
Abstract
Purpose
This study aimed to evaluate long-term functional and radiological outcomes as well as parents’ perception of change and overall satisfaction following hip reconstructive surgery in children with cerebral palsy (CP).
Methods
Medical charts of children between three and 18 years of age with CP who had surgery between 1993 and 2014 by the same surgeon were reviewed. The study sample consisted of 44 children (Gross Motor Function Classification System levels I–V) aged 2–18 years representing 60 hips. Mean follow-up was 8.4 years [1.8–17.5]. A final follow-up evaluation was held to obtain post-operative anteroposterior pelvic radiographs and administer patient-reported outcomes to the caregivers.
Results
Care and Comfort Hypertonicity Questionnaire scores showed that 74–79% of caregivers reported no difficulty post-surgery in terms of child's pain or discomfort during position changes, when participating in general activities, or during sleep. The Lower Extremity Parent-Rated Change Form showed that 58–76% of caregivers reported a better status in their child's overall health, leg function, activity level, and pain post-surgery. Seventy-six percent of the caregivers indicated satisfaction with the overall changes since the surgery. For the 45 hips with both pre-operative and follow-up radiological outcomes, migration percentage improved significantly (p < 0.001) by 36.7%, and there was a 62.2% increase in the number of hips that were located post-operatively compared to pre-operatively. Acetabular coverage improved significantly (p < 0.001) from non-covered to covered in 46.7% of the hips and Shenton's line improved significantly (p < 0.001) from non-intact to intact in 66.7% of the hips.
Conclusion
Hip reconstructive surgery improved long-term functional and radiological outcomes, as well as quality of life for children and caregivers, while changes were perceived as satisfactory to the families. Evaluating pain, function, and satisfaction is important to measure the impact of hip reconstructive surgery on daily life.
Introduction
Cerebral palsy (CP) is a group of disorders that affect movement and muscle tone or posture. It is caused by damage to the immature, developing brain. In most countries, CP is the most common cause of lifelong physical disability with childhood onset, affecting about one in 500 newborns with an estimated prevalence of 17 million people worldwide. 1 Population based studies have shown that one in three children with CP will have hip displacement.2–4 Hip displacement affects both ambulating and non-ambulating children with CP. 1 A subluxated or dislocated hip can significantly decrease the function and quality of life of children with CP by reducing hip motion, impeding the ability to sit, walk and perform hygiene, and most importantly the associated pain.4–7 A direct relationship has been established between hip displacement, defined as a Reimers migration percentage (MP) greater than 30%, and a higher level of the Gross Motor Function Classification System (GMFCS).2,8 The risk of hip displacement increases with GMFCS levels and can reach as high as 64–90% in GMFCS level V.2,3,9
Hip surveillance programs have successfully achieved early detection and treatment of hip displacement. 10 Several studies have reported on the mid to long-term follow-up in children with CP who underwent unilateral or bilateral hip reconstruction surgery.11–14 In most instances, the design was a retrospective review with sample sizes ranging from 12 to 51 children of GMFCS levels III-V. The follow-up period ranged from 34 months to 25 years. Surgical management to restore the hip geometry and reduce pain is widely used with multiple articles reporting on the outcomes of various surgical techniques. 15 The main focus of these reports is on radiological outcomes. However, some reports included pain outcomes. Few studies have investigated functional outcomes and satisfaction following hip reconstructive surgery in children with CP. It was previously noted that when treating children with CP and complex needs, measurement of MP is not sufficient. Reliable quality of life measures are needed to further comprehend the impact of hip involvement and its treatment on children and their families.9,16
The objective of this study was to evaluate long-term functional and radiological outcomes as well as parents’ perception of change and overall satisfaction following hip reconstructive surgery in children with CP.
Methods
This was a non-controlled single-center retrospective study with a prospective cross-sectional follow-up conducted at the Shriners Hospital for Children (SHC)-Canada. Data on demographics, medical and surgical history, and pre-operative radiological findings were collected retrospectively from medical records. The parents were contacted by phone and asked to attend a final post-operative follow-up visit. The follow-up evaluation consisted of two patient-reported outcome measures (PROMs) and anteroposterior (AP) pelvic radiograph. The mean follow-up evaluation was 8.4 years [1.8–17.5].
Participants
Ninety-two (n = 92) children between two and 18 years of age with a diagnosis of CP who had a reconstructive or salvage hip surgery by the same surgeon at the SHC-Canada or the Montreal Children's Hospital during the period 1993 to 2014 had their charts reviewed to be included in the study. After removing those lost to follow-up, refusals, and death, 44 participants were included (Figure 1).
