
Abstract
PURPOSE:
Hip displacement impacts quality of life for many children with cerebral palsy (CP). While early detection can help avoid dislocation and late-stage surgery, formalized surveillance programs are not ubiquitous. This study aimed to examine: 1) surgical practices around pediatric hip displacement for children with CP in a region without formalized hip surveillance; and 2) utility of MP compared to traditional radiology reporting for quantifying displacement.
METHODS:
A retrospective chart review examined hip displacement surgeries performed on children with CP between 2007–2016. Surgeries were classified as preventative, reconstructive, or salvage. Pre- and post-operative migration percentage (MP) was calculated for available radiographs using a mobile application and compared using Wilcoxon Signed Ranks test. MPs were also compared with descriptions in the corresponding radiology reports using directed and conventional content analyses.
RESULTS:
Data from 67 children (115 surgical hips) were included. Primary surgery types included preventative (63.5% hips), reconstructive (36.5%), or salvage (0%). For the 92 hips with both radiology reports and radiographs available, reports contained a range of descriptors that inconsistently reflected the retrospectively-calculated MPs.
CONCLUSION:
Current radiology reporting practices do not appear to effectively describe hip displacement for children with CP. Therefore, standardized reporting of MP is recommended.
Keywords
Introduction
Cerebral palsy (CP) is the most common motor impairment in childhood with an overall prevalence estimated at 2.11/1000 live births [1]. Hip displacement is the second most common orthopedic deformity in children with CP [2]. There is a negative correlation between the severity of displacement, measured by migration percentage (MP) and quality of life (particularly in the domains of health status, communication, and social participation) [3]. By the time hip displacement is clinically recognized, degenerative changes may already require extensive surgeries [3]. Early detection of hip subluxation may reduce invasive surgical interventions, prevent dislocation, and improve outcomes for these children [3]. In addition to potentially alleviating patient morbidity, such outcomes may also benefit healthcare systems by reducing surgical costs [4, 5, 6].
Hip surveillance is the process of identifying and monitoring progressive hip displacement through screening radiographs and clinical examinations at standardized intervals, determined by motor impairment (i.e., higher Gross Motor Function Classification System (GMFCS) [7]. levels, e.g., Levels IV and V, require more frequent surveillance). Surveillance aims to facilitate referral to an orthopedic surgeon at the first signs of hip displacement (e.g., pain, reduced range of motion, radiological evidence of displacement). Reimer’s Hip MP [8] – a radiological measurement of the femoral head’s containment within the acetabulum [9] – is a key measurement to guide clinical decision making and prognosis for hip displacement [10]. Hips with MP
Hip surveillance programs have been implemented in several regions worldwide and, in some cases, have virtually eliminated hip dislocation and the need for late-stage salvage surgeries [3]. Despite the success of hip surveillance programs, they have not been universally implemented; for example, no formal monitoring program existed in the Canadian province of Saskatchewan prior to 2017. The purpose of this retrospective chart review was to understand pre-surveillance surgical practices for hip displacement in the province. A secondary aim was to examine the utility of Reimer’s Hip MP in comparison to traditional radiology reporting for the purposes of hip surveillance.
Methods
A retrospective chart review was conducted to describe the type and number of primary and subsequent hip surgeries performed on children with CP and hip displacement in Saskatchewan from 2007 to 2016. This study was reviewed and approved on ethical grounds, with a waiver of informed consent granted by the research ethics board of the former Regina Qu’Appelle Health Region (REB 19–29).
