
Abstract
PURPOSE:
Unilateral spatial neglect (USN), an inability to attend to one side of space or one’s body, is commonly reported in adult stroke survivors and is associated with poor outcomes. USN has been reported in pediatric survivors of stroke, but its impact is unclear. The purpose of this systematic review was to summarize and evaluate the literature regarding USN in pediatric stroke survivors.
METHODS:
PRISMA guidelines, Scopus, CINAHL, PubMed, and other relevant databases were searched with terms including “children”, “stroke”, and “unilateral neglect”, with the ages of participants limited from to birth to 18 years. Data were extracted from studies on the clinical presentation of pediatric USN, the assessment of this condition, treatment options, or USN recovery.
RESULTS:
A total of 18 articles met inclusion criteria. There were no current prevalence data available. USN presents similarly in children compared to adults. Several different USN assessments were used, however, there were little data regarding treatment options. Furthermore, the data suggest that not all children fully recover.
CONCLUSION:
This systematic review reveals a lack of quality research to inform the assessment and treatment of children with USN. Although the literature spans decades, there remain no guidelines for standardized assessment or treatment. Similar to adults, paper-and-pencil testing may be less able to identify USN than functional assessments. It is likely that there are children who struggle with undetected USN-related deficits years after their injuries. With a rise of pediatric stroke survivors, there is a pressing need for clinicians to be educated about USN in children, clinical presentations, assessments, and treatments.
Introduction
Unilateral spatial neglect (USN), a common condition in stroke survivors, is defined as the inability to attend to, respond to, or identify stimuli on one side of the environment or the body (i.e., difficulty paying attention to items on the left side) which cannot be explained by motor or visual deficits [1]. USN may be present in as many as 50% of adult survivors of right hemispheric stroke and is associated with poor functional outcomes, diminished safety, and longer hospital stays [2–4]. There are several case studies that demonstrate the existence of this phenomenon in children following stroke, however the consequences of pediatric USN are unknown [5–12].
In 2009, the incidence of pediatric stroke was estimated to be 2.4 per 100,000 children for perinatal ischemic strokes and 1.3 per 100,000 children for later childhood strokes which is 2–4 times higher than reports from previous years [13]. However, pediatric rehabilitation clinical best practices are scant with regard to guidelines for assessing and treating children who sustain brain damage including strokes. With growing rates of childhood brain injury and stroke, there is a pressing need to assure that critical impairments such as USN are optimally assessed and effectively treated.
One way to address this need is to compile what is currently known about the clinical presentation of USN, its natural resolution, available assessments, and treatment options for the pediatric population. A synthesis of the research literature will provide this necessary information as a guide for clinicians to gather knowledge on a rarely discussed topic, learn about assessment options, and make informed decisions regarding treatment options. A synthesis publication will also call attention to this often overlooked phenomenon in the pediatric population and provide clinicians and researchers with a succinct reference to find available USN assessments and treatments being performed in both clinical practice and pediatric stroke research.
Methods
Overview
A systematic literature review using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Guidelines was conducted in order to analyze current literature and identify assessments, pediatric USN clinical presentations, treatment options, and USN recovery rates in children following brain damage, including strokes [14, 15, 14, 15].
Search strategy
A systematic search of the literature on USN in children after brain damage, with no limits on publication year, was carried out in the following databases: PubMed, Cumulated Index to Nursing and Allied Health Literature (CINAHL), and Scopus. PubMed was searched using terms (“Stroke” [MeSH]) AND (“Perceptual Disorders” [MeSH]) with the filters English and Child: birth –18 years. SCOPUS was searched using terms (TITLE-ABS-KEY (stroke) AND TITLE-ABS-KEY (neglect AND (hemineglect OR auditory OR attentional OR spatial OR disregard OR hemispatial)) AND TITLE-ABS-KEY (child* OR toddler* OR infant* OR youth OR baby OR babies OR teen*)) with a filter for English language. CINAHL was searched with terms: (stroke AND neglect AND (hemi OR spatial OR disregard OR hemispatial)), limited to the ages of infant, child, and adolescent. Google Scholar, PEDro, and TRIP were also searched with no new results found. In addition, reference lists of relevant articles were screened for other potentially eligible publications.