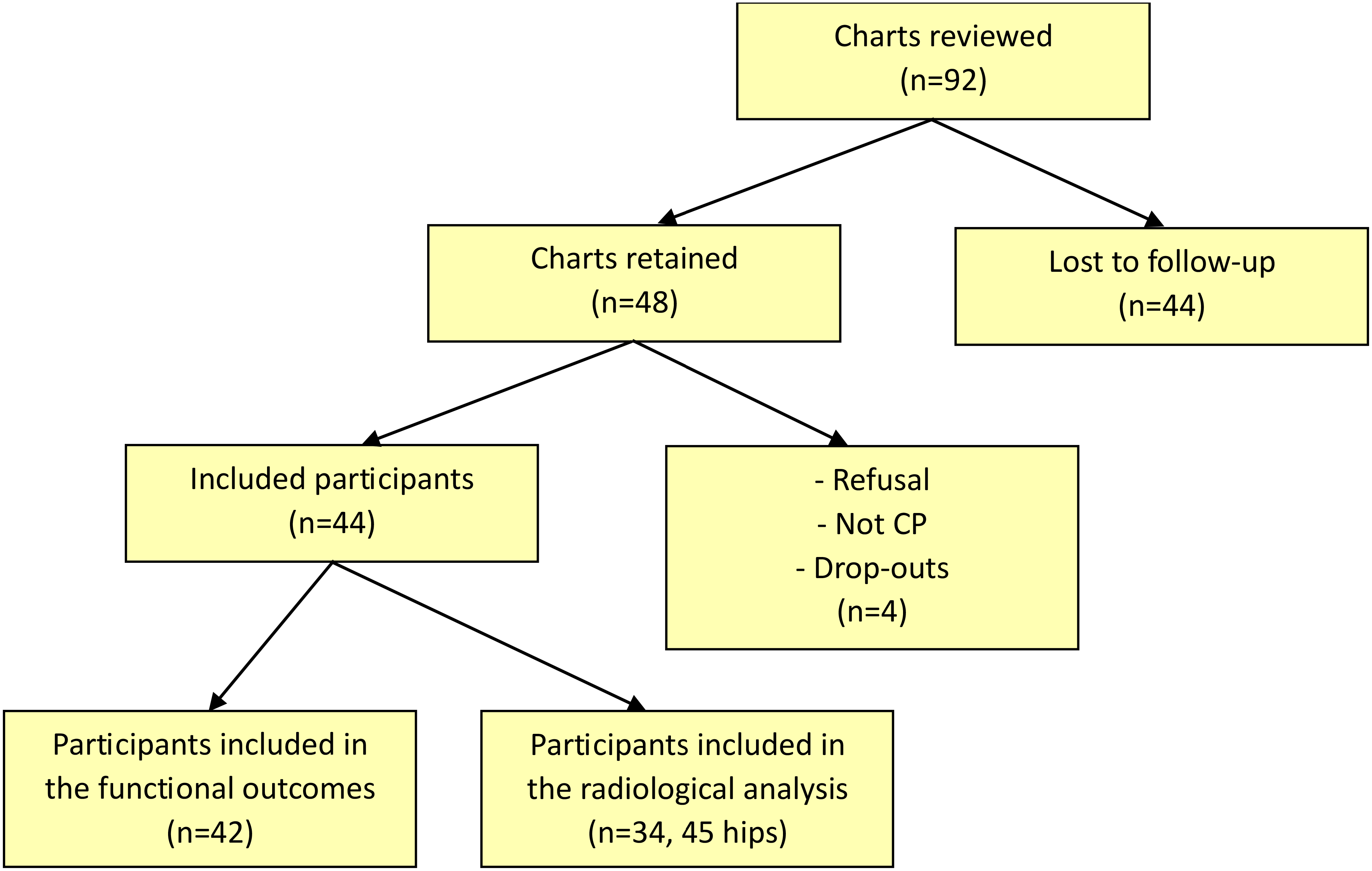
Participants recruitment flow chart. CP: cerebral palsy.
The surgical procedures performed included varus derotation osteotomy (VDRO) +/- Dega osteotomy, VDRO and Shelf, Dega osteotomy alone, and one of two salvage procedures: femoral head resection or valgus osteotomy. VDRO of the proximal femur is performed to reduce the femoral head into the acetabulum. The osteotomy and removal of wedge of bone medially recreates the normal neck shaft angle. The derotation component corrects the internal rotation of the femur that is present in most cases of dislocated hips in CP. After the VDRO, the hip is relocated in the acetabulum and stabilized with a plate and screws. To obtain satisfactory coverage of the femoral head, the shallow acetabulum is addressed by performing a Dega osteotomy in the supra acetabular area. Following this osteotomy, the distal part of the supra acetabular region is lowered and redirected to completely cover the femoral head. The wedge of bone taken from the femur is then grafted in the gap created by the opening of the Dega osteotomy. No internal fixation is necessary at that point.
If the acetabulum is too shallow, the Shelf procedure is indicated to cover the deficient acetabulum. A piece of bone is taken from the iliac crest and inserted in a groove in the supra acetabular region, with bone graft augmentation. This results in enlargement of the area and volume of the shallow acetabulum.
In some cases where reduction of the femoral head into the acetabulum is not feasible, complete excision of the proximal femur, including the femoral head, is indicated. Examples of surgical techniques are illustrated in Figure 2.
