
Abstract
PURPOSE:
This study investigated the effects of the challenge point framework (CPF) to improve stepping reactions and enhance balance in children with hemiplegic cerebral palsy (HCP). The CPF relates practice variables to the skill level of the individual and task difficulty.
METHODS:
Nine children with HCP (age: 7.7±2.4 years) completed six weeks (12 sessions) of a CPF intervention which consisted of progressively fewer sets and repetitions of a stepping reaction task wherein participants sought to improve both step length and reaction rate. Stepping reaction (step length and reaction rate) to a balance perturbation in the anterior, posterior, and lateral directions and static and dynamic balance (via the Pediatric Balance Scale) were measured at baseline, a second baseline 3 weeks later, and post-intervention. Repeated measures ANOVAs determined within-group changes. Cohen’s d effect sizes were calculated.
RESULTS:
Participants improved balance (d = 0.948, p = 0.010), step length (forward d = 0.938, p = 0.002; backward d = 0.839, p = 0.001; and lateral d = 0.876, p = 0.002), and reaction rate (forward d = 0.249, p = 0.042; backward d = 0.21, p = 0.047; and lateral d = 0.198, p = 0.049).
CONCLUSION:
These findings indicate that children with HCP may benefit from completing a CPF program with a motor learning approach. This approach of retraining stepping reactions helped to improve static and dynamic balance. The CPF may aid progression of functional task training in children with HCP aged 4–12, though more studies with a long-term follow-up analysis are needed to confirm this result.
Introduction
Hemiplegic cerebral palsy (HCP) is a common type of cerebral palsy (CP) characterized by movement disorders on one side of the body. Poor postural control is one of the main gait problems in people with CP (1) and can increase fear of falling and fear of sustaining further injuries, which causes patients with HCP to limit their activities and not to be able to perform their activities of daily living independently (2). Thus, improving postural control in patients with CP is important for optimizing independence.
One of the most common reactions to a balance perturbation during daily activities is to take a step forward and regain balance (1). People with central nervous system disorders (such as children with CP or after stroke) have problems with maintaining balance and stepping forward due to slow reaction time and poor motor unit coordination (1). Different interventions have been used to improve stepping and balance, including balance-training (3), gait training, and resistance training (4). These previous interventions demonstrated small to moderate effect sizes, likely suggesting a small treatment effect or small clinical impact of the treatment on the patient and indicating that additional intervention strategies may be necessary.
As a potential strategy for overcoming the limitations of previously-used stepping and balance training interventions and to accommodate performers with different abilities, theorists have proposed the challenge point framework (CPF). The CPF system is a motor learning principle that suggests active involvement of the patient is critical to success of the movement-based intervention. The CPF focuses on the interaction of the individual’s skill and the degree of exercise difficulty (1, 5, 6). Within the CPF approach, the difficulty of exercise training tasks is described as both nominal and functional (6). Nominal task difficulty is the characteristic of the task without consideration of the person performing it. Functional task difficulty is the challenge of the task, considering the skill level of the performer and the conditions under which the task is being completed. Functional task difficulty can be manipulated by clinicians. Given the same task and practice conditions, it is anticipated that children with HCP would require increased cognitive effort or challenge to learn a new motor task. However, it is not known if feedback during practice benefits children with CP in a similar manner to children with typical development (7).
Learning new motor skills for children is essential to increasing their independence and performing activities of daily living. Children with CP have sensory, motor execution, and cognitive impairments that alter their motor learning strategies. It is well established that feedback-enhanced motor skill practice improves learning and skill acquisition. Little information is available to quantify how much feedback is necessary to enhance acquisition and retention of motor skills in children with CP (7).
It has been established, however, that the amount of motor learning that occurs using the CPF is dependent on the amount of information provided. Previous research has tried to determine the optimal level of feedback, or physical guidance, to provide within the CPF, finding that too much or too little information will hinder learning a new motor skill in both children with spastic HCP and typically developing children(6). In other words, complete physical guidance (i.e., 100%) during motor learning prevents the individual from exploring new motor patterns and makes them more dependent and not able to utilize their own sensory information. Whereas limited physical guidance (i.e., 25% or 0%) impairs identification and development of appropriate patterns of motor skills. Thus, the amount of physical guidance provided should be at an optimal level to decrease dependency and optimize identification of appropriate movement patterns. This optimal level of guidance results in a self-regulatory integration of intrinsic feedback stimulated by extrinsic information received through physical guidance to develop new motor skills, thereby improving performance and retention of the motor pattern (10). Thus, the CPF strives to optimize learning by appropriately increasing task difficulty by controlling how much information the patient receives during training (9).
The ability to improve motor skills to enhance postural control in children with HCP is challenging because of the need to respond to multi-directional stimuli appropriately and in a timely manner. Children with HCP, however, may benefit from CPF training. In addition to the description above, the CPF relies on contextual interference and feedback, which has been stated as an effective strategy to improve gait and balance in individuals with CP (7). Previously, the CPF has been shown to be effective in the rehabilitation of people with stroke and Parkinson’s disease (PD) (8). Since children with HCP suffer from functional impairments similar to people with stroke and PD, it can be hypothesized that the CPF may also help these children. But despite the needs of children with HCP, no similar research has been conducted in regard to regaining balance.
