
Abstract
PURPOSE:
To synthesize the evidence on the prevalence and etiology of elbow flexion contractures secondary to brachial plexus birth injury (BPBI).
METHODS:
Using Arksey and O’Malley’s scoping review framework, MEDLINE, EMBASE, PsycINFO, and CINAHL databases were searched, followed by a comprehensive grey literature search. Articles and abstracts of studies of all level of evidence on the prevalence, natural history, clinical presentation, etiology, and treatment of elbow flexion contractures in BPBI were included.
RESULTS:
Of the 884 records found, 130 full text articles were reviewed, and 57 records were included. The median prevalence of elbow flexion contracture in BPBI was 48%. The magnitude of the contractures was between 5 and 90 degrees. Contractures
CONCLUSION:
The etiology of elbow flexion contractures is multifaceted. The contribution of growth impairment in the affected muscles offers greater understanding as to why maintaining passive range of motion in these contractures can be difficult.
Introduction
Children with brachial plexus birth injury (BPBI) typically have elbow flexion contractures with 10 to 20 degrees deficit in extension [1]. However, contractures as severe as 90 degrees have been observed clinically [2, 3]. More severe contractures (
For children with BPBI, the flexed elbow also further exaggerates the limb length discrepancy in the affected limb [5]. The flexed position further shortens a limb that is already smaller in length and overall size [7, 8]. Although the average discrepancy of the affected side is approximately 95% of the length and girth of the unaffected limb, children and their families regard size differences as very important to them [8]. In this way, the contracture is also a cosmetic concern [5, 9, 10]. Further, the internally rotated posture caused by the common deficit in shoulder external rotation in these children positions the flexed elbow, forearm and hand in front of the body (Fig. 1), rather than in a more natural-looking position at the side. This may make the impairment in the arm more apparent and draws attention to the individual during standing and ambulatory tasks.
Left elbow flexion contracture.
Surgical intervention for severe elbow contractures involves variations of an anterior approach to release the skin, fascia, and capsule of the elbow joint in conjunction with the lengthening of one or more flexor muscles [11, 12, 13, 14]. The benefit of surgical release remains unclear because of the reported risk of loss in active elbow flexion [10] and the minimal gains in the active arc of elbow motion [15]. Non-surgical treatments including serial casting, splinting, night splinting and spring-loaded splints to improve elbow extension are effective in reducing elbow flexion contractures in children and adolescents with BPBI [1, 6, 17]. However, long-term adherence is a significant factor in the success of this treatment. Discontinuation of the splint or cast results in recurrence of the contracture and the loss of treatment effects [16]. Overall, long-term results of both surgical and non-surgical treatments are disappointing [18].
An understanding of the etiology of this condition is important to determine why outcomes of current interventions are unsatisfactory. The etiology of the elbow flexion contracture remains unclear, as the contracture occurs paradoxically in the presence of weak biceps muscle strength with equal or greater triceps muscle strength [19]. Several theories based on clinical findings have been proposed [19, 20, 21]. More recent laboratory studies focus on the physiological effects of denervation on the biceps and brachialis muscles as a potential cause of this contracture [3, 22, 23, 24]. Synthesizing the literature on the etiology of elbow flexion contractures will help identify what is known about these contractures and the gaps in our knowledge. This will help further our understanding of the nature of this problem that can then be applied to formulating best practices for the overall surgical and rehabilitative management of elbow flexion contractures.
A scoping review is best suited to consolidate the evidence in this emerging body of literature. This knowledge synthesis method “addresses an exploratory research question aimed at mapping key concepts, types of evidence, and gaps in research related to a defined area or field by systematically searching, selecting, and synthesizing existing knowledge” [25]. The purpose of this scoping review is to synthesize the evidence on the prevalence, natural history, clinical presentation and etiology of elbow flexion contractures secondary to BPBI.
To map the literature, this scoping review followed the six stages of Arksey and O’Malley’s framework: 1. Research question, 2. Identify relevant studies, 3. Study selection, 4. Charting the data, 5. Reporting the results, and 6. Consultation exercise [26]. The recommendations from Levac et al. [27] and Strauss et al. [28] were used to carry out the detailed methods of each step.