Patients were identified via discharge abstract database coding (ICD 10 diagnostic codes G80.0, G80.1, G80.2, G80.3, G80.4, G80.8, G80.9) from the province’s two urban hospital sites that provide surgical care for children with CP and hip displacement. Inclusion criteria were:
Data were collected from electronic and paper medical charts, and entered into REDCap [12] by one investigator at each site. To improve methodological consistency, the senior author completed collection for the initial five files with each of the two investigators at their respective sites. The data collection tool included: home health region, sex, age at surgery, GMFCS level, CP type (topographical and movement disorder), surgical purpose, pre- and post-operative descriptive radiology report findings, and number of subsequent surgeries (i.e., to manage ongoing subluxation and/or remove surgical hardware). Surgical purpose was recorded as either preventative (i.e., lengthening of hip adductors or iliopsoas, or obturator neurectomy), reconstructive (i.e., femoral varus derotation osteotomy or pelvic osteotomy), or salvage (i.e., arthrodesis, femoral head resection with valgus osteotomy, proximal femoral resection with soft-tissue interposition, or replacement arthroplasty) [13].
MP was retrospectively calculated for all available radiographs (pre- and/or post-operative) by one investigator using a mobile phone and HipScreen Application (www.hipscreen.org, Shriners Hospitals for Children, Sacramento, California). This application uses the camera and touchscreen of a mobile device to allow users to position the image of the hip on an MP ruler and calculate the amount of displacement. It has excellent inter-rater (ICC 0.972 to 0.989) and intra-rater reliability (ICC 0.976 to 0.989) for determining MP in children with CP [14].
Data analysis
Hip surgery and MP data were examined for normality. Parametric (normally-distributed) data are presented as frequencies, mean, and percentages. Non-parametric data are presented as median and interquartile range. Wilcoxon Signed Ranks Test examined differences between pre- and post-operative MPs. Right and left hips were separated in the analysis due to dependence of data. Significance was set at
One investigator performed a combination of conventional and directed content analysis [15] to code descriptive data for radiology report findings for those with a corresponding radiology image available. Coding was done using NVivo Version 12 (QSR International Pty Ltd), and key words were inductively grouped into categories and preliminary themes to describe the content of the reports. As well, key words and phrases describing the extent of displacement were compared with the MP for the corresponding radiograph and grouped according to whether the MP was 0–29% (low risk of dislocation) or
Demographics (
67 patients)
Demographics (