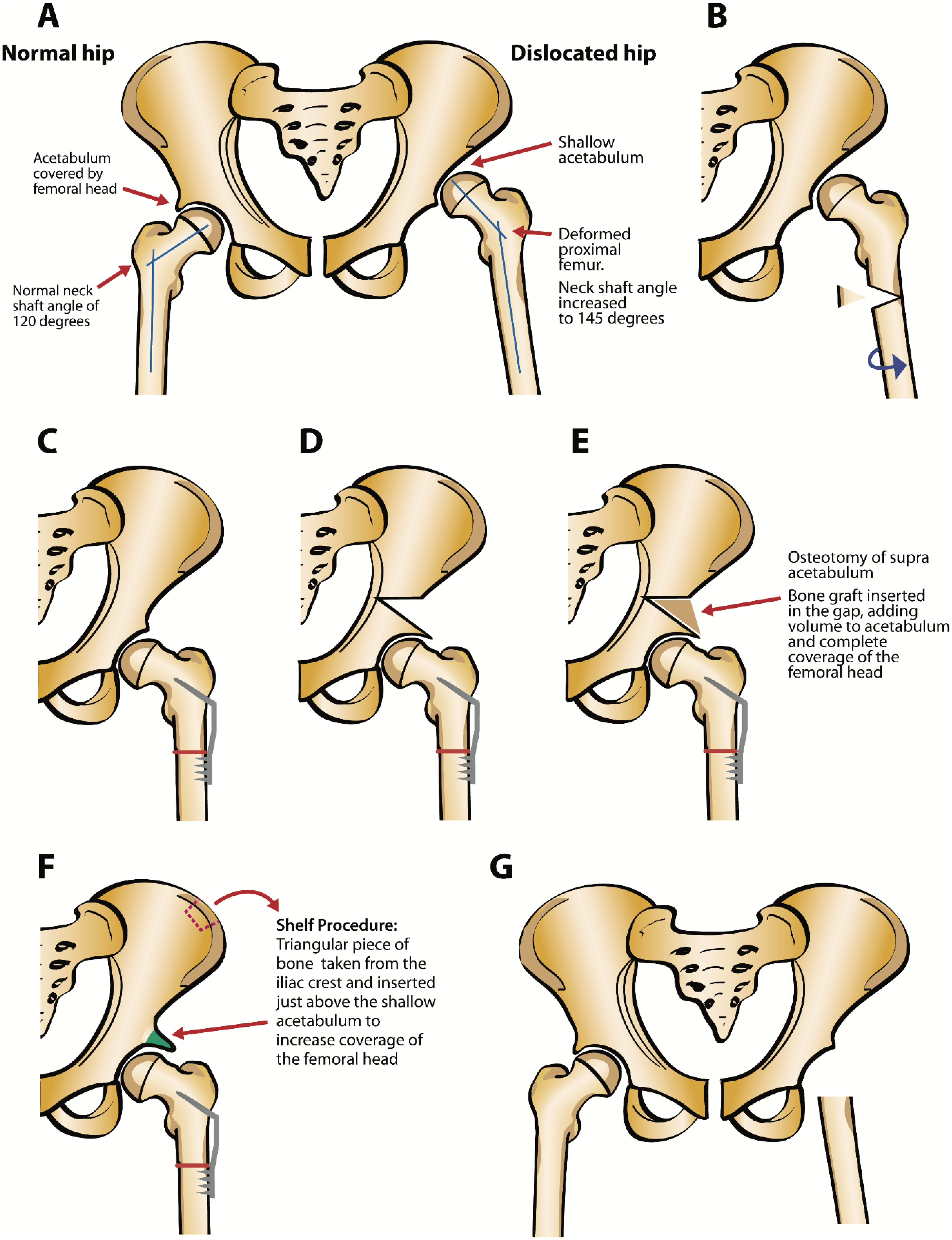
A) Normal and dislocated hip in cerebral palsy. B) Varus derotation osteotomy. C) Stabilization with plate and screws. D) Dega or supra acetabular osteotomy. E) Distal part of acetabular region lowered and bone graft inserted. F) Shelf procedure. G) Femoral head resection.
Ethics approval and consent to participate
This study received institutional approval by the Medical Research Department at SHC International and ethical approval by the Institutional Review Boards (IRBs) of SHC-Canada (McGill IRB study number A04-M49-13B). During the final follow-up appointment, a research assistant working with the orthopedic surgeon explained the study to the family and written consent was given by the family for those agreeing to participate.
PROMs
During the follow-up evaluation, the Care and Comfort Hypertonicity Questionnaire (CCHQ) was completed by the parents for non-ambulating children (GMFCS levels IV-V) to document the effects of hypertonicity on the function and quality of life of children with severe CP. 17 This PROM consists of 21 items divided into four sections: personal care, positioning/transferring, comfort, and interaction/communication. Only items deemed to be affected by lower extremity abilities or hip pain were included for analysis. Items describing ease of positioning/transferring (6 items) were considered proxy for function. Items describing comfort/less pain (3) were considered proxy for quality of life (3). Items are scored on a 7-point scale from very easy to very difficult or no pain to always pain. Scores were then collapsed into three categories: easy, moderate and difficult. Higher scores on the CCHQ denote more difficulty in lower extremity dressing, diapering, bathing, positioning in wheelchair or standing frame, wheelchair transfers, or more pain/poorer sleep.
The Lower Extremity Parent-Rated Change Form (LEC) was used to assess the parent's perspective of change after their child`s hip surgery and was considered a proxy for satisfaction with the surgical intervention. 18 It consists of four questions about changes in global health, lower limb function, general activity, and pain/fatigue, as well as one question about overall satisfaction post-surgery. The first four questions are rated on a seven-point scale ranging from “very much worse” to “very much better”. The question on satisfaction also uses a seven-point scale ranging from very dissatisfied to very satisfied. A higher score on the LEC denotes more satisfaction. The parents completed these questionnaires as most youths also had intellectual delays.
Radiographic measurements
The AP pelvic radiographs taken pre-operatively and at the latest post-operative follow-up were reviewed by two orthopedic surgeons’ fellows. Three measurements were recorded: 1) Hip displacement was measured using Reimers MP.19,20 MP is the fraction of the visible part of the femoral head position, expressed in percent. A cut-off value of 30% and below was considered normal (i.e., located versus displaced).
21
2) Acetabular coverage was measured using the acetabular index, the slope of the acetabulum for patients who had an open triradiate cartilage on radiograph.
10
Sharp's angle, an estimate of total acetabular inclination, was used in older patients for whom triradiate cartilage was closed. A cut-off value of 20° and below for the acetabular index and 42° and below for Sharp's angle were considered normal (i.e., covered versus non-covered).
22
3) Superior femoral head subluxation indicative of acetabular dysplasia was measured using Shenton's line criterion (i.e., intact versus not-intact). Shenton's line is defined as an unbroken arch formed by the top of the obturator foramen and the inner side of the femoral neck.
23
An example of pre- and post-surgery radiograph measurement of a nine-year-old female GMFCS III is illustrated in Figure 3.
