
Abstract
PURPOSE:
To conduct a systematic review of studies on non-surgical and surgical interventions for elbow flexion contractures secondary to brachial plexus birth injury (BPBI).
METHODS:
MEDLINE, EMBASE, PsycINFO, and CINAHL databases were searched for randomized controlled trials, observational studies, and case series studies on treatment of elbow flexion contractures secondary to BPBI. Study quality was evaluated using the Effective Public Health Practice Project tool.
RESULTS:
Of the 950 records found, 132 full text articles were reviewed, and 3 cohort studies and 8 case series were included. The overall methodological quality of included studies was weak. The weak quality evidence demonstrated that significant gains in elbow extension passive range of motion (ROM) can be achieved with serial casting (range: 15 to 34.5 degrees) or elbow release surgery (range: 28.4 to 30.0 degrees). At best, a reduction to an elbow contracture between
CONCLUSION:
The quality of evidence on the effectiveness of interventions for an elbow flexion contracture secondary to BPBI is weak. In the context of insufficient evidence on the risks of pursuing such interventions, it is prudent to attempt non-surgical interventions prior to surgery.
Level of Evidence
: III – systematic review of level IV studies
Introduction
Elbow flexion contractures secondary to brachial plexus birth injury (BPBI) are very common. On average, 50% of children with incomplete neurological recovery after a BPBI will develop a contracture [1]. Although these contractures are often mild (10 to 15 degrees), a third of these children will have contractures
Currently, the primary indications for treatment are severity of the contracture and whether the contracture negatively affects function or satisfaction with the appearance of the limb [4, 5, 6, 7]. The timing and decision regarding the type of treatment is dependent on the child’s unique functional, emotional, and practical needs [8]. Non-surgical interventions are typically offered prior to consideration of more invasive interventions [4, 6, 9]. These interventions include range of motion (ROM) stretching exercises, nighttime orthotics, dynamic spring-loaded orthotics, serial casting, and serial splinting [3, 6, 10, 11]. Non-surgical interventions are reported to reduce elbow flexion contractures in children and adolescents with BPBI [6]. Risks have been reported after non-surgical treatment including loss in elbow flexion ROM as well as radial head instability [6, 11]. Although rare, loss of elbow flexion passive ROM has been reported after serial casting [11], as well as transient loss in active elbow flexion ROM that recovered over time [6]. However, adherence to stretching and splinting is a factor associated with the success of this non-surgical treatment [6].
Surgical interventions are reserved for severe contractures [4]. Most often, an anterior approach to releasing the elbow soft tissue structures is used in conjunction with lengthening one or more of the flexor muscles [4, 9]. Anecdotal evidence suggests that the benefit of releasing the elbow is unclear because of the risk of losing active elbow flexion ROM, thus achieving minimal gains in the elbow arc of motion [4, 12]. It has been reported that lengthening the biceps brachii muscle in these children may negatively affect this muscle which was already weakened by the initial nerve injury to the brachial plexus [13]. Elbow flexion active ROM is critical for activities of daily living (i.e., hand to mouth function). As a result, the general opinion is that surgical management of these elbow flexion contractures is challenging and that outcomes of surgical release are disappointing [14]. However, it is also important to recognize that appearance-related concerns associated with a severe elbow flexion contracture are important factors in the child and family’s treatment decision-making process [15].
The synthesis and comparative effectiveness of non-surgical and surgical interventions for an elbow flexion contracture has not been explored. Therefore, the purpose of this systematic review is to synthesize the evidence on the effectiveness of non-surgical and surgical interventions of elbow flexion contractures secondary to BPBI.
Materials and methods
The methodology of this review was developed following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) [16]. The protocol for this systematic review was published on PROSPERO. MEDLINE, EMBASE, CINAHL, PsycINFO, and Google Scholar databases were searched from their inception until September 22, 2017. The search strategy was developed with an expert medical librarian. The MEDLINE search strategy is found in Appendix 1. The reference lists of key studies were also hand-searched for potentially eligible studies.
