
Abstract
Background:
Labor pain is the nastiest conceivable pain women are involved in during labor and delivery. In this way, the end of labor pain is frequently outlined by myths and equivocalness. Hence, giving a compelling absence of pain in labor remained a challenge specifically in developing countries including Ethiopia.
Objectives:
This systematic review and meta-analysis aimed to explore the pooled prevalence of labor analgesia and associated factors to pregnant women in Ethiopia.
Design:
A systematic review and meta-analysis were utilized in agreement with the Preferred Reporting Items for Systematic Reviews.
Data Sources:
PubMed/Medline, SCOPUS, EMBASE, Web of Science, Google Scholars, and the Cochrane Library and supplemented it with manual were deliberately looked at until January 1–30, 2024.
Methods:
Two authors independently extricated all principal information utilizing standardized data extraction designs, and the analysis was done utilizing STATA version 17. Heterogeneity over the studies was evaluated utilizing I2 measurement. The funnel plot and Egger’s weighted regression tests were utilized to assess subjective and objective publication biases respectively. Also, the pooled effect of labor pain management and the associations were evaluated utilizing a random-effects model.
Results:
The general pooled prevalence of labor analgesia in the present study was 23.3% with a (95% confidence interval (CI): 13.5, 33.1). Maternal age (odds ratio (OR): 1.91; 95% CI: 1.11, 2.77), parity of the mother (OR: 0.28; 95% CI: 0.06, 0.63), history of pregnancy misfortune (OR: 0.12; 95% CI: 0.11, 0.36), length of labor (OR: 2.09; 95% CI: 1.06, 3.13), and awareness about labor analgesia (OR: 1.91; 95% CI: 0.34, 3.49) were significantly related with labor analgesia among pregnant women in Ethiopia.
Conclusions:
The generally pooled prevalence of labor analgesia among pregnant women in Ethiopia was low. Maternal age, parity of the mother, history of pregnancy loss, length of labor, and awareness of labor analgesia were factors influencing labor analgesia among pregnant women in Ethiopia. This finding proposes exceptional consideration to make laboring mothers free of pain by scaling up the strategies and utilizing labor pain administration in a way that universally recognized standards are met.
Registration number:
PROSPERO CRD: 42024525636
Introduction
Indeed, labor is a natural and physiological process; it makes not as it were a physiological but also a mental challenge for most women. The most common mental issues related to labor incorporate pressure, stress, energy, faltering, and dread. Subsequently, it acts as one of the agonizing kinds of pain that the larger part of women confront in their lives.1 –4
Several variables influence the feeling of labor pain, including encounters with past childbirth, education, and religious beliefs.5,6 Women who got to labor pain management had more birth joy by tending to both the physiological and mental viewpoints.7,8 On the other hand, deficient labor pain administration may hurt maternal conditions and influence the advance of labor.9,10 In this respect, women have the right to get the most elevated feasible standard of well-being care, such as physical and psychological.11,12
The approaches to labor pain alleviation are by and large classified into two, pharmacological (outlined to calm pain) and non-pharmacological (pointed at adapting to pain) mediations.8,13,14 The high-income world took labor pain management as a critical issue during the intrapartum period. Hence, laboring mothers have the option to get pain relief methods. 15 On the other hand, in developing nations, the scheduled sort of pain help is aimed at making a difference in bargaining with pain, but the advertising of pharmacological labor pain help is regularly less.16 –18
Participation of the mother in decision-making, sociocultural variables, the relationship of the mother with her benefit caregivers, and the bolster from her family are variables that may be altogether critical in the administration of labor pain for their fulfillment amid the labor and delivery period.19,20 Labor support and care may also include strategies and aid communication between the woman and staff to help her make informed choices. Moreover, it may include passionate bolster for the woman’s accomplice. 21
The practice of labor pain alleviation methods in Ethiopia varies from locale to locale. A study was conducted in Oromia region and the finding uncovered in the general practice of labor and absence of pain was 46%. 10 Another study was done in the same locale and the result delineated that the utilization of obstetric labor absence of pain was 31.9%. 22 Comparable studies were done in the Southern Ethiopia and Sidama regions and the findings uncovered the utilization of labor analgesia was 37.9%, 13.8%, and 41.3% utilized labor analgesics, respectively.1,23,24