A) X-rays anteroposterior (AP) view of a nine-year-old female (Gross Motor Function Classification System level III) showing left subluxed hip. Migration index = 68%, acetabular angle = 36°, Shenton's line not-intact. Patient underwent a left varus derotation osteotomy and Dega pelvic osteotomy. B) X-rays AP view of the same patient at age 15. Migration index = 10%, Sharp's angle = 34°, Shenton's line intact.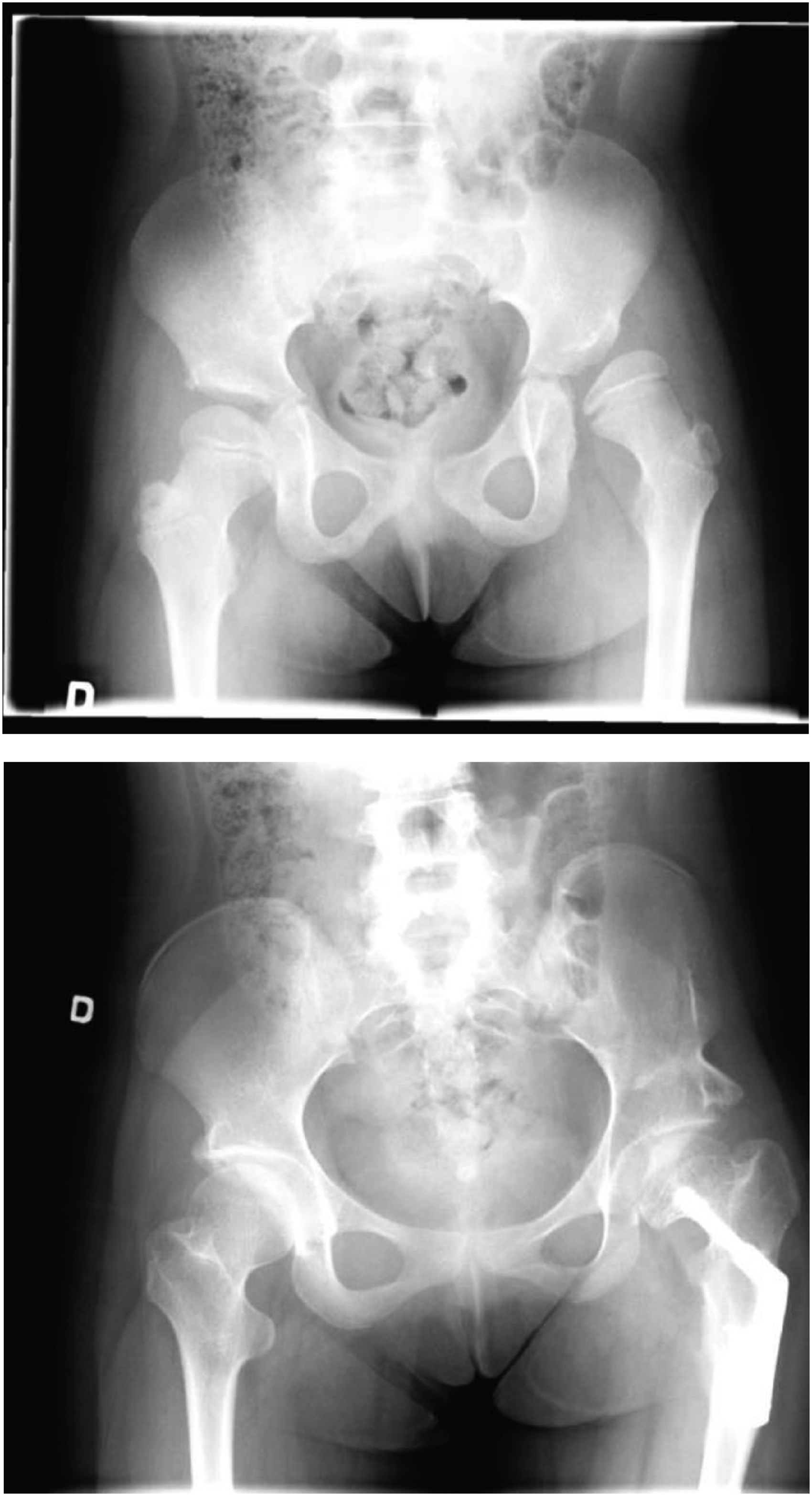
Statistical data analysis
Descriptive statistics (i.e., mean, standard deviation, proportion, range) synthesized the sociodemographics, clinical characteristics, PROMs, and radiological-related outcomes. To assess hip dysplasia change between pre-operatively and at the latest post-operative follow-up, radiological outcomes were compared using Student's paired t-test for MP, and using chi-squared test for hip displacement, acetabular coverage, and Shenton's line. To explore whether the radiological outcome was associated with PROMs, Spearman's correlations were conducted between the three radiological measurements (i.e., Reimers MP, acetabular index, Shenton's line) and specific items on the CCHQ and LEC. The size of the correlation was interpreted as negligible (r = 0.00–0.10), weak (0.10 = 0.39), moderate (0.40–0.69), strong (0.70–0.89), or very strong (0.90–1.00). 24 Statistical analyses were carried out with SPSS v25 software, and the statistical significance threshold was set at .05.
Results
Demographic and clinical data
Sociodemographic and clinical data are provided in Table 1. The 44 participants who underwent hip reconstructive surgery represent a total of 60 hips; 28 unilateral and 16 bilateral. Forty-two (n = 42) participants completed the LEC at the latest follow-up. Thirty-two (n = 32) participants completed the CCHQ. Thirty-four (n = 34) participants with 23 unilateral and 11 bilateral hips for a total of 45 hips had radiological data before and after hip reconstructive surgery. Overall, slightly more than half of the participants were male (52%). The mean age at first hip surgery was 9.0 years, and the mean age at the final follow-up visit was 17.4 years (range: 6–28 years of age) with an average follow-up period of 8.4 years (range: 1.8–17.5 years). The majority of the participants were classified as GMFCS level IV (36%) or V (39%). Sixty-eight percent of the children underwent a hip reconstruction surgery consisting of a VDRO combined with a Dega osteotomy of the acetabulum.
