
Abstract
PURPOSE:
The purpose of the study was to provide reference values for grip and pinch strength for healthy children and adolescents in India.
METHODS:
Grip and pinch strength were recorded for 900 participants stratified into 5 chronological age groups (5–6, 7–9, 10–12, 13–15 and 16–18 years). Grip strength was measured using a Jamar Dynamometer and pinch strength using a Martin vigorimeter.
RESULTS:
The difference in grip and pinch strength between age groups was significant (
CONCLUSIONS:
Findings from the present study provide reference values for grip strength, tip to tip, key and tripod pinch for healthy Indian children and adolescents from 5–18 years of age, which will be useful to guide rehabilitation outcomes in routine clinical practice.
Keywords
Introduction
Grip and pinch strength provide an objective score for the evaluation of hand function [1, 2]. Measurement of grip strength helps to grade the level of motor development, degree of disability, and effectiveness of therapy [3]. However, normative data of grip and pinch strength for children and adolescents across the globe is scarce [4, 5].
Hand grip strength is influenced by nutritional, demographic, and anthropometric factors such as age, gender and body size. Several studies have reported relationships between handgrip and pinch strength with age, Body Mass Index (BMI), gender and dominance [6, 7, 8]. The relationship of hand anthropometric variables with grip and pinch strength has not been reported adequately. People in different parts of the world have different body dimensions, which have an influence on grip and pinch strength.
Relationship between age and hand grip and pinch strength (grey bar is for males and black for females).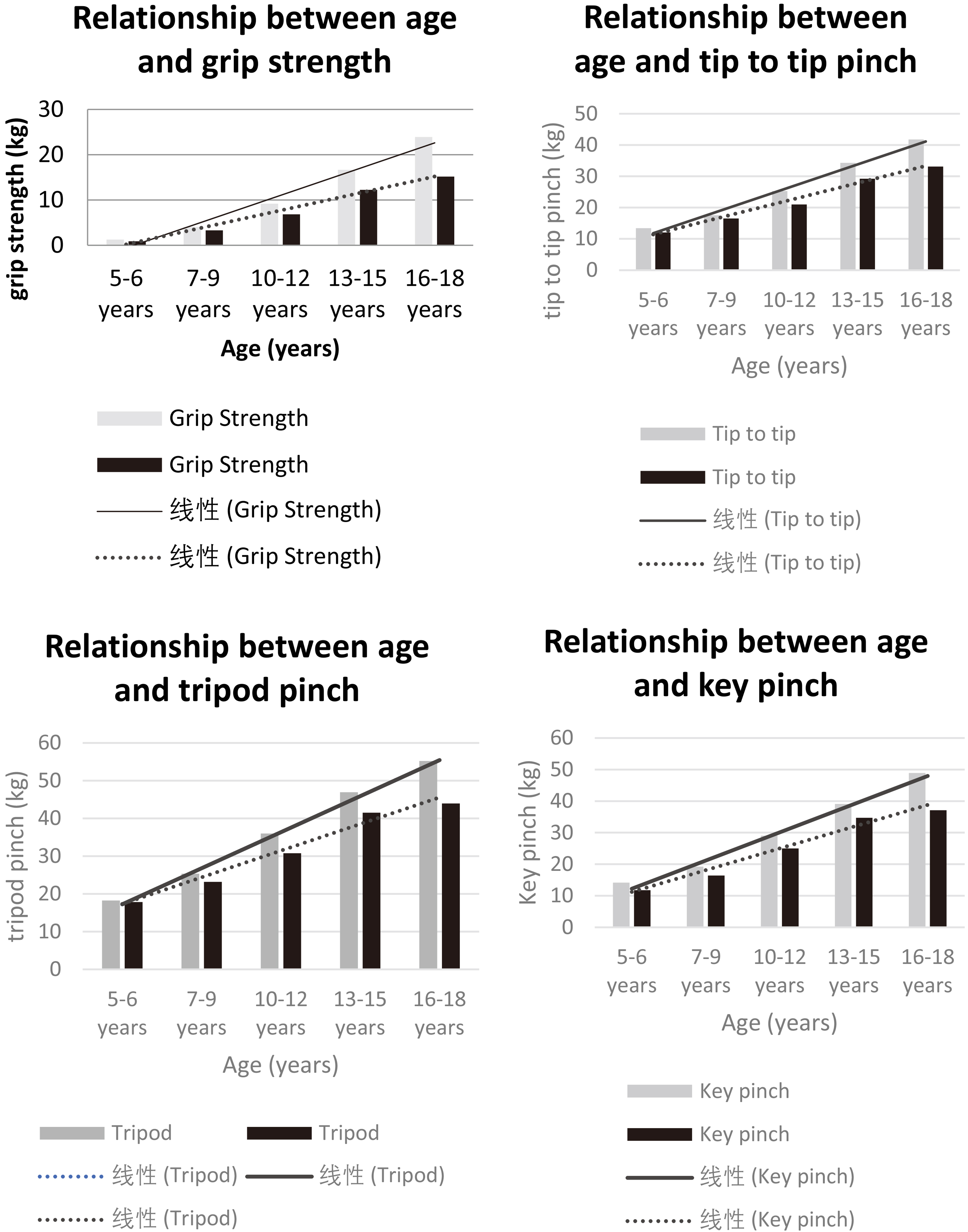
Reference values for grip and pinch strength for the pediatric and adolescent population are available from a few countries including Korea, Netherlands, British Columbia, Australia, United States, and Brazil [2, 3, 9, 10, 11]. However, the methods for obtaining these reference values are highly variable. In addition, the extant literature has established values from varying age ranges, making clinical application limited. Therefore, it would be difficult to compare grip and pinch strength across these five studies. Few studies from India have reported reference values for grip and pinch strength in pediatric and adolescent age groups and have explored associations of grip strength with influencing factors such as relevant anthropometric measurements, age, gender, dominance, and socio-economic status. A study in North India reported grip strength from 747 subjects between the ages of 6 to 25 years. However, a digital Takei dynamometer was used for assessment with the subject in standing position and elbow extended [12]. Another study conducted in West Bengal included 500 rural boys from lower income groups between the ages of 10 to 14 years, which only targets an age range and not the continuum of the pediatric and adolescent population [13]. Although two studies have reported hand function in Indian children and adolescents, a standardized method of measurement was lacking. Additionally, stratification based on chronological age groups was missing. Therefore, an attempt is made to study the influence of anthropometric variables with grip and pinch strength in children and adolescents from India.
Demographic characteristics
It is speculated that at certain critical milestones during growth, it is likely that the grip and pinch strength may vary which is why a composite value for the entire pediatric age span may not help clinicians to evaluate rehabilitation outcomes. Therefore, the present study was designed to generate reference values of grip and pinch strength in healthy Indian children and adolescents stratified in specific age groups. The influence of age, gender, hand dominance, and anthropometric variables on grip and pinch strength was explored.