Generally, the practice of managing obstetric labor pain was 40.1%, which shows only non-pharmacological methods were preferred, as found in a study conducted in the Amhara region. 7 The review of the literature conducted on practices of labor pain management methods using non-pharmacological ways in the Tigray and Addis Ababa regions showed findings of 43.3%, 0% (nil use of pharmacologic methods), and 36.6%.25,26 Common constraints associated with the non-use of available labor pain management methods have been pointed out to be related to limited knowledge, negative attitudes, and institutional factors, such as the unavailability of analgesic drugs in health facilities.3,8,23,27,28 A previous study from Ethiopia established that very few parturient mothers gave birth in a health facility as compared to the mothers who attended at least the first ANC. In this regard, essential elements for the increase in facility deliveries with the decrease in maternal mortality and morbidity include the management of painful labor. 23
These results indicated that there is some inconsistency in the practice of labor pain relief within its health facilities. This systematic review aims to address the magnitude of pooled obstetric pain management practice and its associated factors among pregnant women in Ethiopia.
Materials and methods
Reporting
This systematic review and meta-analysis were performed according to the guidelines for preferred reporting items for systematic review and meta-analysis (PRISMA). 29 This review is registered in The International Prospective Register of Systematic Reviews (PROSPERO) with registration number CRD42024525636
The PRISMA is a 27-item checklist used to improve transparency in systematic reviews. These items cover all aspects of the article, including the title, abstract, introduction, methods, results, discussion, and funding.
Search strategy
A wide search was conducted in universal databases like PubMed/Medline, SCOPUS, EMBASE, Web of Science, Google Scholars, and the Cochrane Library. The Bepress legal repository and the Social Science Research Network were our best sources for finding unpublished articles and papers. We have utilized key terms such as pharmacologic strategies labor pain, labor, pain management, non-pharmacologic strategies, pregnancy, pregnant women, labor pain alleviation, attitude, awareness, willingness, knowledge, antenatal care, desire, obstetric absence of pain, practice, magnitude, determinants, care providers, obstetric care providers, healthcare providers, skilled birth assistants, midwives, nurses, obstetrician, woman, women, mother, maternal, hospitals, “associated risk factors,” and Ethiopia. In the progressed searched databases, the search procedure was based on the aforementioned terms utilizing “Medical Subject Headings (MeSH)” and “All fields” by connecting “AND” and “OR” Boolean operator terms, as suitable. The search was conducted from January 1 to 30, 2024.
Three authors (TEG, TSH, and WO.) independently evaluated the eligibility of all retrieved studies; Search procedure points of interest are provided as a partitioned record (Supplemental File S1).
Data extraction and quality assessment
The Endnote citation manager (version X8, for Windows; Thomson Reuters, Philadelphia, PA, USA) was applied to import the retrieved studies and duplicated studies were removed. Two independent researchers (TEG and LLF) screened all the articles for eligibility criteria: first, abstract and title and second, full-text screening. Microsoft Excel 2013( Microsoft excel spreadsheet) and STATA version 17 (StataCorp LLC, College Station, TX, USA) were used for data extraction and analysis. The data extraction protocol consists of the name of the first author, year of publication, region/area, study design, sample size, prevalence of labor analgesia, and response rate. The quality of the study was assessed by considering sample representativeness, sample size, and appropriateness of statistical analysis, by using a standardized tool adapted from the JBI tool for prevalence studies which have 10 independent lists of critical appraisal questions. 30 The choice and evaluation of the articles’ quality were done independently by two reviewers (TEG and MB). The articles were included in the systematic review after the agreement was made, and differences between the reviewers were fixed via conversation (Supplemental File S1).