Demographic and clinical characteristics of the participants.
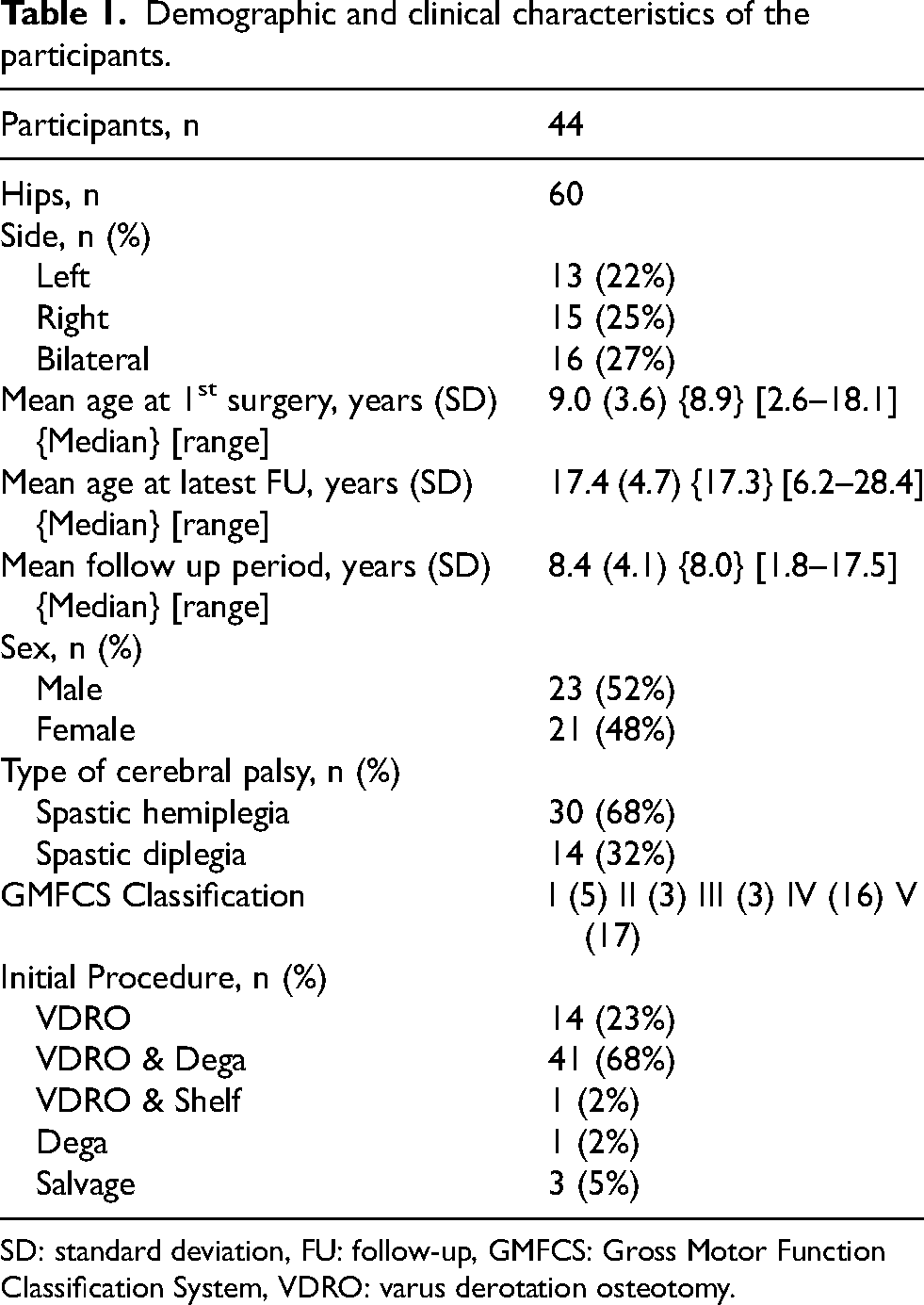
SD: standard deviation, FU: follow-up, GMFCS: Gross Motor Function Classification System, VDRO: varus derotation osteotomy.
CCHQ
At the final follow-up, the majority of caregivers reported no difficulty in terms of pain or discomfort for their child during position changes (74%), when participating in general activities (79%) or during sleep (75%) (Table 2). Furthermore, respondents described the daily tasks of putting on pants in 72% of cases, and positioning in the wheelchair in 90% of cases, as easy or moderately easy. However, respondents reported that positioning their child in a standing frame (45%), transferring in/out of wheelchair (32%), changing diapers (38%), and bathing (34%) remained difficult.
Care and Comfort Hypertonicity Questionnaire (CCHQ). This questionnaire was applicable to non-ambulatory patients (n = 32), GMFCS IV and V.