Thus, the aim of the present study was to investigate the role of the CPF in improving stepping reaction (step length and reaction rate) and to strengthen the maintenance of balance in children with HCP.
Materials and methods
Participants
Nine children aged 4–12 years with HCP referred to physical therapy clinics were enrolled. Inclusion criteria were: 1) aged 4–12 years at the time of enrollment, 2) the ability to walk without the help of an assistive device for at least six minutes, 3) the ability to understand and follow the therapist’s guidelines, and 4) presence of mild to moderate impairment (Gross Motor Function Classification System [GMFCS] levels I-III) (7). Potential participants were excluded if they had any disease that interfered with the study process, such as heart disease or severe vision or hearing problems (9). Individuals who did not attend three consecutive sessions or refused to complete the training sessions did not have their data analyzed in the case series. GMFCS level of the children with HCP was determined by a pediatrician.
All procedures and objectives of the study were explained to parents through an occupational therapist and then the project executor. The protocol was retrospectively registered at the Iranian Registry of Clinical Trials website (https://www.irct.ir/trial/50748[50748]) with ID number IRCT20200905048619N1. Parents of the participants signed a written consent form (Ethics number of IR.KHU.REC.1398.019).
Procedure
Demographic information including height, body mass, age, history, type of disease, duration of treatment, accompanying disorders, etc., was given by the participant’s parents or their occupational therapist. Two identical baseline testing sessions were performed separated by 3 weeks to account for differences in growth and maturation that may have occurred in the enrolled participants. Testing sessions were conducted at the same time of day. The Pediatric Balance Scale (PBS) test was used to assess dynamic and static balance, and the stepping reaction test assessed the reaction time and step length to maintain balance when falling (1). Two days after the second baseline test, participants began a 12-session training protocol. The training exercises lasted for 6 weeks with 2 sessions each week. The duration of each session was 45 minutes. Following completion of the intervention, participants performed a post-intervention testing session that was identical to the baseline testing sessions. This was a preliminary study on the use of the CPF in young patients with HCP, thus children were not randomized into groups for the intervention and no control group was included.
Outcome measures
Stepping reaction (step length and reaction rate)
In this study, the stimulus that triggered the stepping reaction was an internal stimulus. The participant stood upright and was asked to bend from the ankle joint in four directions: forward, backward, right, and left. Participants were asked not to try to prevent falling but to allow themselves to lean far enough that they felt they had to take a step to prevent from falling. During the assessment sessions, the steps taken when leaning forward and backward had to be by the paretic leg. Since the objective of the study was to improve stepping reaction, no lead leg was assigned in lateral leaning, although most participants stepped with their non-paretic leg in lateral leaning control which helped them to react faster and more efficiently. On the contrary, when participants stepped with their paretic leg, they took shorter steps and needed more steps to regain balance. The purpose was not to model real-life situations but to use the center of mass outside the base of support as a stimulus to take steps in multiple directions to prevent falling (1). To reduce the fear of falling, participants were encouraged by the occupational therapist to concentrate on increasing the speed and length of the stepping reaction so as not to pay attention to the limits of their stability. However, the occupational therapist watched participants and ensured they were not just stepping quickly and were following the instruction to lean far enough that they felt they needed to take a step. Participants were given similar exercises for both healthy and paretic legs as the initial stepping leg in maintaining balance. Although they could take as many steps as they needed to regain balance, participants were encouraged to keep their balance in just two to three steps. When performing the lateral leaning task, no lead leg was identified, and participants were allowed to take steps using the contralateral or ipsilateral leg (1).
Each trial was captured using a Canon SX100 camera so that step length and reaction rate could be determined. Step length was defined as the distance between the starting position and the position after the first step was taken. Measurement was recorded in centimeters and did not include the foot length. The reaction rate was evaluated from the moment balance was disturbed (when one foot was off the floor after leaning enough) to the moment when both feet were on the ground after the first step. This time interval was calculated in Tracker (Video Manual Motion Tracker 1.0) software in seconds and averaged over the three repetitions.
To aid in data extraction, special markers were attached to the heels and thumbs of the participants, and the camera was placed perpendicular to the movement surface to record the movements of the markers. This time-motion analysis utilized the Video Manual Motion Tracker 1.0 software package. This technique is based on the inverse projection of the real plane of the field, recorded by a video camera, and then transferred onto the plane of an electronic tablet after importing the video into the software. The calibration processes transfer the real measures onto a computer model to ensure that the measures overlap. Then, the observer manually copies the movement trajectory of a participant using an electronic pen on an electronic tablet during the movement. The system saves each point of the participants’ movement trajectory, which is defined by a set of values (X, Y, t), where X and Y are the orthogonal coordinate axes in the screen plane and t is time. This method enables the recording of the total distance covered as well as the immediate and average velocities of the participants during the movement. Reliability of these methods has been previously established for both intra-observer (intraclass correlation coefficient [ICC] = 0.999) and inter-observer (Pearson product-moment correlation r = 0.994) (14).
