this topic. Of note, an even distribution of experience was represented, but subgroups were too small to allow for meaningful comparisons. Given that 81% of respondents reported working in the academic setting (inpatient or outpatient), this study is more reflective of that population of practitioners. The study was based on practitioner perceptions rather than services delivered and denied, but these findings align well with prior studies documenting gaps in care [13, 14].
New strategies must be employed to meet the cognitive needs of patients living with ABI. While family satisfaction may be a complementary meaningful outcome choice, until the medical system tracks objective, reproducible outcomes, it will be more difficult to determine how to improve the process across institutions, and the current under-resourced and fragmented system is likely to persist. Given the relative knowledge gap about special education for clinicians, translation of medical observations for educational use via a medical staff member with educational training (such as a medical school liaison) is a reasonable recommendation. However, in a cost-conscious medical environment, this study found that many clinicians did not have access to these services. Understanding the impact of educational liaisons on medical-school communication, physician and family satisfaction, as well as downstream outcomes important to physicians and schools alike is a critical step for future studies.
Footnotes
Acknowledgments
BJK would like to thank Megumi Okumura for providing valuable survey input. Naya Fullerton assisted with the creation of the tables and ![]() . The authors would like to thank the International Pediatric Stroke Organization, the Child Neurology Society, and their members for consideration of this survey and their time to provide input.
. The authors would like to thank the International Pediatric Stroke Organization, the Child Neurology Society, and their members for consideration of this survey and their time to provide input.
Author contributions
The study was conceived of and designed by BJK, JMT, NE, and KC. The survey was created by BJK, JMT, NE, and KC. Data analysis and visualization was performed by BJK. The manuscript was written by BJK, JMT, and NE. The authors have no conflicts of interest or funding to report.