Research question
The primary research question was “What is known about the etiology of an elbow flexion contracture secondary to BPBI?” Secondary objectives of the review were to synthesize the evidence on prevalence, natural history, and clinical presentation of these contractures. Natural history was defined as onset, magnitude, and progression of elbow flexion contractures. Clinical presentation was defined as physical signs or symptoms associated with an elbow flexion contracture secondary to BPBI. Etiology was defined as any theorized cause, confirmed cause or manner of causation of an elbow flexion contracture secondary to BPBI.
Identify relevant studies
MEDLINE, EMBASE, PsycINFO, and CINAHL databases were searched from their inception until September 13, 2016. The search strategy was developed with an expert medical librarian at the first author’s (ESH) institution. The MEDLINE search strategy is found in Appendix. Key articles were used to identify Medical Subject Headings and keywords, as well as to evaluate the sensitivity of the search strategy. The references of key articles were also hand searched. Then, a comprehensive grey literature search was conducted including a search of Google Scholar on September 17, 2016, five key journals (Journal of Hand Surgery – American and European Volumes, Journal of Bone and Joint Surgery – American, Archives of Physical Medicine and Rehabilitation, and Journal of Hand Therapy), and the conference proceedings of the International Symposium on Brachial Plexus Surgery (Narakas Meeting) in 2011, 2013 and 2016. The websites of key national, non-profit organizations and hospitals (
Study flow of information diagram.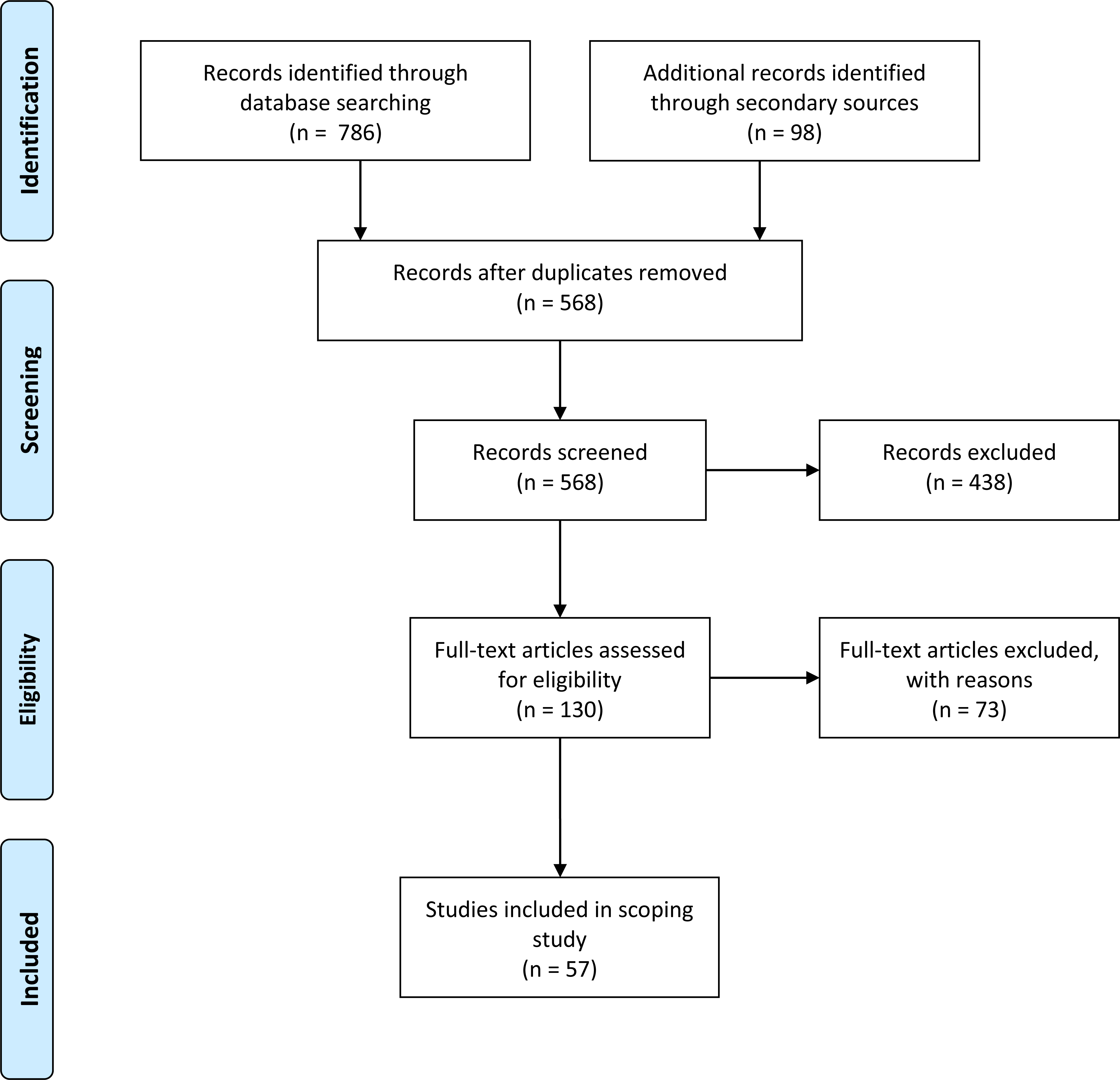
The process for selecting literature in a scoping study differs from a systematic review because the criteria are developed post-hoc based on the increasing familiarity with the literature [27]. In phase one, the first author (ESH) and research assistant reviewed the titles and abstracts. All articles and abstracts of studies of all level of evidence on BPBI as defined as a brachial plexus injury during the birth process were retained. In phase two, two