
Abstract
Abstract
Purpose
This meta-analysis aims to systematically assess and quantitatively pool the best clinical evidence for migration percentage (MP) and odds ratio (OR) for recurrence/reoperation following treatment for hip subluxation in children with cerebral palsy (CP), including Botulinum Toxin A (BNT-A), soft-tissue lengthening and osteotomies
Methods
Pubmed, EMBASE and Cochrane were systematically searched from between 1 January 1953 and 11 January 2017 inclusive for studies reporting resubluxation/reoperation rates, and/or MP following treatment for hip subluxation in children with CP. The primary outcome was odds of resubluxation/reoperation. The secondary outcome was change in MP. Studies were graded for quality using the Newcastle Ottawa Scale. This meta-analysis was performed and reported in accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines.
Results
A total of 14 studies were included in analysis of odds of resubluxation/reoperation and 24 studies were included in analysis of MP. The OR for resubluxation/reoperation was lower for combined osteotomies compared with femoral (OR = 0.49; 95% confidence interval (CI) 0.25 to 0.98) and for femoral osteotomy compared to soft-tissue procedures (OR = 0.20; 95% CI 0.07 to 0.61). There was no difference in odds of recurrence/reoperation between pelvic and femoral osteotomies (OR = 2.27; 95% CI 0.37 to 13.88). Combined osteotomies provided the greatest improvement in MP, while BoNT-A showed no improvement in MP.
Conclusion
Resubluxation/reoperation rates are high; management with osteotomies is preferred to soft-tissue procedures alone in preventing resubluxation/reoperation. This meta-analysis is limited by the observational nature and small sample sizes of many of the included studies, with their inherent risk of bias and lack of homogeneity of patient characteristics at baseline. It is possible that with larger and higher quality studies, the results and conclusions of this analysis may be altered.
Introduction
Hip displacement is common in patients with cerebral palsy (CP), ranging from subluxation to complete dislocation. Hip displacement incidence is linearly correlated with Gross Motor Function Classification System (GMFCS) Level, with the incidence of hip displacement in GMFCS I and V patients being 0% and 90%, respectively. 1 Hip displacement in CP is thought to be due to muscle imbalance and bone deformity resulting typically in lateral, superior and posterior subluxation/dislocation of the hip, which can occur either unilaterally or bilaterally.1,2 However, the role of tone in the development of hip displacement has been questioned. New studies have shown that a weakness of the abductors may be the underlying pathophysiology of hip displacement in CP patients. 3 As displacement progresses, 33% to 70% of patients may experience pain and problems with activities of daily living.1,4 Pelvic obliquity due to structural scoliosis can contribute to hip under-coverage. Hip displacement may contribute to progression of scoliosis. 5 Hip displacement is associated with lower Toileting, Clothing, Transfers, Sitting, Lying, and Sleeping scores on the CP CHILD.6,7
Hip displacement interventions include bracing, injection of Botulinum Toxin A (BoNT-A), soft-tissue lengthening/tenotomy and pelvic and/or femoral osteotomies with closed or open reduction of the hip as necessary. Salvage surgery involving resection arthroplasty may be an option for non-ambulatory children with hip pain and prolonged dislocation, evidence of arthritis or poor hip congruity, or in children medically unfit to undergo reconstructive hip surgery.8,9 Hip surveillance involves clinical and radiographic analysis at prescribed intervals in order to identify hip subluxation at early stages with the goal of treating hip subluxation before severe subluxation or dislocation has occurred. 2
Large prospective studies comparing interventions for hip subluxation/dislocation in CP are not abundant. Many publications are case series,10–14 without a comparative group. Studies that have compared interventions typically only compare two groups.11,15,16–27 Summarizing and pooling results is complicated by variations in reported baseline characteristics and outcomes utilized.
The primary aim of this study was to determine the pooled odds ratio (OR) for failure (resubluxation/resdislocation/reoperation) following treatment, comparing soft-tissue procedures versus femoral osteotomy, femoral osteotomy versus pelvic osteotomy alone and femoral osteotomy versus combined femoral and pelvic osteotomies. The secondary aim was to determine the mean change in Reimer's Migration Percentage (MP) and/or final Reimer's MP for each procedure (BoNT-A, soft tissue, femoral, pelvic, combined osteotomies).
Materials and methods
Medline, EMBASE and COCHRANE databases were systematically searched without language restrictions. Maximally expanded search terms for CP, hip subluxation/dislocation/displacement and treatment methods (BoNT-A, soft-tissue lengthening, femoral and/or pelvic osteotomies), with Boolean operators were employed (Table 1). The period searched was between 1 January 1953 and 11 January 2017, inclusive. A manual search of review articles, bibliographies of included articles was performed to identify other potential studies, in a snowballing technique.