Hand grip strength and pinch strength among children and adolescents: 5–18 years
Percentile values of grip and pinch strength in males and females aged 5–18 years
The study was conducted after obtaining approval from the Institutional Ethics Review Committee (IERC), MGM Medical College, Navi Mumbai. Nine hundred healthy children and adolescents between age group of 5 to 18 years studying in Mahatma Gandhi Mission Primary and Secondary School, Navi Mumbai, state of Maharashtra, India were recruited after the informed consent of parents and chief authority of the school. The school is located in an area of the city largely occupied by people hailing from middle socio-economic strata. Additionally, informed assent was sought from adolescents. Children with a history of trauma, neurological or musculoskeletal disorders, congenital deformity, or cognitive impairment were excluded. The dynamometer and vigorimeter were calibrated before commencement of the study. All measurements were recorded by the same tester.
Hand dominance was determined by asking each participant to pick up a pencil and draw a circle [11]. The American Society of Hand Therapists (ASHT) protocol was adopted in which the participant was seated upright against the back of a chair with feet flat on the floor, shoulder adducted and neutrally rotated, elbow flexed at 90
Hand span was measured from the tip of the thumb to the tip of the small finger. Palmar width was recorded by measuring the distance between the radial side of the second metacarpal joint to the ulnar side of the fifth metacarpal joint [13]. Hand length was measured from the tip of the middle finger to the midpoint of the distal wrist crease. Forearm length was measured from the head of the radius to the tip of the lateral styloid [14]. Arm length was measured by marking the inferior border of the acromion process to the external superior border of radius head [14]. Upper limb length was measured from the inferior border of the acromion process to the tip of the longest finger with both arm and hand in a full extended position [13].
Grip strength was measured using a Jamar dynamometer in kilograms of force (kg) [15]. The handle was set to second position for all participants. A Martin vigorimeter was used to measure pinch strength [15]. Pinch strength was measured using three types of pinches: tip to tip pinch, key pinch and three jaw chuck pinch. The authors attempted to measure grip and pinch strength from 3 years of age, but due to small hand span it was difficult for the younger children to grip the dynamometer.
An average of 3 measurements was computed for all measurements [4]. Data were analyzed descriptively using SPSS (Statistical Package for the Social Sciences, version 16). Mean and standard deviations were computed for all demographic variables, anthropometric measurements of upper limb, hand grip strength, tip to tip pinch, tripod pinch and key pinch variables. A one-way ANOVA was used to compare grip and pinch strength in different age groups. An independent t test was used to compare grip and pinch strength between gender and hand dominance groups. Pearson’s correlation test was used to study the association of grip strength with anthropometric variables (i.e., palmar width, hand span, hand length, arm length, forearm length and upper limb length) in different age groups. The significance level was set at 0.05 for all inferential statistics.