Study selection
The first author (ESH) and a research assistant screened all articles to remove all irrelevant titles and abstracts unrelated to BPBI. Next, two independent reviewers (ESH, JZ) screened the full text version of the articles using the following inclusion criteria: 1. Randomized controlled trial (RCT), observational and case series study designs, 2. Sample included participants less than 18 years of age with a clinical diagnosis of BPBI, 3. Intervention group underwent non-surgical or surgical treatment for an elbow flexion contracture, 4. Evaluation of elbow extension ROM in the affected extremity pre- and post-intervention, and 5. Post-intervention evaluation was at a minimum of 1-month follow-up. A control or comparison group was not required. The exclusion criteria were: 1. Non-English studies, 2. Studies of children or youth with traumatic brachial plexus injuries, and 3. Case studies. As such, this review should be interpreted within the limitation that the included studies were more likely representative of practices in English-speaking institutions.
PRISMA flow of information diagram [16].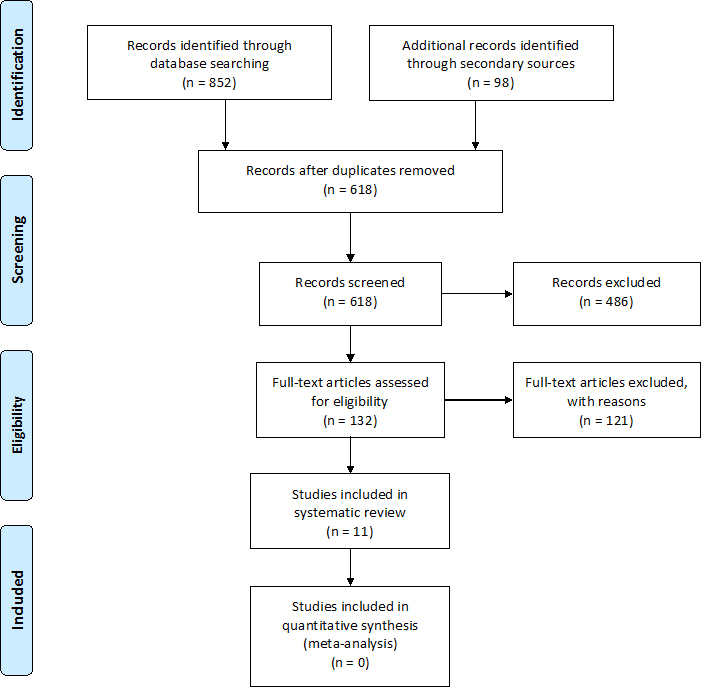
Data was extracted by the first author using a modified version of the Cochrane Consumers and Communication Review Group’s data extraction template and verified by a second reviewer (JZ) [17]. The information collected included authorship and publication details, study methods, participants, intervention and comparison groups (e.g., operational definition, integrity, co-interventions, adherence), outcomes (e.g., assessors, scale validity and reliability), and data analysis (e.g., statistics). The a priori primary outcome was change in elbow passive ROM in the affected extremity at a minimum of an average 1-month follow-up. The secondary outcome was change in upper extremity activity and/or participation from pre-intervention to the last available follow-up post-intervention, measured by observer-reported or patient-reported outcome measure at a minimum of 1-month follow-up. Meta-analysis was not possible due to the heterogeneity of the study design, population, and outcomes measured in these studies. Therefore, an integrative approach that synthesizes quantitative and qualitative data was conducted to analyze the data [18]. More specifically, common variables and themes among the study data were identified through data displaying and comparison.