Comprehensive search strategy
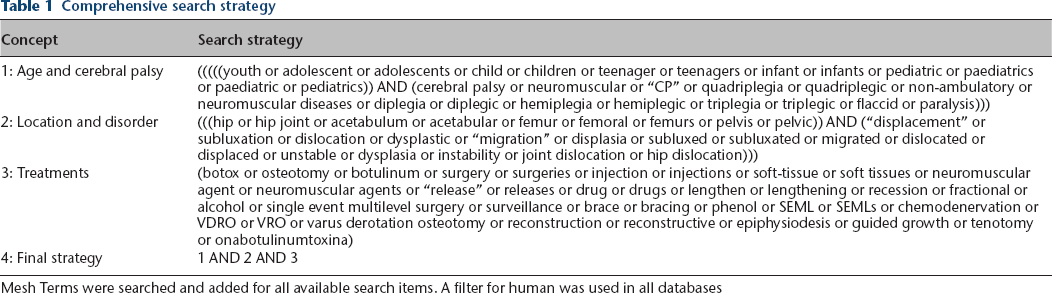
Mesh Terms were searched and added for all available search items. A filter for human was used in all databases
The primary outcome was OR for resubluxation/reoperation between different treatment modalities. Studies were included in the analysis on OR for resubluxation/redislocation if they compared at least two treatments and reported resubluxation/redislocation or reoperation. Randomized trials, cohort and case-control studies were eligible for inclusion. Case reports, case series reporting one type of intervention, reviews, conference abstracts and other publications were excluded as studies without a comparison cannot be used to calculate an OR. Study quality was assessed by the Newcastle-Ottawa Scale, recommended by the Cochrane Collaboration, 28 by two independent reviewers (KNA and CC). Any discrepancies were resolved by a third independent reviewer (ERD). Studies with a quality score of 5 or greater on the 9-point Newcastle-Ottawa Scale were included. 29 A score of 7 to 9 was considered high quality, 5 to 6 considered moderate quality and 0 to 4 considered low quality.
Secondary outcomes were mean change and mean final Reimer's MP for each treatment. MP is indicative of the portion of the femoral head that is laterally subluxatated/uncovered on the AP radiograph; the distance between the lateral border of the femoral head and Perkins line, divided by the width of the femoral head. 30 Studies were included in MP analysis if change in MP and final MP after treatment was reported. Randomized trials, cohort, case series and case-control studies were eligible for inclusion, as data from these types of studies can be pooled to give a weighted average. Studies reporting MP without standard deviations, confidence intervals or standard error were excluded, as these measures are required for pooling. Studies that did not report a measure of error, but included patient level data from which a measure of error could be calculated were eligible. Case reports, reviews, conference abstracts, expert opinion, letters and other publications wereexcluded. No minimum length of follow-up was required for inclusion.
Two reviewers (KNA and CC), independently assessed each title and abstract for inclusion. When in doubt, the full text was assessed for eligibility. Foreign studies were translated using Google Translate and inclusion and exclusion was confirmed with the assistance of a medically knowledgeable native speaker of the language.
Two reviewers (KNA and CC) extracted data, which included CP classification, GMFCS level, Melbourne Cerebral Palsy Hip Classification Scale, mean age at treatment, sex, rate of resubluxation/redislocation/reoperation, pre- and postoperative and final MP, Neck-Shaft Angle (NSA), Acetabular Index (AI), complication rate, mean follow-up time and prior hip treatment. Data was analyzed using Comprehensive Meta-Analysis software CMA V2 (Biostat, Engelwood, New Jersey). 31 Pooled risk estimates were obtained using a random-effects model. Since there was great variability in baseline patient characteristics, surgical methods and type of pelvic osteotomy performed in the studies, the random effects model was selected as it is more conservative, despite low I 2 heterogeneity. Crude ORs were calculated for each study by using reported raw data for resubluxation/redislocation or reoperation and non-events since there were no reported ORs in the studies themselves. Initial MP, final MP and change in MP were pooled for each intervention type, using a random-effects model by the methods of DerSimonian and Laird 32 due to the high heterogeneity (I 2 > 50). Means and [[sc]]sd[[\sc]]s were extracted, or calculated when patient-level raw data was available.
Publication bias was assessed by funnel plot, Eggers regression analysis and Kendall's tau test with a level of significance of 0.05 for a two-tailed analysis. Risk of bias within individual studies was evaluated using the Newcastle Ottawa Scale for quality. Meta-regression was used to evaluate the effect size for odds of increased resubluxation/reoperation and its relationship with study quality, year of publication, age at treatment and preoperative MP. This meta-analysis and systematic review was performed in accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. Meta-analysis results were reported as ORs with 95% confidence intervals (CIs), with a level of significance of 0.05. Pooled migration percentages were reported as a weighted means with 95% CIs.
Results
Fourteen retrospective cohort studies were eligible for inclusion in the assessment of odds ratio of resubluxation/reoperation. The summary of study flow is provided (Fig. 1). Study quality was graded by the Newcastle-Ottawa Scale and pertinent data was extracted (Table 2).15,19,21,26,33–42 Thirteen additional studies were closely considered but excluded for various reasons (Table 3).16,17,22–25,27,43,44–48 No evidence of publication bias was identified on Kendal tau test, Eggers regression or funnel plot (Fig. 2). Three comparison groups were identified: combined femoral and pelvic osteotomies versus femoral osteotomies,15,19,21,26,33–40 femoral osteotomies versus soft-tissue surgery35,41 and pelvic osteotomies versus femoral osteotomy.38,40,42 Other comparisons such as combined osteotomies versus pelvic osteotomy or soft-tissue surgery versus BoNT-A could not be included because there were insufficient publications comparing these treatment modalities.