Inclusion criteria
Two independent reviewers screened search results based on title and abstract. They then completed full-text review of articles appearing to address USN in the pediatric population. Due to the limited literature in this area, all full manuscripts were included (example: case studies), and materials such as conference abstracts were excluded. Articles were excluded if they addressed adult populations, did not address USN, included diagnoses other than brain damage, or involved hemispherectomy due to the different recovery process and prognosis. Full texts were reviewed independently by two reviewers and studies were included after achieving consensus.
Quality assessment
The quality of each study was assessed by two independent reviewers using a modified Downs and Black Checklist which includes 15 questions regarding the reporting of aims, participant characteristics, and statistics as well as internal and external validity [16, 17]. The modified Downs and Black Checklist is used when the literature does not include randomized controlled trials [18]. Each article was scored on a 1-point rating scale, except question 5 which was scored 0–2. When scoring case studies, questions referring to controls were marked N/A, decreasing their potential total scores. Ratings were totaled and reported out of a potential maximal score of 16. Cut-offs were used to group studies into “good” (≥71%), “fair” (54–70%), and “poor” (≤53%) [18].
Data extraction
Data were collected from eligible studies and in-cluded the first author’s last name, publication year and country, age and sex of subjects, assessments used and their psychometric properties if provided, treatments, descriptions of USN behaviors, and recovery timeline. Extracted data were reviewed and confirmed by a second independent reviewer.
Results
Literature search
The initial search resulted in 84 articles after removing duplicates. Twenty-five met the criteria for full-text review. Seven were excluded for not applying to the pediatric population (n = 2) or not referencing USN (n = 5), resulting in the inclusion of 18 articles (Fig. 1). They were published between 1984 and 2018 and included nine case studies [5, 19–24], one case report [7], four case-control studies [8, 25], one feasibility study [26], one cross-sectional study [27], one observational study [28], and one prospective study [10]. The articles addressed children ages 6 months to 17 years diagnosed with cerebral palsy, hemorrhage, traumatic brain injury, or stroke. Characteristics of included studies are provided in Table 1. No meta-analysis was performed due to the limited literature available.
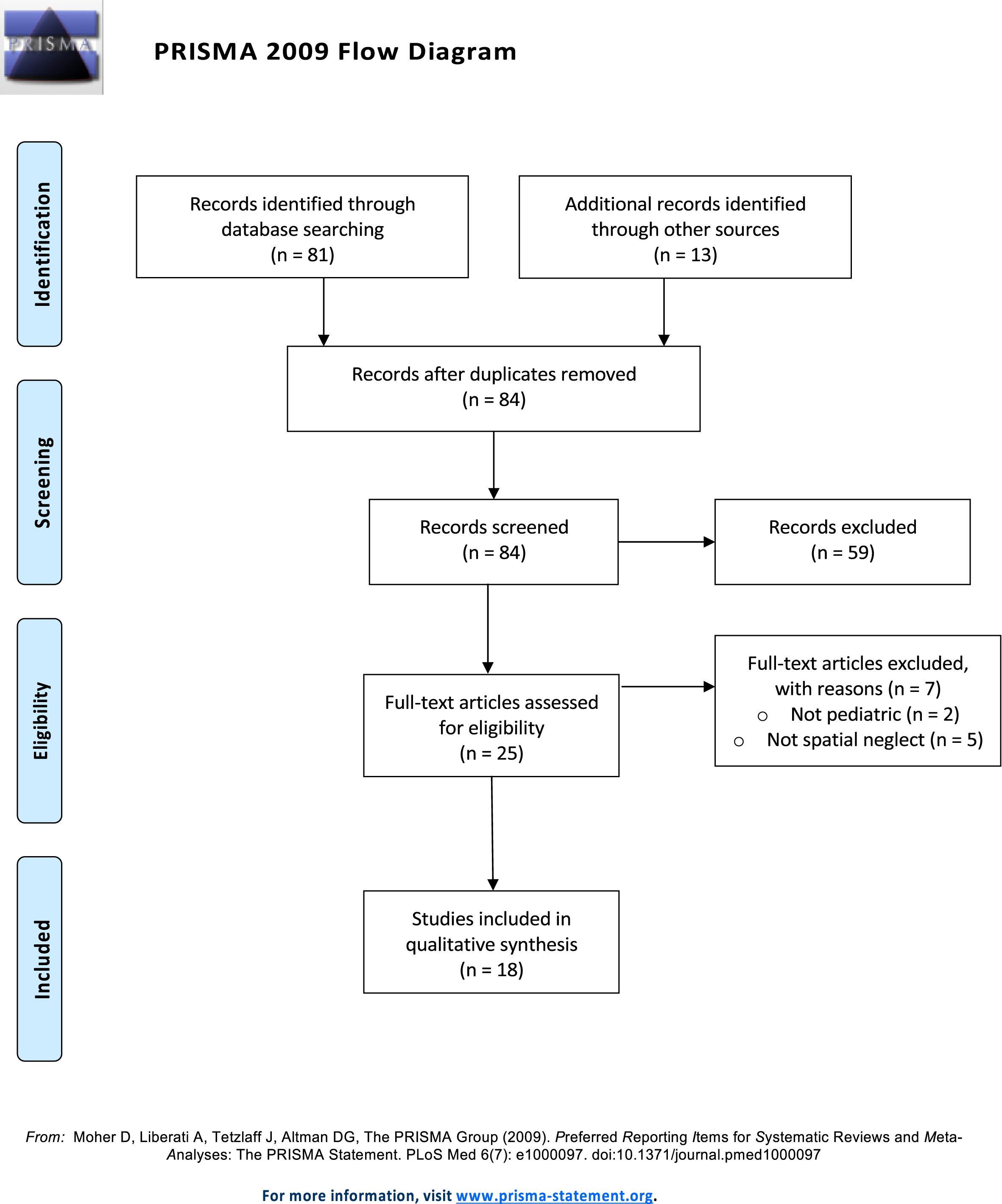
PRISMA 2009 Flow Diagram. This diagram describes the process from initial literature search, finding 84 articles, to final selection of included articles (n = 18).
