
Abstract
PURPOSE:
Measuring self-management behaviors in adolescents and young adults with chronic health conditions has become a priority in health care, yet there is a paucity of instruments that capture these behaviors. The purpose of this psychometric study was to evaluate the reliability and validity of the 17-item generic Adolescent/Young Adult Self-Management and Independence Scale II (AMIS II).
METHOD:
Data were collected from 201 adolescents/young adults (AYA) with spina bifida and 129 of their parents. Exploratory factor analysis, confirmatory factor analysis, Cronbach alpha, frequencies, Pearson correlations, and intraclass correlations were used to evaluate the data.
RESULTS:
The exploratory factor analysis of parent data supported two related self-management
factors (Condition Self-Management and Independent Living Self-Management). Confirmatory
factor analysis of AYA data confirmed these two factors and an overall scale with good
fit statistics (GFI and CFI
CONCLUSION:
Psychometric analysis supports this expanded measure of self-management for AYA with spina bifida. Evaluation of this instrument in AYA with other chronic health conditions is underway.
Background
The life expectancy for the
To successfully transition to adulthood and independent living, AYA must build these advanced self-management behaviors on an understanding and awareness of their chronic health condition [4]. They need to manage medications, order supplies, schedule health care appointments, and incorporate behaviors to prevent complications in daily life. In addition, self-management behaviors for living independently such as managing transportation, finances, insurance, and home maintenance are both critical and negatively affected by a chronic health condition [5, 6, 7]. The paucity of valid and reliable measures for capturing the full range of AYAs’ self-management behaviors limits our understanding of how successful self-management develops and its role in transition and health status. This is particularly important in clinical practice, as administration and interpretation of health risk assessment including self-management in AYA in transition is a billable service. However, a standardized, scored instrument must be used and recorded in the clinical documentation for the encounter in order for services to be reimbursed. The purpose of this paper is to delineate the development and psychometric data for such an instrument: the Adolescent/Young Adult Self-Management and Independence Scale II (AMIS II). The AMIS II, an expansion of the AMIS I, is a generic outcome measure that quantifies incremental achievement of self-management behaviors for AYA with chronic health conditions. Though a generic measure, the AMIS II includes three items that can be tailored to an individual’s condition.
Measuring self-management
Studies of self-management behaviors that have emerged in adults, adolescents, and children have primarily focused on arthritis or heart failure in adults and asthma or diabetes in children or adults [8, 9, 10, 11, 12]. Most of these studies have primarily used condition-specific measures of self-management [13, 14, 15]. While condition-specific measures may have value, it is not feasible to have a disease-specific measure for every condition. Furthermore, most of these measures do not typically address self-management behaviors needed for independent living. Generic measures may be useful in quantifying advanced self-management behaviors that bridge many chronic health conditions. Thus, they provide a common metric for describing the development and trajectory of self-management behaviors.
Recently, several generic measures have been developed for the assessment
of transition readiness in adolescents and young adults that cross chronic health
conditions. The Transition Readiness Assessment Questionnaire (TRAQ) [16], the STARx Questionnaire [17] and the TRxANSITION Scale [18]
each address somewhat similar domains important to transition or self-management and
emerged in the literature after the AMIS I but before the full psychometric testing of the
AMIS II. In the TRAQ, which is based on the readiness for change model, the AYA or parent
report on core skills in five domains. The reporter identifies if the adolescent “does not
know how”, “wants to learn”, “is learning”, “has started” or “always does when needed”.
The STARx Questionnaire measures overall transition readiness with three domains and items
scored never to always. The TRxANSITION Scale is administered by a trained professional in
an interview. The 3-response category used includes: 1
Several of the generic instruments do not measure the self-management behaviors that the AYA actually performs or do not offer enough item responses to demonstrate incremental achievement. Further, the KKIS-SB instrument was designed to be a parent-report or AYA-report questionnaire but only the parental data has been reported. While parent reports are critical, AYA perceptions of their own behaviors are an important component of planning for self-management and transition to independent behaviors. The AMIS II was developed to address these gaps.
