
Abstract
BACKGROUND:
The brachial plexus is a network of nerves exiting the spinal cord through the fifth, sixth, seventh, and eighth cervical nerves (C5-C8) as well as the first thoracic nerve (T1) to conduct signals for motion and sensation throughout the arm. Brachial plexus birth injuries (BPBI) occur in 1.5 per 1,000 live births. The purpose of this study was to determine the perceived change in musculoskeletal health-related quality of life of brachial plexus patients utilizing the Pediatric Outcomes Data Collection Instrument (PODCI). PODCI scores were examined along with the patient’s procedure history (surgical or Botulinum Toxin), extent of involvement and demographics.
PATIENTS:
A total of 81 patients from two to eighteen years of age from nine different states met the inclusion criteria of having a pre-procedure and post-procedure PODCI score along with a Narakas score from 2002–2017. These patients were seen at the Brachial Plexus Center, which is an interdisciplinary clinic at a large academic medical center
METHODS:
This retrospective study utilized PODCI data collected annually during their regular brachial plexus clinic visits. Upper extremity (UE) and global functioning (GFx) scores pre- and post-procedure were stratified by Narakas Classification. Data were analyzed using paired t-test and ANOVA testing.
RESULTS:
Patients with a Brachial Plexus Birth Injury (BPBI) had lower PODCI scores for UE and GFx when compared with the pediatric normative scores for age-matched healthy children. Scores in both UE and GFx domains were higher after procedure in the groups of Narakas I and IV. There was significant correlation between UE and GFx scores and documented first PODCI score (2 years of age) and age at intervention (5 years of age).
CONCLUSION:
Procedures increased the perceived quality of life for children with a BPBI and increased their overall PODCI scores for both UE and GFx.
Introduction
The brachial plexus is a network of nerves exiting the spinal cord through the fifth, sixth, seventh, and eighth cervical nerves (C5-C8) as well as the first thoracic nerve (T1), which conduct signals for motion and sensation throughout the upper extremity (UE). A brachial plexus injury occurs when one or more nerves are damaged, resulting in limited shoulder, arm and/or hand function. Brachial plexus injuries are generally identified following birth or after a traumatic injury such as a motor vehicle collision. When the injury is identified around the time of the birth it is termed brachial plexus birth injury (BPBI). Previous terms for BPBI include birth brachial plexus palsy [1], birth brachial plexus injury, obstetric brachial plexus injury [2], obstetric brachial plexus palsy [3], neonatal brachial plexus injury [4], and neonatal brachial plexus palsy [5]. There is a higher likelihood of BPBI occurring when three or more of the following variables are present at birth: excessive maternal weight gain, labor longer than 61.5 minutes, maternal age greater than 26.4 years, tachysystole, or persistent fetal malpresentation [6].
BPBI occurs in 1.5 per 1,000 live births, resulting in varying degrees of functional deficit [7, 8]. Sixty to sixty-five percent of children with a BPBI recover without intervention, although 30–40% demonstrate residual deficits ranging from mild weakness to a flaccid UE [9, 10]. Musculoskeletal deficits may include a muscle imbalance, joint contracture, and/or shoulder joint deformities [11]. Appropriate non-operative treatment for BPBI may include Botulinum Toxin (BoNT) or interventions such as occupational or physical therapy [12, 13]. Surgical interventions may include nerve grafts, isolated nerve transfers, tendon transfers and/or osteotomies [11]. The selection of treatment depends on the extent of BPBI, which is commonly measured using tools such as the Narakas Classification, Active Movement Scale (AMS) [14], Mallet Classification [15], and Toronto Test Score [15].
The Narakas Classification was designed to identify the level of nerve involvement in a clinical setting when a newborn with BPBI is approximately 3 weeks of age [16]. The nerve injury is categorized as one of four levels based on the patient’s presentation. The initial purpose of this classification tool was to predict the recovery of patients with BPBI [17]. A Narakas I classification indicates the least nerve involvement with C5-C6 limiting shoulder abduction and external rotation along with limited elbow flexion and forearm supination. Narakas I accounts for approximately 73% of all BPBIs [10]. A Narakas II includes C5-C7 which adds weakness of the elbow and wrist extension to the previously listed limitations. Narakas III involves C5-T1 and adds weakness of finger extension and intrinsic muscles. Narakas IV is the most extensive, resulting in a flaccid arm and involving C5-T1 along with Horner’s Syndrome. An individual’s Narakas classification is not changed after it has been given; thus, this scoring system is not appropriate for measuring an individual’s response to treatment.