independent reviewers (ESH, DK) screened the full text version of the potentially eligible citations that fulfilled the following inclusion criteria: articles and abstracts with information on the prevalence, clinical presentation, etiology, and medical management (treatment algorithm, non-operative or operative treatment) of elbow flexion contractures in BPBI. There were no exclusions at this point based on level of evidence [28]. However, the definition of expert opinion (Level 5) was expanded to include both review articles or any opinions expressed by an author in the introduction or discussion of a full-length study article (Level 1 to 4) that evaluated outcomes of elbow flexion contractures. All disagreements over study eligibility were addressed through discussion between the two reviewers (ESH, DK). Resolution was achieved for all discrepancies.
Charting the data
Arksey and O’Malley’s recommendations for charting the data were used by the first author (ESH) to begin the data extraction process [26]. After this initial process of summarizing data on the publication details, intervention, population, aim, methods, outcome measures, and results, the data were discussed with the research team. Expert clinicians (
Type of reports and population studied
Type of reports and population studied
*Of one retrospective case series and one retrospective cohort study.
* median, ** minimum 2-year follow-up, P
The PRISMA flow of information diagram for this scoping review is illustrated in Fig. 2 [29]. The primary search generated 786 records. Searching of secondary sources yielded 26 additional records from hand searching key references and a further 72 records from searching the Internet, Narakas conference proceedings, and key journals. After the duplicates were removed and the remaining articles were screened according to the process described above, 57 records were included. Figure 3 illustrates the increase in the number of reports on elbow flexion contractures secondary to BPBI over the last 25 years. The majority of reports were case studies (40%), followed by review articles (30%), cohort studies (18%), animal models (9%) and abstracts (3%) (Table 1).