Eligibility criteria (inclusion and exclusion criteria)
Articles collected through the searches were evaluated for consideration in the meta-analysis based on the taking after criteria:
Study results that were held in Ethiopia for the prevalence of obstetric labor pain management and their contributing factors.
All published and unpublished studies in the English dialect express sample sizes and study areas.
Observational studies.
The inquiries about subjects were pregnant women.
The journal studies from 2019 to 2024.
The exclusion criteria were as follows:
Those with copy distributions.
Case reports, review articles, case series, and report to editor.
Conference papers or book chapters and/or the full content were not accessible.
Among so numerous articles published already, as it were five met the expressed choice criteria, and details of study selection were provided in Figure 1.

PRISMA flow diagram of studies included in final systematic review and meta-analysis of the prevalence of labor pain management among pregnant in Ethiopia.
Meta-analysis
All analyses were done using STATA version 17 (StataCorp LLC, College Station, TX, USA) and heterogeneity was checked across the studies by computing the I 2 statistical test. We assumed no, low, medium, and high heterogeneity across the studies if the I 2 values were 0%, 25%, 50%, and 75%, respectively. A random-effects model was used to estimate the pooled prevalence with 95% confidence intervals (CIs) since significant heterogeneity was detected between studies. Meta-regression investigation was performed to examine the source of heterogeneity. A visual review of the funnel plot was performed for any potential publication bias, taken after Begg’s rank and Egger’s tests to check for publication bias. In addition, sensitivity and subgroup analysis were performed to ensure consistency of pooled results such as publication year and study area. The second outcome of this study was factors associated with managing the pain of labor among pregnant women in Ethiopia. All potential determinants associated with labor pain relief were determined using the odds ratio (OR) and calculated based on the binary outcomes of the included primary studies. The estimated pooled OR with 95% CI was reported. The review’s findings were presented per PRISMA recommendations. A narrative synthesis, followed by a meta-analysis of forest plots, tables, and figures was used to present the findings of the studies.
Risk of publication bias
The risk of bias included studies assessed using the Hoy risk of bias tool. 31 The heterogeneity was analyzed by the I 2 test, 32 the funnel plot symmetry, 33 and the Egger test, 34 which were used to assess the risks of subjective and objective publication bias, respectively.
Outcome of interest
The primary outcome of this systematic review and meta-analysis was to estimate the national pooled prevalence of labor analgesia and its associated factors among pregnant women in Ethiopia. The provision of adequate labor pain relief can be a basic element for the increment of institutional delivery, and it consequently upgrades women’s satisfaction. It is a critical factor to pinpoint the gaps between the practice of labor pain relief methods and anticipated healthcare outcomes to reduce maternal morbidity and mortality.
Results
In total, 1,981 primary articles were distinguished utilizing different databases. From the total recognized studies, 1,524 articles were removed due to duplication utilizing ENDNOTE and visual appraisal. From the remaining 457 studies, 370 articles were excluded after screening the individual titles and abstracts. The qualification of the remaining 87 full-text articles was evaluated leading to the exclusion of 83 studies that did not display the result of intrigue, were conducted outside of the study range, and had methodological contrasts. At last, five studies were included in this systematic review and meta-analysis (Figure 1).
Characteristics of the included studies
A total of five qualified cross-sectional studies detailed in English were included in this systematic review and meta-analysis. A total of 1,961 pregnant women have taken part in the study. The sample sizes of the studies extend from a minimum of 324, in the Amhara Locale 35 and the maximum sample estimate was 423 from Central Ethiopia. 36 Based on the locale, two from Amhara,14,35 one study from central Ethiopia, 36 Sidama, 37 and Oromia 38 studies were involved in this systematic review and meta-analysis (Table 1).
Characteristics of included studies in the meta-analysis of labor pain management among pregnant women in Ethiopia, 2024.

Pooled estimates of labor pain management
From a systematic review of five-pocket studies, the pooled prevalence of labor pain management among pregnant women in Ethiopia was 23.3% (95% CI: 13.5, 33.1) as shown in Figure 2.