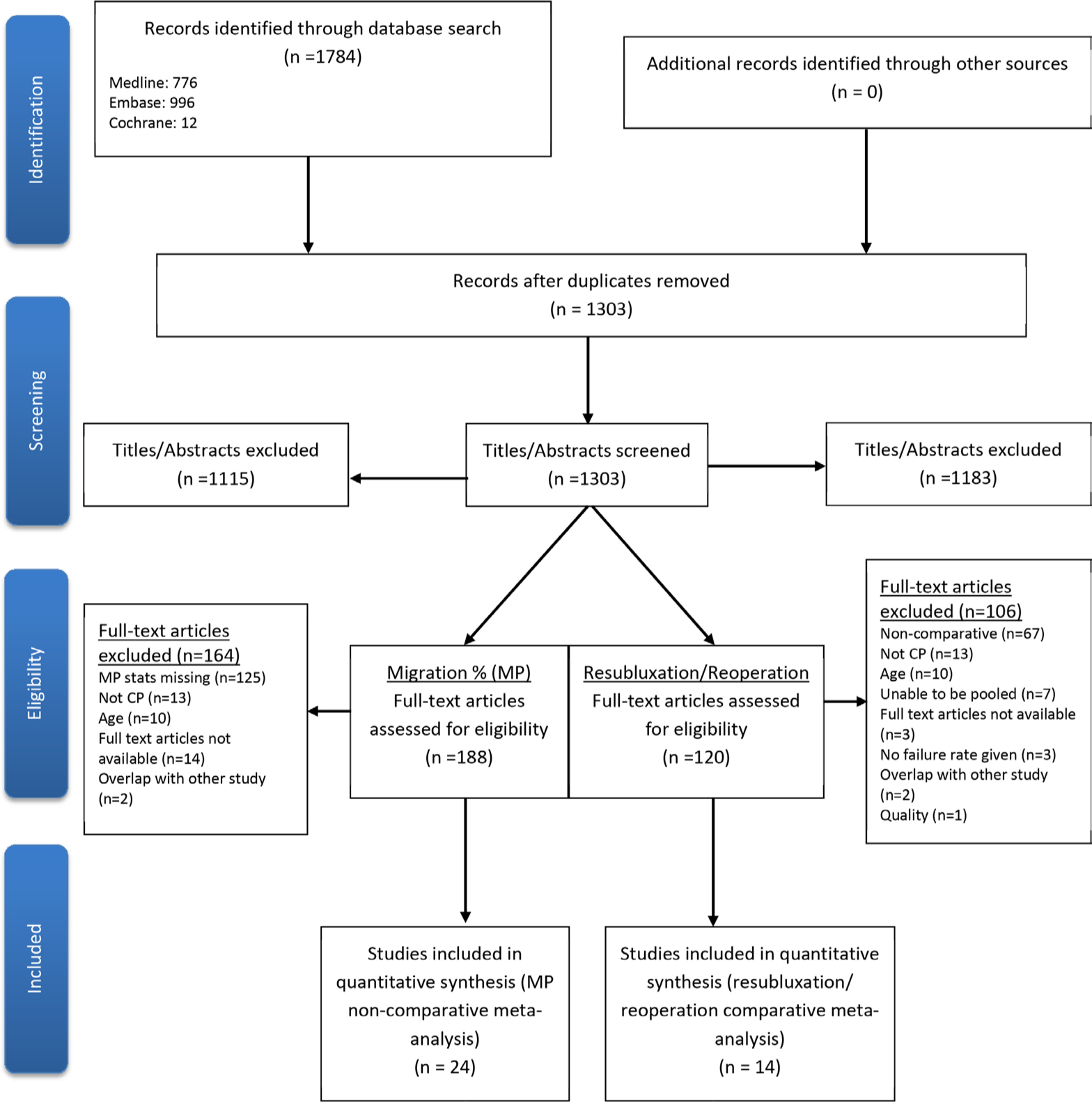
Preferred Reporting Items for Systematic Reviews and Meta-Analyses diagram showing flow of study inclusion (MP, migration percentage; CP, cerebral palsy).
Characteristics of included studies for comparative meta-analysis
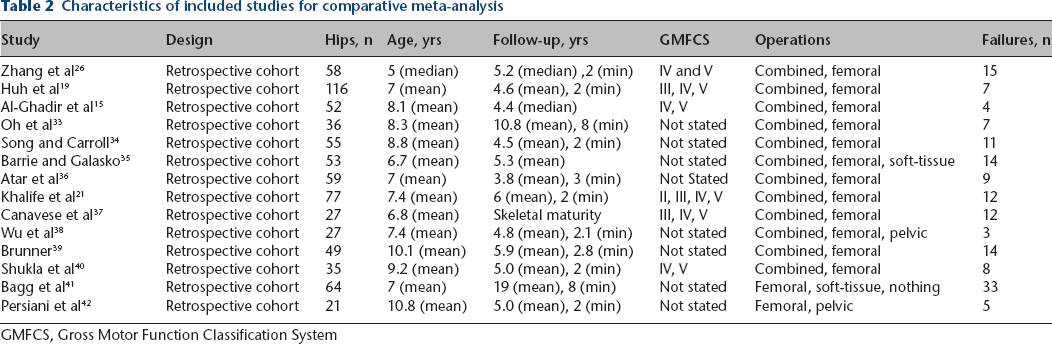
GMFCS, Gross Motor Function Classification System
Studies of potential interest, with reason for exclusion for comparative meta-analysis
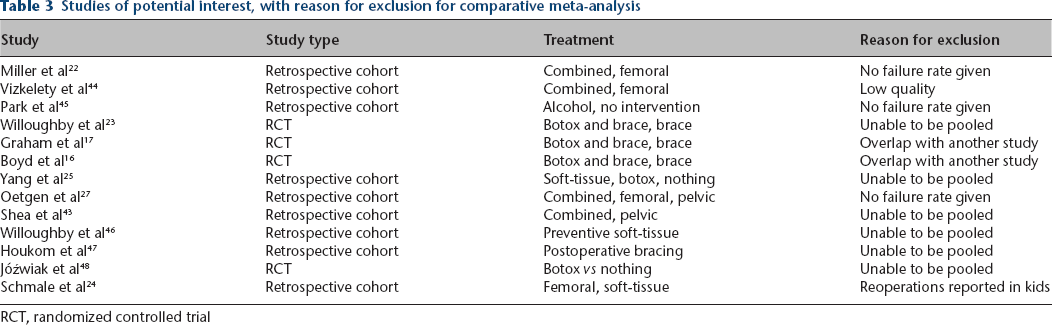
RCT, randomized controlled trial
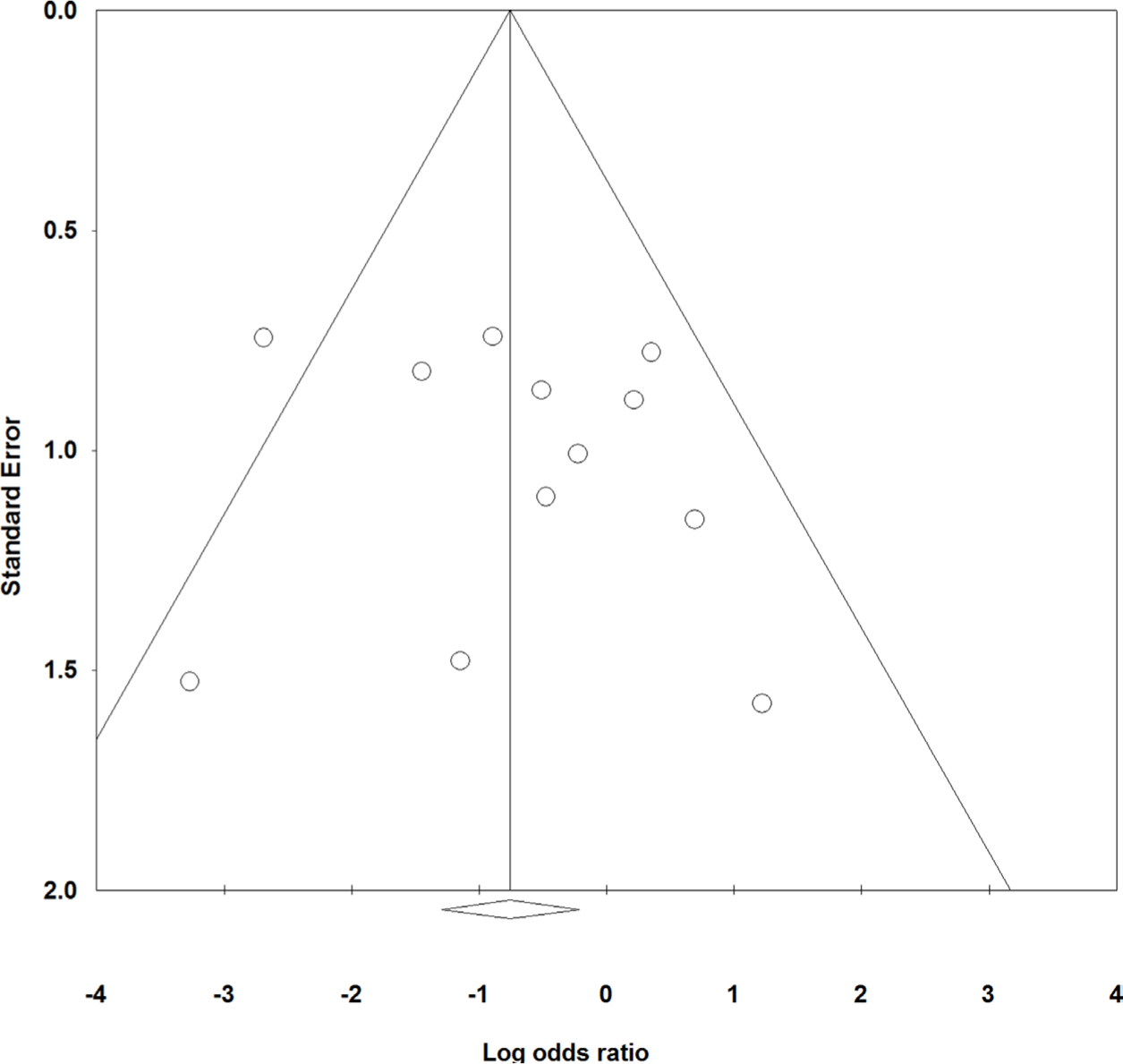
Funnel plot for combined versus femoral group showing no publication bias.
In the combined versus femoral comparison, 45 hips out of 323 hips (13.9%) treated with combined osteotomies were resubluxated/reoperated versus 63 out of 303 hips (20.8%) treated with femoral osteotomies. In the femoral versus soft-tissue comparison, eight hips out of 35 hips (22.9%) treated with femoral osteotomy were resubluxated/reoperated versus 21 hips out of 37 hips (56.8%) treated with soft-tissue surgery. In the pelvic versus femoral comparison, six out of 13 hips (46.1%) treated with pelvic osteotomy were resubluxated/reoperated versus four out of 23 hips (17.4%) treated with femoral osteotomy.
Studies were single centre or small multi-centre populations. Nine studies reported resubluxation/redislocation and five studies reported whether subsequent surgery was performed for recurrent subluxation. None of the included studies blinded authors to treatment allocation or patient outcomes. Two studies used independent reviewers who did not perform the surgery or provide postoperative care to evaluate the radiographs and measure indices such as the MP.15,33 Three studies did not stipulate a minimum follow-up time and some patients may have been followed less than two years.15,33,35 Sample size ranged from 21 hips to 116 hips. In studies that documented GMFCS level,15,19,21,26,37,40 no GMFCS I patients were included. Median age at index operation was 7.4 years; the youngest patient was one and the oldest 17 at the time of surgery.