Prevalence, clinical presentation and natural history
In studied cohorts of children with BPBI, the prevalence of elbow flexion contractures was from 25% to 89% (Table 2). The mean and median prevalence in these studies were 46% and 48% respectively. There were two studies isolated to children with upper trunk injuries (prevalence: 43%, 89%) [19, 30] while the remaining five studies included children with varying types of BPBI (Table 2). Comparative data on prevalence with respect to the severity of injury were not available in the latter studies [1, 31, 32, 33, 34]. Therefore, there was insufficient collective evidence to discern if contractures were associated with the severity of injury. While Van der Sluijs et al. [31] reported a relationship between severity of BPBI (as measured by the Narakas classification), with the development of an elbow flexion contracture, regression modelling was not conducted in their small sample (
Number of publications on elbow flexion contractures in BPBI per year.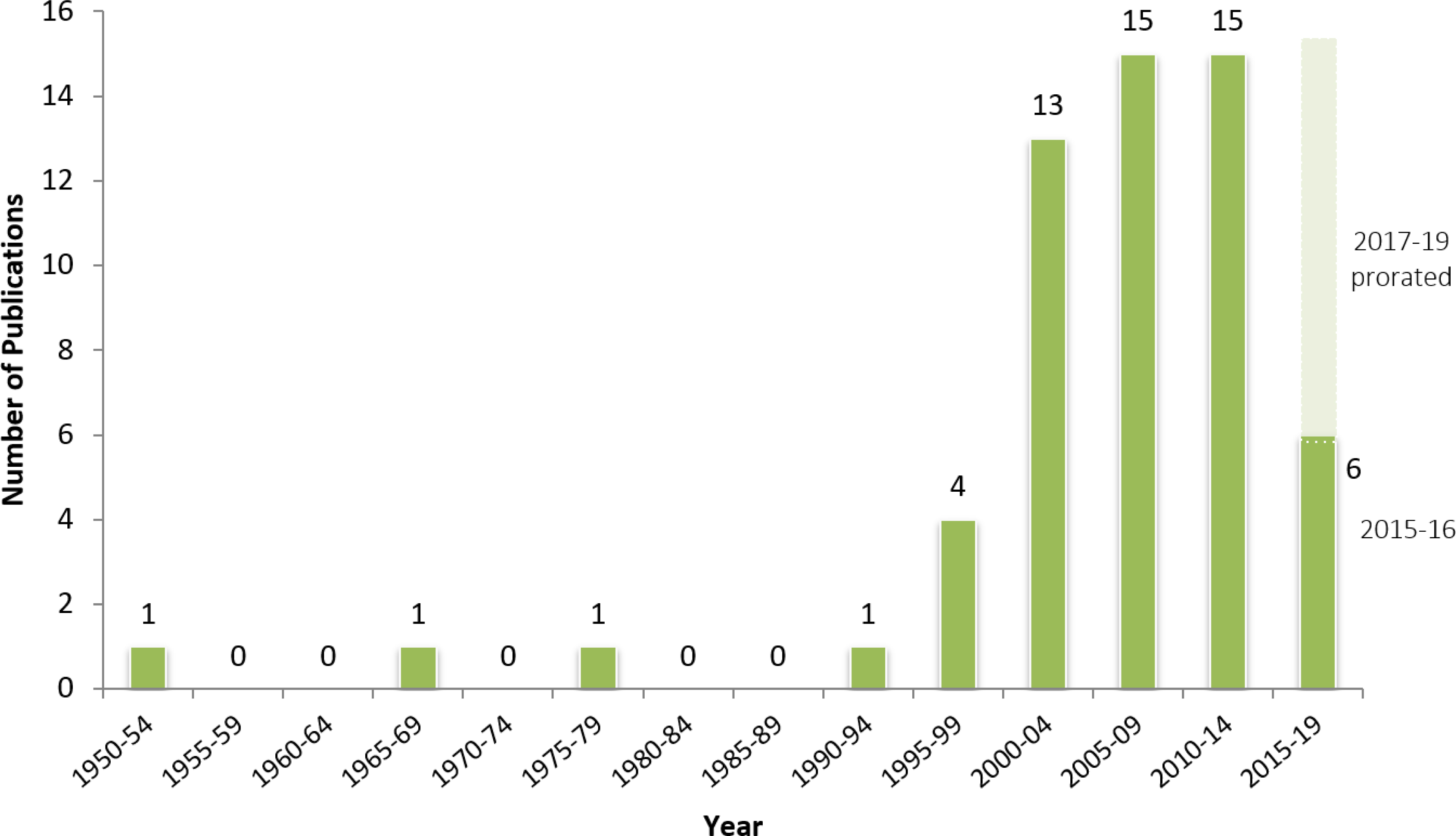
*Studies organized in descending chronologic order, **number of mice used for ErbB signalling experiments, y
Clinically, elbow flexion contractures may occur alongside a supination contracture [10, 19, 32, 35], pro-nation contracture [20, 36], or dislocation at the elbow joint. There were reports of posterior or anterior radial head dislocation, or combined radius and ulna dislocations [2, 34, 37, 38, 39, 40, 41, 42, 43], although, these types of osseous changes in the elbow joint were not always present [1, 44]. Elbow flexion contractures were not typically painful. For example, only 7% of patients in a long-term follow-up study of individuals (8 to 75 years) with elbow contractures secondary to BPBI (
The magnitude of elbow flexion contracture reported was between 5 and 90 degrees [1, 2, 9, 13, 14, 16, 18, 19, 21, 30, 31, 32, 33, 37, 38, 44, 48, 49, 50, 51, 52, 53, 54, 55, 56, 57], and severe contractures (
Elbow contractures were reported to develop gradually and be progressive [1, 5, 34, 37, 43, 46]. While the contracture was not present at birth after a BPBI [20, 43, 58], several reports of elbow flexion contractures secondary to BPBI at or prior to 6 months of age were found in this review [1, 19, 34, 37, 43, 56]. However, the overall literature indicated that the majority of contractures developed after infancy. For example, two anecdotal reports found that elbow flexion contractures began, on average, at 2 years of age [30, 43]. More rigorous evidence by Sheffler et al. in their retrospective cohort study found a median onset of elbow flexion contractures at 5.1 years (0.25 to 14.8 years) after the child’s initial visit to their clinic [1]. The rate of progression of the degree of contracture was 4.4% per year in patients prior to receiving conservative treatment. In children who did not seek treatment, the progression of the contracture was 0.1% per year [1]. This indicates that the progression rate of the contracture varies.