The conceptual framework
Three conceptual frameworks influenced the development of this instrument: the Ecological model of Adaptation in Spina Bifida [20, 21], the Individual and Family Theory of Self-Management (IFSMT) [22], and the International Classification of Functioning, Disability, and Health (ICF) [23]. In the first framework, self-management is a key concept in adaptation. Definitions of self-management generally address developing a cluster of behaviors necessary to manage one’s health condition [24]. Review of the literature and analysis of qualitative interviews of adolescents with spina bifida (SB) led authors of this framework to adopt the following definition of self-management for adolescents with a disability/chronic health condition. The definition was adapted from Schilling et al.’s work with adolescents who have diabetes [25] (italics reflects adaptation).
An ongoing process of shared decision-making and responsibility among youth with
disabilities and their parents to achieve control of their condition,
health, and well-being through a wide range of activities and skills.
The goal of this increasing responsibility is to develop self-management
behaviors needed for transition to adulthood and independent living [22].
The second framework, the IFSMT, delineates self-management behaviors as the proximal outcomes of both the context (e.g., condition-specific, physical/social environment and individual/family factors) and the processes of self-management (e.g., knowledge and skills, self-regulation, social facilitation). As a proximal outcome, effective self-management behaviors contribute to one or more distal outcomes (health status, well-being or quality of life, and potentially reduced health care costs). Delineating and measuring self-management behaviors are central to this theory [22]. Finally, the ICF [23] model focuses not on impairments such as changes in motor function or sensation due to a disease, but on functioning. In addition, the ICF differentiates between capacity (or ability) and actual performance. In this model, self-management behaviors are the actual performance of behaviors that support full participation in society. The integration of these three frameworks led to: (a) an appreciation of self-management as an essential component of adaptation, (b) the identification of behaviors assumed to be central to AYA with a chronic health condition ultimately managing their own health care, and (c) the centrality of self-management behaviors to independent living and full participation in society.
In summary, self-management by AYA with chronic health conditions is an important outcome of comprehensive health care for youth. Self-management includes behaviors to both manage the health care condition and fully participate in the community. While there are a number of emerging measures of components of self-management, none to date address the incremental assumption of responsibility (with items that measure total assistance with activity needed; maximal assistance needed, moderate assistance needed, minimal assistance needed, or only supervision needed in order to implement these behaviors). In addition, there are few generic measures that accommodate condition-specific information. The AMIS II was developed in order to address this gap.
AMIS II exemplar items and definitions
AMIS II exemplar items and definitions
AMIS II development
The 17-item AMIS II was an expansion of the 10-item AMIS I [26]. Both the AMIS I and AMIS II are a structured
interview rated by health care providers. The AMIS I was initially developed by an
interdisciplinary team in order to be a practical measure of the adolescent’s increasing
responsibility for and implementation of self-management behaviors. Initially, the AMIS I
items were developed and definitions and scoring criteria were generated for each. Content
validity was then conducted using health care professionals, parents of AYA with a chronic
health condition and the AYA themselves [26].
One goal of the AMIS I authors was to create an instrument that was complementary to the
functional assessment measures addressing basic self-care and mobility, such as the
WeeFIM
Particularly useful were select items developed by Lollar in an early unpublished study of independence in disability. These items were adapted with permission for our expanded scale (D. Lollar, personal communication, March 2005). Lollar’s personal safety item was used in revising the AMIS I safety item that had a ceiling effect. Further, components of Lollar’s questions on problem solving, access, and family involvement were integrated into the AMIS II. Scale items addressing community living, insurance, condition knowledge, and complication prevention suggested by the qualitative data were also added. In addition, the socialization item that was inconsistently endorsed by the content validity experts for AMIS I was revised to address social communication. The knowledge, complication prevention, and medication items can be tailored to the individual’s specific condition. These changes resulted in a 17-item AMIS II. The overall scoring approach used in the AMIS I was retained for the AMIS II. Definitions and unique criteria for scoring were developed for each of the new or revised domains using the structure established with the initial 10 items (see Table 1 for exemplar items and definitions).