Forest plot showing the pooled prevalence of labor pain management among pregnant women in Ethiopia, 2024.
Subgroup analysis
The subgroup analysis focusing on the sample size revealed that the sample of less than 400 had the highest prevalence (26.87%, with a confidence interval of 19.03, 34.7), whereas sample size ⩾400 had the lowest prevalence (20.92%, with a confidence interval of 6.5, 35.33) as shown in Figure 3.
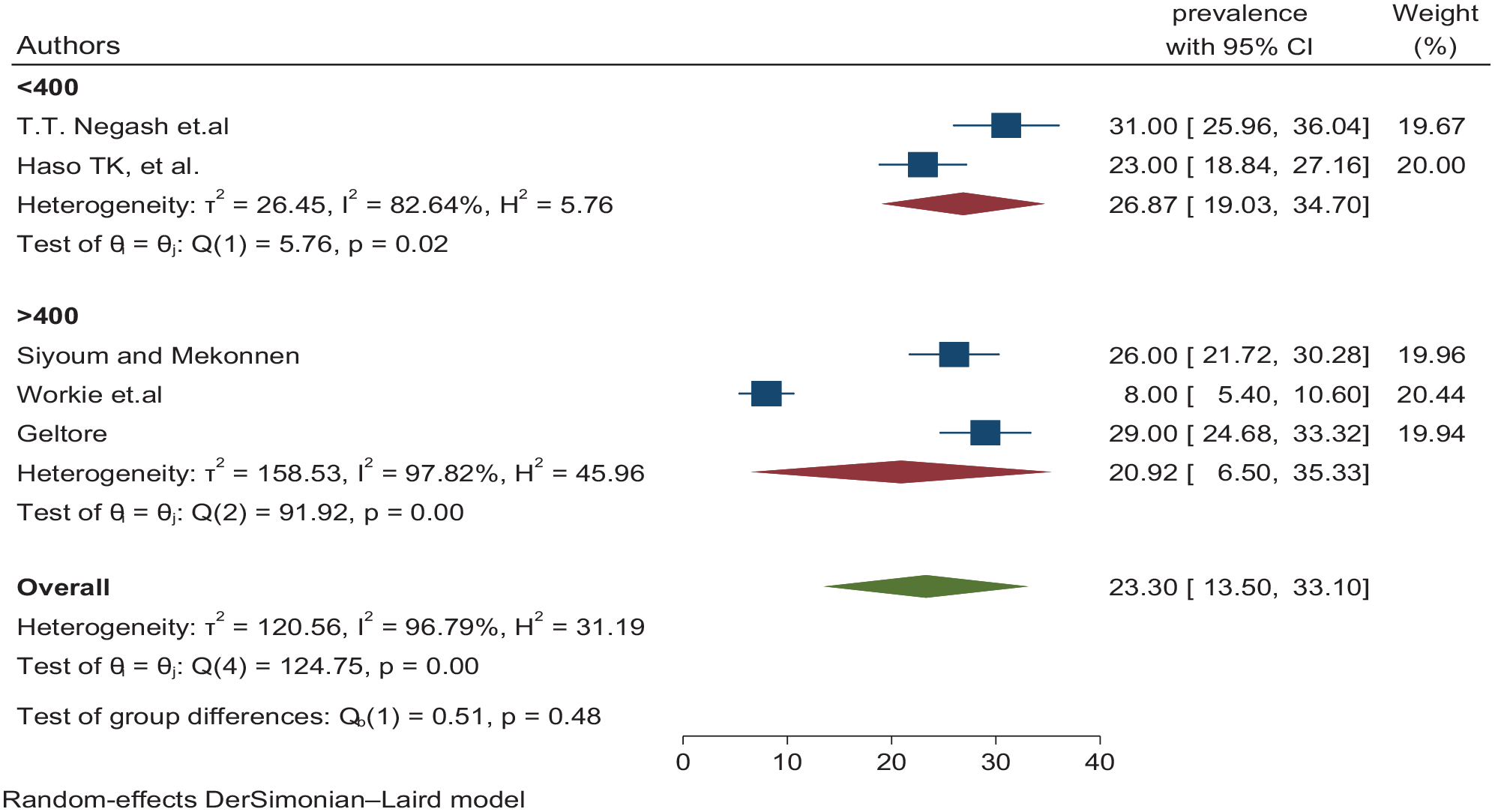
Subgroup analyzes the pooled prevalence of labor pain management among pregnant women in Ethiopia, in 2024.