Results
Grip and pinch strength were recorded for 900 participants. Demographic details are presented in Table 1. The total sample was stratified into 5 chronological age groups of 5–6 years, 7–9, 10–12, 13–15, and 16–18 years. Fifty boys and 50 girls between 5–6 years of age were tested; all remaining age groups consisted of 100 boys and 100 girls.
Anthropometric variables such as palmar width, hand span, hand length, arm length, forearm length and upper limb length were measured. Mean values for grip, tip to tip, tripod, and key pinch strength for boys and girls in both the dominant and non-dominant hand are presented in Table 2. Percentile values for grip, tripod, tip to tip and key pinch strength for boys and girls are presented in Table 3. Comparison of grip and pinch strength between age groups was significant (
Correlation of dominant hand grip strength with upper limb anthropometric variables
Correlation of dominant hand grip strength with upper limb anthropometric variables
Our findings revealed strong positive correlation of all anthropometric variables with grip and pinch strength among males and females (correlation coefficient,
The findings of present study provide reference values for grip and pinch strength for children and adolescents aged 5 to 18 years in India. It was observed that mean grip and pinch strength was low compared to scores obtained in studies conducted in various continents across the globe [2, 3, 9, 10, 11] (see Table 4).
A recent systematic review reported that the hand grip strength of children and adults in developing countries was poor compared to those in developed countries [27]. The difference in normative reference values for grip strength between regions may be explained by differences in body size and composition including mean height and weight [27].
Cursory comparison of present findings with average values generated from the western population revealed that the hand grip and pinch strength of Indian pediatric and adolescent population was weaker. Shorter stature [19] and lower BMI of Indian children and adolescents compared to their age-matched counterparts across other continents could explain weaker hand grip and pinch strength [4, 20].
Hand grip and pinch strength was influenced by age, gender and anthropometric variables.
An increase in grip and pinch strength was observed with chronological age, consistent with previous studies [1, 3, 9]. It is reported that as a child grows, muscle bulk and cross-sectional area increases bringing about a change in muscle fiber type and motor unit distribution that causes an increase in muscle mass and strength which is likely to contribute to greater strength [20].
The least gender difference in grip strength was noted (0.35 kg) in the 5–6 year group and maximum gender difference (8.75 kg) was noted in the 15–18 year group. The least difference between males and females in tip (1.05), tripod (0.39) and key (2.38) pinches was noted between 5–6 years and maximum difference was noted to be 8.63, 11.28 and 11.83 in the 15–18 year group, respectively. Males demonstrated higher mean values in all anthropometric variables compared to age-matched females.
However, boys and girls demonstrated a strong influence of all anthropometric variables on hand grip and pinch strength. In the age group of 5–18 years, a strong positive influence of palmar width, hand span, hand length, forearm length and upper limb length on hand grip strength was noted (excluding palmar width in females). It is known that the isometric force exerted by a muscle is dependent upon its length when tested [21]. Hence, it is speculated that the greater the length of the hand, greater is the lever arm available for larger force generation resulting in greater grip strength. It can be recommended that anthropometric measurements should be taken into account to improve hand grip and pinch strength. The findings of the present study concur with previous studies which report positive correlation of hand grip strength with hand length, arm span, body height and hand circum-
Cursory comparison of findings from present study with studies reporting hand grip and pinch strength from different population groups
Cursory comparison of findings from present study with studies reporting hand grip and pinch strength from different population groups
ference. Hand and palm length also showed a positive influence with hand grip strength [22, 23, 24].
A major limitation of this study was that although the authors intended to report hand grip and pinch strength for children beginning with 3 years of age, it was not feasible to measure the grip and pinch strength with a dynamometer and Martin vigorimeter. Children aged 3 and 4 years demonstrated smaller hand span and were unable to position their hands to adequately measure hand grip and pinch strength. Another limitation of the study was that the overall nutritional status, activity profile, sports profile, and socioeconomic data were not recorded, which is likely to influence hand grip and pinch strength. Sample size estimation was not performed based on power analysis.
Conclusion
Findings from the present study provide reference values for grip strength, tip to tip, key and tripod pinch for the healthy Indian pediatric and adolescent population based on boys and girls from 5 to 18 years of age. A linear rise in grip strength was noted from the 5–6 year age group to 16–18 years. Boys demonstrated greater grip and pinch strength compared to girls in all age groups. No difference was found between the dominant and non-dominant hand. A moderate positive association was noted between grip strength and upper extremity anthropometric variables in the age group of 5–6 years. In the age group of 5–18 years, there was a strong positive association between grip strength and upper extremity anthropometric variables like palmar width, hand span, hand length, forearm length and upper limb length.
Footnotes
Acknowledgments
The project was funded by MGM School of Physiotherapy, Navi Mumbai; a constituent unit of MGM Institute of Health Sciences.
Conflict of interest
The authors have no conflicts of interest.