
Abstract
CASE DESCRIPTION:
A 2-month-old child required a bilateral limb amputation, right transtibial, and left transfemoral after a deep burn compromising one-third of the body surface area. Traumatic amputations of lower limbs at such an early age are uncommon and underreported in the literature, especially in middle-income countries.
OBJECTIVE:
To describe the long-term follow-up of the prosthetization process after traumatic bilateral amputation of a 2-month-old patient.
TREATMENT:
The process started with compensatory prostheses for independent sitting, followed by exoskeletal devices with SACH feet, and finally introduced dynamic feet and knee to achieve progressively independent gait.
OUTCOMES:
The patient achieved functionality, autonomy, and social interaction for his age. The habilitation process continues to improve his independent gait and support upcoming life changes.
CONCLUSION:
Through a multidisciplinary approach, family support, and timely changes of device components according to the child’s development, this patient has been able to achieve a normal life.
Case description
This case presents a 31-day-old boy with no relevant perinatal history, who suffered deep thermal burns in the lower limbs, accounting for 30% of the body surface area. After 21 days of hospitalization, the patient required amputation of the lower limbs –transtibial on the right side, and proximal third transfemoral on the left side. From that moment, the team started a pre-prosthetic management plan as part of the in-patient rehabilitation. During the hospitalization, the surgical team applied multiple skin grafts in the residual but considered it unnecessary to perform skin flaps or revision of the stumps. The patient’s legal guardian has authorized the publication of this case and the photographs, and review by the institutional board was not required for this case report.
Treatment
At five months old the patient attended our outpatient protheses clinic with good skin scarring, preserved sensitivity, and full range of motion in the right knee. During that visit, the team prescribed a pylon-type compensatory prosthesis for the left side matching the length of both legs, so the patient could sit, kneel, and crawl (Fig. 1a). At 8 months old, we adapted pylon-type prostheses for both limbs for the patient to crawl easily and start standing with help (Fig. 1b). During the following months, the ortho-prosthetist adjusted the devices as the patient grew. At 30 months old, considering the availability of components for small children, including no availability of small dynamic feet in the country, the team changed the devices for an exoskeletal left transfemoral prosthesis with pelvic band, no knee joint, and Solid-Ankle Cushion Heel (SACH) foot and an exoskeletal right transtibial prosthesis with SACH foot (Fig. 1c), to train standing equilibrium and gait in the habilitation plan. Four months later, when the patient had the protheses, a child-type walker with front wheels was prescribed. For the following years, as the child grew, he used anatomically designed sockets with multiple interfaces and frames with increasing longitude. The ortho-prosthetist changed both components whenever the patient needed. At 5 years and 7 months old, the team replaced both terminal devices for dynamic feet, added a single axis hip joint due to its lower weight and a polycentric fluid control knee to the left prosthesis to reduce inappropriate movements in the gait, improve tolerance of uneven surfaces and facilitate changes in velocity and direction. At six years, the team substituted the left socket for a double-walled hybrid with soft internal material Kondylen-Bettung Münster (KBM) one to decrease the valgus of the prosthetic knee, and the walker for Canadian canes so the patient could be more independent, increase the interaction with surroundings, and facilitate school integration. At 7 years, the right transtibial prosthesis suspension system was switched for a shuttle-lock-pin system (Fig. 1d). Table 1 describes the prostheses that the patient has had during the habilitation process. Since the first amputation procedure, there has been no residual limb overgrowth or skin problems that required reinterventions by the orthopedic department.