Narakas classification
Narakas classification
On the other hand, the Pediatric Outcome Data Collection Instrument (PODCI) is designed to measure an individual’s perceived quality of life in response to treatment. The PODCI was developed by the American Academy of Orthopedic Surgeons [18]. The PODCI is also known as the AAOS/POSNA Outcomes Instrutment [18]. The PODCI has been validated for pediatric musculoskeletal conditions and shown to be sensitive to change over time. Within the PODCI scoring there are six subscales: Transfers and Basic Mobility, Upper Extremity and Physical Function (UE Function), Sports and Physical Function (Sports Function), Pain/Comfort, Happiness, and Global Function (GFx) [18, 19, 20]. Scores are scaled from 0 to 100 with 100 being the highest level of perceived function or happiness [21]. The scoring is normative, which allows comparing scores between individuals even if they are different ages. A higher score indicates better functioning.
The purpose of this study was to determine the perceived change in musculoskeletal health-related quality of life of brachial plexus patients utilizing the Pediatric Outcomes Data Collection Instrument (PODCI). The study brings a new perspective not found in current literature. The relationship between PODCI scores, objective outcomes, and extent of injury (by Narakas Classification), was also analyzed.
This retrospective study was approved by the institutional review board at Cincinnati Children’s Hospital Medical Center and informed consent was waived. The age-appropriate PODCI questionnaire was given to all BPBI patients 2–18 years of age annually during their regularly scheduled clinic visits. All patient/parent age-appropriate pre- and post-procedure PODCI scores were collected. Procedure is defined as surgical intervention (e.g., isolated nerve surgery, humeral osteotomy, muscle release and/or transfer, glenoid osteotomy or wrist/hand procedure) or BoNT. Medical records of 361 BPBI patients between the ages of 2 to 18 years who were seen between January 2002 to August 2017 were retrospectively reviewed. Relevant data including age, sex, laterality, Narakas classification, PODCI scores and operative reports were gathered. The upper extremity and global functioning domains of the PODCI were collected because these were most relevant to BPBI. A total of 81 patients were included in the study, and baseline demographics are shown in Table 2. There were 18 patients who had a primary nerve surgery prior to initial PODCI.
