
Abstract
PURPOSE:
There is a general lack of evidence on the efficacy of rehabilitation training methods after childhood stroke. The aim of the current paper is to provide an example of a multidisciplinary assessment and intensive patient-centered rehabilitation program that was devised following the Clinical Guidelines for Childhood Stroke Diagnosis, Management and Rehabilitation, based on the International Classification of Functioning, Disability and Health.
METHOD:
The case of a 13-year-old teenager with physical, linguistic, cognitive and emotional impairments after acute ischemic stroke (AIS) in left middle cerebral artery territories is presented and his neurorehabilitation program is described.
RESULTS:
After an intensive and comprehensive rehabilitation period, the patient showed significant improvement involving language abilities, cognitive flexibility, logical reasoning and motor independence. A 6-month post-stroke follow-up evaluation showed further gains in spontaneous language, improved motivation and collaboration, reduction of impulsiveness and better general motor stability.
CONCLUSION:
This case highlights how an intensive, patient-centered, interdisciplinary rehabilitation approach can lead to good improvement across different domains, maximizing the spontaneous recovery in children and adolescents after AIS.
Introduction
Arterial ischemic stroke (AIS) in pediatric patients is rare yet recognized as a significant cause of acquired brain injury and life-long morbidity [1]. Its incidence is progressively increasing and ranges from 1.3 to 13 per 100,000 [2]. Stroke etiology in childhood is broader than in adulthood and it is often of unknown origin [3]. Cerebral arterial dissection, which may occur spontaneously or after trauma, can be considered a rare cause of ischemic stroke in children [4].
Although ischemic stroke in children is generally perceived as having a more favorable outcome compared to adults, in a significant number of cases it leaves patients with residual impairments and long-term motor, cognitive, and behavioral consequences [5].
Recovery is a complex process occurring through a combination of spontaneous and learning-dependent processes grounded on restitution, substitution and compensation mechanisms [6]. In order to set up a specific rehabilitation program, neuropsychological and motor testing are essential to assess the presence of neurocognitive and/or physical impairments. Child-based rehabilitation promotes and assists neural plasticity, optimizing recovery and outcome [7]. Taking into account all of the International Classification of Functioning, Disability and Health (ICF) domains, benefits of intensive and early multidisciplinary treatment are highlighted by the Clinical Guidelines for Childhood Stroke Diagnosis, Management and Rehabilitation [8]. The use of the ICF model in clinical practice allows providers to move from purely medical or social models of disability toward a biopsychosocial framework, focused on the dynamic interactions between the health condition and the personal and environmental factors at play (Fig. 1) [9].
Biopsychosocial model of the International Classification of Functioning, Disability and Health – Children and Youth version (ICF-CY).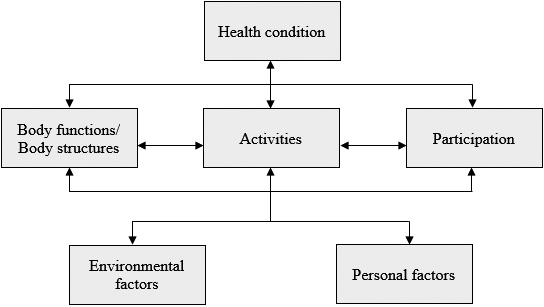
A 13-year-old Italian teenager with neither family history of neurological disease nor previous medical history except for favism disease is described.
On the day of the AIS, he suddenly mentioned left orbital and facial pain, fell to the ground and developed aphasia and right hemiplegia, without losing consciousness. There was no antecedent trauma. In the morning of the onset of symptoms, headache and vomiting occurred.
Upon the patient’s arrival to the Hospital, he had aphasia, left head and gaze deviation and right hemiplegia. A first Magnetic Resonance Imaging (MRI) revealed a dissection of the left internal carotid artery and a homolateral acute ischemic territorial lesion (see Fig. 2). An attempt of mechanical thrombectomy of the occluded left Middle Cerebral Artery (MCA) was performed without success.