In the combined versus femoral comparison, the Dega osteotomy19,21,33,34,37,38,40 was the most commonly reported pelvic osteotomy (seven studies), while the San Diego osteotomy,15,40 Triple38,40 and Shelf37,40 were the less commonly reported. In the femoral versus soft-tissue comparison, soft-tissue procedures included iliopsoas, adductor and rectus femoris releases/recessions/lengthenings.
The odds of resubluxation/reoperation were significantly lower for combined osteotomies compared with femoral alone (OR = 0.49; 95% CI 0.25 to 0.98) (Fig. 3). The odds of resubluxation/reoperation were significantly lower for femoral osteotomies compared with soft-tissue surgery (OR = 0.20; 95% CI 0.07 to 0.61) (Fig. 4). The odds of resubluxation/reoperation were not statistically different for pelvic versus femoral osteotomies (OR = 2.27; 95% CI 0.37 to 13.88) (Fig. 5). One study, Wu et al, 38 had no failure for either treatment and, therefore, an OR could not be calculated. Meta-regression demonstrated no association between study quality or age at time of treatment and effect size for odds of resubluxation/reoperation. There were significantly lower odds of resubluxation/reoperation with more recent year of publication (slope = -0.10; p < 0.01), while odds of resubluxation/reoperation with initial higher MP was not statistically significant (slop e = 0.07; p > 0.05).
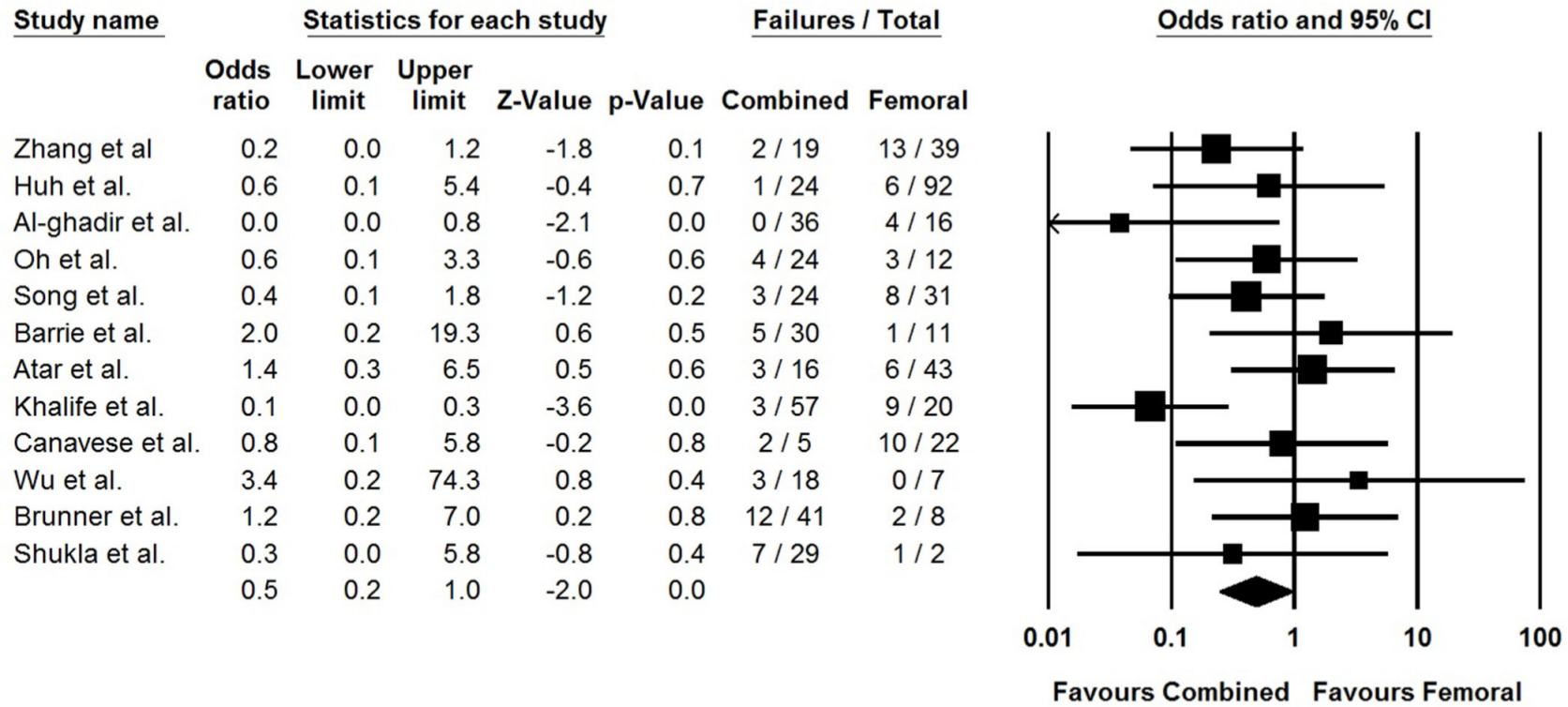
Forest plot showing decreased odds of resubluxation/reoperation for combined osteotomies compared to femoral osteotomy alone (CI, confidence interval).