A total of 87 charts were identified. Twenty patients were excluded as they did not meet inclusion criteria: fifteen had primary hip surgeries outside the study time frame, three underwent surgeries unrelated to hip displacement, one had no documented diagnosis of CP, and one chart was improperly purged.
Data from 67 patients (115 surgical hips) were analyzed (Table 1). Mean age at the time of primary surgery was 8.67
Primary and subsequent surgeries
Primary and subsequent surgeries
MP measurements for the 92 hips (41 children) with both radiographs and radiology reports available were:
Percentage of hips with pre- and post-operative MP of 0–29% and 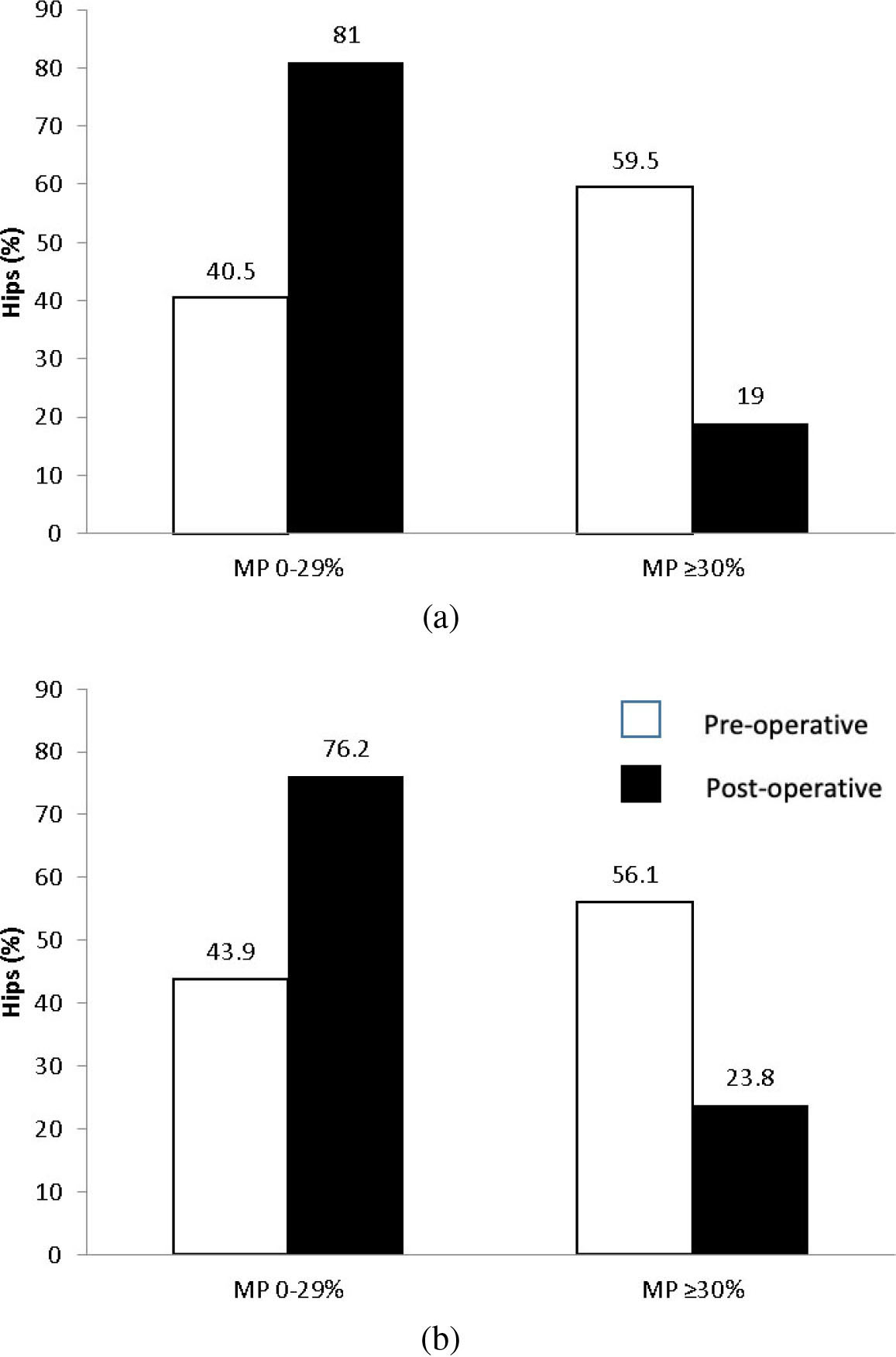
Radiologists described several aspects of the hip radiographs in their reports, including the shape and spatial orientation of the femoral head, neck, and/or acetabulum. The degree of displacement was described for 78/92 hips, and varied descriptors inconsistently reflected the MP (Table 3); these included: subluxation (34), dislocation (17), displacement (4), and migration (1). As well, radiologists often used qualifiers to describe the extent of displacement (e.g., “minimal”, “mild”, “moderate”, “severe”) or highlight a change from a previous radiograph. Some reports described the direction of displacement (primarily “superior-lateral”). MP was documented for two hips (one radiograph), and the degree of “coverage” was described as an absolute distance in four hips. Hip alignment was described as normal for 22 hips, of which 18 had an MP
Most common descriptors used in radiology reports to describe hip displacement and the number and range of MPs corresponding to those terms
When the radiology report descriptors were compared with the MPs and grouped according to whether the MP was 0–29%, 30–99%, or
1) MP was high enough to indicate clinical concern (i.e.,
2) MPs that were not high enough to cause clinical concern (
3) MP and report descriptors generally agreed. Agreement could only be confirmed quantitatively where the radiologist estimated or calculated the MP, or in extreme cases where retrospectively-calculated MP was a) 30–99% and the radiologist reported the hip was normal (18/92 radiographs), or b)
This study explored hip subluxation surgery in children with CP over a ten-year period in a Canadian province without a formalized hip surveillance program. During this time, 67 patients underwent primary hip surgery, consisting of mostly bilateral, preventative procedures. A majority of these procedures were performed on children with high GMFCS levels. Although no salvage surgeries were performed, seven hips (in 6 children) were dislocated at the time of primary surgery and two remained dislocated post-operatively. Radiology reports demonstrated that MP was reported for only one radiograph, and a range of descriptors was used to subjectively describe hip displacement, without meaningful relationship to the MP.
