
Abstract
PURPOSE:
To explore the existing literature on non-pharmacological and non-surgical pain management in children and adolescents with cerebral palsy (CP).
METHODS:
Databases (Cochrane Library, PubMed MEDLINE, Ovid Embase, and PsycINFO) were systematically searched to identify literature on non-pharmacological and non-surgical interventions for relieving pain in children with CP or similar conditions.
RESULTS:
Thirteen publications met the inclusion criteria. Based on study designs, the overall level of evidence of the included studies was low, justifying the use of a scoping review. Only three were randomized controlled trials. Pain reduction was reported in 8 of the 13 studies from following interventions: physiotherapy/rehabilitation, massage, cranial osteopathy, swimming and aquatics, and assistive devices. These complementary strategies should not omit conventional treatment, and a multidisciplinary approach using multifaceted treatment of pharmacological and non-pharmacological therapy is recommended to increase the pain-relieving effect.
CONCLUSION:
The results indicate that physiotherapy, massage, swimming exercise, and various assistive devices can have pain-relieving effects. We found limited evidence on the topic of non-pharmacological and non-surgical treatment of pain in children with CP. Due to the lack of power in the included studies, no true evidence-based recommendations can be made from the collected articles; thus, further studies with larger cohorts and more power are needed to substantiate evidence-based treatment of pain in children and adolescents with CP.
Abbreviations
Cerebral palsy Gross Motor Function Classification System Botulinum neurotoxin A Randomized controlled trial Quality of life The Training and Support Program Adapted sports Activities of daily living
What this paper adds
Treatment of chronic pain in children with CP should be multidisciplinary. Physiotherapy, massage, swimming exercise, and various assistive devices can have pain-relieving effects. There is limited evidence for non-pharmacological and non-surgical pain-relieving strategies in children with CP.
Introduction
Cerebral palsy (CP) is a non-progressive neurologic disturbance caused by damage to the immature brain in pregnancy or up to two years of age. The incidence is around 2.1 per 1,000 births [1] with a large prevalence of prenatal causes [2]. The diagnosis entails physical and potentially cognitive impairments, which vary from mild to severe.
Spasticity is considered to be the most common feature associated with CP, but an overlooked clinical issue is pain. A majority of children with CP suffer from chronic daily pain, which is the most commonly reported physical comorbidity of CP and is usually related to dystonia and muscle spasticity [1, 4]. Despite this, pain is one of the least understood and studied physical comorbidities of CP [4].
Recurrent musculoskeletal pain has been reported in 62% of children with CP [3, 6]. Eriksson et al. (2020) found in their registry study of 3,545 children a correlation between presence of pain and low gross motor function, measured by the Gross Motor Function Classification System (GMFCS) [7]. The GMFCS is divided into five levels; level I describes the highest level of functional ability and level V the lowest. The study found that children and adolescents in GMFCS III and V were more likely to report pain than those in GMFCS I. However, this correlation has not been consistent throughout other, albeit smaller, studies [8]. Eriksson et al. also found an almost linear progression of incidence of pain by age. The proportion of children with pain increased from 32.8% at age 4-5 years to 57.3% at age eighteen [7].
Most children with CP undergo different interventions, including surgeries, intra-muscular botulinum neurotoxin A (BoNT-A) injections and rehabilitation (i.e., physiotherapy) to relieve spasticity, gain better function, and relieve pain [9]. Though the intention is to alleviate pain, these interventions can cause procedure-related pain [4]. Previous studies have shown that almost 1:2 children with CP experience pain during therapy such as physiotherapy [8].
Little is known about the evidence of the management of chronic pain in children and adolescents with CP. A systematic review was recently conducted on pharmacological and surgical pain management. The authors looked at the management of pain in children and adolescents with CP and the efficacy of interventions such as different surgical procedures, BoNT-A injections, intrathecal baclofen therapy, oral and inhaled drug therapies, and analgesic injections. Besides pharmacological and surgical treatment, non-pharmacological methods have been suggested as a solution to manage chronic pain. This includes physiotherapy, massage, environmental adjustments, and occupational therapy [10, 11]. The systematic review also looked at different non-pharmacological interventions to relieve procedural pain including massage, clown care therapy, physiotherapy, and virtual reality. However, they find that all therapies are scientifically unsubstantiated, and higher quality evidence on pain management in children and adolescents with CP is needed [12].