Brain magnetic resonance imaging showing the acute left ischemic lesion on FLAIR axial scans.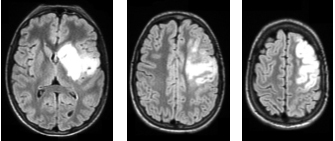
In the Intensive Care Unit, the patient was maintained in a medically-induced coma for 5 days, while he was treated with anticoagulant, antibiotic and infusion therapy. A central venous catheter and a nasogastric tube were positioned. Vital signs were within the normal range, routine blood examination and ECG were normal, and EEG showed no epileptiform discharges. Five days after the onset of symptoms, another MRI confirmed a left hemisphere ischemic lesion, and a CT Angiography study showed a lack of visualization of the supraclinoid tract of the left MCA (see Fig. 3). After 40 days, the anticoagulant was switched to antiplatelet therapy.
Brain CT angiography revealing left internal carotid artery occlusion.
Tests for vasculitis, prothrombotic states, and viral neurotropic antibodies, as well as genetic analysis for Fabry disease, assessments of plasma amino acids concentration and oropharyngeal swab were all negative. Transesophageal and transthoracic echocardiography were normal.
The patient was transferred to our Neurorehabilitation Center where he was on antiplatelet therapy. A multidisciplinary team cooperated in order to obtain a global view of his difficulties. An intensive (4–5 hours per day for 106 days) neurological rehabilitation training was designed according to his specific needs and focused on speech therapy, cognitive function training, motor and occupational therapy and psychological support.
For each area of intervention, the patient underwent an initial assessment aimed at identifying a specific rehabilitation pathway.
A standardized clinical evaluation of his communicative behavior revealed the presence of motor speech disorders and severe aphasia. The patient’s speech was dysarthric, almost unintelligible. Also, his spontaneous language was not fluent, characterized by word-finding impairment and by several phonemic and semantic paraphasic errors. The absence of function words and inflections revealed the presence of agrammatism. Repetition and naming impairments were detected. Comprehension was relatively good, with some difficulties in understanding grammatical contrasts. Since the patient’s motor deficits prevented him from manipulating writing instruments, the agraphia could not be assessed.
A comprehensive neuropsychological examination highlighted the presence of several difficulties in problem solving, planning, cognitive flexibility, self-monitoring and cognitive inhibition. Mild deficits were found in the nonverbal intelligence domain. No impairments of perception, memory or attention were observed.
The patient presented with severe right hemiplegia with right upper limb hypotonia. He was only partially autonomous in postural changes. Thus, he was completely dependent in basic (BADL) and instrumental (IADL) activities of daily living, needing physical assistance. Motor tests showed a good performance in static sitting balance and more difficulties in dynamic sitting balance and coordination.
Specific linguistic, cognitive and motor tests with raw scores and percentages of accuracy are reported in Table 1.
Linguistic, cognitive and motor scores at admission, discharge and follow-up
Linguistic, cognitive and motor scores at admission, discharge and follow-up
na
With respect to behavioral and psychological response, the patient struggled to establish a good working alliance with all of the specialists, showing avoidance signals and emotional unavailability. He presented consistent anxiety-related behaviors, psychological distress and poor motivation, and refused complex exercises in order to avoid frustrating experiences. In addition, he showed poor self-reflection ability, attempting to escape from negative thoughts and feelings.
After the initial speech evaluation, a twice daily rehabilitation program was focused on articulation, verbal production and auditory and reading comprehension. For specific tasks, see Table 2.
Linguistic (A), cognitive (B), physical (C) and occupational (D) therapy specific tasks
Linguistic (A), cognitive (B), physical (C) and occupational (D) therapy specific tasks
Compensatory approaches for aphasia intervention in adult patients, such as the Promoting Aphasics’ Communicative Effectiveness (PACE) [19] and the application of Semantic Feature Analysis (SFA) [20], were adapted to the patient’s needs. Moreover, a smartphone and tablet were used to facilitate communication.