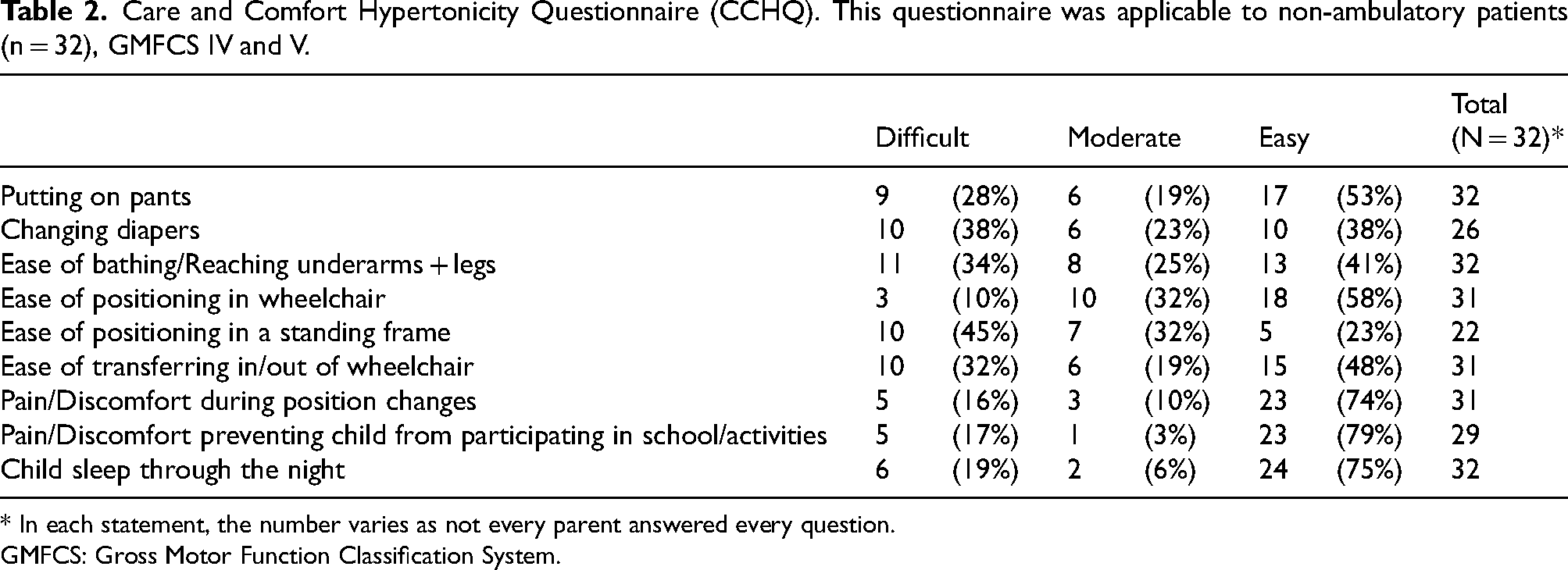
* In each statement, the number varies as not every parent answered every question.
GMFCS: Gross Motor Function Classification System.
LEC
At the final follow-up, caregivers reported a better status in their child's overall health (76%), leg function (58%), activity level (63%), and pain (68%) following reconstructive hip surgery (Table 3). Moreover, 76% of the caregivers were a little satisfied, satisfied or very satisfied with the overall changes since the surgery.
Lower Extremity Parent-Rated Change Form. This questionnaire was applicable to all patients (n = 44), GMFCS I to V.
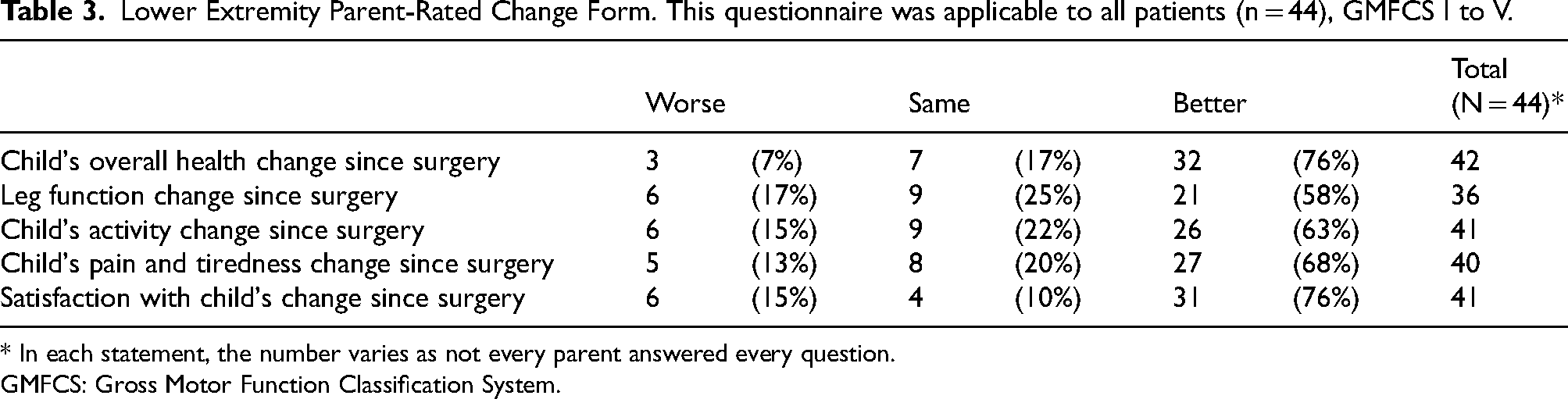
* In each statement, the number varies as not every parent answered every question.
GMFCS: Gross Motor Function Classification System.
Radiological measurements
Among the 45 hips for which both pre-operative and final follow-up radiological measurements were available, migration index improved significantly (p < 0.001) by 36.7%. Additionally, there was a 62.2% increase in the number of hips that were located post-operatively (39) compared to pre-operatively (11) (Table 4). Acetabular coverage improved significantly (p < 0.001) from non-covered to covered in 46.7% of the hips as measured by the acetabular index or Sharp's angle. Finally, Shenton's line improved significantly (p < 0.001) from non-intact to intact in 66.7% of the hips.
Radiological Measurements.