Furthermore, there is an overall recommendation towards a multidisciplinary approach in the treatment of chronic pain in children with CP [10, 12]. Many families of children with CP also seek out complementary therapy for pain management outside of their prescribed therapy; these can include cranial osteopathy, acupuncture, yoga, and massage. But the families express a lack of information about the possible effects and benefits of complementary therapy as well as concerns about their child receiving a non-evidence-based treatment [13]. This uncharted topic is immensely important due to the high prevalence of recurring or chronic pain in children and adolescents with CP. To the authors’ knowledge, there is no existing review on non-pharmacological and non-surgical management of chronic pain in children with CP, and it is important to assemble the evidence to be able to perform a multidisciplinary approach in pain management. This scoping review provides an overview of the existing literature on non-pharmacological and non-surgical strategies to relieve chronic pain in children and adolescents with CP, and also identifies gaps in the knowledge on the topic.
Methods
The research question
Based on the existing literature, what is the scope of knowledge of non-pharmacological and non-surgical treatment of pain in children and adolescents with CP?
Search strategy
This scoping review was conducted according to the PRISMA(-ScR) guidelines and based on a systematic search of existing literature [14]. Contrary to a systematic review, a scoping review has a broader approach and aims to map the key concepts of a broader research question. Furthermore, scoping reviews are used to identify gaps in the research knowledge base [15]. According to Munn et al. (2018), scoping reviews can aim to identify the types of available evidence in the given field [16], which is the primary focus in this paper.
A protocol has been registered on OSF prior to submission of the final paper and is assessable at https://osf.io/xp52n.
To identify relevant literature, a search was conducted in PubMed MEDLINE, Ovid Embase and Cochrane Library from earliest existing literature to July 2019. Later in the process, the database PsycINFO was included and searched up to January 2020, with the same search string as the other databases. MeSH terms and Emtrees were explored to expand the search, and both MeSH terms and Text Words/Keywords were searched to include articles that are not yet indexed. More details on the search strategies within each database are presented in the search protocol in Table 1.
Search protocol
Search protocol
Two authors (NF, JSM) independently screened titles and abstracts for eligibility. When discrepancy occurred, the selection was discussed and, if necessary, a third reviewer was consulted (CW). If eligibility was still unclear, it was included in the first screening. Full-texts of the literature were then obtained and another screening for eligibility was conducted. If any discrepancy occurred in the full-text evaluation, a third reviewer was again conferred. Lastly, a chain search was done to identify relevant articles through reference lists.
The inclusion criteria were as follows: Subjects being 0–18 years of age Subjects with the diagnosis of CP or other chronic brain damage Subjects with experience of chronic pain Inclusion of a non-pharmacological intervention for the management of chronic pain Systematic reviews, scoping reviews, meta-analysis, randomized controlled trials (RCTs), interventional studies, cohort studies, case-control studies, case reports/series or qualitative interviews English, Danish, Norwegian or Swedish language articles Full-text articles
Even though the main focus was children with CP, the search was expanded to include all evidence on children with any chronic brain damage with the same symptomatology as CP.
The exclusion criteria were as follows: Adult participants Studies on acute pain Studies on headache and migraine Studies on post-surgical pain or procedural pain Studies on surgical interventions Languages other than English, Danish, Norwegian, or Swedish No full-text available
Synthesis of results
The included studies are presented narratively in this paper, incorporating a qualitative analysis and a few quantitative results. The qualitative presentation of the data is grouped in various types of interventions, which are analyzed or commented on in each study included. Additionally, tables and forms present the findings for a more convenient overview. The following information was recorded for each study included: author, year of publication, database of availability of the study, title, aim, intervention or pain management characteristics, study design, sample size and population age, safety of the interventions, duration of effects, and results and/or conclusion on the efficacy of pain management (cf. Table 4). The grouping of interventions is defined in Table 2, and study design with number of studies is presented in Table 3.
Characteristics of studies included
Characteristics of studies included
*N/A = not applicable.
Interventions grouped in subheadings
*N/A = not applicable.
Study design of included studies
A decision tree is illustrated in Fig. 1 to guide practitioners in non-pharmacological management of pain in children with CP. It is based on the evidence found in this article and includes quality of evidence, based upon study design.