Early conjectures on the etiology of elbow flexion contractures described osseous changes to the elbow following immobilization of the elbow in a flexed position after BPBI in infancy (Table 3) [33, 42, 49]. However, splinting was not the only therapy intervention implicated in elbow flexion contracture development. Elbow dislocation associated with using the elbow as leverage during forceful passive range of motion exercises to counteract an internal rotation contracture at the shoulder was discussed in early reports where the resultant dislocation was presumed to cause an elbow flexion contracture [37].
After these initial reports, Ballinger and Hoffer [19]. conducted a study in 1994 that found that 85% of elbow extensors were at least one muscle grade (Medical Research Council scale) stronger than the elbow flexors in 34 children with C5–C6 injury who had elbow flexion contractures (Table 3). This provided evidence that muscle imbalance alone cannot fully explain the development of these contractures. However, imbalance in muscle strength may still be a factor, especially in cases of specific BPBI lesions that result in flexor dominance over extensors [36]. For example, in a total plexus injury with severe insult to C7, the elbow extensors may experience marked weakness compared to elbow flexors [17, 36, 59].
Since Ballinger and Hoffer [19] highlighted the paradox of elbow flexion contractures, the number of publications on elbow flexion contractures have increased (Fig. 3). Indeed, ten of the 12 studies reviewed were published after Ballinger and Hoffer’s study. The evidence from studies with the specific objective of determining etiological factors associated with elbow flexion contractures is summarized in Table 3. The majority of the evidence was based on anecdotal evidence from clinical observations. Several potential etiological factors reported based on expert opinion and clinical observations include: flexor domination over extensors due to earlier timing of reinnervation of flexors [19], elbow flexor training effect from therapeutic expectations or positioning preferences [9, 17, 18, 19, 54, 55, 60], fibrosis in muscle after birth trauma [20, 31, 35, 46], co-contraction of elbow flexors and extensors [1, 9, 14, 41, 43, 52, 61], and developmental motor apraxia [51]. There was one observational study that showed that overactivity of the long-head of the biceps brachii muscle is an associated factor in elbow flexion contractures [21]. The remaining studies investigated the characteristics of the elbow flexor muscles in BPBI. This includes five murine model studies.