Balance
In the present study, the PBS test was used to assess static and dynamic balance (10). This test consists of 14 practical test items, including transitioning from sitting to standing, turning 360 degrees, and reaching with an outstretched arm. Each item is scored from 0 to 4, and the total scores are calculated from 56 possible points. Higher scores indicate better performance. The test-retest and inter-rater reliability are both high for the PBS (ICC = 0.99) (16).
Interventions
The step reaction task used in the assessment was also used in the intervention with the same instructions. The focus of the study was to improve regaining balance through learning, not just rehabilitating the paretic leg; therefore, both healthy and paretic legs served as the initial stepping leg in maintaining balance. To encourage maximal effort and reduce fear of falling, participants wore a seat belt around their waist that was controlled by the occupational therapist.
Exercises were performed twice a week for six weeks, for 45 minutes each session. Exercises were performed in three stages. Participants completed the stepping task in each stage until they met their optimal step length obtained from baseline data, at which point they were asked to practice with a new challenge. It was expected that the step length would decrease as the exercise became more difficult.
In the first stage, the participants performed blocked practice (not random practice) in all directions to optimize the initial acquisition of the motor learning with both legs. They practiced three sets of 60 repetitions (10 repetitions with each leg in each forward, backward, right side and left side) with brief rest periods in a standing position between repetitions and a seated rest period of approximately 5 minutes between sets.
In the second stage, exercises were done randomly in two sets of 60 repetitions to enhance motor learning (30 random repetitions in each forward and backward directions). In this stage, the children received more information during the exercises to know which foot to start with. Moreover, with the aim of increasing the difficulty of the functional exercise, children were asked to hold a half-full glass of water during exercises as an extra challenge in addition to randomness in this stage. New challenges added in the second stage increased the reaction time, and with more practice, the children could achieve better reaction time (1).
In the third stage, the training consisted of stepping with only the affected leg in two sets of 40 repetitions (20 repetitions in each forward and backward directions). In this stage, children were asked to start the task with their eyes closed and open their eyes when they felt disturbed and wanted to take a step (1).
Physical support from the seat belt and support from the therapist was reduced to just the belt and then the support of the therapist without the belt in each progression of the task. Feedback from the occupational therapist included instructions such as “walk faster” or “take longer steps” (the exact amount was not specified because subjects had different rehabilitation procedures, and it was not possible to determine an exact criteria). Feedback was guided by the principle of value of error estimation. Specifically, participants were asked their opinion of the quality of their stepping task performance and the therapist provided feedback based on the participant’s response. The therapist initiated this discussion with the participant if they observed that progression was hindered by repetition of errors. Additionally, feedback was tapered by the therapist at each level of functional task difficulty such that feedback was initially provided after 5 repetitions within each block tapered to 10 repetitions or following 6 tapered to 30 tapered again to 60 repetitions during random practice (1). Feedback from the therapist was provided to improve the response (1) and was decreased as repetitions progressed such that only feedback related to the movement was given to the patient in the final sessions.
Statistical analysis
Descriptive statistics including mean and standard deviation were used to analyze the data. The Shapiro-Wilk test was used to investigate the normal distribution of data, and equality of variance was determined using Levene’s test. Repeated measures ANOVAs were then performed to determine differences between each testing time point (pre-test 1, pre-test 2, and post-test), and t-tests were then used if there was a significant omnibus p-value. An alpha of 0.05 was used for all tests of statistical significance. The minimal detectable change (MDC) at the 90% confidence interval (CI) was calculated from the pre-test 1 and pre-test 2 data using the following formula to indicate the minimal change between 2 measurements required for the change to be considered a real change: MDC = 1.65×SEM×√2, in which SEM is the standard error of measurement. Effect sizes (ESs) and 95% CIs were then calculated to provide a measure of clinical meaningfulness. Cohen’s d ES statistic was subsequently calculated by dividing the difference between the means (pre-test 2 and post-test) by the standard deviation from the baseline time point. Finally, ESs of 0.2, 0.5, and 0.8 were respectively considered ‘small,’ ‘moderate,’ and ‘large’ (17). As in many cases, p-values and indicators of statistical significance alone did not answer the questions of primary interest. Such questions typically involve making decisions under conditions of uncertainty. Because that was the case, point estimates and measures of uncertainty in the form of CIs were more informative summary statistics (18). Therefore, the 95% bootstrap CIs of means difference were used to confirm and guarantee the results. On the other hand, the main idea behind the bootstrap was that, in some situations, it is better to make inferences about the population parameters using only the data at hand, without making assumptions about underlying distributions (19).
SPSS software version 22 was used for statistical analysis (IBM Corp., Armonk, NY, USA).
Results
Baseline characteristics
The mean and standard deviation of the demographic and general characteristics of the subjects are presented in Table 1. In the end, nine participants accomplished all 12 sessions (Fig. 1).