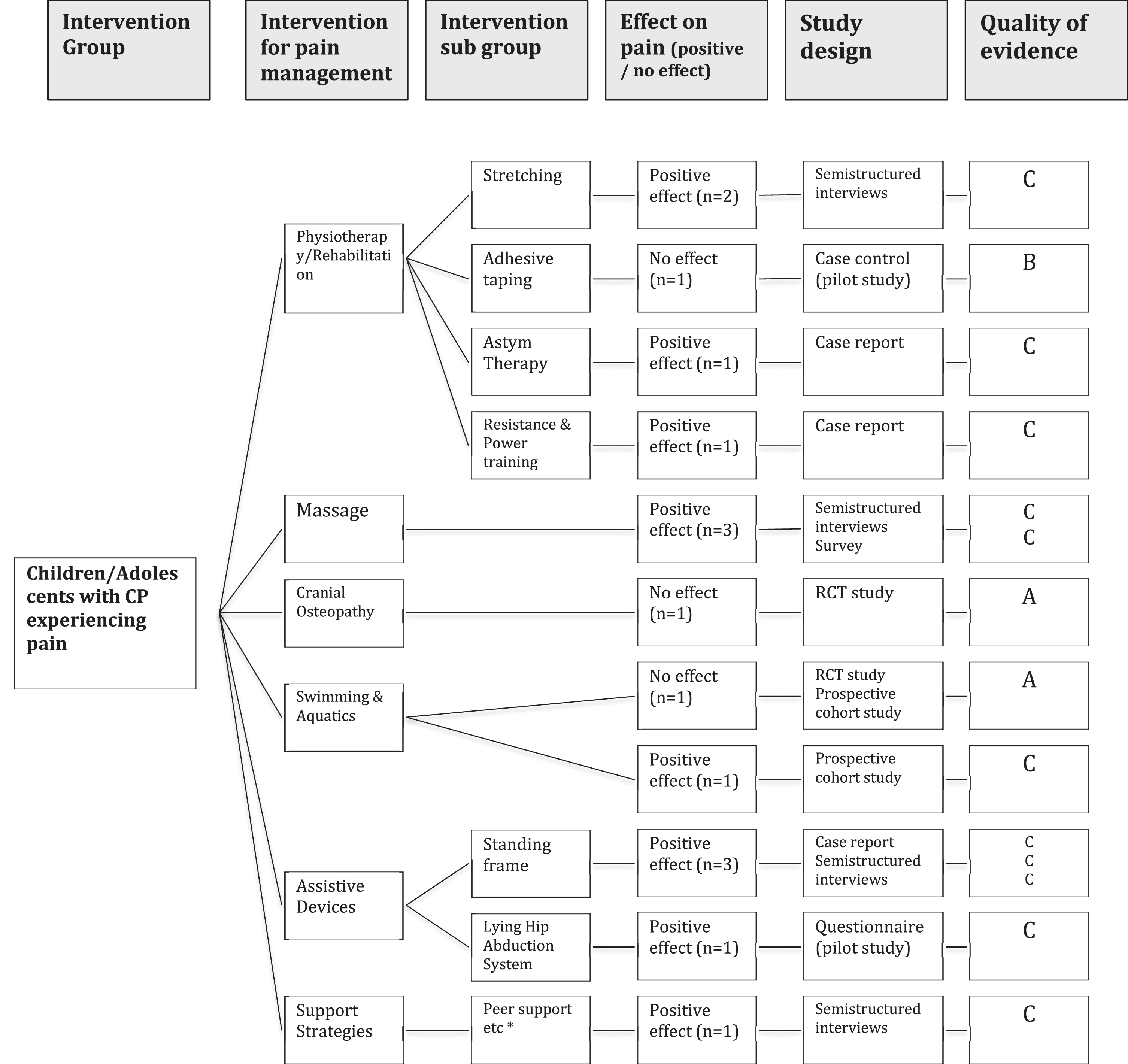
Decision Tree. Decision tree to guide practitioners in non-pharmacological management of pain in children with CP. Based on the evidence found in this article. Includes quality of evidence, based upon study design. n = x, meaning number of studies. * Peer support / Adaption of daily schedule / Multidisciplinary communication / Distraction / Emotional support.
Generally, all included studies had pain relief as a secondary outcome and were primarily focusing on motor function, deformities, or quality of life (QoL). For each article included in this scoping review, only sections concerning pain management have been reviewed. Pain management was the focus, and any other findings of management efficacy (e.g., mobility, gross motor function, school attendance, etc.) were excluded. QoL evaluations were included if the study specified a pain assessment within the evaluation.
The level of evidence, quality of the studies included, and risk of bias were not appraised, since this is generally omitted in this type of review [14]. Moreover, this review does not aim to conclude on recommendations towards non-pharmacological pain relief in children with CP, but rather aims to provide an overview of the existing knowledge.