Sensitivity analysis
We investigated deeper into the heterogeneity’s origins through a leave-one-out sensitivity analysis. This examination showed that excluding each study individually from the analysis did not significantly alter the estimated average prevalence. An average prevalence remained within the 95% CI of the overall average prevalence obtained when all studies were included. Consequently, an average prevalence was not influenced by any single study. Additionally, the sensitivity analysis revealed that excluding each study individually resulted in the average prevalence of 23.3 (with a 95% confidence interval of 13.5–33.1) as shown in Figure 4.

Sensitivity analyzes for the pooled prevalence of labor pain management among pregnant women in Ethiopia, 2024.
Meta-regression
Substantial heterogeneity was observed among the studies incorporated into the meta-analysis. To explore the sources of this heterogeneity, we conducted a meta-regression analysis, incorporating variables such as publication year and sample size. However, publication year and sample size in meta-regression analysis did not reveal a significant impact on the observed variation as shown in Table 2.
Meta-regression to identify the source of heterogeneity for the pooled prevalence of labor pain management among pregnant women in Ethiopia, 2024.

CI: confidence interval.
Bias in publications
By visually inspecting a funnel graph, the symmetric distribution of labor pain management among pregnant women in Ethiopia was evaluated without publication bias as shown in Figure 5.
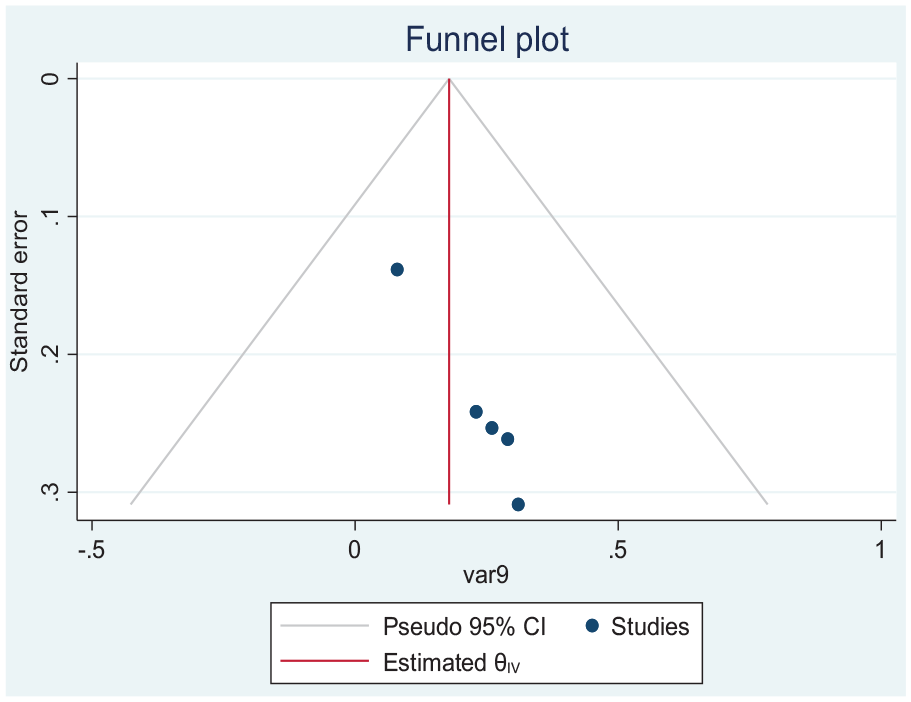
Funnel plot meta-analysis of labor pain management prevalence in Ethiopia.