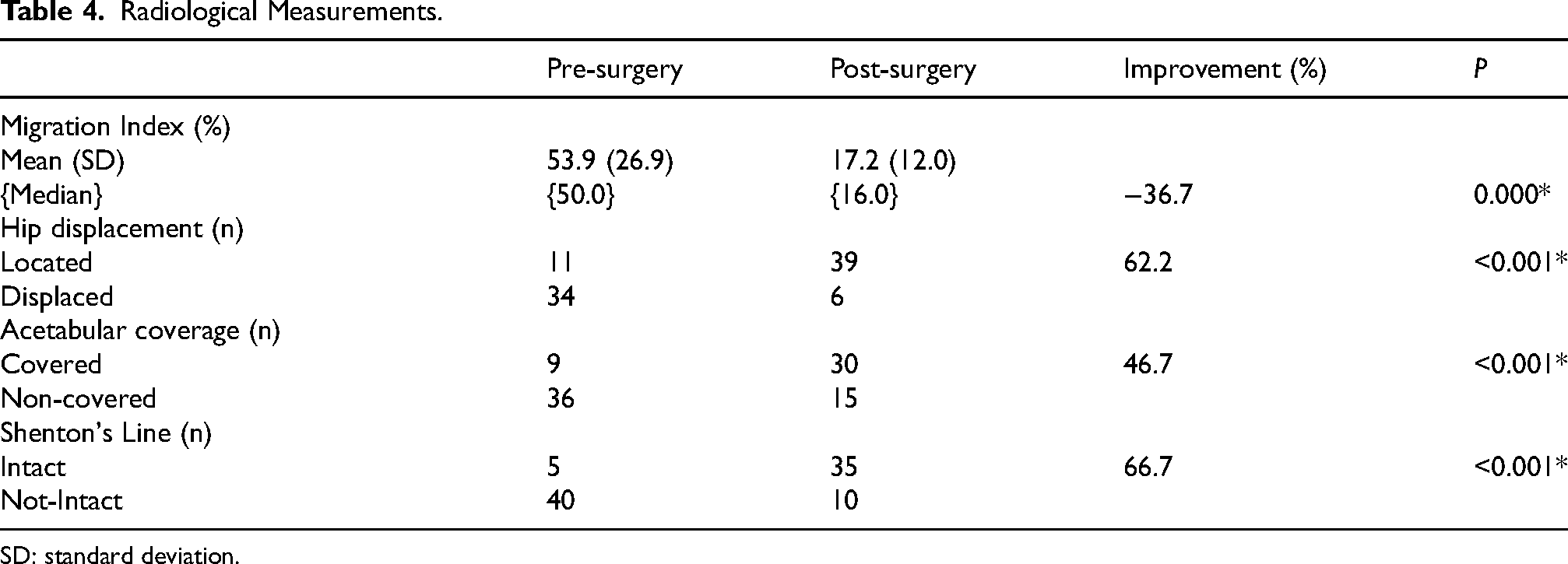
SD: standard deviation.
Complications
Of the 60 hips, there were five complications: periprosthetic fracture (n = 1), femoral neck fracture six years post hardware removal (n = 1), and hardware removals (n = 3). No infections were reported; however in two instances, the reconstruction failed requiring a femoral head resection and a McHale salvage procedure.
Exploratory analysis between the post-operative radiological measurements and functional outcomes
A moderate correlation was found between hip congruency and wheelchair transfers (CCHQ) (r = -0.548, p = 0.0229, n = 17). Moderate correlations between hip coverage and satisfaction with change (LEC) (r = 0.470, p = 0.02025, n = 24), change in positions (r = -0.418, p = 0.095, n = 17) and sleep (CCHQ) (r = -0.539, p = 0.0209, n = 18) were found. Lastly, a moderate correlation was found between Shenton's line and sleep (CCHQ) (r = -0.438, p = 0.0680, n = 18). The items of the CCHQ demonstrated an inverse correlation as lower scores denote less burden of care. The other items on the CCHQ and LEC showed negligible or weak correlations with the radiological measurements (results not shown).
Discussion
In the past, many studies have examined the issue of hip subluxation or dislocation in youths with severe CP and the outcomes of the bony surgery offered to treat this debilitating condition. In addition to the radiological findings of improved MP and integrity of the hip joint, there is widespread consensus that good clinical outcomes post-operatively can be described as decreased level of pain intensity or frequency, easier degree of caregiving, and overall parental satisfaction.25–28 To assess outcomes post-operatively, two reports by the same author on cohorts with similar inclusion criteria used a retrospective design with chart review focusing primarily on pre- and post-operative radiological findings.14,29 Some authors included subjective assessment of function (e.g., sitting balance or perineal care) and/or pain using informal questionnaires or telephone interviews rather than standardized functional outcome measures.5,13,30 Recent studies used the Caregiver Priorities and Child Health Index of Life with Disabilities (CPCHILD) questionnaire as their outcome measure 25 and visual analog scales to report on pain.31,32 However, only one study reporting on parent satisfaction following salvage surgery was found. 30
In the current study, clinical outcomes of decreased pain, ease of caregiving, and overall caregiver satisfaction in addition to radiological outcomes were the focus. The CCHQ and the LEC were chosen as measurement tools, and radiological outcomes using MP, acetabular index, and Sharp's angle assessed changes in hip displacement and coverage. The CCHQ was developed in 2006 to evaluate the functional care needs of the CP population. The questionnaire overall captures the burden of care associated with living with a child who is fully dependent. Nine of the 21 CCHQ items were used in this analysis to describe the daily tasks and situations that are particularly relevant to youth experiencing painful hip displacement. Since the inception of the CCHQ, other PROMs have been developed that specifically target functional outcomes and quality of life of individuals with CP at the GMFCS levels of IV and V, notably the CPCHILD. 33 This questionnaire is very comprehensive with 37 items categorized into six domains and three scales to assess level of difficulty, assistance, and intensity. Its length prevented its use for this study's purposes. The PedsQL-CP module is another example; while shorter in length, it does not specifically focus on any particular GMFCS level. 34 Initially the PedsQL-CP module was included to measure health-related quality of life aspects. However, the items did not address the life situation of children with severe CP and the parent responders had difficulty completing the questionnaire despite its brevity.