Clinical evidence from imaging (CT, MRI) and murine models provide supportive evidence that elbow flexion contractures develop as a result of denervation in the upper limb muscles in the neonatal period (Table 3) [3, 62]. Injury to the brachial plexus outside the neonatal period may not necessarily result in such a contracture [3]. More specifically, the denervation process negatively affects the biceps brachii and brachialis muscles as demonstrated by evidence of fatty infiltrations, shortened length, and decreased cross-sectional area [3, 22, 31, 44, 56, 58].
Afferent innervation preservation has the potential to provide a protective effect on the denervated muscles by preserving muscle spindles through ErbB signaling activity [24]. Brachialis pathology was more significant than the biceps in both clinical and animal studies [23, 44]. Fibrosis of these muscles also occurs, but in the later stages of the contracture [23].
Implications of an elbow flexion contracture
The negative functional and aesthetic impact of these contractures due to the inability to achieve full elbow extension and the exaggerated limb length discrepancy was mentioned in many reports [1, 2, 3, 5, 9, 11, 12, 13, 16, 17, 21, 38, 41, 47, 50, 52, 60] Five studies provided a descriptive non-standardized account of the child’s and family’s concerns [2, 9, 13, 21, 47]. One study surveyed the opinion of surgeons who provide care to children with BPBI, and found that 50% of those polled viewed an elbow flexion contracture as a problem when the contracture is
Discussion
The collective clinical experience from this review indicates that elbow flexion contractures are a common sequela of BPBI that affects, on average, half of children with BPBI who have an incomplete neurological recovery. However, issues of both over and under-estimation of the prevalence are associated with the studies reviewed. An overestimation of the prevalence may occur because the children in these studies were more likely to have more severe injuries due to sampling from a clinic setting. Conversely, the retrospective nature of the six of seven studies reviewed relied on documentation of health care professionals on the presence and magnitude of these contractures in a clinical setting. Underreporting of contractures may be experienced due to errors of omission by attending clinicians in documentation or if the presence of a mild contracture was missed.
The majority of elbow flexion contractures are mild, but approximately a third of children with a contracture will have an extension deficit of 30 degrees or greater. When the contracture reaches this severity, theoretically it can have a negative impact on the child’s function during activities of daily living [4]. However, this review found that rigorous evidence on the functional and aesthetic impact of elbow flexion contractures secondary to BPBI is lacking. There is a gap in the literature on the activity limitation and participation restrictions caused by this impairment from the perspective of those with this impairment. Sheffler et al.’s study is helpful in highlighting some of the concerns with evaluating the functional and aesthetic impact of these contractures [21]. They reported that children with elbow flexion contractures secondary to BPBI had below normal performance on the PODCI upper extremity scale. However, it is difficult to isolate the effect of the elbow on overall arm function. A valid method of evaluating the functional and aesthetic impact of the elbow flexion contracture is difficult when the appearance, as well as motor and sensory function of the entire limb is affected after a BPBI. Elbow specific tools may be helpful, however most assessments of the elbow are not designed for this population.
This review found that elbow flexion contractures gradually progress during childhood. Sheffler et al. found a progression at 4.4% per year in patients prior to receiving conservative treatment [1]. However, it is important to consider, as stated by the authors themselves, that those who seek treatment are more likely to have more severe contractures. Further, it is unclear from this average rate what proportion of children did not progress at all. From their study, one can appreciate the difference in the progression of mild contractures, as those who did not seek treatment progressed 0.1% annually. However, identifying and directly studying those whose contractures do not progress at all is an important step to understanding the etiology and nature of this condition.
Therapeutic interventions may play a role in the presence and progression of this contracture. The historical evidence from this review demonstrated that using a splint to immobilize the elbow joint in flexion can lead to an elbow flexion contracture. This lesson was shown to be still relevant, as a report of an elbow flexion contracture after splint immobilization surfaced in 2014 with the use of the pilot version of the sup-ER splint [49].
