
Abstract
PURPOSE:
The aim of this study was to assess serum vitamin D levels and related factors in children with cerebral palsy (CP).
METHODS:
One hundred and nineteen children with CP between the ages of 1 year to 10 years 9 months who were admitted to the children’s inpatient rehabilitation unit of a tertiary rehabilitation hospital between January 1, 2017, and December 31, 2018, were included in this study. Demographic and clinical characteristics were obtained from the patient files. CP types and serum 25 hydroxyvitamin D (25OHD) levels were recorded. Gross Motor Function Classification System (GMFCS) was used to assess the functional level.
RESULTS:
Mean age was 5.1±2.9 years. Forty-two (35.3%) were girls, 105 (88.3%) were spastic, and 14 (11.7%) were ataxic and mixed type CP. Mean GMFCS level was 4 (IQR:2). Thirty-one (26.1%) were getting extra liquid feed while the rest were eating a normal diet. Mean serum 25OHD level was 27.4±15.7 (3–79) ng/mL. Vitamin D levels were normal in 68 children (57.1%), whereas 36 (30.3%) had vitamin D insufficiency and 15 (12.6%) showed vitamin D deficiency. Those whose serum vitamin D levels were within a normal range had a median age of 3.8 (IQR:4.2) years. On the other hand, mean age was 6.4 (4.3) years for those with low vitamin D level (p < 0.0001). Vitamin D level was 19.8 (21.4) ng/mL in those (n = 88) who had regular diets, whereas it was 31.0 [16] ng/mL in those (n = 31) who were getting extra liquid feed (p = 0.015). There was no statistically significant correlation between vitamin D level and gender, GMFCS, CP type, season or antiepileptic drug treatment. A binary logistic regression model showed that older age and having only regular meals were significant risk factors for low vitamin D.
CONCLUSION:
In this study, 42.9% of the children with CP had low vitamin D. Older children with CP or those who had regular diets were higher risk groups in terms of low vitamin D.
Keywords
Introduction
Cerebral palsy (CP), most often caused by injury to the underdeveloped brain in the intrauterine period, is the leading cause of disability in children all over the world [1]. CP leads to activity restriction due to increased tone, dystonic posture and movement difficulties. The incidence is 2–3 per 1000 live births; however, it is more common in premature infants [2].
Comorbidities such as epilepsy, cognitive dysfunction, malnutrition, hearing and visual difficulties, along with gastrointestinal problems are frequently seen in children with CP [3–5]. Dysphagia, gastroesophageal reflux, and constipation are common problems of the digestive system [6]. Recurrent respiratory tract infections may develop because of these digestive problems. Chewing, swallowing, and drooling issues are frequently seen especially in those with spastic quadriplegia [5]. Nutritional problems may be seen in 22% of those with spastic quadriplegic CP [7]. Eating difficulties, nutritional problems, antiepileptic drugs, and limited outdoor activities may lead to vitamin D insufficiency or deficiency [8, 9]. Vitamin D is required for calcium absorption, bone development, and overall bone health in children; therefore, low serum vitamin D levels may lead to rickets, hyperparathyroidism, increased fall risk and decreased bone density [10]. Vitamin D is also important for bone mineralization, and decreased bone mineralization is the main factor in childhood osteoporosis [11]. Low levels of vitamin D also cause reduced intestinal absorption of calcium, which leads to increased parathyroid hormone secretion. Mobility restriction, decreased sunlight exposure, nutritional problems, and some medications in children with CP are factors associated with low bone mass [12–14]. In addition, growth retardation that can be seen can also cause low peak bone mass [13]. In addition, low bone mineral density is a serious problem for bone health [14–16], leading to increased risk of fractures. Fractures adversely affect both physical and social life in children with CP who already have limited mobility [12].