Selection of data sources
Through the electronic database search, 1,820 articles were identified, which was reduced to 1,340 articles after deduplication. Of these, 93 abstracts met the inclusion criteria. After full-text assessment, another 80 articles were excluded. One study that met the inclusion criteria was later excluded as it was simply evaluating another study, which was already included [17]. Chain searching and screening of reference lists did not add to the final collection of publications. Ultimately, 13 articles met the inclusion criteria after full-text analysis. Of the 13 included articles, only two were RCTs (cf. Table 3).
The eligibility process is demonstrated as a flow diagram in Fig. 2.
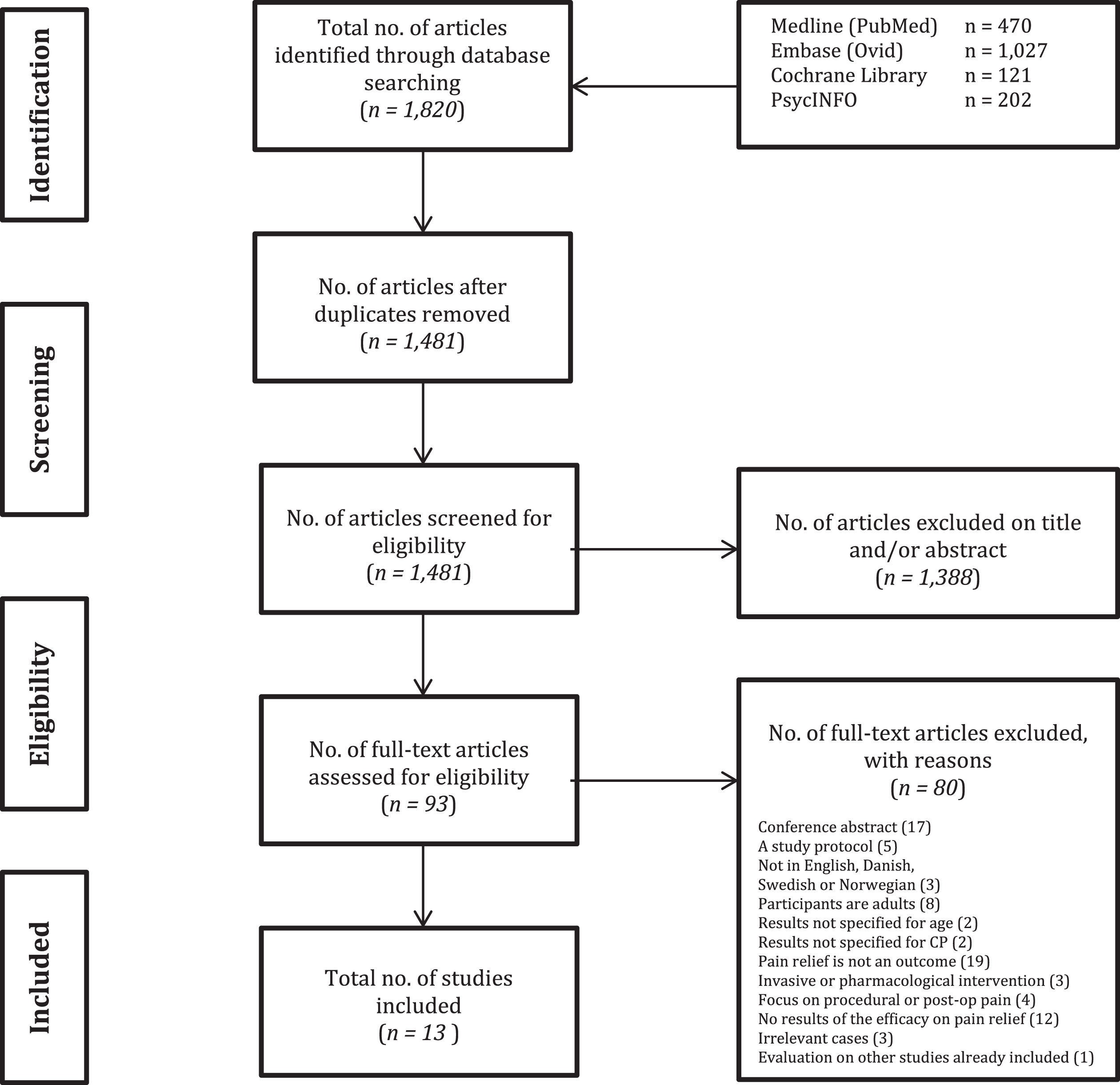
Flow diagram of the eligibility process.
