
Abstract
PURPOSE:
Assess the effects of stay-at-home orders on access to services utilized by families of children with disabilities (CWD).
METHODS:
Cross-sectional weekly surveys were fielded over four weeks, during which western Pennsylvania was under stay-at-home orders. Respondents were divided into families of CWD (N = 233) or without CWD (N = 1582). Survey questions included measures of socio-economic status, and families of CWD answered questions regarding access to services pre and post-initiation of stay-at-home orders. Differences between families with and without CWD were analyzed using chi-square tests.
RESULTS:
Among families of CWD that had used services previously, 76.6% of survey respondents stated that they had decreased access, with the greatest percentage experiencing loss among those previously utilizing early intervention (75.5%), outpatient therapies (69.1%), or school-based therapies (80.7%). Compared to families without CWD, families of CWD were more likely to report lower pre-COVID-19 annual incomes (p < 0.001), job or income loss related to COVID-19 (p < 0.001), and higher levels of perceived stress (p < 0.001).
CONCLUSION:
CWD experienced loss of services during stay-at-home orders implemented as COVID-19 mitigation measures. Due to decreased access to needed services, CWD may be at risk of medical complications and loss of developmental progress.
Introduction
Stay-at-home orders and school closures during the coronavirus disease 2019 (COVID-19) pandemic had extensive consequences for children and families, especially those with fewer financial resources and greater healthcare and educational needs [1, 2]. One group at elevated risk of negative consequences were children with disabilities (CWD), particularly those who were part of marginalized populations [3, 4]. CWD often utilize extensive therapeutic and medical services [5], which are critical in optimizing function, and minimizing the impact of impairments [6]. These services traditionally are provided in-person, and access was disrupted due to COVID-19 mitigation measures [7].
The present study examined challenges faced by families with CWD during the stay-at-home order. Specifically, access to early intervention (EI), outpatient, and school-based services was assessed using a repeated cross-sectional survey, the Family Strengths Survey (FSS), part of an ongoing academic community collaborative called “The Pittsburgh Study.” [8]. In addition, differences in job loss and household income between families with and without CWD were examined to better understand the degree to which families of CWD were affected by COVID-19 mitigation measures.
Methods
Initiated April 3, 2020, the FSS was a weekly anonymous survey of families in western Pennsylvania developed to identify strengths and needs of families during the pandemic. Surveys were available in English and Spanish, with invitations to participate distributed online through list-servs and social media. Completion of the survey could be done online or by telephone, although all responses in this study were obtained online (due to rare telephone participation). The FSS was reviewed by the institutional IRB prior to implementation and determined to be exempt. Eligibility was based on whether the respondent lived in western Pennsylvania, was 18 years or older and was pregnant, or had children under 17 years of age. Starting on April 17, 2020, questions identified CWD using a modified screener question based on the Children with Special Health Care Needs Screening tool [9]. Specifically, the survey asked whether “child(ren) in the home or immediate family have health problem(s) that cause them to be limited in their ability to do things that other children of the same age can typically do.” Respondents answering yes to this question were asked about service use over the prior six months and during the prior week, specifically about EI, outpatient or home-based therapies, school-based services, durable medical equipment (DME)/supplies, home nursing or home health aide services, and respite services. Perceived stress was measured between April 17 and May 1 using a modified set of standardized questions from the Perceived Stress Scale (PSS; [10]) validated in prior studies [10, 11]. The PSS responses were totaled and categorized into low, medium, or high stress based on previously published thresholds [10, 11].
Results from four weekly cross-sectional surveys fielded April 17-May 14, 2020, during which time western Pennsylvania was under stay-at-home orders, were pooled for analysis. Of the 2,384 surveys initiated, 1,815 (76.1%) met eligibility requirements and were fully completed. Differences in demographic characteristics, job loss, and perceived stress between families with and without CWD were analyzed using chi-square tests. Analyses were performed using Stata 16.0 (StataCorp, College Station, TX).
Results
Of the 1,815 completed surveys during the four-week period, 233 were by families with CWD. Surveys by those with CWD were more likely to report lower pre-COVID-19 annual incomes (p < 0.001), and job or income loss related to COVID-19 (p < 0.001; Table 1). In addition, surveys by families with CWD were more likely to report higher levels of perceived stress (p < 0.001) than other families.