Vitamin D level can easily be screened by measuring serum 25-hydroxyvitamin D (25OHD). However, there are different cut-off values for the definition of vitamin D deficiency and insufficiency worldwide [17, 18]. Institute of Medicine (IOM) Committee accepts 30 ng/ml 25OHD for the cutoff value of parathyroid hormone control and calcium absorption [18]. Moreover, they used the cut off value of 20 ng/ml for the definition of vitamin D deficiency. On the other hand, according to the Global Consensus Recommendations, <12 ng/ml is defined as vitamin D deficiency and values between 12–25 are accepted for insufficiency [17]. Because of these different cutoff values, the results of the studies must be carefully evaluated. Vitamin D deficiency has been defined as the threshold values for sufficient skeletal mineralization and mineral ion equilibrium for the prevention of nutritional ricketts in global consensus report. The cutoff values determined by the Global Consensus Recommendations for strong evidence of nutritional rickets includes defining vitamin D deficiency at values of 25OHD <12 ng/ml. Although vitamin D levels in children with CP are generally lower than those in normal children. There are limited studies investigating them in those with CP [8, 20]. Therefore, the aim of this study was to evaluate serum vitamin D levels and the related factors in children with CP who were admitted to the pediatric rehabilitation unit.
Method
One hundred nineteen Caucasian children between ages of 1 year to 10 years 9 months with CP who were admitted to the inpatient rehabilitation unit of a tertiary rehabilitation hospital between the dates of January 1, 2017, and December 31, 2018, were included in this cross-sectional study. This study was approved by the Ethics Committee of Health Sciences University, Sadi Konuk Training and Research Hospital (No: 2019-07-13). All of them had a CP diagnosis made by a child neurologist. There were no ethnic and racial differences in study population. Exclusion criteria were the regular use of prescribed or non-prescribed Vitamin D supplements in the 6 months before the study and any diseases possibly affecting vitamin D metabolism. Demographic and clinical data were collected from the patient files. Fasting serum vitamin D levels at admission to the rehabilitation unit were measured by electrochemiluminescence immunoassay, and vitamin D status was classified according to the global consensus recommendations.
Serum vitamin D levels <12 ng/mL (30 nmol/L) were considered as vitamin D deficiency. Levels between 12–20 ng/mL were considered as insufficiency. Serum vitamin D > 20 ng/ mL (50 nmol) was considered sufficient [17]. The Gross Motor Function Classification System (GMFCS) was used to determine functional levels. GMFCS is a 5-stage practical test that delineates mobility levels in children with CP and can be used both during clinical practice and research [21]. Children at GMFCS Level 1 can walk independently, run and jump; however, balance, speed, and coordination skills are decreased. In Level 2, children can walk, but walking in crowded places or on rough, uneven surfaces is difficult. They may run or jump up to a certain extent. Children categorized as Level 3 can walk with the help of walking devices and may use wheelchairs for longer distances. At Level 4, it is very hard for children to walk, and they primarily use wheelchairs or power mobility. It is impossible for children to walk or sit independently at Level 5, and they are unable to utilize power mobility.
Statistical analysis
The minimum sample size was calculated by using the rule of thumb for logistic regression models, in which a minimum of 10 outcome events per predictor variable (EPV) is needed. In this study, the number of potential predictors were seven; age, diet, gender, GMFCS, CP type, seasons, and antiepileptic drugs. Thus, the minimum sample size for this study was calculated as 70 cases.
Normal distribution of the data was analyzed by Kolmogorov Smirnov test with Lilliefors Significance Correction and Shapiro-Wilk test. Data having normal distributions were presented as mean±standard deviation (SD); data having non-normal distributions were provided as median and interquartile range (IQR); categorical data were given as frequency and percentage. Normal and low serum vitamin D levels by gender and diet type were compared using Yate’s corrected Chi-square. Normal and low serum vitamin D levels by GMFCS were compared using Pearson Chi-square. The Mann-Whitney U test was used to analyze the statistical difference in the age and GMFCS between subjects with normal and low serum vitamin D levels. Statistical difference in the mean vitamin D between children with normal vitamin D levels and those with low vitamin D was analyzed with the Mann Whitney U test. Statistical difference in the mean of vitamin D levels between girls and boys was analyzed with Mann Whitney U test. Statistical differences in the mean level of vitamin D among GMFCS subgroups were analyzed by Kruskal Wallis. Seasonal differences in the mean level of vitamin D were also analyzed by Kruskal Wallis. Spearman test was used for correlation analysis. Risk factors for low serum vitamin D level were assessed using a (forward-conditional) binary logistic regression model. If a p-value was <0.05, the factor was included in the regression model; however, factors with p-value >0.1 were excluded. The fit of the regression model was analyzed using Hosmer-Lemeshow test. Risk ratio was expressed as Exp (B) (Odds ratio). Significance was set at p level <0.05. Statistical analysis was conducted using PASW Statistics software, version 18.