Characteristics of included studies
Results from the Downs and Black checklist for study quality are detailed in Table 2 [16, 17]. Thirteen of the studies were of good quality [7, 20–28], two studies were fair [5, 29], and three were poor [6, 19].
Downs and Black Checklist
Downs and Black Checklist
All questions were scored on the following scale: yes = 1; unable to determine = 0; no = 0. Question 5 is an exception, with scores allocated yes = 2; partially = 1; no = 0. N/A = Not Applicable. 1. Is the hypothesis/aim/objective of the study clearly described? 2. Are the main outcomes of the study clearly described? 3. Are the characteristics of the patients included in the study clearly described? 5. Are the distributions of principle confounders clearly described? 6. Are the main findings of the study clearly described? 7. Does the study provide estimates of the random variability in the data for the main outcomes? 10. Have actual probability values been reported? 11. Were the subjects asked to participate in the study representative of the entire population from which they were recruited? 12. Were those subjects who were prepared to participate representative of the entire population from which they were recruited? 16. Were any of the results based on “data dredging”? 18. Were the statistical tests used to assess the main outcomes appropriate? 20. Were the main outcome measures used accurate (valid and reliable)? 21. Were cases and controls from the same population? 22. Were the cases and controls recruited over the same period of time? 25. Was there adequate adjustment for confounding in the analysis?
The extracted data are organized below in the following categories: USN behaviors, assessments used to detect USN, USN resolution, and USN treatment. The major focus of the results is on the assessments used to detect USN as that was most often addressed in the literature.
USN behaviors
A variety of symptoms were described that indicated USN. These behaviors fell into three main categories: those observed during paper-and-pencil tasks, visual attention, and functional activities. The majority of behaviors were related to visual attention and functional activities with only one author reporting behaviors of neglect seen during paper-and-pencil activities. These results are presented in Table 3.
USN Behaviors Described and Assessments Used
USN Behaviors Described and Assessments Used
There were a large variety of assessments used throughout these studies to evaluate USN. These were grouped into four categories; paper-pencil, visual attention, functional activities, and assessments created by clinicians. A total of 70 assessments are reported, with 45 of them detecting USN in at least some children. Results are displayed in Tables 3 and 4.