Factors associated with labor pain management practice among pregnant women
This systematic review and meta-analysis identified the most often occurring related variables, which were maternal age, parity of women, previous history of pregnancy loss, duration of labor, and awareness of labor analgesia as shown in Figure 6.

Factors associated with labor pain management among pregnant women in Ethiopia, 2024.
Labor analgesia among participants, whose age group of 25–31 years was higher than those participants whose age group was 18–24 years. More specifically, meta-regression from two studies14,38 showed pregnant women whose age ⩾25 were almost twice as likely to practice labor pain management than pregnant women of the age group 18–24 years (OR: 1.91; 95% CI: 1.11, 2.77). The pooled results of two studies37,38 showed primigravida women practice labor pain management 72% less likely compared to multipara mothers (OR: 0.28; 95% CI: 0.06, 0.63; I 2 = 50.2%). Similarly, findings from meta-regression of two studies37,38 showed study respondents who had a previous history of pregnancy loss were 88% less likely to utilize labor pain management methods than those who hadn’t a previous history of pregnant loss (OR: 0.12; 95% CI: 0.11, 0.36; I 2 = 41.5%). The pooled results of two studies36,37 showed that short duration of labor <12 h were positively associated with labor pain management than their counterparts (OR: 2.09; 95% CI: 1.06, 3.13; I 2 = 15.4%). Additionally, findings from two studies36,38 showed study participants who had awareness of labor analgesia were almost two times more likely than those who had no awareness (OR: 1.91; 95% CI: 0.34, 3.49; I 2 = 10%).
Discussion
The study findings showed that negative sentiments during labor can prolong the progress of labor or indeed make the mother despise being pregnant once more which in turn leads to an obsessive fear of childbirth which accounts for 6%–10% of pregnant women. 39 Numerous low and middle-income nations, the issue of labor pain alleviation, and the conceivable outcomes or determination on how and what to do when is not well recognized. 13
The overall pooled prevalence of labor pain administration among pregnant women in the present study was 23.3% This is comparable with past studies conducted in Ethiopia (25.7%). 37 However, this finding is lower than the findings of India (34%), 40 Nepal (72.2%) 41 but, higher than the results of studies conducted in Nigeria (6.7%). 42 The possible clarification might be due to different cultural practices. In the subgroup investigation, the prevalence of labor pain administration varied on sample size. The subgroup investigation centering on sample size appeared that the sample less than 400 had the highest prevalence (26.87%, with a confidence interval of 19.03, 34.7), whereas sample size ⩾400 had the lowest prevalence (20.92%, with a confidence interval of 6.5, 35.33). The possible clarification might be varieties in the need for awareness, inadequate respectful maternity care, and unavailability of labor-management protocols, the study period, and the sociocultural characteristics of mothers, health offices’ rules, and regulations. The other possible clarifications might be due to negative attitudes toward labor analgesia, the need for consideration for labor pain, the setting of the health settings, and the lack of a trained workforce might be obstacles to utilizing labor pain management.
In this systematic review and meta-analysis, we moreover found that maternal age, parity of women, history of pregnancy loss, term of labor, and awareness about labor absence of pain were found to be factors related to labor pain administration among pregnant women in Ethiopia. In the current systematic review and meta-analysis, the odds of labor analgesia among pregnant women who were aged 25–31 years were nearly two times more likely to hones labor pain administration than pregnant women aged 18–24 years (OR: 1.91; 95% CI: 1.11, 2.77). This finding was consistent with studies from Jeddah Saudi Arabia 43 this might be because women aged 25–31 had a better level of understanding of things than their counterparts.
This study also uncovered the odds of labor analgesia practice among primigravidae mothers are 72% less likely compared to multigravida mothers. The current finding is conflicting with studies conducted in the Netherlands, 44 India, 40 Nigeria, 45 and Sweden. 46 The distinction might be due to contrasts in culture and setting. Labor pain resilience and expression of pain escalated is influenced by cultural, physical, and mental factors.