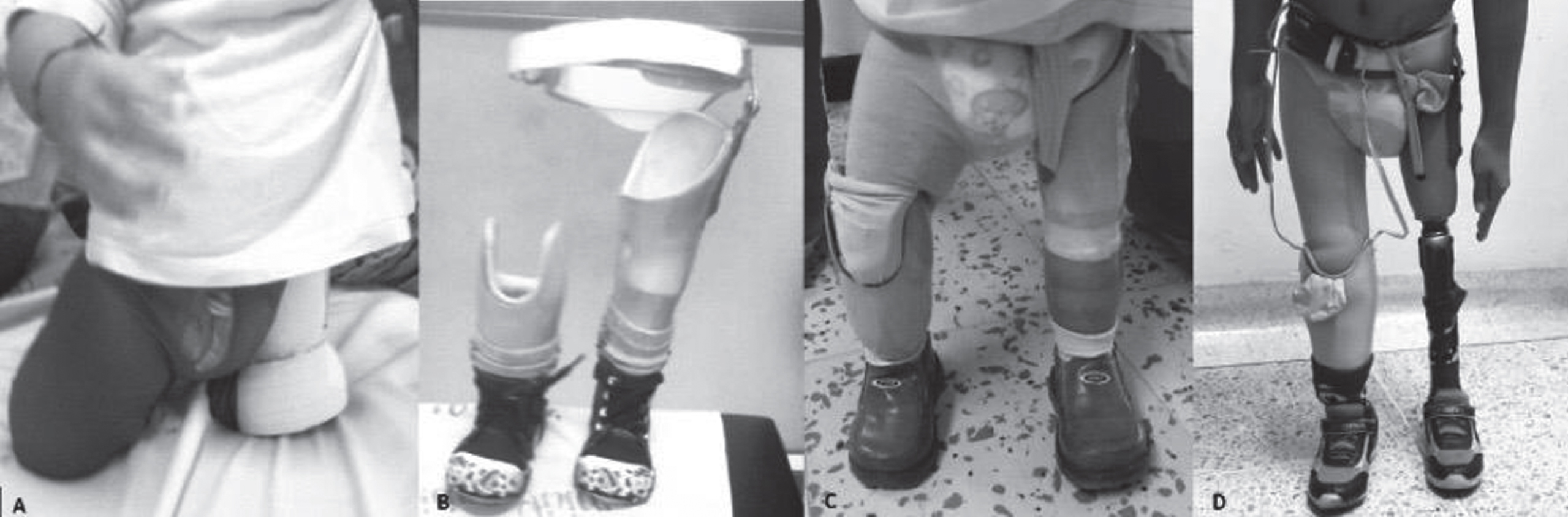
Patient Prostheses a. Compensatory prostheses of the lower right and left limbs, with a long socket for crawling and pelvic support. b. Pylon-type prosthesis. c. Exoskeletal prosthesis for left transfemoral amputation with a pelvic band and additional support of neoprene without knee joint, SACH foot. Exoskeletal right transtibial amputation prosthesis with supracondylar socket, neoprene support, SACH foot. d. Exoskeletal prosthesis for left transfemoral amputation with pelvic band, single-axis hip joint, full contact socket, fluid control polycentric knee (pneumatic and pediatric), dynamic foot flexible keel. Exoskeletal prosthesis for right transtibial amputation with full contact socket, fastening system by silicone liner shuttle-lock-pin, and dynamic foot flexible keel.
Patient prostheses timeline
Pediatric rehabilitation medicine, physical and occupational therapy, and ortho-prosthetist collaborated to define the precise moments to change the prosthetic components. Rehabilitation objectives with this multidisciplinary team were: adapting to the different components of the prosthesis; gaining independence in everyday activities and gait pattern; and playing activities appropriate for the patient’s age. This collaboration has allowed adapting to the prostheses and accomplishing development of the patient, including gross motor milestones. Family and health group support have been vital to guarantee timely access to health services and social integration.
The patient is now 8 years old; he performs daily activities appropriate for his age, puts on and takes off his protheses independently. He started school in an integrated classroom at 6-year-old, can walk 500 meters with Canadian canes and occasionally plays soccer with his peers. The follow-up in the out-patient protheses clinic and pediatric rehabilitation continues, focusing the habilitation plan on training of gait and equilibrium to reduce support of walking aids, and assuring school integration. The patient and his family have seen the importance of the habilitation process for achieving development and maintaining social integration.
Discussion
This case is relevant for three main points: traumatic burn amputations are uncommon at such an early age, use of prosthetic knees before independent walking achievement in bilateral lower limb amputations in children is not the usual practice, and clinical cases in middle income countries and their challenges are under-reported in scientific literature.