Demographic and baseline characteristics of subjects
Demographic and baseline characteristics of subjects
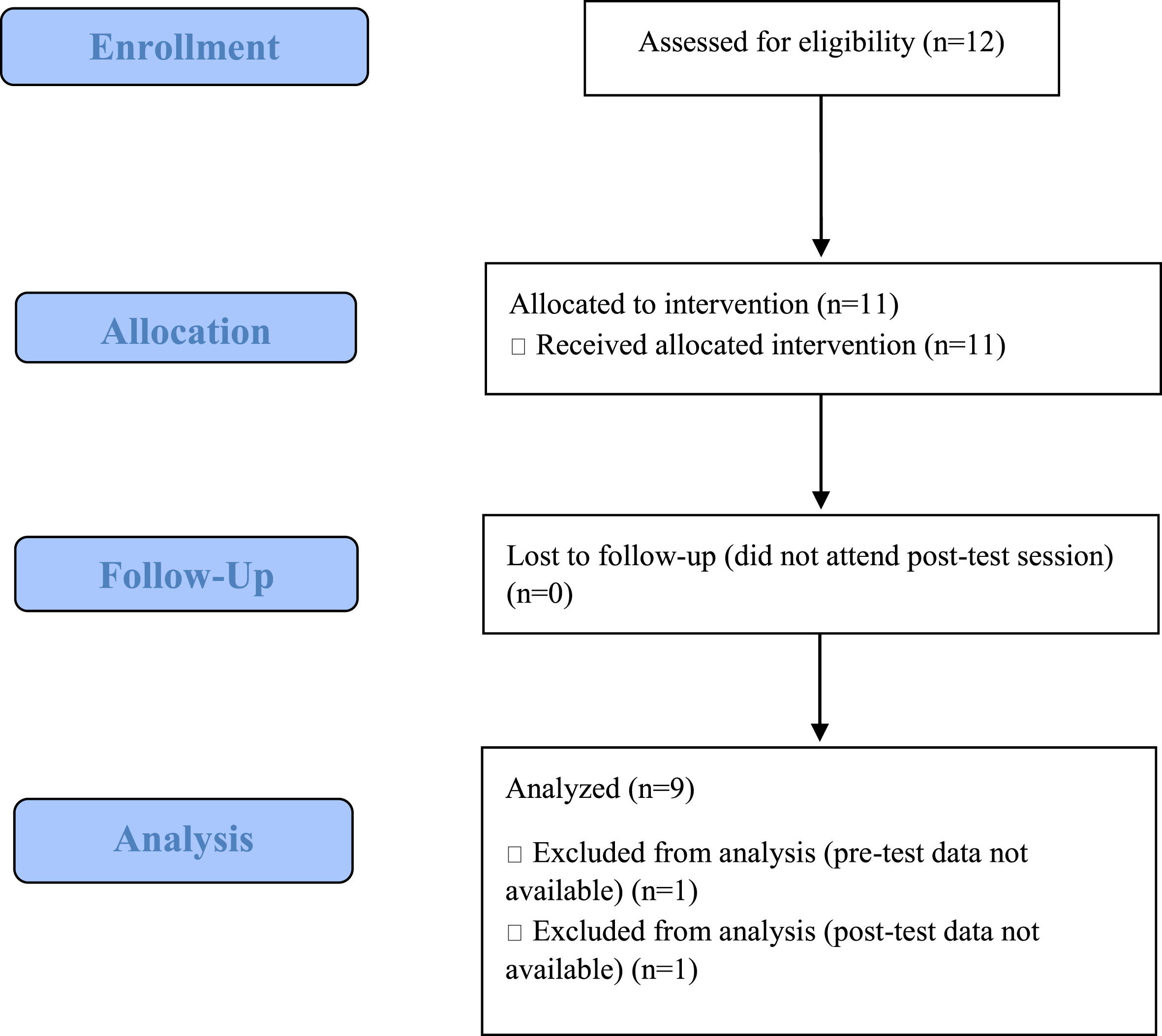
Study flow diagram.
Many participants scored a zero for the stepping tests at pre-test. Specifically, 11 participants effectively completed (i.e., received scores on) the pre-test static and dynamic balance assessments; 9 effectively completed the pre-test forward stepping reaction rate, backward stepping reaction rate, lateral stepping reaction rate, and lateral stepping reaction length assessments; and 8 effectively completed the pre-test forward stepping reaction length and backward stepping reaction length tasks. The two individuals who could not perform the majority of tasks at pre-test were removed from the analysis (Table 2).
Descriptive statistics
PBS: Pediatric Balance Scale.
The results of the Shapiro-Wilk test indicated normal data distribution (balance, P = 0.081, step length, P = 0.088; backward, P = 0.121; and lateral, P = 0.219), and reaction rate (forward, p = 0.329; backward, p = 0.387; and lateral, p = 0.148).
The bootstrap method was used to find 95% CIs for the means difference pre-test 1 and pre-test 2, pre-test 2 and post-test, and post-test and pre-test 1 (pairwise comparisons).
Based on 1,000 samples given by a simple random sampling method with replacement, the 95% bootstrap CIs of means differences were performed by percentile bootstrap method.