The sources of evidence have been grouped into six subheadings as shown in Table 2, and the number of studies under each subheading varies from one to four per intervention. Characteristics of the included studies are described in Table 4 and quality of evidence is evaluated in Fig. 1.
Physiotherapy/rehabilitation
Brunton et al. (2013) conducted a report on semi-structured interviews of 10 adolescents and young adults with CP in order to describe the bodily experience of CP and the management of pain and fatigue. The study was included because two of the participants were younger than 19 years (aged 15 and 16 years). The participants reported that the use of stretching, rest, a good night’s sleep, avoiding painful activities, finding different methods of mobility than usual, and swimming were good pain-relieving strategies [18].
Another physiotherapeutic management tool is adhesive taping, which has elastic properties that allow movement of the body and soft tissue while protecting and supporting the joints [19]. In a pilot study, Ghalwash et al. (2012) investigated the effect of adhesive taping for controlling genu recurvatum and pain reduction in children with diplegic CP. Fourteen children (mean age 6.22 years) were randomized into two groups; one group received adhesive taping and one group received a knee cage, which is a knee orthosis that permits free knee flexion but controls degree of extension and prevents hyperextension. Both groups received physiotherapy in a 12-week program. The study found no statistically-significant effect of adhesive taping in controlling genu recurvatum and reducing pain [19].
Scheer et al. (2016) described the use of Astym® therapy to improve hamstring flexibility and Achilles tendinopathy in a case report on an eight-year-old child with CP. Astym® is a non-invasive soft tissue stimulation tool that addresses soft tissue dysfunction by using a handheld topical instrument. The child underwent eleven Astym® sessions including physiotherapy treatments (stretching and physical exercise). The study found improvements in muscle tone and flexibility as well as decreased pain when standing and walking [20].
Another prospective single-subject case report by Gannotti et al. (2015) described the long-term health benefits of a speed, resistance, and power-training program performed while seated. The case report was based on a young adult with CP who had followed the training program from age 14.5 to age 20. The program was individualized and tailored to the participant. The workout was comprised of various boxing activities such as flexibility exercises, punching with focus mitts, and strength and power training with increasing repetitions. Initially, the program was once a week for 1.5–2 hours but progressed after two years to 3–5 times per week. After one year, the adolescent already reported improvement of lower back pain as a result of the training exercise [21].
Two of the abovementioned studies are case reports, and generalization of the results is inexpedient. As for any other single-subject study, future research including more subjects should verify the results of Astym® therapy and resistance and power-training.
Massage
Powell et al. (2009) reported on the efficacy of a specific Training and Support Programme (TSP) involving massage provided by the parents to their children. Forty-three children between 4-18 years of age participated. The efficacy was analyzed through semi-structured interviews with children with CP, providing qualitative data on the children’s perception of the TSP. The study found improvements in the children’s health as a result of massage, including reduced pain, muscle relaxation, and improved mobility and bowel movements. One child reported beneficial aspects of the TSP as, “Pain, it helps with my pain sometimes” [22]. Since the study was based upon interviews, no statistical analysis was performed.
Another survey was conducted by Glew et al. (2010) to determine the use of massage among children with CP and the reasons for its use. One hundred families with a child with CP between the ages of 17 months and 21 years were included. From the questionnaires, they concluded that 51% of the surveyed children were receiving massages at the time the survey was conducted. Thirty percent of the parents who sought and used massage believed that it decreased pain for their child [23]. In general, massage therapy might have a pain-relieving effect.
Cranial osteopathy
Cranial osteopathy covers a group of techniques that release tension by palpating bones throughout the whole body, using very little force and a gentle pressure [24]. Wyatt et al. (2011) conducted an RCT study estimating the effects of cranial osteopathy on physical function and general wellbeing in children with CP aged 5–12 years. One hundred and forty-two participants were randomised to either six sessions of cranial osteopathy with a registered osteopath or a waiting list. Primary outcome measures included Gross Motor Function Measure (GMFM-66) and Quality of Life Child Health Questionnaire (CHQ-PF50). Parental assessments of pain and sleep diaries completed before and after six months of intervention were included as secondary outcome measures. According to the authors, cranial osteopathy and massage are some of the most-used complementary therapies in the population. The study found no significant differences between the intervention group and control group in general nor with respect to pain. In conclusion, there was no evidence that cranial osteopathy leads to sustained improvement in motor function or pain [24].