A specific daily neuropsychological rehabilitation program was designed with paper and pencil exercises and computerized tasks using the rehabilitation software “ERICA” [21]. Cognitive training was focused mainly on executive functions, while sustained, selective and divided attention tasks were aimed at reducing impulsivity (see Table 2). The complexity of each exercise was progressively increased to match the patient’s improvement in accuracy and processing speed and decrease of impulsiveness.
The motor impairment was treated with physiotherapy sessions twice daily. Exercises were aimed at strengthening muscles, decreasing spasticity, improving transferring abilities and postural changes, increasing balance and posture control during standing and walking, walking indoors and outdoors independently and climbing up and down stairs. See Table 2for specific tasks. A carbon fiber ankle-foot orthosis (AFO) and a nighttime brace for the right upper limb were adopted to maintain a full active range of motion and prevent contractures. In addition to traditional physical therapy, electrostimulation, virtual reality activities and hydrokinetic therapy were performed.
Two occupational therapy sessions per day were aimed at improving fine upper limb motor skills in order to enhance the patient’s participation and increase his independence during ADLs.
Psychological support was provided in twenty sessions and focused on cognitive processing of the patient’s traumatic experience. Imaginative techniques and metacognitive strategies were taught to decrease restlessness and support him during his difficult rehabilitation training. The last sessions were dedicated to the return of the patient into society and school. During the sessions, he established a good therapeutic alliance, with increasing self-disclosure and emotional openness over time. His use of defense mechanisms was gradually reduced, which allowed for greater availability and cooperation in working with all of the team’s specialists.
At discharge, the patient showed general improvement. Advancement was particularly evident in verbal comprehension and understanding of grammatical contrasts, as well as in naming and articulation abilities. Due to better speech intelligibility, a significant gain in spontaneous language was observed, with an increased communicative intent that included conversations on topics of everyday life.
A second neuropsychological assessment showed better nonverbal logical reasoning and an increased ability to coordinate thoughts and behavior, with more cognitive flexibility, as well as improved planning and self-monitoring skills.
Regarding motor skills, the patient reached good autonomy in postural changes and walking ability, requiring supervision only on uneven surfaces. If helped by supervisors with verbal reminders, he was more independent in BADL and IADL.
Results of the final assessment are summarized in Table 1.
With respect to the emotional domain, the patient demonstrated greater reduction of impulsiveness, good availability and cooperation with all of the team’s specialists, increased emotional availability and reduction of social withdrawal.
After discharge, the patient was reintegrated into home and school life with environmental support (e.g. orthotic devices for mobility, optimal arrangement of furniture, digital tablet for communication, daily living aids). He attended the last months of middle school and passed his eighth grade finals.
Follow-up assessment
A 6-month post-stroke follow-up assessment was performed after a period of sub-intensive (three days a week) speech therapy and neuro-motor training in a different structure. The evaluation showed a general stability in both linguistic and motor domains, with further mild improvement in all tests. The executive functions, in particular planning and self-monitoring abilities, were the only areas in which the patient showed a mild decrease in performance compared to his discharge evaluation. Written language assessment highlighted the presence of mild agraphia. For raw scores and percentages of accuracy, see Table 1.