The case presents an uncommon etiology of amputation in young children, since burns are rarely reported. Limb amputations in children have a prevalence of 38.5 cases per 100,000 children in the United States, with 80% of them related to congenital limb deficiencies [1]. Accidents are the second most common cause with 13.8% of the cases. They exhibit two incidence peaks during childhood: between 0 and 5 years – around 40% of cases – and between 14 and 17 years [1, 2]. Traumatic amputations in children frequently relate to entrapment between objects and machinery; burns are an uncommon cause listed usually under “other causes” [2]. The most common levels of major amputations are transradial in the upper limb, and transtibial in the lower limb [3].
Children with amputations frequently present two complications: length discrepancies and skin problems. The tibia tends to overgrow during the child’s development, which leads to frequent need of reinterventions to remodel the residual limb [4]. On the contrary, the residual femur usually remains short since most of the length development depends on the distal epiphysis, leading to lever arm difficulties on the movement of the hip or requiring treatment as a hip disarticulation which happened in the presented case [4]. The most frequent complication is skin problems, with more than half of them requiring reinterventions to guarantee adequate skin cover. The patient has not presented this complication this far [5]. During childhood, there is neuroplasticity that helps remodel the cerebral body image, making extremely uncommon phantom sensation and pain in children younger than ten years [6, 7].
Among the amputations related to burn accidents, this child is also an infrequent case. Burns rarely repercuss in amputations, incidence is between 1.1% and 1.5% of the admitted patients to specialized units around the world [8–10]. The patients who require amputations are more frequently males in their twenties, suffer electric burns, and have compromise of the upper limb [8–10]. The youngest patient reported in these series is 14 years old, which makes the patient significantly younger [8]. Nevertheless, up to a quarter of the patients require amputation of multiple limbs, as it happened in this case [9, 10]. These cases present with specific complications: requiring more escharotomies and skin grafts –as occurred with this patient; losing skin grafts during the prothesis adaptation and suffering infections with resistant germs [8, 10].
The second relevant characteristic of this case is early incorporation of a prosthetic knee. Young children with amputations present a challenge to rehabilitation teams, requiring constant work to balance the accomplishment of gross motor milestones and safety of the patient [7]. To accomplish these objectives, the classic approach to above-the-knee amputations is delaying the introduction of the prosthetic joint until the patient has a stable gait pattern without assistive walking devices. This usually occurs around the third year of age in children with unilateral lower limb amputations [5, 7]. In children with bilateral lower limb amputations accomplishing equilibrium in the gait pattern is challenging, so in most cases, they use blocked prosthetic knees during stance [6]. During the last decades this paradigm has been changing, considering that around 96% of pediatric patients with lower limb amputations accomplish an independent gait pattern in the long term [3]. Many authors believe earlier knee introduction produces superior gross motor development in children with lower limb amputations [7, 11]. Studies have found that early introduction of the prosthetic knee generates a symmetrical crawling pattern that closely resembles the normal one, reduces abnormal hip circumduction movements during gait, generates a more symmetrical length of the step, and facilitates velocity gain with age [12–14]. However, all these studies have only included patients with unilateral lower limb amputations, making this patient a novel case of early introduction of knee articulation in a bilateral lower limb amputation [11–14].
The third significant condition of this case is the context and country in which it was presented. For middle-income countries, like Colombia, burns are among the principal causes of disability: 18% of burned children have a permanent disability, as was the case of this patient [15]. It is even more worrisome that children under five suffering burns have twice the risk of dying as the ones in high income countries, making it even more important in these countries to guarantee a multidisciplinary approach and family support [15]. In Colombia, children under 5 represent more than half of the burned children and account for more than 20% of the deaths related to burns [16]. After these accidents, health insurance coverage acts as a facilitator in Colombia since most people have access, and protheses and habilitation are covered, reducing the out-of-pocket costs for the family [17]. Nevertheless, accomplishing social inclusion might have important barriers. For example, in Colombia, 90% of children with disability do not go to school [18].
Conclusions
This case illustrates an appropriate habilitation process of a bilateral lower limb amputation secondary to burns in a child. It opens the possibility for early use of dynamic knee in the prothesis of these types of patients and highlights the importance of a multidisciplinary approach and family support for appropriate development and social integration in middle-income countries.
Conflict of interest
The authors have no conflict of interest to report.
Ethical considerations
The patient’s legal guardian has authorized the publication of this case and the photographs, and review by the institutional board was not required for this case report.