Results
Forty-two children (35.3%) included in this study were girls, and 77 were boys (64.7%). Fifty-one had spastic quadriplegic CP (42.9%), 48 had spastic diplegic CP (40.3%), 11 had ataxic CP (9.2%), 6 had unilateral spastic CP (5.0%) and 3 had mixed CP (2.5%). Other demographic, clinical, and laboratory data are shown in Table 1. In this study, the mean serum vitamin D level was 27.4±15.7 (3–79) ng/mL. Serum 25OHD level was within normal limits in 68 children (57.1%). Thirty-six (30.3%) had vitamin D insufficiency (12–20 ng/mL), and 15 (12.6%) had vitamin D deficiency (<12 ng/mL).
Demographic, clinical and laboratory characteristics
Demographic, clinical and laboratory characteristics
Those whose serum vitamin D levels were within normal range had a median age of 3.8 (IQR:4.2) years. On the other hand, mean age was 6.4 (IQR:4.3) years for children with low levels of serum vitamin D (p < 0.0001). The mean age of subjects with low serum vitamin D levels, 6.4 (3.9–8.3) years, was significantly higher than that of normal subjects, 3.8 (2.1–6.3) years (p = 0.0001). There was thus an inverse correlation (r = –0.442, p = 0.0001) between age and serum vitamin D level (Fig. 1). Mean serum vitamin D level was 25.5 (25.9) ng/mL for girls, and 25.1 (22.9) ng/mL for boys (p = 0.340).
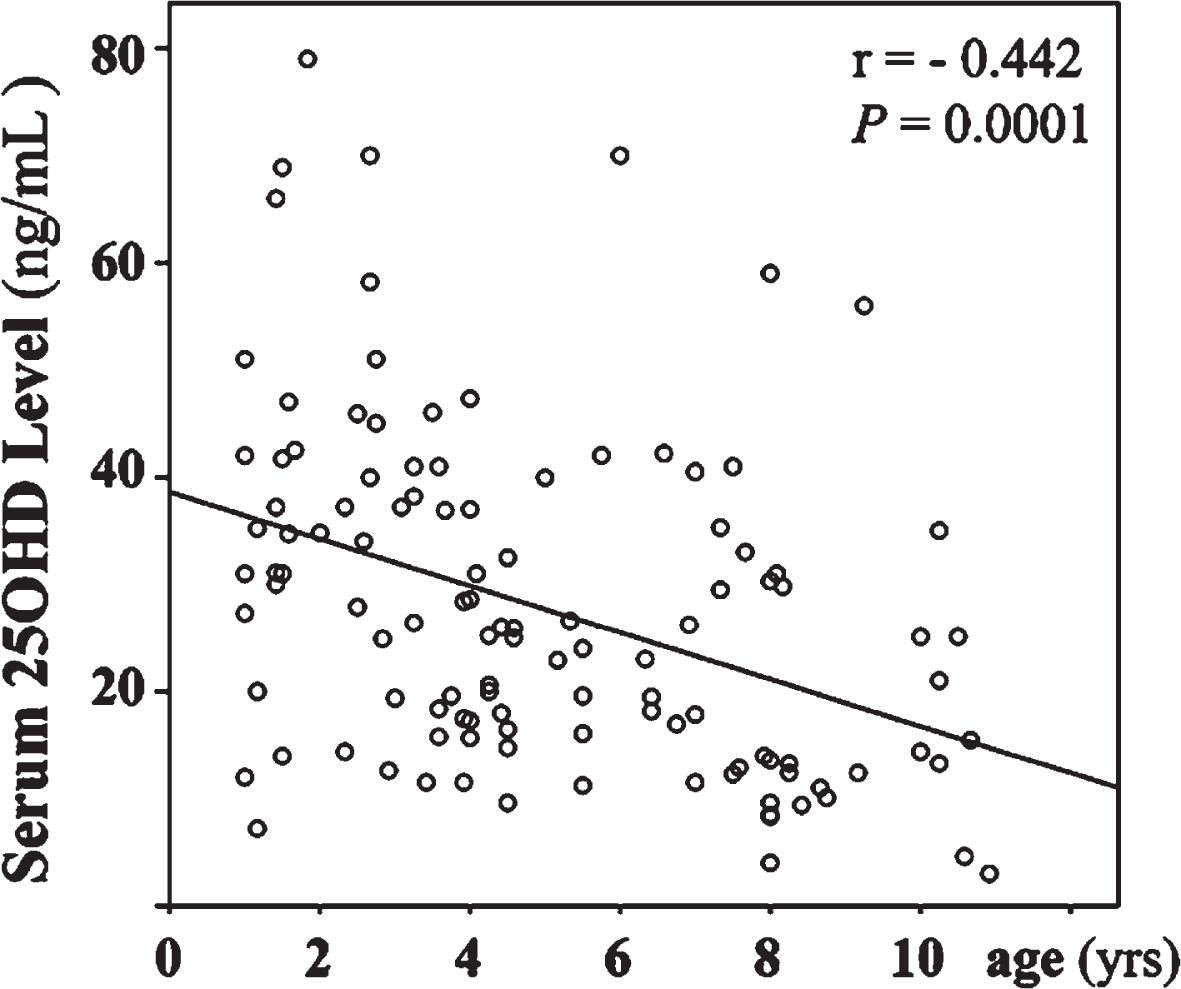
Correlation between age and serum vitamin D level.
Thirty-one (26.1%) were fed balanced liquid feed formulated for those 1 to 10 years, and serum vitamin D level was significantly lower in children who were fed a normal diet than those who got extra liquid feed (Table 4). There were no statistically significant differences in terms of serum phosphorus and calcium between children who were fed a normal diet and those who got extra liquid feed (Table 2).