Demographic characteristics and perceived stress levels from the family strengths survey
Demographic characteristics and perceived stress levels from the family strengths survey
*When data was missing for a certain characteristic, that subject was not included in the totals for that characteristic. **Only measured between April 17-May 1, 2020 (N = 958).
Among families with CWD, services most often used in the six-months pre-COVID-19 were EI (22.8%), outpatient therapies (36.1 %), and school-based therapies (48.9%). During the stay-at-home order period, 76.6% of surveys by families noted reduced access to usual services in the prior week (Fig. 1). Of those that had utilized EI, outpatient therapies, or school-based therapies, 75.5%, 69.1%, and 80.7%, respectively, reported reduced access in the prior week. The reductions in access to DME and nursing services were 9.3% and 18.8% in the prior week. Only two surveys indicated use of respite care pre-pandemic, with both reporting reduced access. Among surveys by families with CWD, 60.3% stated that they had a plan for their child’s care should they or another child’s caregiver become ill.
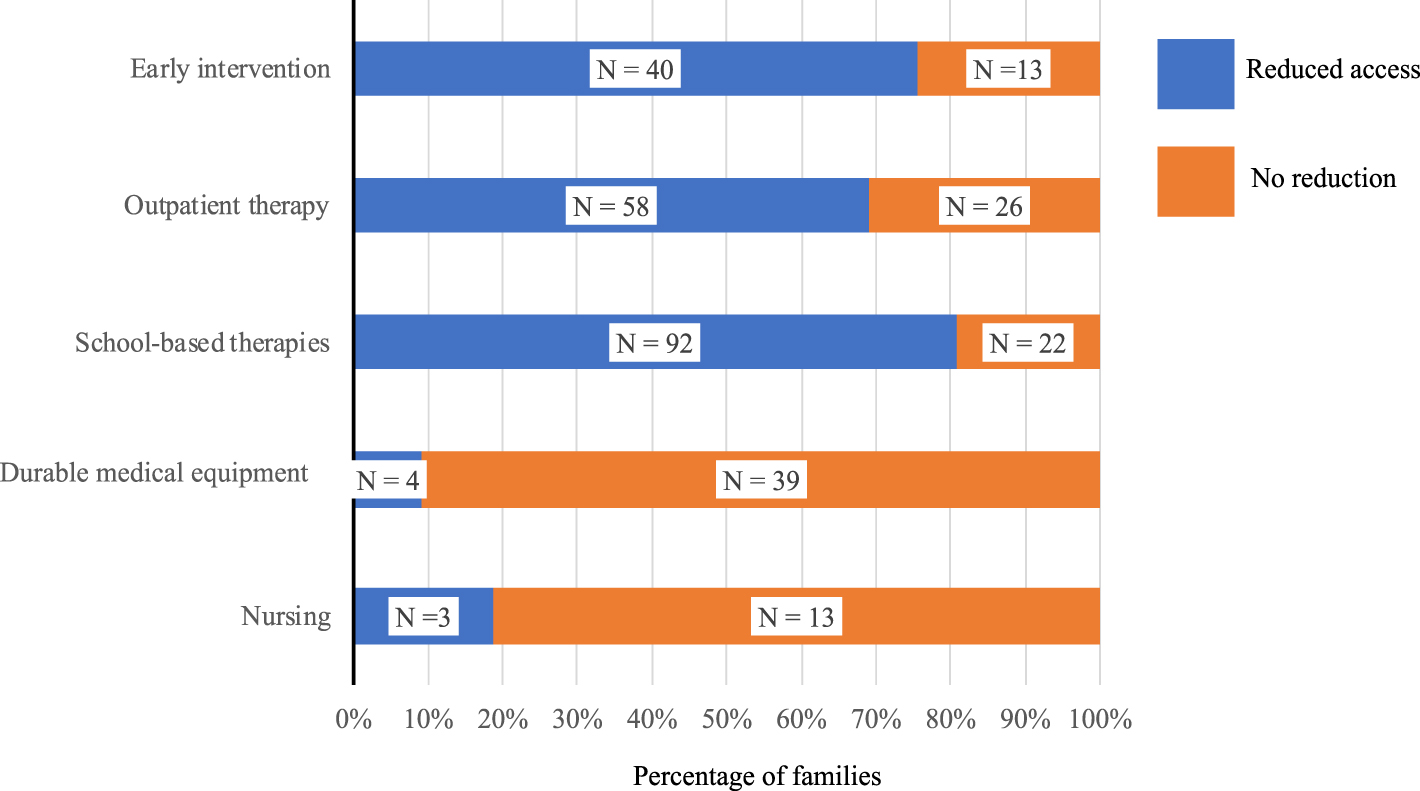
Changes in access to services for CWD following implementation of COVID-19 mitigation measures. Results show numbers of survey responses, as well as percentages.