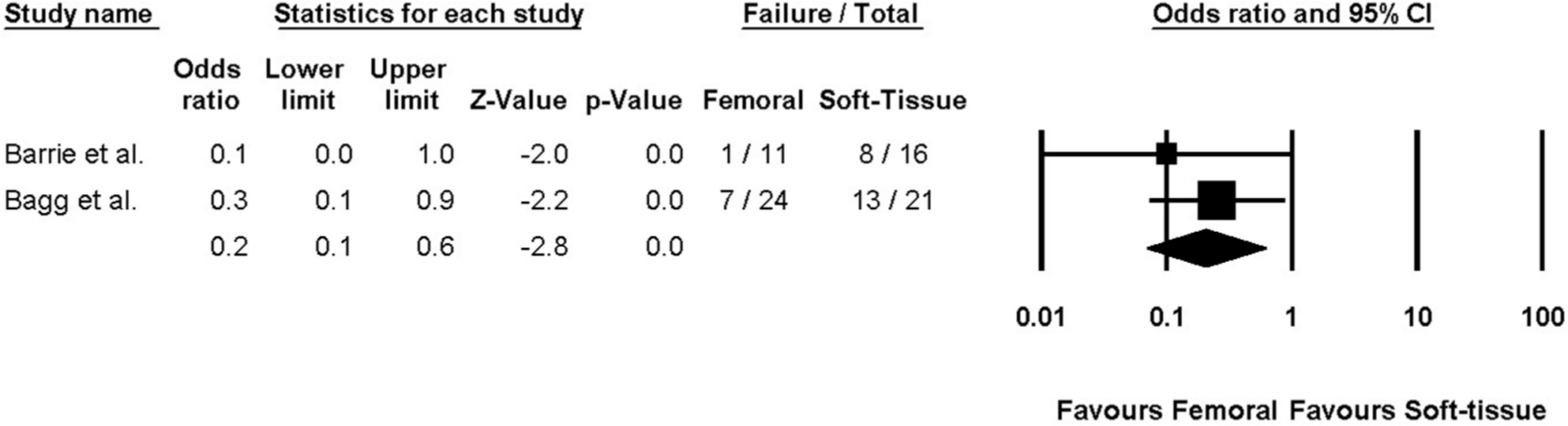
Forest plot showing decreased odds of resubluxation/reoperation for femoral osteotomy compared to soft-tissue procedures (CI, confidence interval).
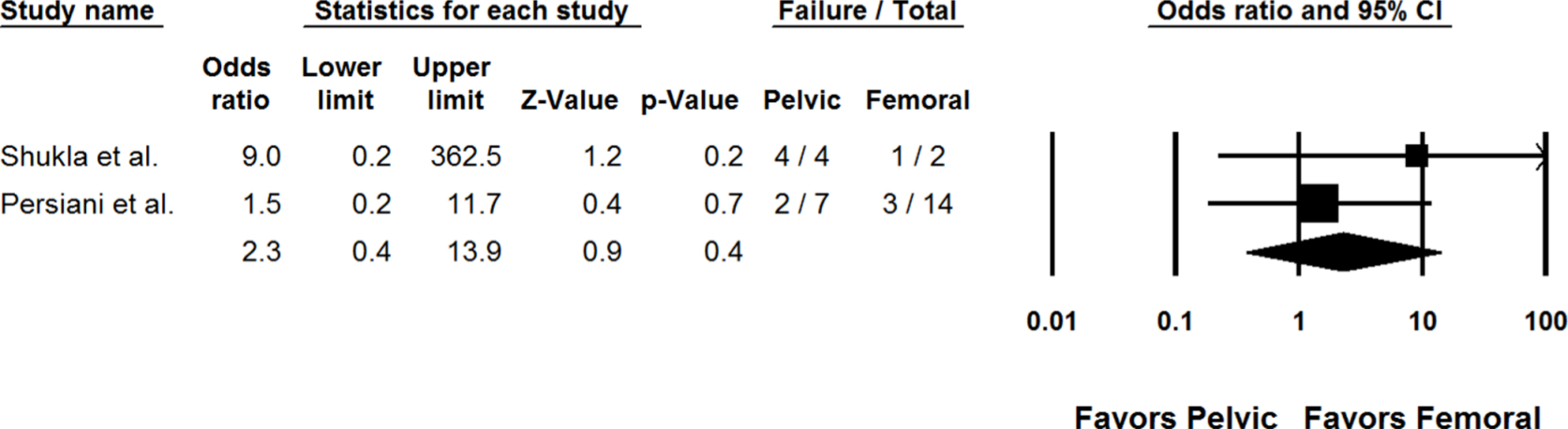
Forest plot showing no difference in odds of resubluxation/reoperation between femoral and pelvic osteotomy.