Swimming and aquatics
Physical activity and exercise have been found to be beneficial for the prevention of pain and improvement of gross motor function as well as increasing QoL [25–28]. Swimming and aquatics are low-impact forms of exercise; hence they are thought to be beneficial to children and adolescents with movement limitations and difficulty with land-based physical activity. Due to neurologic impairments and physical disabilities, children with CP can have limited ability to perform physical activities and sports [27]. In an RCT study, Declerck et al. (2016) investigated specific benefits of a swimming intervention for young people with CP [27]. Fourteen children and adolescents with CP, aged 7–17 years, were randomly assigned to either a swimming or a control group. Pain was assessed with the Visual Analogue Scale and the revised Faces Pain Scale. The study found no significant changes in the sensation of pain over time when comparing the groups or within the groups [27]. The authors find it notable that the children did not experience increased levels of pain, since exercise often leads to pain and the population is therefore associated with a higher chance of inactivity. Even though this is an RCT study, it is under-powered by the low number of participants in the trial. With more participants, the study would gain more evidential power and might change the outcome.
Feitosa et al. (2017) assessed the effect of adapted sports (AS) on QoL, including a pain domain, in adolescents with CP [28]. AS was defined as swimming and/or soccer. QoL was assessed by the Pediatric Outcome Data Collection Instrument (PODCI), which assesses pain and comfort in one of its six domains [29]. Seventeen adolescents with CP aged 6–18 years were included. A separate analysis on the effects of the two modalities of AS was not possible from the reported results, and consequently the effects of swimming alone cannot be extracted. The study found a beneficial effect of AS on QoL, which also included a pain and comfort subdomain [28]. A subdomain analysis did not show significant improvements in the pain and comfort domain alone, but did reveal that children with diplegia had a better effect in this domain than children with hemiplegia.
Assistive devices
Rivi et al. (2014) conducted a case study assessing the effectiveness of the standing frame, a tool for postural support. Pain due to constipation was assessed as a secondary outcome. One child (five years of age with CP) was chosen to use a standing frame for eight weeks in total. Comparison was done with an initial assessment during a two-week baseline phase before the standing frame was introduced. The study found a notable reduction in pain caused by constipation and stool evacuation. During the baseline phase, the principal caregiver reported four episodes of pain due to constipation or evacuation (28%), whereas in the three weeks of intervention phase, no experience of pain related to constipation or evacuation was reported [30]. As the study’s authors argued, future single-subject research should verify these results by including more subjects.
Goodwin et al. (2018) interviewed 12 children with CP aged 8–18 years to explore the effects of standing frames as an assistive tool on postural management. The study qualitatively reported benefits of the standing frame regarding pain relief, e.g., “I know that if I sat in here 24 hours a day, seven days a week I would get quite tight and I would get probably a lot more pain than I do if I wasn’t in the standing frame.” [31] However, they also reported that the use of the assistive tool could cause pain and discomfort, especially if the child is not well positioned in the device or has other painful musculoskeletal complications that are worsened by standing [31].
Hankinson et al. (2002) investigated the use of a lying hip abduction system (Jenx Dreama®) and its influence on hip stability, sleep, and ease of positioning in a pilot study consisting of seven children with CP aged 4–14 years. The lying hip abduction system consists of a modular mattress altered for individual needs. The device incorporates padded supports to maintain correct positioning of the trunk, hips, and legs. Results on pain relief, sleep, and ease of positioning were obtained through a parental questionnaire given at the end of the baseline and intervention periods. The authors reported a significant pain reduction during daily dressing and hygiene procedures with a mean change in score of –0.6 on a 5-Point Likert Scale after one year [32].
Mixed
Through semi-structured interviews, Nilsson et al. (2016) explored how professionals in a South African school setting responded and reacted to a child with CP in need of pain management. Schoolteachers and professionals were divided into focus groups, giving statements on the topic and answering specific questions such as, “How would you react when a child with CP is in pain?” and, “Which other strategies have you tried to manage pain in children with CP?” The report provided no quantitative results on the efficacy of the interventions mentioned, but the descriptive statements of the schoolteachers’ management of a child’s pain were subcategorized into three main categories (environmental, treatment, and support strategies). They reported that assistive devices such as pillows, standing frames, and adapted chairs and wheelchairs were helpful for the child’s functioning. Other useful environmental modalities were peer support, adaption of a daily schedule, collaboration with parents, and communication between therapists and educators to improve pain management. The discussed non-pharmacological treatment strategies with positive effects were stretching and repositioning, massage, and warm baths –all assessed qualitatively. Effective support strategies included distraction from the pain, emotional support, external health care support, and professional team collaboration. They concluded that a multidisciplinary approach is important in the treatment of chronic pain [33].