The presence or absence of pain is a crucial aspect of caregiving and considered an indicator of surgical success. Earlier studies included frequency or intensity of pain as an outcome in post-operative studies; however its measurement was often from the medical chart, anecdotal, and/or subjective.28,31,32 In this study, at the latest follow-up, most respondents to the CCHQ did not report pain during positioning, activity, nor sleep. The current study showed that most parents found ease in caregiving during dressing and positioning in a wheelchair to be present for several years post reconstructive surgery as measured by the CCHQ, thus supporting the earlier evidence (gains in sitting and overall less pain) reported by studies using subjective measures.13,30 Furthermore, the LEC score regarding pain showed 68% of the caregivers reported the level of pain was better since surgery and 88% reported pain was either unchanged or better. Moreover, results were similar to a previous study using the CPCHILD questionnaire to investigate the relationship between overall function and hip displacement among children with CP, which found that mobility and personal care scores were significantly improved in children who had reconstructive surgery. 27 However, results show that reconstructive surgery does not fully eliminate the burden associated with bathing, diapering, using a standing frame, and wheelchair transfers.
The study also measured the parents’ degree of satisfaction with the orthopedic procedure as well as their perception of the level of change in key health domains (positive or negative) following surgical intervention. According to LEC scores, 76% of the parents indicated they were either a little satisfied, satisfied or very satisfied with the changes. This finding is similar to that of Knaus and Terjesen who reported a satisfaction rate of 74% at 1–6 years following proximal femoral resection. 30 The results support the findings of earlier studies that hip reconstructive surgery remains an advantageous treatment for hip dysplasia. 35
Radiological measurements were available pre-operatively as well as at the latest follow-up, and comparison of these measurements indicated there were significant improvements in the MP and hip geometry as compared to the pre-operative measurements. A decrease in MP is referenced widely as the outcome that defines a successful hip reconstructive surgery. Indeed, high MP has been shown to have a significant association with higher pain intensity 31 and lower quality of life. 16 In this study, the mean MP at a mean follow-up period of 8.4 years was 17.2%, which is in line with the findings of early studies reporting MPs of 8.1–20% over follow-up periods ranging from 2–7.3 years.25,29 It must be noted, however, that radiographic measurements are but a proxy for fully assessing surgical outcomes. Surgeons have acknowledged that measurement of MP and other measures of congruency or containment are insufficient when dealing with children with complex needs.9,36 The analysis of the current study data showed only a moderate correlation between radiological measurements and functional outcomes. Even though this analysis was exploratory due to the small sample size, it is reassuring to note that parents perceive better function in some areas with improved radiological findings. It is perhaps not surprising that more general items of the CCHQ and LEC (such as participation, global health) were not correlated with radiological measurements.
This study had limitations of power, lack of pre-operative QoL assessments and no control group. First, being a single site study led to a negative impact on the statistical power of this work. Long term follow-up initiated by a single paediatric centre is inherently challenging as patients are transferred to adult centers and difficult to contact. However, the research team succeeded in scheduling a final clinic visit for slightly more than half the eligible cohort of patients. This prospective follow up visit at a mean of 8.4 years after their latest visit allowed for more recent radiographs and administration of PROMs, thus strengthening the design of this study. Another limitation, as previously mentioned, is the lack of baseline information on pain and caregiving burden (from the CCHQ) and pre-operative QoL assessment. The positive reports at final follow up cannot be solely attributed to the surgery. The retrospective design of this study and the lack of a control group prevent inference of causality and represent a further limitation of this study. Completion of the questionnaires by parents was appropriate for this study as the majority of participants had significant cognitive delays. Recall bias by the parents may have been present. When daily function is being examined and participants have adequate communication skills, child report can be an option. In addition, information on post-operative complications and pre-operative status is dependent on the completeness and accuracy of the medical record and thus subject to bias. The study population included parents of children classified as GMFCS levels I and II who did not complete the CCHQ questionnaire.
Conclusion
The objective of this study was to evaluate long-term radiological and functional outcomes as well as parental satisfaction following hip reconstructive surgery in children with CP. Measuring radiological outcomes alone is insufficient. It is imperative to also evaluate pain, function, and satisfaction to ensure that the impact of hip dysplasia on daily life has also been addressed.
At the final follow-up, the majority of caregivers reported their child as not having pain/discomfort during position changes, general activities, and sleep. Nevertheless, the burden of care on families remained significant with respect to certain daily tasks. Most respondents indicated a better or similar status in key domains of their child's health. Three-quarters of the caregivers were satisfied with the overall changes experienced after the surgery to treat hip dysplasia. Hip congruency improved from the pre-operative period in 81% and 74% of the cases as measured by MP and Shenton's line respectively. Acetabular coverage improved in 56% as measured by acetabular index/Sharp's angle.
The CCHQ is a meaningful measurement tool particularly for the CP population with GMFCS levels of IV and V due to its focus on understanding the burden of care experienced by the family. Its short length includes 21 items while ensuring compliance and a complete response. The LEC score, also brief with only five questions, is recommended as an outcome tool for reconstructive or salvage surgery in the CP population particularly due to its inclusion of parent satisfaction. Future studies using prospective methodologies and relevant PROMs such the CCHQ, the LEC, and/or the CPCHILD are needed for this population to provide more definitive evidence of the association between functional improvement, or lack thereof, with hip reconstruction. Considering both radiological evidence as well as reports of satisfaction, pain, and function can assist in the planning and implementation of effective orthopedic interventions.
Footnotes
Acknowledgments
The authors declare that this study has received no financial support. Dr Dahan-Oliel is supported by a clinical research scholar award from the Fonds de la Recherche du Québec – Santé (Junior 1: 2020–2023; Junior 2: 2024–2027).
The authors would like to thank Sofia Addab for assistance with administrative details and Guylaine Bedard and Mark Lepik for assistance with graphics.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.