Demographic and injury characteristics of patients with BPBI
Demographic and injury characteristics of patients with BPBI
Baseline characteristics of patients with brachial plexus birth injuries seen in the brachial plexus center between 2002–2014 (
Inclusion and exclusion criteria are as follows:
Inclusion
Brachial Plexus Birth Injury (BPBI) Ages 2–18 years of age at time of pre-procedure PODCI Documented Narakas Classification before 3 months of age Procedure such as a surgical intervention or BoNT One pre- and one post-procedure PODCI questionnaire was collected for each patient English primary language for patient and guar-dians
UE and GFx PODCI scores are higher after procedure. A) UE scores. B) GFx scores. Open boxes are pre-procedure scores, and filled boxes are post-procedure. 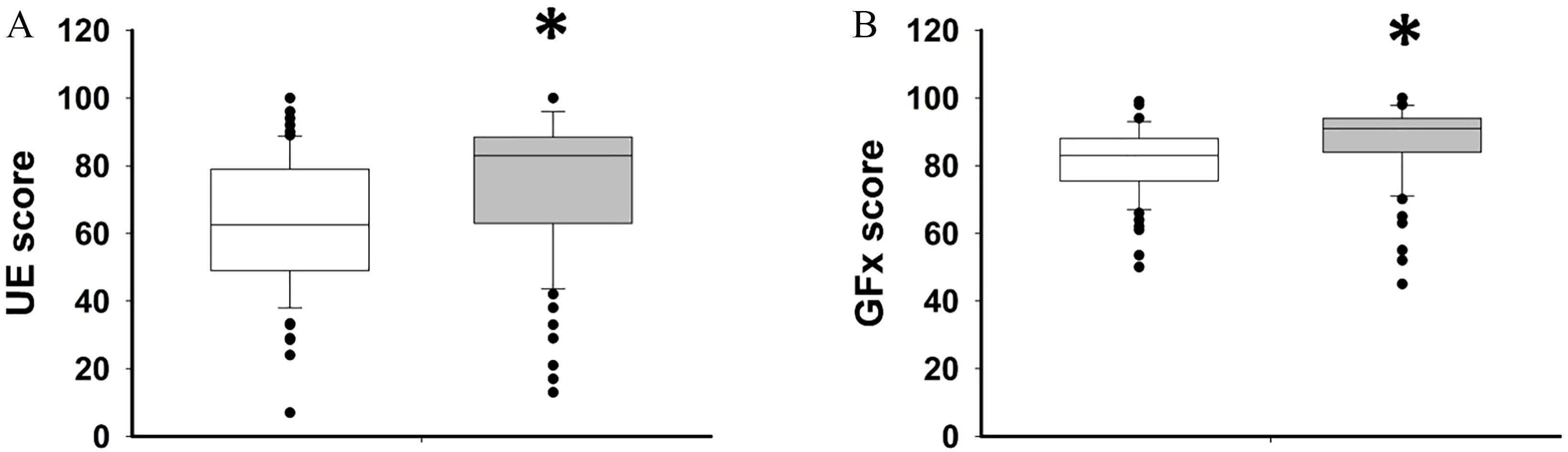
UE and GFx PODCI scores pre- and post-procedure, stratified by Narakas score. Scores in both UE (A) and GFx (B) domains were higher after procedure in Narakas 1 and 4 subgroups. Open boxes are pre-procedure and filled are post-procedure. 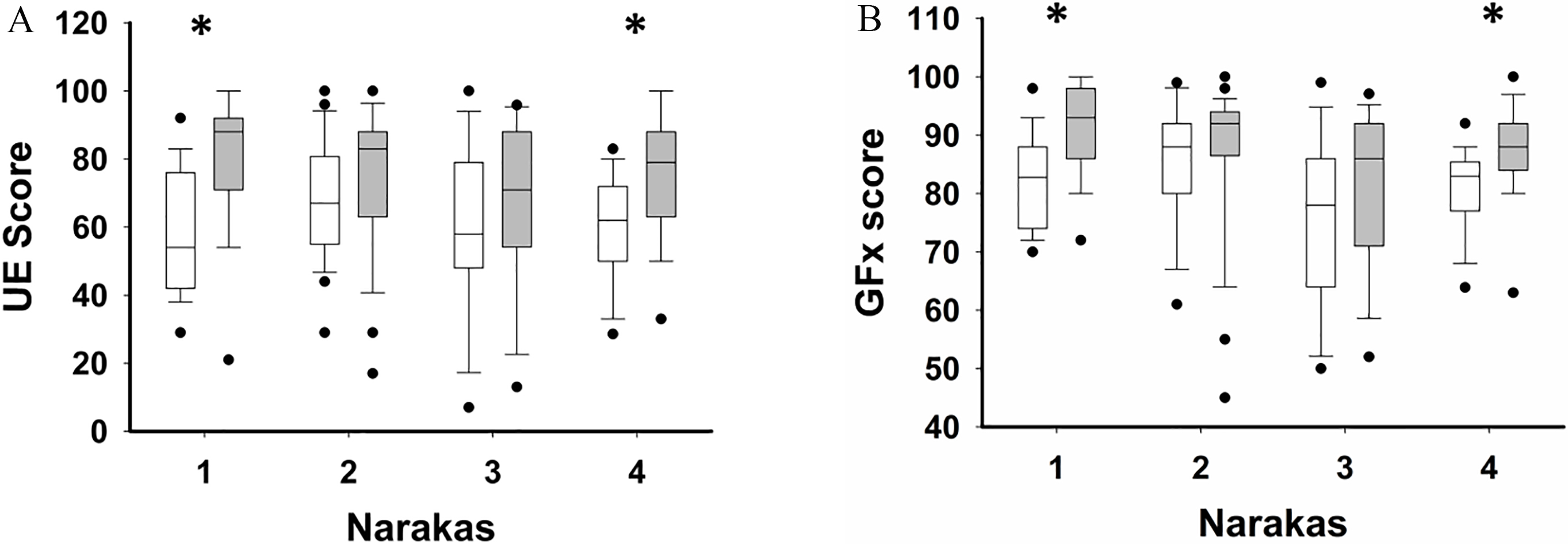
Exclusion
Traumatic BPI or Acute Flaccid Myelitis Patient did not have a surgical intervention or BoNT between PODCIs Incomplete PODCI scoring Children who had any other neurologic condition
Standard practice incorporated annual completion of PODCI questionnaires during patients’ regularly-scheduled clinic visits. All PODCI questionnaires were recorded on paper and collected during their visit. For patients with multiple interventions, their original PODCI was used in order to be consistent. Global functioning PODCI scores along with UE scores were compared with published pediatric age-matched normative data. All data were entered into a secured database and was calculated using normative scoring values. All of the values were rounded prior to calculation and are shown as whole numbers for presentation purposes.