Modified ICF-CY model considering the patient’s characteristics and his rehabilitation program.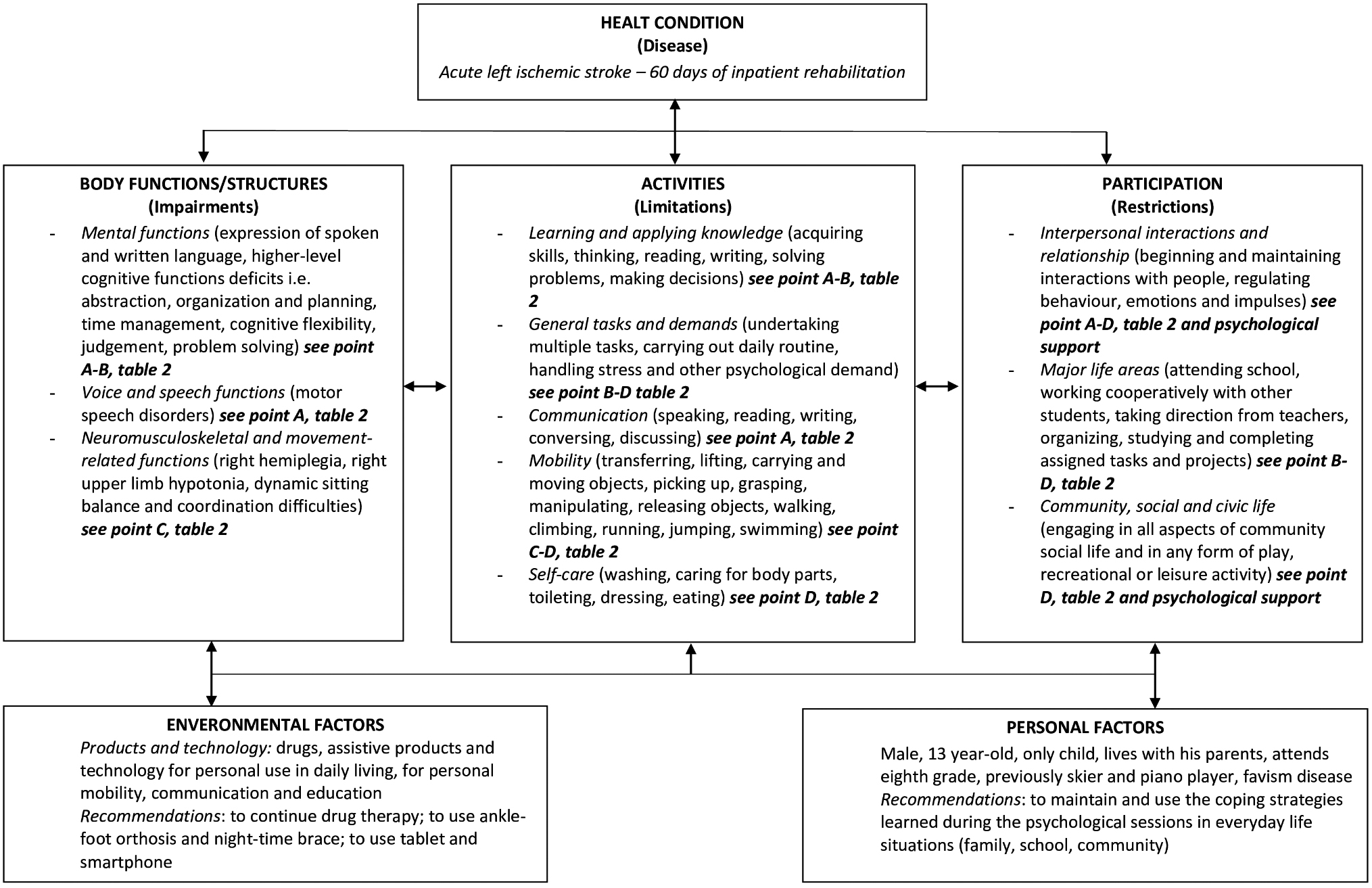
The aim of this paper is to report the multidisciplinary assessment and the patient-centered rehabilitation program of a 13-year-old AIS patient who subsequently made significant clinical improvement. As the Clinical Guidelines for Childhood Stroke Diagnosis, Management and Rehabilitation suggest, an early, intensive and multimodal intervention was developed [8]. Referring to the ICF model, the patient functioning was considered in terms of the dynamic interactions between his disability and environmental and personal factors (Fig. 4). The ICF, supporting both medical and social models of human functioning and disability, provides a multidimensional framework that can be used to set up comprehensive and interdisciplinary approaches to assessment and intervention (Tables 1 and 2 and Fig. 4). Moreover, it offers a common language for health, social and educational services that can be used across different settings and disciplines [9].