Quality assessment
Two independent reviewers (ESH, JZ) administered the Effective Public Health Practice Project (EPHPP) [19, 20] quality assessment tool to evaluate the following domains of each study: selection bias, study design, confounders, blinding, data collection method, and withdrawals and drop-outs (Available from:
Non-surgical versus surgical treatment: Elbow extension rom at mean pre-, interim, and post-intervention follow-up times.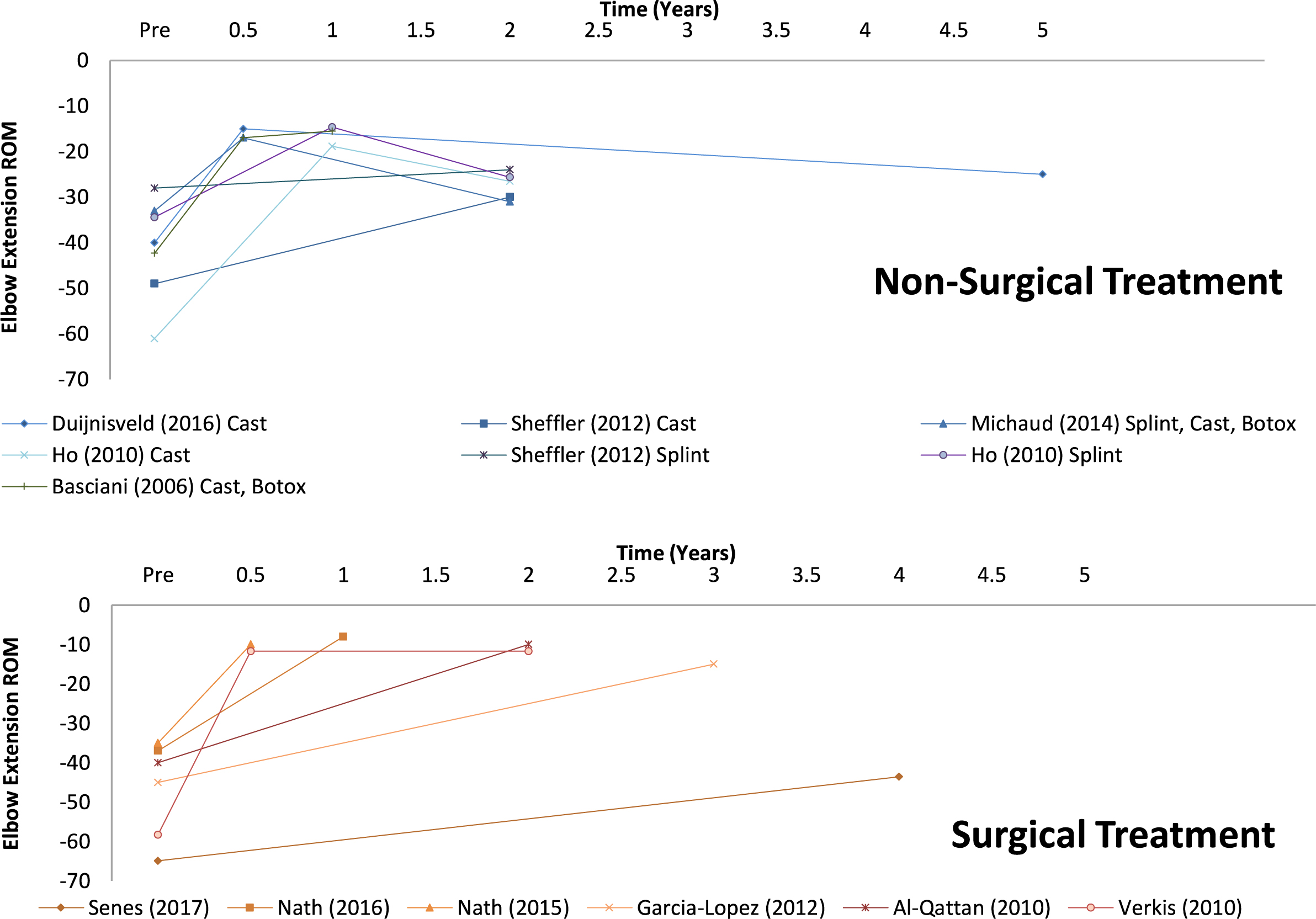
The PRISMA flow of information diagram for this review is illustrated in Fig. 1 [16]. Three cohort studies and eight case series were included in this review. Five studies evaluated the effectiveness of non-surgical treatment including serial casting, serial or dynamic splinting, and botulinum toxin type A injection to bicep brachii followed by serial casting or dynamic splinting. The remaining studies evaluated three types of surgical interventions: arthrodiatasis, humeral rotational osteotomy, and anterior surgical release of the elbow with muscle lengthening. The effectiveness of these interventions are reported based on the a priori primary outcome measure: elbow extension passive ROM. A visual overview of the results of these studies are presented in Fig. 2. The effectiveness of botulinum toxin type A as a stand-alone treatment for elbow flexion contractures in BPBI is not reported in this review because of the use of co-interventions including serial casting or the use of a dynamic elbow orthoses. As such, the two studies using botulinum toxin type A are represented in Fig. 2 with their respective co-interventions [21, 22]. The secondary outcome, upper extremity activity and/or participation as measured by observer-reported or patient-reported outcome, was not measured in the studies of non-surgical treatment. Two surgical studies evaluated patient/parent satisfaction using unstandardized measures [7, 23]. Garcia-Lopez et al. evaluated overall patient satisfaction with surgery, while Al Qattan evaluated parental satisfaction with the change in the appearance of the limb after the procedure. Overall, there was insufficient rigorous data to analyze patient-reported outcomes after treatment for an elbow flexion contracture. The characteristics of the eleven studies are summarized in Table 1. Only pediatric patients who received treatment for an elbow flexion contracture are included in this table.