In general, it was found that the CPF is effective in improving gait (gait length and reaction speed) and enhancing balance in children with HCP (all differences in post-test and pre-test 1 are in incremental gait variables and decreasing in response speed). This is a good result, as is the case with the pairwise comparison of the post-test and pre-test 2. Some variables for the pairwise comparison of the pre-test 1 and pre-test 2 did not see these positive results, which it can be said that no change occurred; these variables are denoted in red in Table 3.
Bootstrap for one-sample test
aUnless otherwise noted, bootstrap results are based on 1,000 bootstrap samples. bBased on 998 samples. cBased on 999 samples. dBased on 997 samples. *Indicates significant differences.
Mauchly’s test was significant for all variables, i.e., the variance of the different steps was not equal for all variables. Therefore, the Mauchly’s sphericity assumption and Huynh-Feldt tests were used. In conjunction with pairwise comparisons, the results suggest that there were significant differences between the values of variables in the pre-test 2 and post-test and the pre-test 1 and post-test time points. These results are also objectively visible in the profile plot diagrams and the error bars on the estimated means (Figs. 2–4).
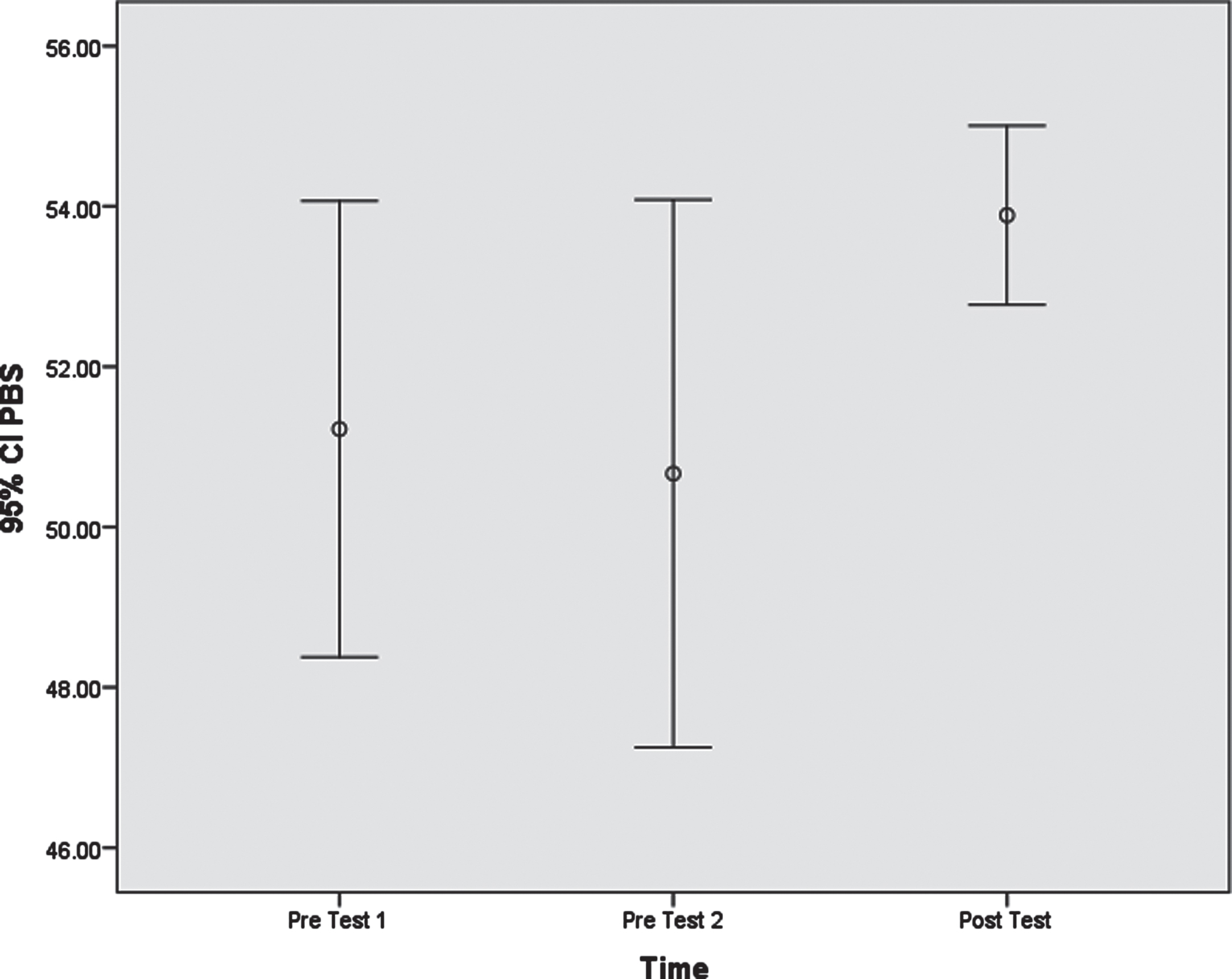
Error bars on the estimated means of the Pediatric Balance Scale.