Several studies have documented surgical practices pre-and post-hip surveillance implementation. In Australia and Sweden, salvage procedures were discontinued shortly after implementation of surveillance practices [3, 4, 7, 8, 9, 10, 11] due to early identification and reduced incidence of dislocation. A more recent exploration of surgical care for children with CP GMFCS levels III-V, compared Sweden (a center with a surveillance program) and Norway (a center without surveillance) [16]; while the number of surgeries was similar between sites, the age at primary surgery was younger (5.7 vs. 7.6 years) and fewer number of dislocations occurred (1 vs 18) in Sweden. These findings imply that implementation of hip surveillance programs may reduce the incidence of hip dislocation and therefore the numbers of subsequent salvage surgeries.
Although a reduction in salvage surgeries has been described as a potential outcome of hip surveillance, none of the patients underwent salvage surgeries during our study period. It is possible that individual surgeon philosophy of care may have affected these outcomes. While no salvage surgeries were performed, six children (9.0%) had dislocation within our surgical based cohort, which is much higher than the 2.5% of children reported in a population-based study from Scotland (a country with a hip surveillance program) [17] and similar to the 9% dislocation rate observed in Sweden prior to implementation of hip surveillance [4]. These discrepancies in results may be due to sample size differences in studies. Although salvage surgeries can reduce pain, they are associated with complications [10]; therefore, it is also possible that patients/families of children with dislocation declined the procedure, the child’s overall health status precluded surgery, or surgeons recommended alternate approaches. Furthermore, children in this sample were older at primary surgery than Elkamil and colleagues [16] reported in Sweden and Norway. Both age at primary surgery and incidence of dislocation may be important variables to monitor as surveillance programs are implemented.
Hip surveillance requires a multidisciplinary approach. Radiologists play a key role in successfully measuring and tracking hip displacement to inform clinical decision making. The term displacement has been used to refer to hips with MP
Limitations
Due to the province’s small population, our sample size was limited and these results should be compared to data from larger populations with caution. Given that this study examined a surgically-treated cohort, the true incidence of dislocation in children with CP in the province’s population was likely much higher than the data indicated. As well, patients lost to follow-up or accessing surgical interventions outside the study area were not reflected. Additionally, due to the long study period and retrospective design, changes in health care processes and technology may have impacted the data available. For example, only 92 hip radiology reports had radiographs available for MP measurement. Lastly, standardized radiographic patient positioning was likely not used, although it is recommended for accurate MP measurement. While positioning has not been shown to significantly impact the validity of results [20], the extent to which this may have affected calculation of MP in this study is unknown.
Future research is planned to evaluate the impact of implementing a CP hip surveillance program in this region. Additional studies may help to understand the role of surgeon/family preference in surgical decision making or radiologists’ perspectives in incorporating MP as part of a hip surveillance program.
Conclusion
This study described a variety of preventative and reconstructive procedures performed for hip displacement in a center without a formal hip surveillance program for children with CP. A significant number of hips had progressed to dislocation at the time of primary surgery, suggesting the potential value of implementing a hip surveillance program in this region. Radiology reporting practices did not consistently and effectively communicate the degree of hip displacement; therefore, routine reporting of MP is recommended to help inform care for children undergoing hip surveillance. This information may improve standardization of hip surveillance and ultimately outcomes for children with CP.
Footnotes
Acknowledgments
The authors would like to thank Dr. Matthew Pechey for his help with data collection along with the Health Information Management Services of the Former Regina Qu’Appelle Health Region for their support.
Conflict of interest
The authors have no conflicts of interest to disclose.