USN Behaviors Reported, Recovery, and Assessments Used
USN Behaviors Reported, Recovery, and Assessments Used
*
Treatment for Neglect
Paper-and-pencil assessments consisted of line bisection tests, cancellation tests, spontaneous drawing tasks, copying tasks, clock drawing tasks, and reading, writing, or arithmetic tasks. There were 33 reported uses of paper-and-pencil assessments in 12 of the studies. Twenty-one of these assessments successfully detected USN. These tests are described in Table 3, along with the corresponding study.
Visual attention
Several studies used visual assessments to detect USN. A majority of these were written visual attention and visuo-motor assessments that were not originally designed to detect neglect. However, some more functional visual attention assessments were used, such as measuring eye movements and visual gaze tracking. There were 19 visual assessments described as being used to identify USN in five of the studies. Ten of these detected neglect. Each of these is described in Table 3.
Functional activities
Several functional tasks were used as informal assessments of USN. Five studies reported four different functional assessments, and three of these identified USN. These are described in Table 3.
Clinician-created
Several authors describe USN assessments that they had developed themselves. Ten of the articles reported on eight different clinician-created assessments, and all eight were successful in identifying USN. These are described in Table 3.
Other
A few other assessments were used that did not fit into these broad categories. These included pro-prioceptive pointing tasks, simultaneous tactile stimulation, dichotic listening tasks, and diffusion tensor imaging. They are shown in Table 4 with their corresponding studies. All together, these other assess-ments were used six times in four studies, with three of them detecting USN.
Assessments that detected USN
Of the assessments described above, some were more successful in detecting USN than others. In Table 4, assessments displayed in bold were able to detect USN. Most of the assessments that detected USN were functional or clinician-created, while several of the paper-and-pencil evaluations were unable to detect USN in children who were demonstrating USN symptoms.
Psychometric properties of USN assessments
No psychometric data was reported for any USN assessment used.
USN resolution
Some studies had longer periods of follow-up and reported on the resolution or continuation of USN symptoms. These results are displayed in Table 4, with assessments bolded if they still detected USN after the follow-up period. Many of the children who were followed long-term continued to display USN after the time when it was previously expected that they would have recovered given the lack of long-term data assessing unilateral spatial neglect in children after unilateral brain damage.
Treatment
Of the 18 studies reviewed, only three addressed the treatment of USN. Bollea (2007) describes a 12-month treatment consisting of play activities, bimanual training, and developmental treatments [22]. These used selective contexts where a white board is placed on the non-neglected side to decrease distractions, while the toys and activities are placed on the neglected side. As the child progressed through a full year of treatment, they advanced from passive range of motion to more active treatments to help them meet developmental milestones. Konynenbelt (2015) described recommendations provided to a child’s father such as offering foods and toys on the neglected side, turning the child’s head while keeping their gaze forward, and spinning the child to activate the vestibular ocular reflex [12]. Riquelme (2015) used prism glasses as a treatment for USN while the children played games or completed ecological tasks such as stringing beads or placing coins in a bank [26]. Each child completed 2 sessions of 20 minutes and demonstrated after effects of midline gaze shifts toward the neglected side.
Discussion
The purpose of this study was to compile what is currently known with respect to the clinical presentation of pediatric USN, its natural resolution, available assessments, and treatment options. These results provide a resource for clinicians to better understand a rarely discussed topic, learn about assessment options, and review the limited treatment evidence currently available.
USN behaviors
While USN was evident in some writing tasks, gaze orientation, and tracking abilities, it was most commonly described during functional tasks [7, 24]. Children had difficulty with a variety of activities due to USN. Parents reported collisions while walking in both Johnston (1986) and Grossi (2001), resulting in injuries and difficulty in everyday life [6, 20].
Identifying USN symptoms is difficult in this population as it can be challenging to determine whether deficits shown by children are due to purely physical impairments or a combination of physical and cognitive impairments (such as USN). Assessing activities of daily living is an important part of any evaluation of a child with a brain injury. USN behaviors should be noted during these activities in addition to the physical difficulties they may have. These functional skills (eating, dressing, etc.) currently do not appear on the USN assessments described in this review.