Because descriptions of post-stroke rehabilitation training in childhood are rare, we referred to adult-stroke literature, adapting the therapeutic environment to the patient’s specific needs in terms of modality, intensity and location of the intervention.
Since children and adolescents usually show consistent difficulties working in structured settings, which are required in adult standard training [22], it is important to customize the treatment in accordance to the young patient’s needs [23]. All therapeutic interventions were tailored to the teenager’s specific profile. Therapists tried to develop a good working alliance with him by including some enjoyable tasks in each session. Literature highlights how high levels of patient engagement seem to be strongly associated with better rehabilitation outcomes [6]. In agreement with these results, consistent improvements in all rehabilitation tasks were observed as the patient became more interested, cooperative and involved in training.
Speech therapy sessions followed scientific recommendations for adult aphasic patients [24] and were adapted to the teenager’s characteristics. As literature suggests, familiar technology was incorporated for a more functional treatment [22]. After the rehabilitation period, the patient’s language improved, even more clearly at the follow-up evaluation, where he showed greater communicative intent and a general reduction of inhibition.
Concerning cognition, substantial evidence supports the effectiveness of cognitive rehabilitation after acquired brain lesions, highlighting how neuropsychological treatment can help patients learn and compensate for residual limitations in this area [24]. Cognitive tasks were mainly assigned to the patient using the software ERICA [21] and included computerized exercises based on advanced cognitive rehabilitation models. Problem-solving tasks were administered to improve executive functions while attention exercises were aimed at reducing impulsivity. The presence of executive functioning deficits is known to moderate and negatively affect the overall response to treatment [24]. Moreover, during adolescence, the brain is still changing and the frontal cortex, classically associated with the control of executive functions, is partially immature and still developing in an injured brain. Cognitive tasks require patients to create new strategies and consequently new neural circuits that replace damaged ones. During treatment, the complexity of each exercise was progressively increased as the patient showed better cognitive flexibility and self-monitoring skills. The patient’s profile showed a partial reappearance of difficulties after a period without any training for cognitive functions. This is consistent with other case descriptions that indicate nonsignificant decrements of performance between discharge and follow-up assessments [25]. Hence, we can infer that intensive treatment is effective and should be long-term in order to maintain results over time.
Physical and occupational therapies were individualized and exercises followed a task-oriented approach. Also, traditional physical therapy was utilized. Electrostimulation and hydrokinetic therapy were introduced too. Following recent findings [26], virtual reality activities were added and were well accepted by the teenager. At discharge, the patient showed general motor improvements, reaching good autonomy in postural changes, gait and ADLs. His advances remained largely unchanged at follow-up. Increased emotional availability and cooperation were observed over time with all of the team’s specialists.
In conclusion, this case highlights how an early, intensive and comprehensive multidisciplinary rehabilitation program following the Clinical Guidelines for Childhood Stroke Diagnosis, Management and Rehabilitation can lead to significant improvement in children after AIS. In accordance with the ICF model, the treatment was tailored to the patient’s specific needs, environment and personal factors, in order to obtain the best outcome possible and allow the child and his family to achieve a higher quality of life. Further studies with a larger number of patients are needed to support evidence of efficacy of childhood stroke rehabilitation related to Clinical Guidelines.
Footnotes
Acknowledgments
The authors would like to thank the patient and his family, as well as the World Health Organization for the permission to reproduce their material. All authors gave their consent to paper submission and approved the current version of the paper. They agreed to take public responsibility for all the paper’s content. The first two authors contributed equally to the work. In addition, the authors ensured that they have written entirely original work and appropriately cited or quoted the considered studies. No financial support for the research, authorship and/or publication of this article was received.
Conflict of interest
The authors have no conflict of interest to report.