Statistical analysis was done using the Sigma Plot software package (Systat, San Jose, CA). Aggregate pre- and post-surgical PODCI scores were analyzed using paired t-test. These data were also stratified by Narakas classification, and scores analyzed by 2-way analysis of variance (ANOVA) with repeated measures. Significant main effects were further analyzed using the Holm-Sidak post-hoc method. Data were transformed by square or square root as needed to satisfy normality and equal variance assumptions. The data were examined for evidence of factors that may influence outcome of procedure by using Spearman correlations between other collected data points and UE or GFx PODCI scores. Chi-square analysis was used to analyze number of surgical procedures by Narakas classifications. For the multiple correlation analysis, p value cutoff was adjusted using a Bonferroni correction. Otherwise, significance was set at
Results
Review of the initial 361 patient records resulted in a pool of 146 patients who had surgical intervention or BoNT. Of this group, 81 patients met the inclusion criteria of having a completed PODCI prior to and following surgical intervention or BoNT with a documented Narakas Classification. Table 2 shows the demographics of the patients included in this study.
Paired t-test showed that the included patients had a significant effect of procedure on both UE (
Summary of correlation analysis results
Summary of correlation analysis results
In each line, the R value (top) and p value (bottom) is displayed for each correlation. After Bonferroni correction, the only correlations that are statistically significant are UE score to Global Functioning score and age at initial PODCI score to age at procedure (both
Time between pre-procedure and post-procedure scores is not correlated with change in UE or GFx scores. Score changes from pre- to post-procedure for UE (A) and GFx (B) for each subject were plotted, and linear regression performed to examine the correlation between age change and score change. The solid lines indicate the regression line, with dotted lines representing 95% confidence limit. The equation and r2 values for the regression are indicated on the graphs. There was not a significant correlation between age change and score change for either UE or GFx scores.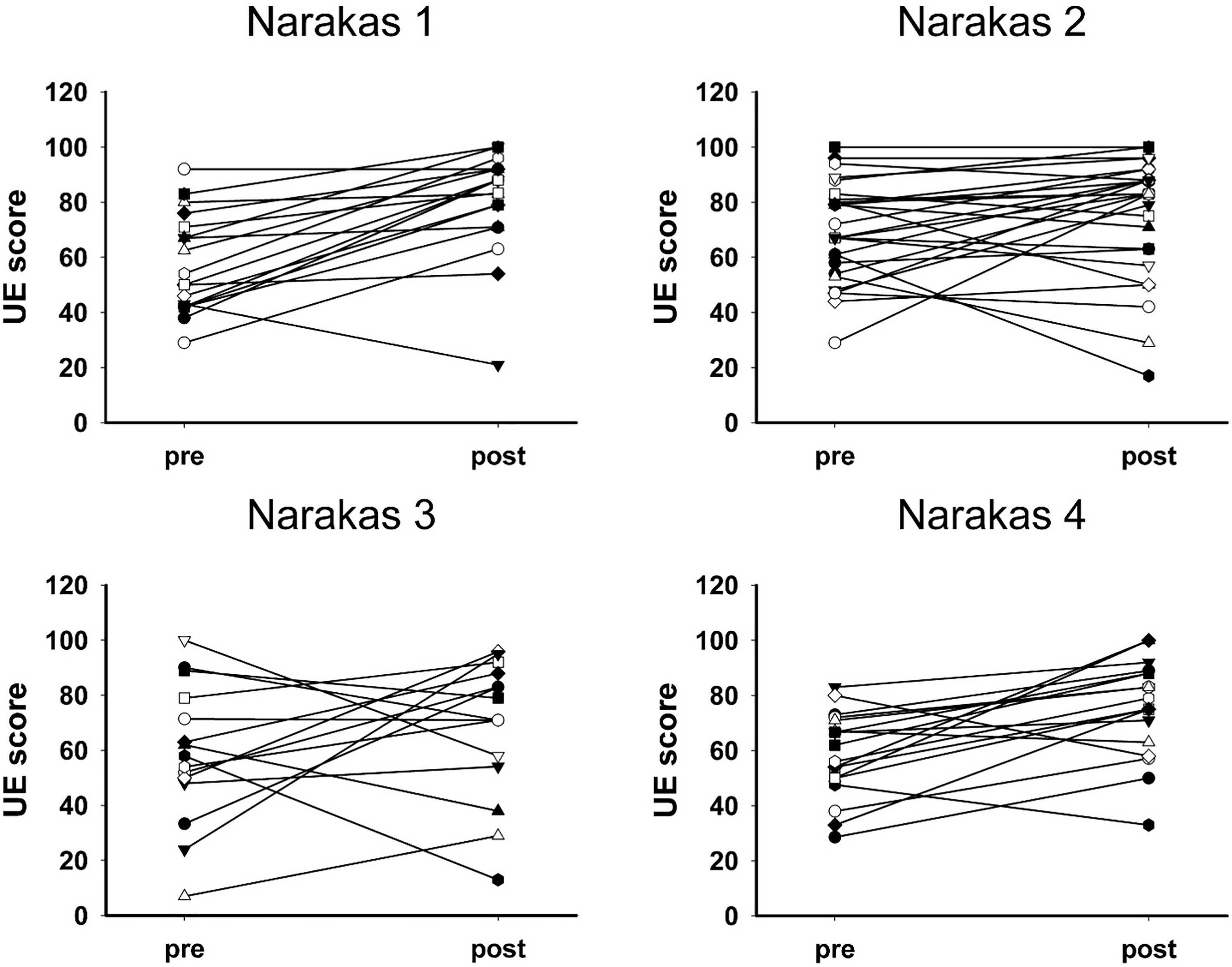
To investigate potential factors associated with improvement after procedural intervention, multiple Spearman correlational analyses were performed. Factors included in the multiple correlations were Narakas classification, affected limb (right versus left), and PODCI scores (UE and GFx subscales), initial age, age at procedure, time elapsed between initial