Assessments used
Paper-and-pencil
Paper-and-pencil assessments were most commonly used in these studies. However, many of these tests did not successfully detect USN.
Line bisection and cancellation tests were able to detect neglect in some children. They also showed neglect often if provided other assessments, suggesting these written assessments may be unnecessary [30–34].
Spontaneous drawing may be a useful assessment for USN, as it would differentiate between allocentric and egocentric USN depending on whether the child drew complete pictures or filled the entire page. It is also a developmentally appropriate activity for children. Copying tasks may have many of the same benefits as a spontaneous drawing test.
Clock drawing assessments detected neglect in some children that other written assessments were unable to detect [35]. Performance on the clock drawing assessment seemed to be correlated with lesion location [35]. A clock drawing assessment is also able to help determine the type of USN (allocentric vs egocentric) but may have more limited use in children unable to tell time or understand analog clocks.
Reading, writing, and arithmetic tasks could be used as functional assessments of neglect because they can be made age-appropriate. These tests are physically simple to complete while being cognitively challenging which would suggest that they may be more sensitive at detecting USN than simpler tests. This idea is supported by adult literature stating that USN is revealed more often during more difficult tasks, as well as by Laurent-Vannier (2003) who reported that some children who had seemed to experience full USN recovery on assessments still demonstrated USN behaviors such as running into objects on the neglected side when tired or challenged [7].
Overall, it seems that the more functional/applicable to real life the test is, the better it may be at detecting USN. This is confirmed by the detection of USN more frequently on drawing tasks than line bisection or cancellation tests [5, 19]. This inconsistency could again be related to the increased cognitive demand on the child resulting in more USN behaviors being discovered. This is similar to what has been found in adults with USN [36].
Visual attention
Several tests used were not specific USN assessments. However, some of these visual-motor assessments were helpful in detecting USN. Thus, these tests may indeed detect USN, however, it is unclear whether they should be used in combination with or instead of assessments specifically for USN.
Eye movement measures may be more helpful than the written visual assessments. Saccadic latency and accuracy, visual reaction time, and the Gaze Orientation Scale all were able to identify USN [37]. This suggests that eye tracking measurements may be able to detect USN in younger children (e.g. infants, toddlers, preschoolers) who may be unable to complete other functional assessments or written assessments. They also could be used during functional assessments in older children to provide more information.
Functional activities
Very few functional assessments were reported in these studies. Children demonstrated USN behaviors during activities of daily living as reported by Lauren-Vannier (2003), while functional tasks were used by Grossi (2001) and did not detect USN [6, 7].
Clinician-created
Perhaps due to the limited number of formal functional assessments, many clinicians chose to create their own. Each of these were able to detect USN in patients. There were a wide variety of assessments which included tasks such as kicking skittles or locating toys, each designed for a specific patient population. While some of these may be more widely applicable than others, two of these have been replicated in other studies. The object removal assessment used by Bollea (2007) and Trauner (2003) is useful in that it can be adjusted for use with infants as well as older children with the simple addition of verbal instructions [8, 22].
The Teddy Bear Cancellation Test was developed as a pediatric version of earlier described cancellation tests [7]. This test may be more child-friendly but still has the limitations of cancellation tests, namely that they may be too simplistic to detect the subtle forms of USN that may persist chronically. This may be illustrated by the one child in Laurent-Vannier’s 2006 study who did not demonstrate USN on the Teddy Bear Cancellation Test, although showed USN in other life activities [10].
The numerous clinician-created assessments seem to suggest that clinicians prefer using more functional assessments over traditional paper-and-pencil assessments. However, further evaluation is needed to determine the sensitivity and specificity of these clinician-created assessments.
USN resolution
Almost all children followed long-term were still demonstrating signs of USN months or years after injury. This suggests that clinicians need to assess USN in both the acute and chronic stages. The child in Johnston(1986) experienced their brain lesion during infancy yet failed a simulated driving test at the age of 14 due to inattention toward the left side [20].