Twenty-four studies were eligible for inclusion in the pooled analysis reporting on final MP and/or change in MP. Data were extracted (Table 4) and the pooled results reported (Table 5), including mean initial MP, range of initial MPs, percentage of non-ambulatory patients, change in mean MP and mean final MP for each treatment method.7,12,15,19,24,25,34,35,37,42,43,48–60
Characteristics of included studies in migration percentage meta-analysis
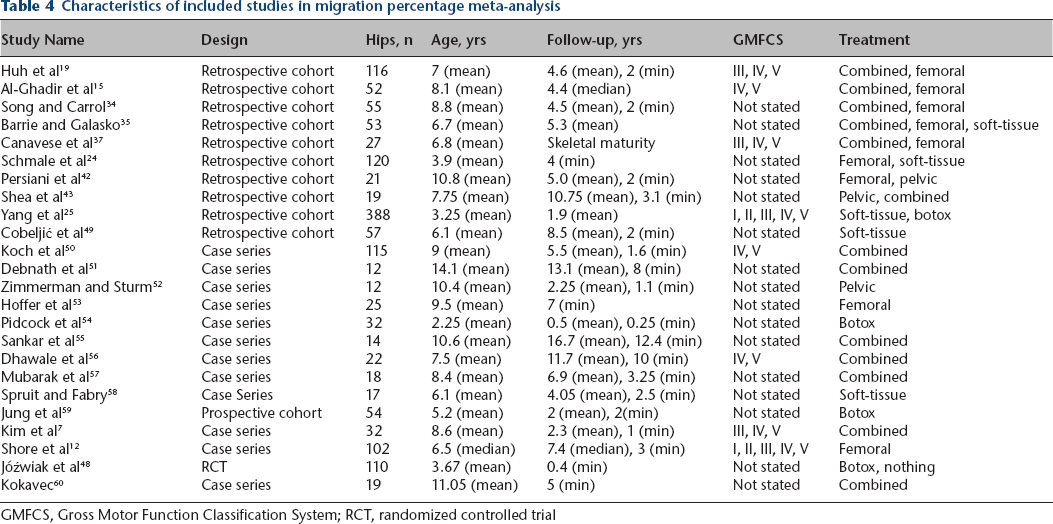
GMFCS, Gross Motor Function Classification System; RCT, randomized controlled trial
Results of migration percentage (MP) meta-analysis*
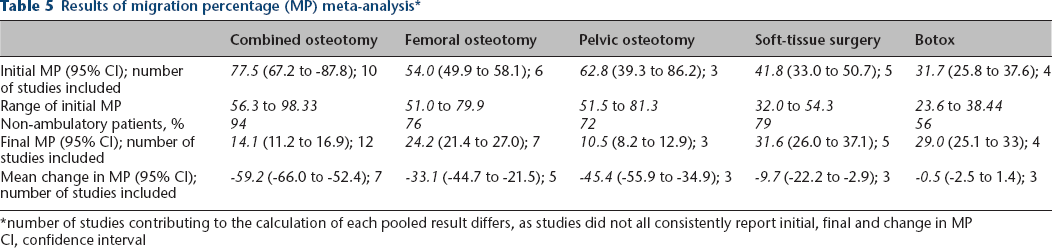
number of studies contributing to the calculation of each pooled result differs, as studies did not all consistently report initial, final and change in MP
CI, confidence interval
For patients treated with combined osteotomy, almost all patients were non-ambulatory, while for those treated with isolated femoral or pelvic osteotomy or soft-tissue release approximately three-quarters were non-ambulatory and approximately half treated with BoNT-A were non-ambulatory (Table 4). Combined pelvic/femoral osteotomy resulted in 60% improvement in MP, while isolated pelvic osteotomy improved MP by 45%, isolated femoral osteotomy by 33%, soft-tissue procedures by 10% and there was negligible improvement with BoNT-A (Table 5).
Discussion
The aim of this meta-analysis and systematic review was to systematically analyze the odds of resubluxation/dislocation/reoperation following treatment for hip subluxation/dislocation inpaediatric patients with CP and to assess improved hip coverage for each method by way of final MP and change in MP after treatment. The OR for resubluxation/reoperation in the combined osteotomy versus femoral osteotomy group was 0.49 (95% CI 0.25 to 0.98), in the femoral osteotomy versus soft-tissue group was 0.20 (95% CI 0.07 to 0.61) and in the femoral osteotomy versus pelvic osteotomy was 2.27 (95% CI 0.37 to 13.88). Combined femoral and pelvic osteotomies provided the greatest improvement in MP, followed by pelvic osteotomy alone, femoral osteotomy alone and then soft-tissue procedures. There was no evidence of improved MP with BoNT-A.
BoNT-A multiple comparative studies investigated the effectiveness of BoNT-A on hip subluxation, including one randomized controlled trial (RCT).16,17,23 MP was reported but information required (sds, correlation coefficients, t-values) in order to pool the results was not available. In an RCT comparing BoNT-A to bracing, 8.7% more patients required subsequent reconstructive surgery in the BoNT-A group compared with the brace group. 23 One study compared BoNT-A with soft-tissue surgery, but as it was the sole study of this type it could not be included as meta-analysis requires at least two studies with the same outcome measures and comparative groups for pooling. This study reported minimal change in MP in both the soft-tissue lengthening and the BoNT-A groups. MP change was not statistically different between the groups (soft-tissue MP of -3.3%, BoNT-A MP-1.6%). 25 In pooled non-comparative analysis, the change in MP following BoNT-A was negligible. Based on this limited analysis, BoNT-A should not be a primary treatment method for hip subluxation. However, BoNT-A could still play a role in providing temporary improvement in hip range of movement, ease of care, improved comfort and improved gait function.61,62
Soft tissue
Soft-tissue procedures performed before the age of four to six years have been suggested for children with severe CP to reduce spasticity in hip adductors and flexors that are thought to contribute to subluxation. 63 However, other studies have found that children who underwent soft-tissue procedures have high reoperation rates. 64 In this analysis, reoperation/resubluxation rates with soft-tissue procedures ranged from 50% to 77%; femoral osteotomy was 80% less likely to undergo reoperation/resubluxation than soft-tissue procedures alone. The improvement in MP following soft-tissue procedures was only 9.7%. Following soft-tissue procedures, the likelihood of further surgical intervention is high. These procedures remain an option; they may potentially delay bony surgery in a very young child. Families should be counseled that pursuing soft-tissue surgery, particularly in lieu of bony surgery, will most likely be of short-term benefit and that the child may need to undergo a more extensive surgery in the future.
Osteotomy
The decision to proceed with femoral osteotomy alone, pelvic osteotomy alone or combined osteotomies may primarily be informed by the severity of the hip subluxation (greater MP), the AI (with surgeons preferring to include pelvic osteotomy typically with AI > 25), intraoperative assessment of stability (with surgeons adding pelvic osteotomy if a hip is unstable after femoral osteotomy alone) and surgeon preference. There was a 51% decrease in odds of reoperation/resubluxation among those who underwent combined pelvic and femoral osteotomy procedures as compared with those who underwent femoral osteotomies alone, and the change in MP was of greatest magnitude compared to other treatments. Patients receiving combined osteotomies had greater deformity at baseline.