Comparison of normal and low serum vitamin D levels by gender and diet type
*Yates’s corrected Chi-square test, **Pearson Chi-square test.
Serum vitamin D, phosphorus, and calcium levels in children who had a normal diet and had extra liquid feed
Vitamin D data are given as median (interquartile range), *Mann Whitney U test.
There was no statistically significant difference in serum vitamin D levels for patients categorized in different GMFCS levels (Table 3). Although vitamin D levels tended to be lower during winter and spring, there was no statistically significant difference between seasonal values (p = 0.06, Fig. 2). Age and diet were determined to be predictive risk factors for low serum vitamin D levels by binary logistic regression analysis (Nagelkerke r square 0.239, Hosmer Lemeshow test, p = 0.915, Table 5). This regression model explained 23.9% of low serum vitamin D level and predicts that the odds of hypovitaminosis D is 30% greater with 1-year increase in age. The same model predicts that the odds of hypovitaminosis D is 390% higher in children who are only consuming their usual meals (Table 5). Sex, GMFCS, CP type, seasons, and antiepileptic drugs did not correlate significantly with vitamin D.
Serum vitamin D levels according to the level of motor function
Vitamin D data are given as median (interquartile range), *Kruskal-Wallis test. GMFCS: Gross Motor Function Classification System.