score and post-surgical score, and number of procedures done (Table 4). There were no significant correlations of any of these factors with Narakas classification. There were significant correlations between UE and GFx scores (
Intervention and Outpatient BoNT injections with their associated Narakas Classification
Individual subject pre- and post-procedure UE scores. Scores are stratified for Narakas levels 1–4 (A-D, respectively). 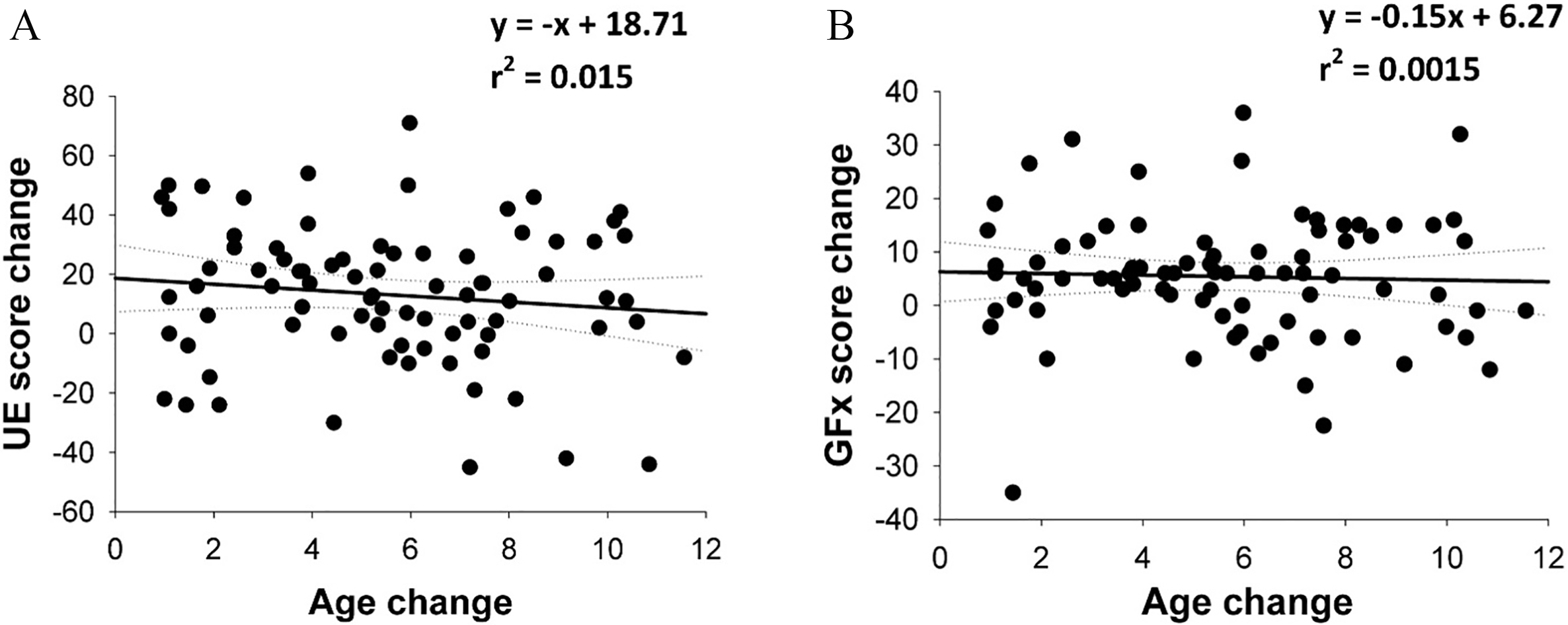
Individual subject pre- and post-procedure GFx scores. Scores are stratified for Narakas levels 1-4 (A-D, respectively). 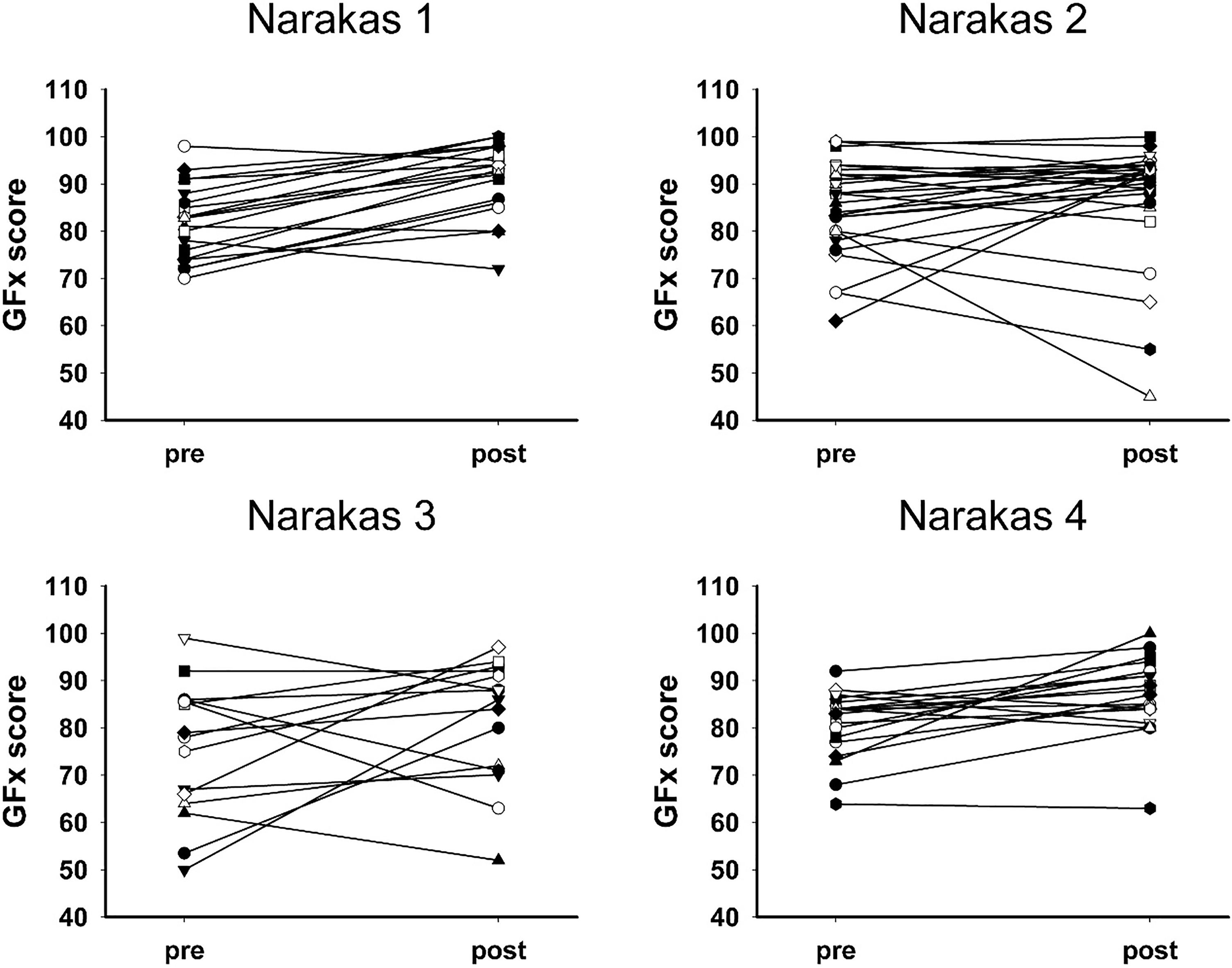
There were 19 Narakas I (23%), 28 Narakas II (35%), 15 Narakas III (19%) and 19 Narakas IV (23%) patients. There was an increase in PODCI UE and GFx scores across the board for all four Narakas groups. The greatest increases were noted for Narakas I and IV patients. Narakas I had an overall increase of 23 points with UE and 10 points in GFx after procedure. Narakas IV had an UE increase of 17 points and GFx increased 6 points. Additional details are noted in Fig. 1 for the Narakas II and III groups.
Table 4 shows the surgical interventions that the 81 study participants underwent. These included brachial plexus primary and secondary nerve surgeries, shoulder release and tendon transfers, biceps rerouting, humeral osteotomy, wrist tendon transfer, free gracilis muscle transfer, radial osteotomy and BoNT. By Narakas classification, there were 19 procedures performed on Narakas I patients, 28 on Narakas II patients, 15 procedures on Narakas III patients, and 19 procedures on Narakas IV patients.
PODCI scores of UE and GFx increased from pre-procedure to post-procedure. The increase was statistically significant in Narakas I and IV patients, but not in Narakas II or III patients. There was no correlation between age at procedure, number of procedures, sex, limb (left versus right) or either PODCI score changes or Narakas classification. Overall, these results support the idea that procedural intervention in children with BPBI improves perceived quality of life, as measured through UE and GFx PODCI scores.
Narakas I and IV patients have very different levels of nerve involvement; however, the surgical options for these two groups are clearly defined. Narakas I patients have specific deficits and there are specific surgery options such as a spinal accessory nerve to suprascapular nerve or a tendon transfer surgery. Narakas IV patients that have a flaccid extremity warrant a brachial plexus exploration nerve repair. On the other hand, Narakas II and III patients have intervention options but these options are not as defined as Narakas I and IV.