Few studies assessed pelvic osteotomy alone. It may be relatively uncommon for patients with hip instability to undergo a pelvic osteotomy for CP in the absence of other procedures. Only two studies were included in this comparative analysis, with only 13 hips undergoing pelvic osteotomy alone. There was no significant difference in the odds of failure of treatment between isolated pelvic osteotomy and femoral osteotomy. Although pelvic osteotomies delivered a final MP of approximately 10%, this finding is limited by the small number of hips analyzed (25 hips) and should be interpreted with great caution.
Limitations
This meta-analysis has a number of limitations. First, due to variations in the outcomes reported, not all comparative studies were eligible for inclusion. Our comparative analysis was limited to studies that included two or more treatment arms and reported rates of reubluxation/redislocation/reoperations. The majority of comparative studies did not consistently report NSA or AI and thus these outcomes were not suitable for comparative meta-analysis.22,27,43 Although MP was reported in many comparative studies, the necessary sds, correlation coefficients and/or t-values required for pooled comparative analysis were not reported, as such we could not perform a comparative analysis between groups such as odds of improved MP.
Second, patient characteristics differed between treatment groups within each original study and between studies. For instance, patients that underwent combined femoral and pelvic osteotomy surgery had more severe hip subluxation than patients undergoing a single osteotomy or soft-tissue procedure alone. There was variability in initial MP, pattern of CP involvement, severity of CP involvement including ambulatory status, length of follow-up and prior treatment for the hips between the treatment groups at baseline. In meta-regression, higher initial MP was not associated with increased odds of resubluxation/redislocation/reoperation; however, this was under-powered, with only four studies being eligible for inclusion in this sub-analysis.
Third, we selected resubluxation/redislocation and/or need for reoperation as the primary outcome measure. The need for reoperation and the definition of resubluxation/redislocation is quite subjective and the threshold at which surgery will be undertaken may differ between treating surgeons. As we did not have clinical or radiographic data on individual patients, we used the definition of resubluxation/reoperation/failure provided by the surgeons/authors of the original articles.
Fourth, while our search strategy attempted to include all possible nomenclature for the disorder and treatment modalities, there may be other relevant studies that were not identified and included. Fifth, the included studies in the comparative analysis (of OR for resubluxation/reoperation) were all observational in nature with relatively small sample sizes, with inherent risk of bias; many studies were of only moderate quality. It is possible that with larger and higher quality studies, the results and conclusion of this analysis may be altered.
Sixth, there is insufficient study-level data to differentiate between different surgical techniques. In particular, the surgical technique for soft-tissue releases/lengthening could include everything from a percutaneous recession at the musculotendonous junction of a single muscle, to complete tenotomy/myotomy of multiple tendons and muscles. Included studies did not provide details on which muscle/tendons were lengthened (adductor longus, gracilis, adductor brevis, adductor magnus, psoas, rectus femoris or other), whether the lengthening was fractional or complete tenotomy, open or percutaneous or whether any adjuncts such as botox, phenol or neurectomy were included. It is possible that a very extensive soft-tissue release may have different results than a more conservative release, but this cannot be elucidated from the current meta-analysis.
Finally, the numbers presented for final MP is a combination of improved MP from surgery and worsening of MP from the natural progression of hip development in CP over the years between surgery and final follow-up. The reported improvements in MP are conservative as the improvement in MP likely was greater immediately after surgery. As an example, following femoral and pelvic osteotomy MP may have gone from 80% to 15%, but only a final MP three years later of 20% was reported. Reporting of MP improvement immediately after surgery is a more accurate measure, but due to many studies reporting change in MP at final follow-up, not immediately postoperatively, this is a reasonable alternative for the purposes of understanding gross improvements expected from the discussed procedures.
In conclusion, there are many surgical options available for children with CP-related hip subluxation/dislocation. The results of our study do not support the role of BoNT-A in treatment of hip subluxation; there is no evidence for improved MP following BoNT-A. Soft-tissue procedures provide a moderate improvement in MP, and are associated with a relatively high rate of subsequent surgery. Soft-tissue procedures are unlikely to provide definitive treatment for hip subluxation, but may be a smaller, relatively low morbidity intervention to delay the need for greater surgery, such as in a very young or medically unstable child. These results are consistent with recent prospective work (not included in this pooled analysis due to lack of necessary statistical measures required for pooling) that has reported low success rates for soft-tissue surgery in children with higher GMFCS levels. 65
Combined pelvic and femoral osteotomies provided the greatest improvement in MP and the lowest odds of subsequent resubluxation/redislocation/reoperation; osteotomies are favourable when compared with soft-tissue surgeries. For patients with more severe hip subluxation (greater MP) and those at high risk of resubluxation, (higher GMFCS) performing both femoral and pelvic (combined) osteotomies may provide optimal results.66,67 This study is limited primarily by the moderate quality of the included studies, none of which were prospective. Further prospective study using both radiographic and patient reported outcomes such as CPCHILD may help to better differentiate the outcomes and indications for each treatment regimen.
Footnotes
CC: Data curation; Formal analysis; Investigation; Writing – original draft; Writing – review and editing.
DMS: Methodology; Supervision; Writing – original draft; Writing – review and editing.
ERD: Conceptualization; Methodology; Formal Analysis, Supervision; Writing– original draft; Writing – review and editing.