Postural preferences may also play a role in elbow contracture development and persistence. Elbow flexion posturing may be advantageous for children with BPBI as a compensatory strategy to optimize upper extremity function. It can provide stability for gripping and manipulative activities in the presence of instability or weakness at the shoulder or wrist joints. As electromyographic evidence suggests, the elbow flexors may also be overworking as a means of stabilizing the shoulder [2, 21, 33]. Elbow flexion contractures associated with a shoulder internal rotation contracture may also contribute to the posturing of the elbow. Al-Qattan found a reduction in the degree of elbow flexion contracture after surgical correction of a shoulder internal rotation contracture with a derotational osteotomy of the humerus [9, 52, 60]. He postulated that the internally rotated position of the shoulder results in a compensatory abduction of the shoulder in order to optimize function of the limb. As a result, there is a preference to posture the elbow in slight flexion with the hand resting naturally in front of the body [60].
Lastly, this review clearly illustrates the evolution in the understanding of the etiology of elbow flexion contractures from anecdotal clinical observations to objective evidence from medical imaging and laboratory science. Evidence from murine models has advanced our understanding of the physiological causes of elbow flexion contractures and potential avenues to remediate this problem. There is clear evidence that muscle imbalance and fibrosis in the flexor muscles are not primary contributors to this problem. The evidence points towards the physiological response of muscle denervation that results in the failure of growth in the sarcomeres of the flexor muscles. More specifically, denervation results in loss of ErbB signaling in the muscle spindles. Interventions to improve the rate of reinnervation after injury or prevent denervation effects may help prevent the development of these contractures. Nikolaou et al. explored the effects of preserving afferent innervation to the muscle spindle in order to preserve muscle spindles and longitudinal growth of affected muscles [24]. Their findings offer direction towards exploring the potential of ErbB signal modulation as a mechanism to prevent the development of elbow flexion contractures after BPBI. It also spurs the need for clinical research to explore the effects of early reinnervation on the occurrence of elbow flexion contractures.
In summary, this scoping review identified that approximately 50% of children with residual impairment after a BPBI are affected by an elbow flexion contracture. The etiology of these contractures is multifaceted. Muscle imbalance does not play the primary role in these contractures, although it may still affect children with BPBI lesions who recover with significant weakness in elbow extensors. Similarly, splint positioning, postural preferences, and level of activity that uses the elbow through its full range of motion may play a small role in the occurrence, severity, and progression of contractures. However, the best evidence to date on the primary etiology of these contractures is that denervation of the elbow flexors in the neonatal period causes physiological changes that negatively impact muscle growth. Further investigations at a physiological level to study the changes to the implicated brachialis and biceps brachii muscles may help further our quest to remediate this problem.
Footnotes
Acknowledgments
The content of this scoping review, in part, has been used by the first author for personal use in a dissertation that will not be published commercially. The authors also wish to thank Ms. Willa Stevenson for her contributions to this review. This work was funded by the SickKids Perioperative Services Innovation Fund.
Conflict of interest
The authors have no conflict of interests to report.
Appendix
#
Searches
Results
1
exp brachial plexus neuropathies/or exp paralysis, obstetric/or exp brachial plexus/or exp birth injuries/or ("axillary plexus" or "brachial nerve plexus" or "brachial plexus" or "musculocutaneous nerve" or "neuralgic amyotroph*" or "plexus brachialis").mp.
31368
2
exp elbow/or exp elbow joint/or ("articulatio cubitii" or "cubital joint*" or elbow*).mp.
29344
3
exp contracture/or (contracture* or stiff*).mp.
71986
4
(infan* or newborn* or new-born* or neonat* or baby or babies or child* or youth or kid or kids or toddler* or boy* or girl* or adolescen* or teen* or juvenile* or p?ediatric*).mp.
3644717
5
(elbow? adj3 (flexion* or exten*)).tw.
4156
6
1 and 2 and (3 or 5) and 4
360