Related to COVID-19 pandemic mitigation measures in the early pandemic period, access to essential services for CWD were severely curtailed, placing these children at significant risk for loss of developmental progress and medical complications. This study found that families with CWD had lower pre-pandemic income, which is consistent with prior studies [12, 15]. In addition to this lower pre-pandemic income [14], data show that families with CWD were more likely to report income loss during this time period, suggesting that those with CWD were more likely to experience additional socioeconomic setbacks during the implementation of early COVID-19 mitigation measures.
This study adds to the growing body of literature on the effects of COVID-19 on access to services for CWD, showing significant disruption of therapeutic services. In a recent nationwide survey of 1,100 families representing 2,300 children, meeting special education needs was the second greatest challenge during COVID-19, with only 27% of caregivers noting that their child’s IEP or 504 Plan was ‘met well’ or ‘mostly met’ [16]. Caregivers of children with neurogenetic conditions also reported that the COVID-19 pandemic moderately or severely disrupted their children’s therapies, and telehealth was not meeting their needs [17]. In addition, 44% of parents surveyed reported low satisfaction with therapy services, with children who receive school-based services having less access to telehealth than those receiving services in EI or outpatient settings [18]. To fill these gaps, parents often provided therapies in place of trained therapists [19]. Taken together, it is clear that provision of services was significantly limited. Thus, the results on developmental outcomes are as of yet unknown.
It is noted that the FSS, while distributed widely across western Pennsylvania, is a non-random sample. In pooling weekly surveys over four weeks, it is possible that the same individuals responded multiple times. Chi-squared analyses were used to compare families with and without CWD, without the use of adjusted associations, as per previous FSS analyses [8]. In addition, as this study is based on self-reported data, there is the possibility of misreporting. Regarding the representation of the population of the area, the racial makeup of this study is similar to that of the region overall [20], with 81.6% of the population identifying as white. However, other studies have shown racial disparities in terms of prevalence of disability [13], which was not seen in the sample used (Table 1), although the prevalence of disability (12.8%, Table 1) falls within the range of estimates of disability among children [15]. Consequently, these results should not be considered representative of the region or national population. Furthermore, during the survey period, parents of CWD reported higher perceived stress. There is no data to compare pre-mitigation stress and no assumptions can be made about causality.
These limitations notwithstanding, the findings point to the critical need to identify and increase support for families with CWD as this pandemic and mitigation strategies evolve and in preparation for future public health emergencies. Children, particularly those who are medically vulnerable, racial and ethnic minorities, and those living in poverty, require greater support [3, 21]. As school districts evaluate strategies for in-person classes and community agencies continue remote service provision where possible, families are weighing the risks of COVID-19 exposure vs loss of needed services, further highlighting the persistent inequities in care for CWD. In addition, given the strong relationship between medical complexity and social determinants of health [22], CWD need specific attention regarding access to needed services and educational supports. It is incumbent on all of those providing these services to think critically about how to ensure that CWD maintain access to services in a way that decreases risk of exposure to COVID-19 while providing support to maintain and strengthen development.
Footnotes
Acknowledgments
Thank you to Dr Stacey Cook for her support of this project.
Conflict of interest
Dr. Miller receives royalties for writing content for UpToDate (Wolters Kluwer), unrelated to the content of this manuscript.
Funding
All phases of this study were supported by the Shear Family Foundation, Grable Foundation, UPMC Children’s Hospital of Pittsburgh Foundation, and the University of Pittsburgh Department of Pediatrics.