Discussion
This study confirms the initial presumption that there is a lack of substantial evidence on the topic of non-pharmacological pain management for children with CP. Though the research demonstrates an overall positive effect of various non-pharmacological pain-relieving interventions (8 out of 13 papers), the quality of evidence and power of the research is low. Table 4 summarizes all included studies and their findings regarding pain relief. Assistive devices (standing frames and the lying hip abduction system) have showed benefits in reducing pain [30–32, 34]. Positive effects on pain were seen in 3 out of 4 studies related to physiotherapy [18, 21]. Two studies, based on interviews, found massage therapy beneficial to pain [22, 23]. The interventions have not been tested systematically or in a controlled trial, which is advisable for further research.
Four studies failed to find any pain-relieving effect from their interventions, which entailed cranial osteopathy, adhesive taping, and swimming [19, 27]. Two studies did not quantitatively evaluate the efficacy of the interventions but merely described different interventions used by children with CP or caregivers to manage pain [18, 33]. In conclusion, these beneficial findings need further evaluation and more powerful research to substantiate the evidence.
A pain-relieving effect of physiotherapy during childhood was found, which also seems to be effective in adulthood. A retrospective survey by Jahnsen et al. (2003) was found through the systematic search, but was initially excluded because participants were adults. However, the adult participants elaborated on their experiences during childhood, namely that as children they participated in regular and frequent physical therapy sessions with positive effects on pain. This should ideally continue into adulthood, as the most common motivation of the participants for continuing with physiotherapy was pain relief [35]. Fowler et al. (2007) also commented on the importance of physical fitness to prevent chronic pain. They suggested that a lack of physical fitness might contribute to secondary conditions such as pain [36]. This is confirmed by Swiggum et al. (2010) in their literature review on implications for pediatric physical therapy. They encourage implementation of regular exercise routines early in childhood, as this might lead to pain-reducing exercise habits later in life. They suggested that families should encourage their child to be regularly physically active despite the pain [37]. The results of this review indicate that physiotherapy is beneficial as a pain reducing treatment, though it is notable that physiotherapy itself, and especially stretching when performed, has been associated with intense and frequent pain in children with CP [38].
Ninety-three articles have been assessed for eligibility for this paper, and more than 80% of these were excluded for various reasons (see Table S1, appendix). A common reason for exclusion was that pain relief was not included as an outcome; thus, there were no results regarding efficacy on pain reduction for the explored intervention.
A larger variety of interventions was anticipated. Acupuncture is known to be effective for the treatment of chronic pain in general [39], but no literature was found matching the inclusion criteria on acupuncture as a pain management tool in children with CP. Yang et al. (2015) included four non-Cochrane systematic reviews on children with CP in their overview of the efficacy of acupuncture on activities of daily living (ADL) as a supplement to conventional treatment alone. Pain relief as an outcome was not assessed in any of the studies. Acupuncture used in addition to conventional treatment seems beneficial for children with CP in improving ADL [40], but whether or not it can be beneficial as an analgesic agent in children with CP has yet to be investigated.
Of the included studies, only 2 out of 13 (15.4%) were RCTs and one of them included only fourteen participants, which weakens the power. A large portion (38.5%) of the included studies was based on interviews with qualitative results and outcomes. The lack of substantial evidence on the topic justifies the use of a scoping review instead of a systematic review. The aim was to elucidate the state knowledge on non-pharmacological pain treatment rather than conclude on recommendations on non-pharmacological pain relief in children with CP.
Though pain reduction has been demonstrated through many of the above-described non-pharmacological and non-surgical methods, these interventions are usually insufficient as a single-method therapy and should be combined with oral medications, invasive pain relief such as BoNT-A injections, and surgical interventions.