The previous history of pregnancy loss was moreover related to labor analgesia. The finding is bolstered by studies conducted in Ethiopia. 37 This seems to be due to a few women not practicing labor analgesia, due to the fear that it may prolong their labor and lead to another pregnancy loss since they moreover have past mental trauma.
Our study found that pregnant women who had a history of short length of labor were 2.1 times more likely to practice labor analgesia than their counterparts. This was upheld by studies done in the Netherlands. 44
Moreover, pregnant women who were aware of obstetric labor analgesia were 1.91 times more likely to practice labor analgesia compared to women who did not have awareness about labor analgesia. Comparable finding was reported in in India 47 and Belgium. 48 This might be due to the truth that pain relief in labor is to make a sincerely fulfilling involvement where a woman is delivering a healthy infant with as small trouble, pain, and fatigue as possible.
Implication of the study
The study gives a compressive outline of the prevalence of labor analgesia among pregnant women in Ethiopia. The data is pivotal to tailor intercession and improve positive maternal and neonatal outcomes. This information can advise clinical guidelines for the management of labor pain management among pregnancies. This study contributes significantly to the body of knowledge, impacting clinical practice, policy advancement, and future investigative endeavors in the area.
Limitations of the review
This study has its limitations. Since the study incorporates only a cross-sectional study, it did not address the cause and impact relationship of the factors and the outcome factors. The other limitation of this study is that only English language-based articles or reports were collected to conduct this meta-analysis. The data presented in this analysis cannot be used to decide if the appropriate use of an approved WHO program by clinicians and nurses had any effect on pain management during labor. There is also an incredible variety in sample size from study to study, which may impact the evaluated prevalence reported. Small numbers of published papers were collected from the locales included in this study, so the prevalence of labor pain management among pregnant women may not be completely represented.
Conclusion
The study revealed that the generally pooled prevalence of labor analgesia practice among pregnant women was 23.3%. These results are not positive, especially when it is expected that women ought to be gotten, among other things, successful pain alleviation during labor. Maternal age, parity of women, history of pregnancy loss, duration of labor, and awareness about labor analgesia were significantly associated with labor pain administration. Health professionals should be prepared with the required attitudes, knowledge, and abilities, and progress struggles must be made in conveying health facilities with the required materials and workforce. Hence, we suggested future researchers consider randomized controlled trials to evaluate the practice of pain management on its impact on clinical outcomes. Suitable rules and strategies for the utilization of obstetric analgesia are also key elements
Supplemental Material
sj-docx-1-whe-10.1177_17455057241275442 – Supplemental material for Predictors of labor pain management among pregnant women in Ethiopia: A systematic review and meta-analysis
Supplemental material, sj-docx-1-whe-10.1177_17455057241275442 for Predictors of labor pain management among pregnant women in Ethiopia: A systematic review and meta-analysis by Teketel Ermias Geltore, Tesfahun Simon Hadaro, Woldetsadik Oshine, Merkin Bekele and Lakew Lafebo Foto in Women’s Health
Supplemental Material
sj-docx-2-whe-10.1177_17455057241275442 – Supplemental material for Predictors of labor pain management among pregnant women in Ethiopia: A systematic review and meta-analysis
Supplemental material, sj-docx-2-whe-10.1177_17455057241275442 for Predictors of labor pain management among pregnant women in Ethiopia: A systematic review and meta-analysis by Teketel Ermias Geltore, Tesfahun Simon Hadaro, Woldetsadik Oshine, Merkin Bekele and Lakew Lafebo Foto in Women’s Health
Supplemental Material
sj-docx-3-whe-10.1177_17455057241275442 – Supplemental material for Predictors of labor pain management among pregnant women in Ethiopia: A systematic review and meta-analysis
Supplemental material, sj-docx-3-whe-10.1177_17455057241275442 for Predictors of labor pain management among pregnant women in Ethiopia: A systematic review and meta-analysis by Teketel Ermias Geltore, Tesfahun Simon Hadaro, Woldetsadik Oshine, Merkin Bekele and Lakew Lafebo Foto in Women’s Health
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.