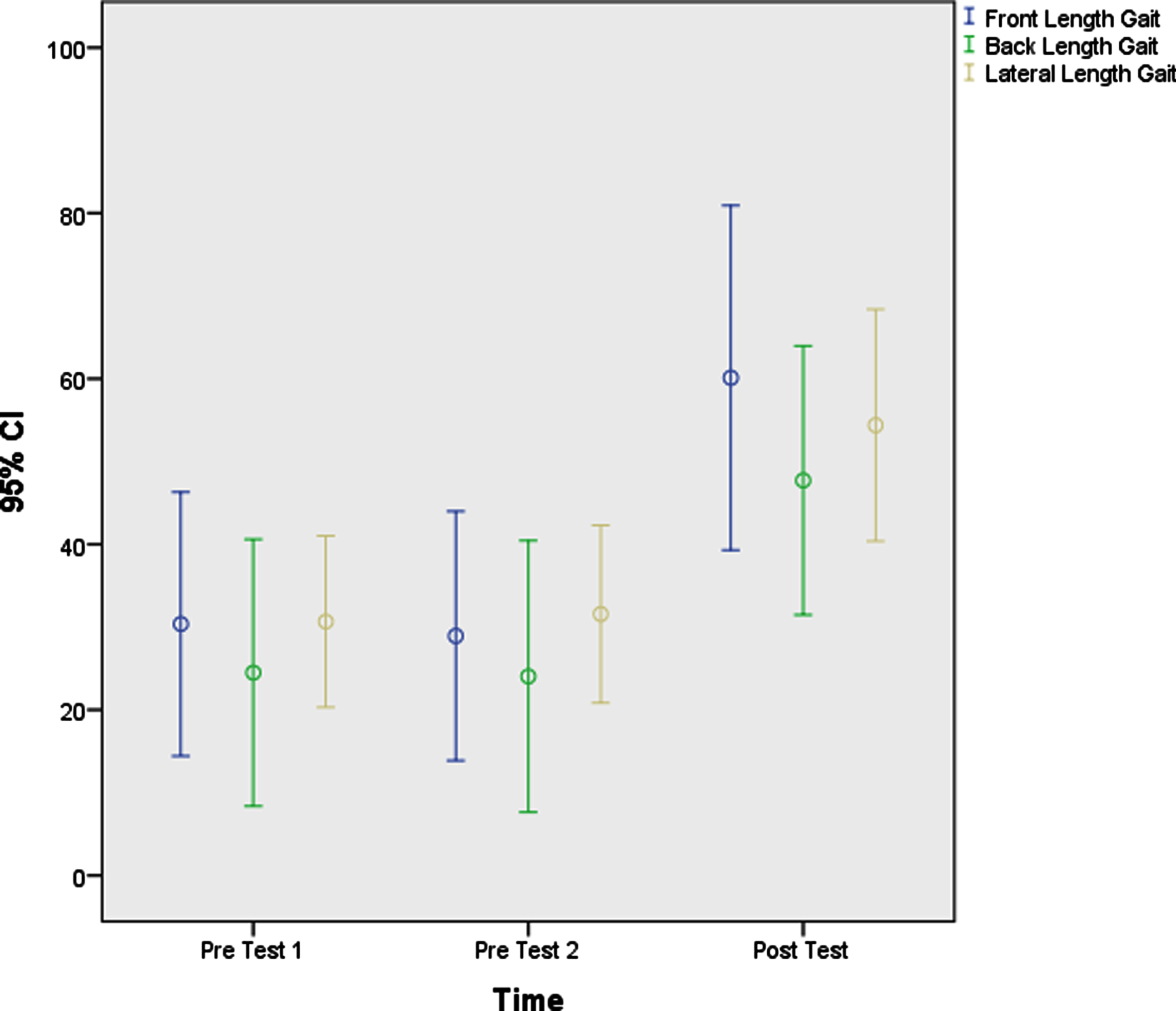
Error bars on the estimated means of length gait (Front, Back, Lateral).