The causes and sites of pain in children with CP are as individual as the condition itself [4], and the underlying pain mechanisms are not well understood. There is growing evidence for both inflammatory and centralized pain mechanisms [41]. Blackman at al. published a review in 2018 with an overview of the current knowledge of pathophysiology of pain in individuals with CP. Musculoskeletal pain, e.g., dislocated hip joints, is released by primary hyperalgesia from an inflammatory reaction in the joints, producing a sensitization of nociceptors in the tissue. Blackman et al. suggest that the prolonged muscle contractions and sustained abnormal bodily postures can result in an increased primary hyperalgesia and inflammatory sensitization. Further sensitization of the central nervous system may result in persistent and chronic pain [4]. A centralized pain mechanism, and the proposed reason for neuropathic pain, in individuals with CP has been suggested to be a consequence of periventricular leukomalacia (PVL). PVL is an impairment of the white matter in the brain, caused by cerebral asphyxia or other complications in the development of the immature brain during pregnancy, complications during delivery, or disorders to the brain during the first year of life [41]. There is a need to better understand the pathophysiology of pain in CP in order to improve the treatment. With the large variety of pain in this population, the treatment must be tailored to the specific needs of the child, as recommended by Flett et al. (2003) [42]. They underlined the important role of physical therapy, orthoses, assistive devices, stretching, exercise, and mobility enhanced through castings to achieve better success from surgical and pharmacological interventions. Ostojic et al. (2019) reported that a multidisciplinary approach is considered best practice in managing chronic pain in the general pediatric population [12]. One of the studies included in this scoping review recommended a multidisciplinary approach as well [33].
In conclusion, further research on non-pharmacological and non-surgical approaches to reduce chronic pain in children with CP is needed [12, 30]. Particularly, there is a lack of quantitative research with large cohorts and strong scientific designs such as randomized and blinded controlled trials. The Decision Tree in Fig. 1 illustrates which of the interventions included in this study had positive effects on pain and which had no effect. The findings should be assessed with respect to study design and thus quality of evidence. The figure demonstrates that the quality of evidence of the findings mostly consists of strength C. Both RCTs found no effect and, as Table 4 illustrates, one included only fourteen subjects, which can argue against strength A classification of quality of evidence.
Future research should focus on improving the methods and aims for adequate powered studies with increased numbers of included subjects to implement these methods in clinical treatment and aspire to evidence-based multidisciplinary approaches in pain management in children and adolescents with CP.
Study limitations
It was difficult to conduct a systematic review because of the heterogeneity of the research and the low methodological level of evidence on the topic in general, which justifies the use of a scoping review. The risk of publication bias in the included studies has not been taken into account, and therefore potential bias from the original studies may be incorporated in this review. Likewise, the level of evidence in all the articles used in this paper has not been reviewed in depth, and quality assessment was based solely on study design.
Many of the studies included did not have pain evaluation as their primary endpoint. This may weaken the extracted data, but it also emphasizes the general need for evidence on the topic. Moreover, interview-based studies were included. Most of them did not conclude on the efficacy of the treatments, but merely commented on or discussed different approaches. These reports were included because of their value in elucidating the area of knowledge.
The search string is the frame of reference, and the search strategy attempts to cover the full area of knowledge, especially by including multiple synonyms or similar terms to each search word. Other literature databases could have been included to optimize the collection of references.
Potentially, the inclusion and exclusion criteria would introduce limitations to the data collection. The exclusion of languages other than English, Danish, Swedish, and Norwegian restricted the included evidence.
A few studies with adults as participants, e.g. Jahnsen et al. [35], were identified and could possibly have been of interest to the topic and of use in generalizing pain management in people with CP, but these were excluded due to the age criteria.
Conclusion
This scoping review discovered several possible strategies for non-pharmacological and non-surgical management of chronic pain in children with CP. The results indicate that physiotherapy, massage, AS (i.e., swimming exercise), and various assistive devices might have pain-relieving effects. The studies included in this review consist mostly of qualitative interviews and single-subject case reports, which have low quality of evidence. The two RCTs evaluated cranial osteopathy and swimming. These showed no significant effects, and one of the studies was underpowered. Complementary strategies with beneficial effects on pain should not exclude conventional treatment, and a multidisciplinary approach is recommended when treating children with CP and chronic pain.
Due to the lack of power in the included studies, no true evidence-based recommendations can be made from the collected articles. This scoping review must instead be seen as an overview of the existing knowledge and a stepping-stone towards further research. Even though this review does not perform a thoroughly critical appraisal of the studies included, it is clear that further strong investigations are required on the topic of non-pharmacological treatment of pain in children with CP in order to make future recommendations. There is a need for higher quality of evidence, larger cohorts, and longer follow-up periods.
Footnotes
Acknowledgments
The authors have no acknowledgements
Conflict of interest
The authors have no conflict of interest to report.
Ethical considerations
This study, as a literature review, is exempt from Institutional Review Board approval.