Some studies also found that different assessments may suggest a full recovery while others are able to detect more subtle deficits. This may suggest that children learn to compensate quickly on easier tasks (such as the line bisection test) but have difficulty on more challenging tasks as they age or develop new attention skills. This correlates with USN in adults, as they may learn to complete simpler paper-and-pencil assessments correctly yet still demonstrate signs of USN during functional, everyday tasks such as driving, grocery shopping, or preparing a meal [36].
Johnston (1986) describes a child who was able to pass several paper-and-pencil assessments including the line bisection test, yet during a more challenging test such as a driving test or functional walking task was still clearly demonstrating noticeable USN symptoms [20]. While USN assessments need to be functional and challenging in the acute stage, they should also continue to challenge children over many years so that USN is able to be accurately assessed and they are provided with the necessary treatment. Further investigation is needed into the timeline of resolution of USN as well as the process of USN resolution.
Treatment
Only three studies addressed treatment. Two were case studies, and one involved parent education and recommendations only. Of the two treatments presented, one did not address how long the effects lasted, and the other protocol was highly intensive and likely unrealistic for real-life application in a clinical setting [22, 26]. The lack of literature addressing treatment options suggests that more research is needed to determine what treatment is best for children with USN.
Limitations
The primary limitation is that the authors might have missed available literature because the search terms for USN were varied. In children, searching “neglect” resulted in studies of child abuse neglect. Therefore, as many qualifiers (hemispatial, etc.) as possible were included. There is a chance that studies not using these qualifiers or using “neglect” as a term may have been missed. Additionally, developmental disregard is a condition that may be similar to USN, though existing literature linking the two is scant, and thus was not addressed in this review [38, 39].
Another limitation of this study is the wide date range. Due to the small volume of material the search was not limited to a specific range of publication years, resulting in studies from 1984 until 2018 being included. Some of the older studies did not include details such as the citations of commonly used assessments. This contributed to some potential challenges with the use of the modified Downs and Black checklist, as several of the included articles were unable to be fully scored.
A third limitation is the variety of brain lesions included in this study. While the literature searches were primarily limited to stroke and cerebral palsy, other brain lesions were mentioned. The authors chose to include these conditions to provide the most information possible. However, the results could be confounded because the findings are not limited to a specific condition, such as strokes. This provides a potential shortfall in the way that USN presents itself throughout the developmental process as there may be differences between how children exhibit USN after injury versus how infants develop symptoms after their injuries.
Conclusions
The purpose of this systematic review was to compile current evidence on the clinical presentation of pediatric USN, its natural resolution, available assessments, and treatment options. The literature search yielded only 18 articles, the majority of which were case studies. Because of the limited literature, the results cannot point to definitive clinical recommendations. However, they do suggest the following: First, USN may be more evident in challenging vs. easy tasks. Second, the Teddy Bear Cancellation Test, eye tracking, and functional assessments appear to be the most sensitive for detecting USN. Third, USN may not resolve over time which suggests a need for repeated assessments as the child ages and engages in increasingly more complex behaviors such as driving. Finally, there is a great need for intervention studies to develop evidence-based treatments for these children.
Next steps
As previously stated, there are several needs in this field. There is currently no prevalence data as to how many children with brain lesions experience USN. In addition, because of the wide variety of assessments in use, it may be beneficial to the field to have a standardized functional assessment battery with a variety of age-appropriate levels. Virtual reality may be an option to build engaging and adaptable assessments and treatment tools. Moreover, there is a clear need for intervention studies that lead to treatment guidelines. The next steps in this area should begin to target these gaps and provide education for clinicians and parents that USN exists and should be addressed in the child’s plan of care.
Footnotes
Acknowledgments
This project was supported at least in part by the following: T32 DC0014435, PI: Dubno, “Interdisciplinary Research Training in Otolaryngology and Communication Sciences”, Role: predoctoral fellow; P20GM109040, PI: Kautz, COBRE in Stroke Recovery; VA 1 IK2 RX002420-01A2, PI: Grattan, “Improving Measurement and Treatment of Post-Stroke Neglect”.
Conflict of interest
The authors have no conflicts of interest to report.