Children with upper and total plexus injury were represented in the samples of surgical or non-surgical intervention studies (Table 1). The age range of the patients in each study are shown in Table 1. Three studies did not report this information. Non-surgical treatments were initiated as early as two years of age. While, the median lower age limit for the surgical interventions was 9.4 years, and earliest at four years of age.
Study Characteristics and interventions
Study Characteristics and interventions
P
Quality assessment of included studies
The overall methodological quality of included studies, as evaluated by the EPHPP Quality Assess-ment [20], was weak (Table 2). The highest level of evidence of included studies was four [24]. Three cohort studies were evaluated as moderate study designs (Tables 1 and 2), but did not have control groups [11, 21, 22]. Although, sample sizes were small (Table 1, Range
Effectiveness of serial casting
Four studies evaluated the effectiveness of serial casting (Table 3) [3, 6, 11, 22], including the study by Basciani and Intiso [22] that used serial casting concurrently with botulinum toxin type A injections. Although two of the four studies were prospective cohort designs, these are weak quality studies demonstrating that serial casting is effective in improving elbow extension ROM in children with elbow flexion contractures [3, 6, 11, 22]. In these studies, statistically significant improvement in elbow extension ROM was reported at final follow-up even though treatment effects were lost in two of the three studies that had interim follow-up [6, 11]. At final follow-up (Range: 1 year to 5 years), the mean/median improvement in elbow extension was between 15.0 and 34.5 degrees (Fig. 2) in the serial casting cohorts studied [3, 6, 11, 22]. In studies that documented more than two follow-up evaluations, the best-achieved outcome was a reduction to an elbow flexion contracture between
Two of the three studies that documented outcomes in elbow flexion strength using MRC demonstrated no change in elbow flexor muscle strength pre- and post-intervention [11, 22]. Duijnisveld et al. was the only study that reported pre- and post-active and passive flexion ROM outcomes. In this study, the median passive elbow flexion ROM significantly decreased from the initial 150 degrees to 140 degrees at 4 weeks (median) after serial casting, and then increased again to 145 degrees. Qualitatively, Duijnisveld et al. reported that four children in their cohort loss elbow flexion of 50 degrees or more [11]. However at final follow-up, the range in passive elbow flexion ROM was 125 to 150 degrees in the entire cohort. Ho et al. reported that
Summary of results
Summary of results
one patient had temporary loss in active elbow flexion ROM after serial casting [6].
Effectiveness of Progressive Splinting: There were two weak quality retrospective studies (case series, cohort) that demonstrate that the effectiveness of progressive splinting in reducing the angle of elbow flexion contracture secondary to BPBI is limited (Table 3) [3, 6]. Obtaining Ho et al.’s raw data on their sample (
Lastly, Michaud et al.’s (
There were four weak quality retrospective case series on a variety of approaches to surgically release of the elbow that included lengthening of either [23, 26, 27] or both brachialis and biceps brachii muscles (Table 1) [23, 31]. One approach included resecting the tip of the olecranon [27]. These cases series were all small samples (Range: 7 to 11) of children in their preadolescent or adolescent years (mean age
One weak quality retrospective case series reported on the results of three adolescents that underwent arthrodiatasis (closed distraction lengthening procedure) [25]. These patients were found to have a mean increase in elbow extension ROM of 46.7 degrees and an overall mean improvement in arc of movement of 55.0 degrees. Lastly, a weak quality retrospective showed that a mean improvement of 35.0 degrees of elbow extension ROM was experienced in case series of children who underwent derotational osteotomy of the shoulder to improve elbow ROM and appearance of limb [7]. However, statistical comparison of the intra-subject change was not reported in either studies [7, 25].
Active ROM in elbow flexion was reported in two of the six surgical studies [23, 27], which found that elbow flexion ROM remained the same pre- and post-surgery. There were four studies that evaluated elbow flexion muscle strength using the MRC that found no changes in flexor strength pre- and post-surgery [23, 25, 27, 31]. Similarly, Al-Qattan also reported no change in elbow flexion strength as measured by the modified Al-Qattan’s muscle grading system [7].