The PODCI is a well-validated outcomes assessment tool developed in 1994 by the American Academy of Orthopaedic Surgeons, Pediatric Orthopaedic Society of North America, American Academy of Pediatrics and Shriner’s Hospitals [22, 23]. It measures health-related quality of life in patients with musculoskeletal disorders. Squitieri et al. [22] identified the PODCI as easy to understand and complete when addressing specific functional issues associated with BPBI [24]. Parents and patients in their study preferred the PODCI and the authors found that comparing scores before and after the intervention can help treatment of the patient [24]. Normative PODCI scores range from 0 to 100, with 0 being the lowest perceived function and 100 being the highest. The parent completed the questionnaire for children 2–10 years of age, while patients 11–18 years of age completed it independently [12]. There are normative values for the following PODCI subscales: Transfers and Basic Mobility, Upper Extremity and Physical Function (UE Function), Sports and Physical Function (Sports Function), Pain/ Comfort, Happiness, and Global Function [25]. We specifically analyzed UE and GFx scales in the current study. The UE section measured difficulties encountered while performing activities of daily living and other activities involved in occupational performance. GFx is an average of the scores from the first four domains (UE function, transfers and basic mobility, sports and physical function, and pain and happiness/comfort). UE and GFx subscales are directly related to BPBI and upper extremity function.
Huffman et al. documented that individuals with BPBI had lower parent-completed PODCI scores compared to healthy normative data [20]. These patients also had significantly lower PODCI scores in UE, sports, and GFx versus the healthy control subjects. More importantly the PODCI showed promise as a tool for measuring perceived baseline and postoperative gains for BPBI patients [20]. These results suggested that perceived UE and GFx of patients with BPBI after a procedure are closer to normative scores for children in their appropriate age group.
The majority of prior literature regarding utilization of the PODCI with BPBI has shown lower PODCI scores in BPBI patients as compared to normative data [12, 20]. This is shown by Bae et al., who reported lower PODCI scores in patients with BPBI than those in the normative group [12]. Results of this study suggested that PODCI scores are useful for documenting perceived deficits in patients with BPBI as compared to healthy controls [12]. UE and GFx scales were specifically analyzed in the current study. The findings of the current study are consistent with Bae et al. as the BPBI patients had lower PODCI scores versus healthy normative data. Following procedural intervention, patients’ PODCI scores were closer to healthy normative scores.
Dedini et al. analyzed patients with BPBI who had a procedural intervention with documented pre- and post-PODCI scores. Dedini et al. [25] identified that the increase in post-operative PODCI scores was positively correlated with UE and GFx [25]. This is consistent with the current study findings, showing that procedural interventions are associated with increased UE and GFx scores. These increased scores are consistent with improvements in perceived function and quality of life after procedural intervention.
Narakas I and IV patients scoring changes were statistically significant and had increases in both UE and GFx scores. The equivocal findings in Narakas II and III’s may represent a fruitful area for future research in predicting who might benefit from procedural intervention, since some patients perceived benefit and others did not (as illustrated in Figs 3 and 5).
In this study, pre-intervention PODCI scores range from UE: 59–69 and GFx: 68–81. This is in comparison to reported scores for healthy controls that typically range in the mid-90s [22]. Although UE and GFx PODCI scores improved from pre-procedure to post-procedure, the post-procedure results remain lower than those reported for healthy controls. This suggests that decreased perceived function persists after procedural intervention, which is consistent with the center’s clinical experience. This further suggests that more work is needed to improve the ability to intervene in children with BPBI and that PODCI scores may be an important way to track perceived functional improvements obtained through intervention.
Although there were 983 PODCIs completed between 2002–2014, many of the patients lacked one PODCI (pre- or post-) score or Narakas classification; this caused much of the available PODCI data to remain unused. Lack of post-procedure PODCI occurred due to lack of patient follow up or patient/parent documentation. Narakas scores were unavailable if the patient was first seen after 3 months of age. A possible study limitation is the PODCI questionnaire because it was not created specifically for individuals with UE conditions or BPBI. BPBI patients are typically able to compensate well and often function using their own adapted methods which are potentially different than healthy aged matched children found in the normative data [9]. Lastly, data from one institution’s practice and lack of long term data could be seen as a limitation. Expanded research on the topic of perceived quality of life for individuals with BPBI, including multicenter involvement, is recommended for future consideration.
Conclusion
Brachial plexus birth injuries limit upper extremity function in children and adolescents. This study found that these deficits impact perceived quality of life noted through use of the UE and GFx sections of the PODCI. Both UE and GFx scores increased after a procedure particularly in Narakas I and IV patients. However, the specific characteristics examined in this study, including sex, age, left versus right arm, time since injury, and pre-surgical PODCI scores were not associated with changes in UE and global function outcomes.
Footnotes
Conflict of interest
The authors have no conflicts of interest.