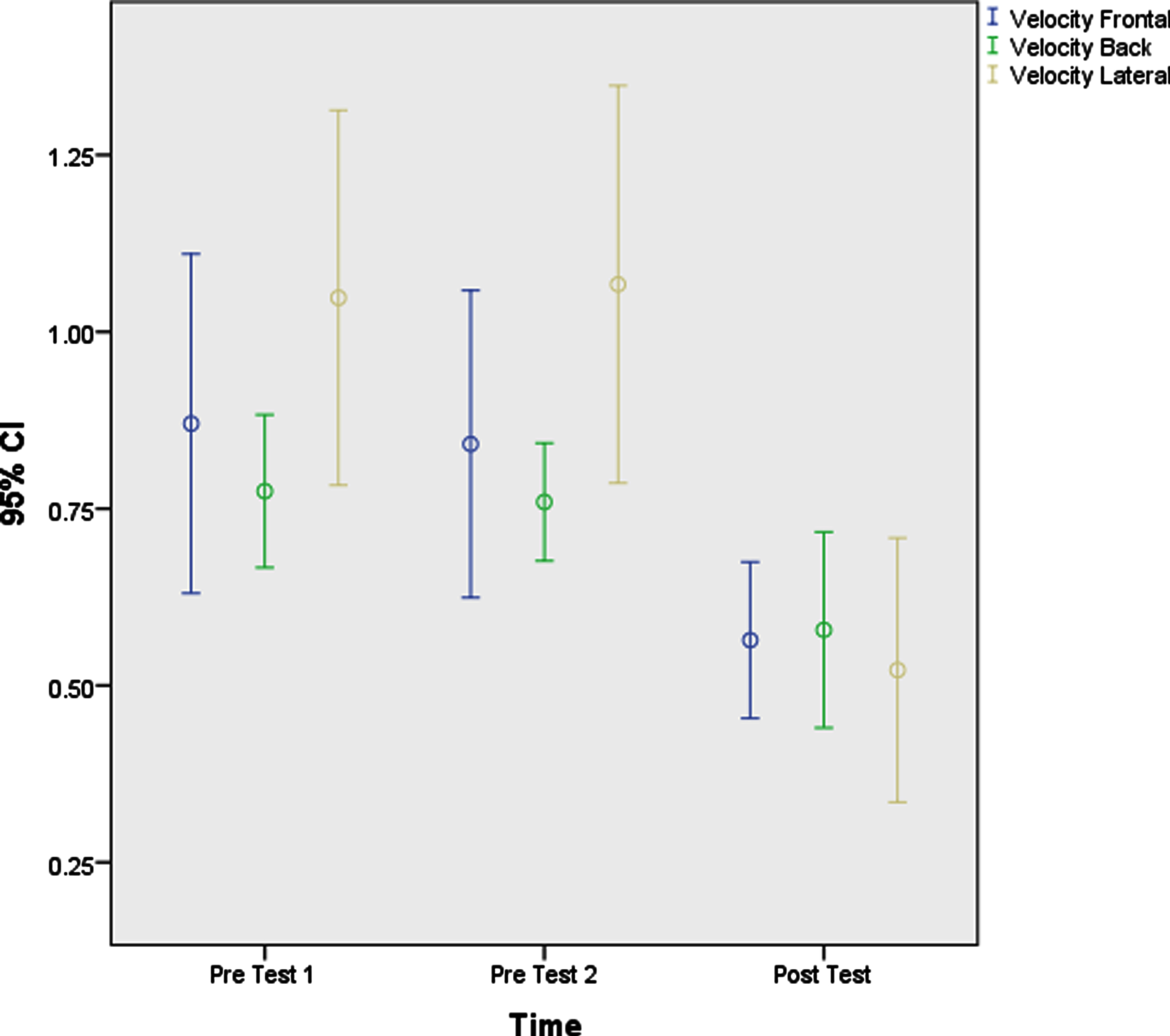
Error bars on the estimated means of velocity (Front, Back, Lateral).
The MDC for the forward stepping reaction was 0.23 s. The change from pre-test to post-test exceeded the MDC for 7/9 participants (64%). The MDC for backward stepping reaction was 0.13. This change was exceeded from pre-test to post-test by 7/9 participants (64%). The change from pre-test to post-test exceeded the MDC of 0.37 s in 8/9 participants (73%). The MDC for forward stepping reaction length was 15.2 cm. This change was exceeded by 6/9 participants (55%). Notably, 8/9 participants’ (73%) changes in backward stepping length reactions exceeded the MDC of 13.6 cm. The MDC for lateral stepping reaction length was 14.4 cm. This change was exceeded by 6/9 participants (55%). The MDC for balance was considered≥2.4 points. Importantly, 8/9 participants exceeded the MDC for this variable (73%).
Discussion
The purpose of the present study was to investigate the role of the CPF in improving stepping reaction (step length and reaction rate) and to strengthen the maintenance of balance in children with HCP. Results demonstrated significant improvement in step length and reaction time of the paretic leg and static and dynamic balance after CPF intervention in children with HCP with medium to large ESs. The children could regain balance using their non-paretic leg, but they might experience a situation in which they cannot use it instantly. In this study, the goal was to improve children’s ability to regain balance after a disturbance by taking a step with either leg in such a situation. They were given exercises for both legs in training sessions but assessment was done for the paretic leg (in leaning laterally, no lead leg was assigned). Similar outcomes have been reported in patients after stroke and those with PD (1,12). Importantly, at the individual participant level, over 55% of children improved stepping reaction time and/or step length at post-test compared to baseline. To the investigators’ knowledge, this study was the first to investigate the CPF in children with HCP.
According to the CPF, the impact of provided feedback on motor skill acquisition and knowledge of performance is dependent on the type, timing, and meaningfulness of the information provided (5). In this study, only verbal feedback was used. All children (typically developing and with CP) can benefit from practice with augmented feedback when learning a motor task (10). Hemayattalab and Rostami compared retention of throwing skills in children with HCP who practiced in 100%, 50%, and no feedback conditions. Those who practiced with 50% feedback performed with the least error, suggesting that increased feedback may interfere with motor learning. According to these findings, full feedback was not used (11).