Lastly, the graphs in Fig. 2 illustrate the importance of interim and long-term follow-up after treatment for an elbow flexion contracture. Only one surgical study conducted an interim evaluation [25], while only one non-surgical intervention study did not provide more than one follow-up evaluation [3]. The interim evaluations were important in demonstrating loss in treatment effects at long-term follow-up after serial casting or splinting (Table 3, Fig. 2). For example, 20 (49%) of children in Duijnisveld et al.’s study had 37 recurrences of contractures
Discussion
Overall, there is weak quality evidence on the effectiveness of non-surgical and surgical treatment of elbow flexion contractures secondary to BPBI. The interpretation of these results are limited by weak study designs, small sample sizes, lack of long-term and interim follow-up, and omission in reporting pre- and post-elbow flexion active ROM and strength outcomes. However, statistically significant improvements in elbow extension passive ROM after serial casting or surgical release of the elbow joint with muscle lengthening were reported. In the studies of serial casting that reported interim outcomes, treatment gains were lost at long-term follow-up, although the overall degree of improvement was still statistically significant [6, 11]. One surgical study had interim follow-up data, but overall, no concerns with loss in treatment effects were reported in the surgical studies [25].
This review found insufficient evidence to support the effectiveness of the other non-surgical and surgical interventions reviewed. First, progressive splinting was not found to have a significant effect on reducing the degree of elbow flexion contracture. While treatment effects were lost for both serial casting and progressive splinting, the relative loss in treatment gains after serial splinting rendered this intervention less effective. However, it is important to consider that children who underwent splinting had milder contractures. Therefore, the potential magnitude of change (i.e., ceiling effect) was less compared to those who had casting. Further, children with milder contractures may have less motivation to adhere to treatment because 20 degrees of improvement from
A critical finding in this review was the lack of pre- and post-elbow flexion active ROM and strength outcome evaluation reported in both non-surgical and surgical studies. Although the MRC and goniometer ROM measures were considered favorable data collection methods in the quality assessment, challenges in its use of the MRC with the BPBI population has been identified [32]. The use of the MRC was problematic because it is not effective in children under 5 years of age, and there are different definitions of this scale, including one version that does not consider the ROM of the movement tested [33]. The authors of the studies reviewed did not specify if ROM was considered in the use of the MRC. As such, the use of the MRC scale in young school-aged children in both non-surgical [22] and surgical [26] studies should be interpreted with caution.
Reporting of elbow flexion active ROM outcomes were insufficient (i.e., two out of six studies) in the surgical studies in the context of the known risks associated with lengthening the elbow flexors. However, of those who measured these outcomes reported no change in elbow flexion strength and ROM. In the non-surgical studies, the loss in elbow flexion was transient in some patients and the overall degree of loss in elbow flexion ROM appeared minimal [6, 11]. More specifically, Duiijnisveld et al. found a statistically significant loss in elbow flexion passive ROM between initial, 4-weeks after casting and long-term follow-up times. However, these findings were in the context of a median 5 to 10 degrees of change in ROM at end range elbow flexion. The relative lack of variability in the degree of elbow flexion ROM (e.g., at initial evaluation, the median elbow flexion passive ROM was equal to the maximum value measured.) between patients may have also contributed to the statistical significance of these findings [11]. Further, final elbow flexion passive ROM was between 125 and 150 degrees in the entire cohort. Overall, in the presence of insufficient evidence on the safety and risks of pursing non-surgical and surgical interventions for an elbow flexion contracture, it is prudent to attempt less invasive interventions prior to discussing surgical options. This recommendation is also reflective of clinical practice reported in the literature. Surgery is typically reserved for youth with persistent severe contractures after failed attempts of non-surgical treatments, and if they have difficulty in performing daily activities and major aesthetic abnormalities are reported [4, 23].
In the studies reviewed, the timing of when non-surgical and surgical treatment were offered was reflective of the above clinical practice. On average, non-surgical treatments were initiated earlier than surgical interventions, thus children who had surgery were older. However, despite earlier initiation of non-surgical treatment, the nature of these contractures, as well as the progressive changes in the elbow joint may have contributed to the inability to achieve attain full passive ROM in elbow extension. Although the etiology of elbow flexion contractures are multifaceted [1], recent clinical and lab studies have shown evidence that a large contribution to these contractures is the effects of denervation at the time of the initial birth injury that causes failure in growth of the affected flexor muscles [1]. As such, the shortened and tight muscles may not have had the potential to achieve optimal length to allow full ROM. Further, bony changes to the radius and/or ulna, as well as radial head dislocations have been described [6, 34] that may have contributed to permanent changes to elbow joint ROM and inability to achieve full ROM with non-surgical and surgical treatment. Further investigations on the etiology and elbow joint pathology in children with elbow flexion contractures are needed to optimize management.