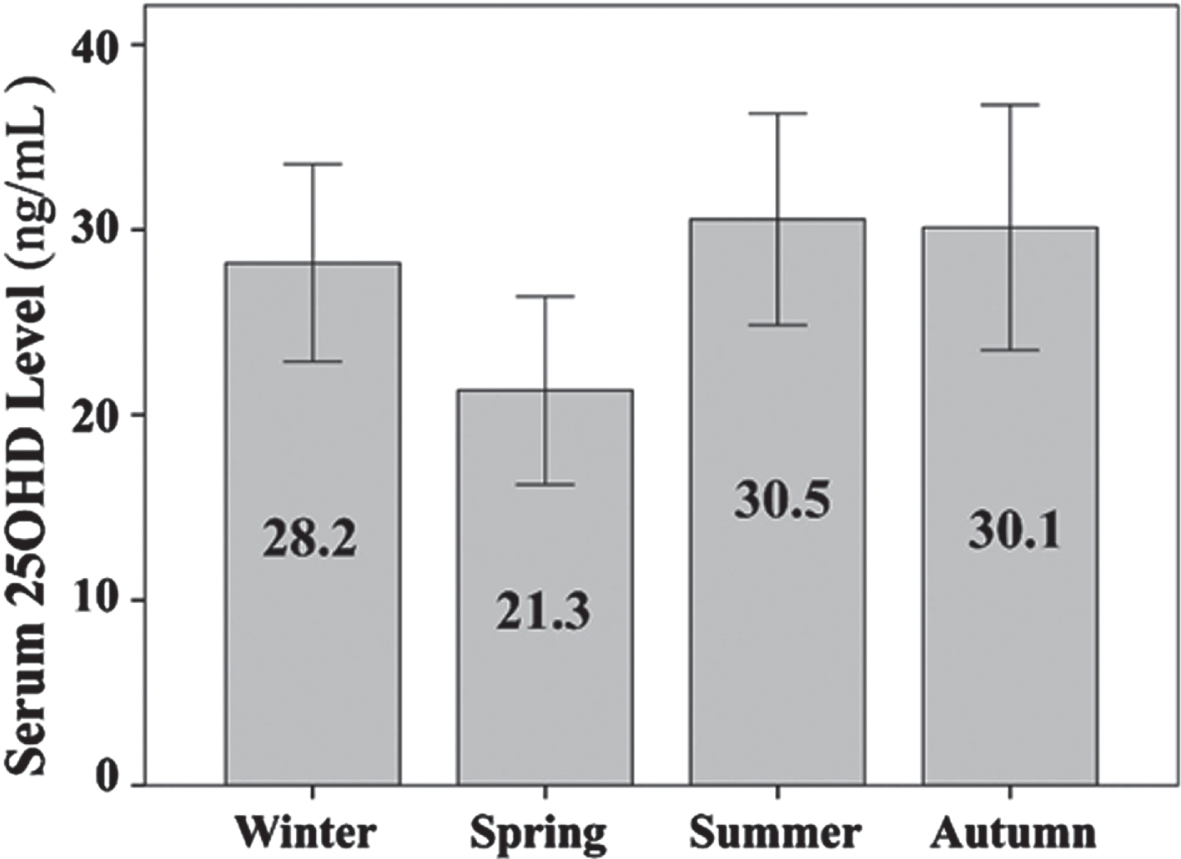
Mean serum vitamin D level according to the seasons (Error bar with 95% CI).
In this study, the mean vitamin D level was 27.4±15.7 (3–79) ng/mL in the children with CP. Median vitamin D level was reported as 35.6 (26.75–64) nmol/L in a group of children with CP between 2–10 years in a previous study [15]. The authors concluded that vitamin D levels were lower than those of the controls. In another study, mean vitamin D levels were reported as 28.03±24.2 ng/ml and 30±1.94 ng/ml in children with CP and in controls, respectively [9].
In this study, 42.9% of the children with CP had either vitamin D insufficiency or deficiency.
Thirty six (30.3%) had vitamin D insufficiency (12–20 ng/mL) and 15 (12.6%) had vitamin D deficiency (<12 ng/mL). In previous studies, vitamin D deficiency (<20 ng/mL) and insufficiency (20–30 ng/mL) rates in those with CP were 26.4–44.6% and 23.1–33.6 %, 61%, respectively (8,9,20). In another study, vitamin D level was reported to be <25 ng/mL in 60% those with CP [19]. Akpinar [20] reported that serum vitamin D level was <30 ng/mL in 60% of those with CP with a mean age of 7.59±6.09 [1–17] years. In the same study, vitamin D insufficiency and deficiency rates were suggested as 33.6% and 26.4, respectively. Moreover, the author suggested that there was severe deficiency in 13.8% of those whose vitamin D levels were <10 ng/mL. A previous study suggested that vitamin D deficiency rates were 44.6% in children with CP [9]. Manohar et al. [8] concluded that vitamin D deficiency and insufficiency rates were 32% and 61%, respectively. Vitamin D deficiency and insufficiency rates were lower in this study, likely because of the lower vitamin D cutoff values for the definition of deficiency and insufficiency according to the newest consensus recommendations.
An interesting finding was that older children with CP as well as those who had only regular meals had a higher risk for low serum vitamin D in this study. However, serum vitamin D level was higher in those who had liquid feed. In this study, 28 (23.5%) had liquid feed which contains various minerals like calcium, phosphorus, magnesium and vitamins (including vitamin D) in addition to protein. More than half of the children with CP had malnutrition [22, 23]. Mostly, swallowing problems were responsible for malnutrition, which may cause growth retardation.