The content and scheduling of augmented verbal feedback from the physical therapist were designed to assist in initial problem solving and then tapered to avoid the possibility that they might interfere with motor learning as skill level progressed. In the first week of practice, information was provided to the participants regarding an effective stepping reaction requiring sufficient speed and length to control the momentum of the body. This information set the parameters for the content of feedback during the remainder of practice. Participants were provided information regarding 2 aspects of the stepping reaction. The first was knowledge of the results of the stepping reaction (the occurrence of a fall or not) through information inherent in the task (the pull of the seat belt) and verbal feedback regarding the level of assistance required. The second was knowledge of the performance of the stepping reaction through qualitative verbal feedback about the speed and amplitude of the initial and follow-up steps observed by the treating physical therapist, for example, “steps need to be faster” or “try stepping further” (no absolute values of distance or speed were provided). Because participants had different levels of motor recovery and progressed through training at different rates, individualized augmented feedback was provided to adjust the optimal challenge for each learner. Additionally, the provision of verbal feedback during the task was guided by the principle of the value of error estimation combined with knowledge of the results to enhance motor learning. Feedback was added after each participant was asked to provide an opinion about the quality of their performance of the stepping reaction. The therapist initiated discussion with the participant if progression appeared to be hampered by repetition of errors. At each level of functional task difficulty, feedback was tapered by the therapist (approximate progression: following 5 then 10 repetitions during blocked practice, and following 6 then 30 then 60 repetitions during random practice) (1).
It has been shown that people with chronic stroke (>6 months) demonstrated impaired implicit learning during a serial reaction time task performed with the limb ipsilateral to the lesion. The impaired motor learning was attenuated somewhat by the provision of explicit information regarding the sequential pattern that was being learned. Boyd and Winstein have suggested that the improvement noted in their study may have been due to the simplicity of the rules governing the “to-be-learned” serial motor task (20). The requirement to take faster or longer steps in the current study might be easier than sequential instruction with precise, kinematic information (e.g., description of how to move the joints of the limb specifically). Thus, it is possible that the simplistic nature of the feedback in the present treatment strategy contributed positively to motor learning as demonstrated through improved task performance.
In terms of static and dynamic balance, the CPF improved both outcomes at post-test compared to both pre-test time points; however, the effect sizes were small. Choi et al. investigated the effect of a motor learning task using a treadmill on balance in children with spastic CP and reported the superiority of the motor learning task over control participants in balance improvement (21). Nearly 75% of the participants in the current study improved their balance using the CPF system. The CPF reinforces learning based on the level of information provided during performance (1). It can be assumed that information poses a challenge to the individual, and that knowledge of performance increases when information is provided. Simple commands, such as requests to take longer or faster steps, can be more effective than providing accurate and detailed kinematic information (such as accuracy in joint movements) (1). Therefore, presenting simple feedback in the present study could have had a positive effect on motor learning and balance performance.
Practice is the most important factor influencing the continuity of skill improvement and motor learning. In fact, it has been demonstrated that the amount of practice is directly related to the development of skills (5). In the present study, instead of doing a variety of exercises, patients continued repetition of a specific exercise using the CPF such that it might improve learning motor skills. It is also important to acknowledge that learning occurs through committing errors, especially when the level of exercise difficulty is controlled in a way to increase learning. In the present study, the error correction method was used. In the controlled stepping reaction, the error was falling to the ground. Children did not experience a fall as their physical support diminished gradually as they progressed. Only two children, both classified as GMFCS level III, fell several times during training due to severe spasticity in the affected leg. According to the theories and information provided in postural control and the principles of motor learning and the CPF, participants performed blocked exercises in early stages with the least challenge and then improved their performance through random exercises. As children developed their skills, feedback was given less and less frequently, so they could find the solution to their problems and correct themselves in future repetitions.
The present study has some limitations. First, caution should be taken in interpreting and generalizing the results of this study, as the present study was conducted on a small sample size. Second, there was no control or typically developing group. An important limitation regarding bootstrapping analysis is that it may destabilize the CIs and increase Type I error risk when the sample size is small, as was the case with this study. However, the various modes of analysis in this paper holistically present an accurate representation of the data for use in development of future, larger scale trials. Future studies with larger sample sizes and control groups should be conducted.
A third limitation was the lack of a crossover task that made it unclear if the intervention would carry over to other balance-demanding activities. This study was performed to demonstrate that use of the CPF is possible in children with HCP and lay the groundwork for future studies using larger sample sizes and a randomized, controlled trial design. Despite the present limitations, the CPF appears promising for use in children with HCP.
Conclusion
The results of the present study showed that balance, step length, and step time all improved in children with HCP following the present CPF intervention. The use of CPF principles is recommended in future research focusing on balance in children with cerebral palsy.
Footnotes
Acknowledgments
The authors have no acknowledgements.
Conflict of interest
The authors have no conflicts of interest to report.
Ethical considerations
This study was approved by the Institutional Review Board at Kharazmi University (IR.KHU.REC.1398.019) on July 28, 2019.
Funding
No funding.