A major challenge of non-surgical interventions for elbow flexion contractures in BPBI is also sustaining treatment benefits over time. Treatment gains are made in the short-term, but not maintained because long-term nighttime splinting is essential after all non-surgical treatment to sustain treatment effects. One possible reason for the need for ongoing stretching with a nighttime splint is related to the potential etiology stated above. Physiological changes from denervation in the neonatal period that resulted in failure of growth in sarcomeres of the flexor muscles [35], may make stretching theses muscles to full length a difficult feat.
Another factor associated with success of non-surgical treatment is the challenge of treatment adherence [6, 11]. Nighttime splinting requires ongoing regular follow-up as the splint requires re-molding to ensure proper fitting in the growing child. As such, non-surgical treatment requires long-term commitment of time and resources (e.g., missing school, employment, travel to appointments) from the child and family. Adherence may also be affected by the youth’s motivation to straighten the elbow. This leads to the importance of evaluating the extent to which these interventions influence the individual’s daily function, and perceived satisfaction with appearance of the limb. Future studies on treatment adherence in this population is needed, and it is essential that both youth and parental perceptions and experiences with treatment are studied.
This review also identified a gap in the use of patient-reported outcome measures to evaluate the effectiveness of both non-surgical and surgical interventions for an elbow flexion contracture. Although eliciting patient and family satisfaction with treatment is a good start, future studies should elevate the importance of patient-reported outcomes further by using standardized questionnaires (e.g., Patient-Reported Outcomes Measure Information System – PROMIS,
Lastly, statistical comparison of non-surgical and surgical interventions were not possible in this review due to the weak quality of the studies and heterogeneity of outcome measures. However, this review provides an opportunity to discuss the observations that the treatment gains from serial casting were comparable to the gains achieved with an elbow release surgery. The range in pre-treatment angle of elbow contracture in the serial casting and surgical groups were comparable: casting was
The recommendations of this review should be considered within the context that the reviewers did not contact all the authors of the reviewed studies when information was missing or unclear. Although seeking clarification may have addressed some of the reporting issues, it was felt that this would not significantly improve the strength of the overall recommendations. The numerous issues of risk of bias and quality in the studies reviewed would still render the recommendations from this review as weak [36].
Conclusions
Overall, the quality of the evidence on the effectiveness of non-surgical and surgical intervention for an elbow flexion contracture secondary to BPBI is weak. However, this weak quality evidence demonstrated that significant gains in reducing the elbow contracture can be achieved with serial casting or elbow release surgery, although complete elbow extension passive ROM is not attained. Further, loss in treatment effects occur with non-surgical interventions if long-term nighttime splinting is not adhered to. The results of this review must also be interpreted in the context of insufficient evidence on the safety and risks of pursing non-surgical and surgical interventions, thus prudent to attempt non-surgical interventions prior to surgery. Scientifically rigorous long-term follow-up studies with interim evaluation that measure patient reported outcomes including functional and appearance-related concerns, are needed to further investigate the effectiveness of both non-surgical and surgical treatments.
Footnotes
Acknowledgments
The content of this systematic review, in part, has been used by the first author for personal use in a dissertation that will not be published commercially. The authors also wish to thank Willa Stevenson for her contributions to this review. This work was funded by the SickKids Perioperative Services Innovation Fund.
Conflict of interest
The authors have no conflict of interests to report.
Appendix 1
Medline search strategy
#
Searches
Results
1
exp brachial plexus neuropathies/or exp paralysis, obstetric/or exp brachial plexus/or exp birth injuries/or (“axillary plexus” or “brachial nerve plexus” or “brachial plexus” or “musculocutaneous nerve” or “neuralgic amyotroph*” or “plexus brachialis").mp.
33852
2
exp elbow/or exp elbow joint/or (“articulatio cubitii” or “cubital joint*” or elbow*).mp.
34932
3
exp contracture/or (contracture* or stiff*).mp.
91327
4
(infan* or newborn* or new-born* or neonat* or baby or babies or child* or youth or kid or kids or toddler* or boy* or girl* or adolescen* or teen* or juvenile* or p?ediatric*).mp.
4092490
5
(elbow? adj3 (flexion* or exten*)).tw.
5184
6
1 and 2 and (3 or 5) and 4
399