In this study there was not a significant correlation between motor functional status measured with GMFCS and serum vitamin D level in children with CP. Thus, the severity of functional status did not seem to be related to vitamin D level. Those who can walk may be able to spend more time outside their homes and, thus, more sunlight exposure might be expected. However, the children with CP who were able to ambulate had low vitamin D levels in this study.
Moreover, there was not any difference in terms of serum vitamin D levels between sexes in this study. Antiepileptic drug treatment was not correlated with hypovitaminosis D. Vitamin D levels were not related to sex, CP types, mobility status, or use of antiepileptics in a previous study [9]. Moreover, the authors suggested that age was negatively correlated with vitamin D levels. In another study, eating problems, decreased sunlight exposure, antiepileptic drugs, functional status, and CP type were found to be related to low vitamin D levels in the children with CP [8]. Seth et al. concluded that antiepileptic drugs and decreased sunlight exposure were related to low vitamin D levels [19].
Another finding of our study was that when seasons are considered, the lowest vitamin D levels were seen in spring and winter respectively. The highest serum vitamin D levels were measured in fall and summer. On the other hand, there was no statistically significant difference in the level of vitamin D between different seasons (p > 0.05). Previous studies also reported that serum vitamin D levels were low in spring and winter [23, 24].
Since low levels of serum vitamin D appeared to have no association with functional status or seasons, there may be other factors responsible rather than patients’ exposure to sun [24, 25]. Living in a high latitude might be a risk factor for vitamin D deficiency [26–30]. This study was designed at the Istanbul Physical Medicine and Rehabilitation Training and Research Hospital located in Istanbul, northwest of Turkey, latitude 41. Furthermore, vitamin D levels may differ by ethnicity and race [31]. Blacks and Hispanics have lower serum vitamin D concentrations than Caucasians [32]. Therefore, older age and following a normal diet were determined as major risk factors for low vitamin D levels. Previous studies also reported that vitamin D deficiency was seen more frequently in older children [24, 25]. Also, in this study, children who were getting liquid feed showed statistically higher levels of vitamin D. Liquid feed contains calcium and vitamin D as supplements. It is beneficial for children to consume vitamin D fortified milk and dairy products, especially during periods when children cannot get enough sunlight to increase vitamin D levels [33]. A study by Holmlund et al. on children and adolescents with chronic diseases reported that vitamin D levels were higher in subjects that received supplementation [34]. Moreover, vitamin D supplementation was found to be correlated with high serum levels in children with spina bifida [35]. A randomized controlled study by Brett et al. on children between the ages of 2–8 showed that consuming 400IU/day of vitamin D fortified food supplements for six months during fall and winter was effective in increasing serum 25(OH)D3 levels during the first three months [36]. The same study also highlighted that after six months of following this regimen, serum vitamin D levels were not maintained and the intervention was not effective in terms of bone and body composition on DXA measurement. In the case of vitamin D deficiency, supplementation is needed because of the lack of vitamin D in foods [37].
This study has some strengths and limitations. To the authors’ knowledge, there is limited knowledge about the serum vitamin D levels in children with CP. On the other hand, not having data on the children’s body mass index, vitamin D content of the feeds, sunlight exposure, PTH levels, and fracture history are the limitations of the study. The results cannot be attributed to all the children with CP because the study includes those who were in a tertiary rehabilitation hospital. Moreover, a control group is missing in this study. Another major limitation of this study in terms of generalizability is the fact that all subjects were Caucasian and they are generally expected to have higher levels of vitamin D as compared to Black, Hispanic, or Asian children.
In conclusion, 42.9% of the children with CP who were admitted to a rehabilitation hospital and had no regular vitamin D consumption had either vitamin D insufficiency or deficiency. Being older and eating regular meal were the risk factors identified for low vitamin D levels in this cohort of children with CP.
Conflict of interest
The authors have no conflicts of interest.
Ethical considerations
This study was approved by the Ethics Committee of Health Sciences University, Sadi Konuk Training and Research Hospital (No: 2019-07-13).
Funding
No funding to declare.