Evaluation of the AMIS II
Participants
In this psychometric analysis, AMIS II data were collected in three studies exploring adaptation and secondary conditions, and transition experiences in AYA with SB. The three studies included:
A feasibility study of adaptation included 9 AYA with SB aged
12–25 years of age (M A multi-site study of secondary conditions and adaptation in SB
included 131 AYA with SB aged 12–25 (M A multi-site study of transition experiences included 61 AYA with
SB aged 21–25 from sites in the East and Midwest (M
These studies yielded a total of 111 parents and 201 AYA for the psychometric analyses.
Characteristics of adolescent/young adult and parent participants
Characteristics of adolescent/young adult and parent participants
LOL
Inclusion criteria for AYA in each of the studies included: (a) no
previous documentation of intellectual disability, (b) English speaking, and (c) no
major health conditions (e.g., life threatening, progressive, or incapacitating
disabilities) other than SB. All studies used an in-person or telephone interview to
collect AMIS II data from parent or AYA. Telephone interviewers participated in
extensive training to establish inter-rater reliability. In the feasibility and
adaptation studies, data collectors established inter-rater reliability with the first
author (
All measures used for concurrent validity of the AMIS II were used
and described in our earlier study of the AMIS I with the exception of one measure
(Responsibility adolescent takes for care) [26]. Level of lesion, a measure of muscle innervations and an indicator of SB
severity, was abstracted from the medical record by a single investigator at each site.
Level of lesion was identified as sacral, lumbar, or thoracic. Adolescent
decision-making maturity was measured with the Adolescent Decision-Making Inventory, a
structured interview rated by the data collector. Decision-Making Participation was
measured by adolescent report on the Decision-Making Subscale of the Adolescent
Activities Inventory. AYA reported on this 19-item subscale. The five response patterns
for this this subscale are: the parent always decides; parent usually decides, AYA has
input; 50/50 decision; the AYA usually decides, parent has input; the AYA always decides
(1–5 scale). The parent report on the Chores subscale of the Adolescent Activities
Inventory was used to identify frequency of responsibilities and jobs in the home.
Response patterns included: does not do at all (1), does occasionally (2), or does
routinely (3). Finally, both the parent and adolescent report of self-care was measured
by 4 items from the self-care scale of the WeeFIM
Data analysis
In the current analyses, the data from parents in the feasibility and
adaptation studies (
Descriptive analysis was used to summarize characteristics of the sample
and variables used for concurrent validity. Preliminary analysis of parent data determined
if factor analysis was appropriate using Bartlett statistics, Kaiser-Meyer-Olkin statistic
(KMO), and index of determination. Exploratory factor analysis, using principal axis
analysis with an oblique rotation (delta
CFA using the AMOS 9 statistical software package was conducted to determine if the factor structure identified in the exploratory analyses of parents fit the AYA data. Substantial modification indexes indicating significant correlations were also included in the final structural equations model (SEM). CFA fit statistics criteria used to evaluate goodness of fit included:
Absolute Chi Square and relative Chi Square ratio which adjusts for
sample size (Chi Square/df) were used to evaluate the difference of data from the
model. A Chi-Square that is large and insignificant and a Chi square/df value lower
than 2 were used to indicate an acceptable model [30, 31]. The Goodness of Fit Index (GFI), Adjusted GFI (AGFI), and
Comparative Fit Index (CFI) where values at or near 0.90 indicate goodness of
fit [32]. The root mean square error of approximation (RMSEA) [33] scores less than 0.06 was used to indicate
good fit [32].
Cronbach alpha was used for internal reliability assessment and Pearson
correlations were used for assessing relationships between AMIS II scores and concurrent
validity measures. The measures used were known to be related but distinct from
self-management, thus a moderate relationship would be considered evidence of concurrent
validity for the AMIS II. The intraclass correlation (ICC) was used to evaluate stability
between administration of the instrument at a two-week interval and the relationship of
parent and AYA total AMIS II scores. ICC can be interpreted as 0.50–0.60 moderate; 0.70
adequate, 0.80 very good or strong; or 0.90 excellent [34]. The significance level for the correlation analyses was set at
Adolescent young adult self-management and independence scale standardized
regression coefficients, errors, and correlations.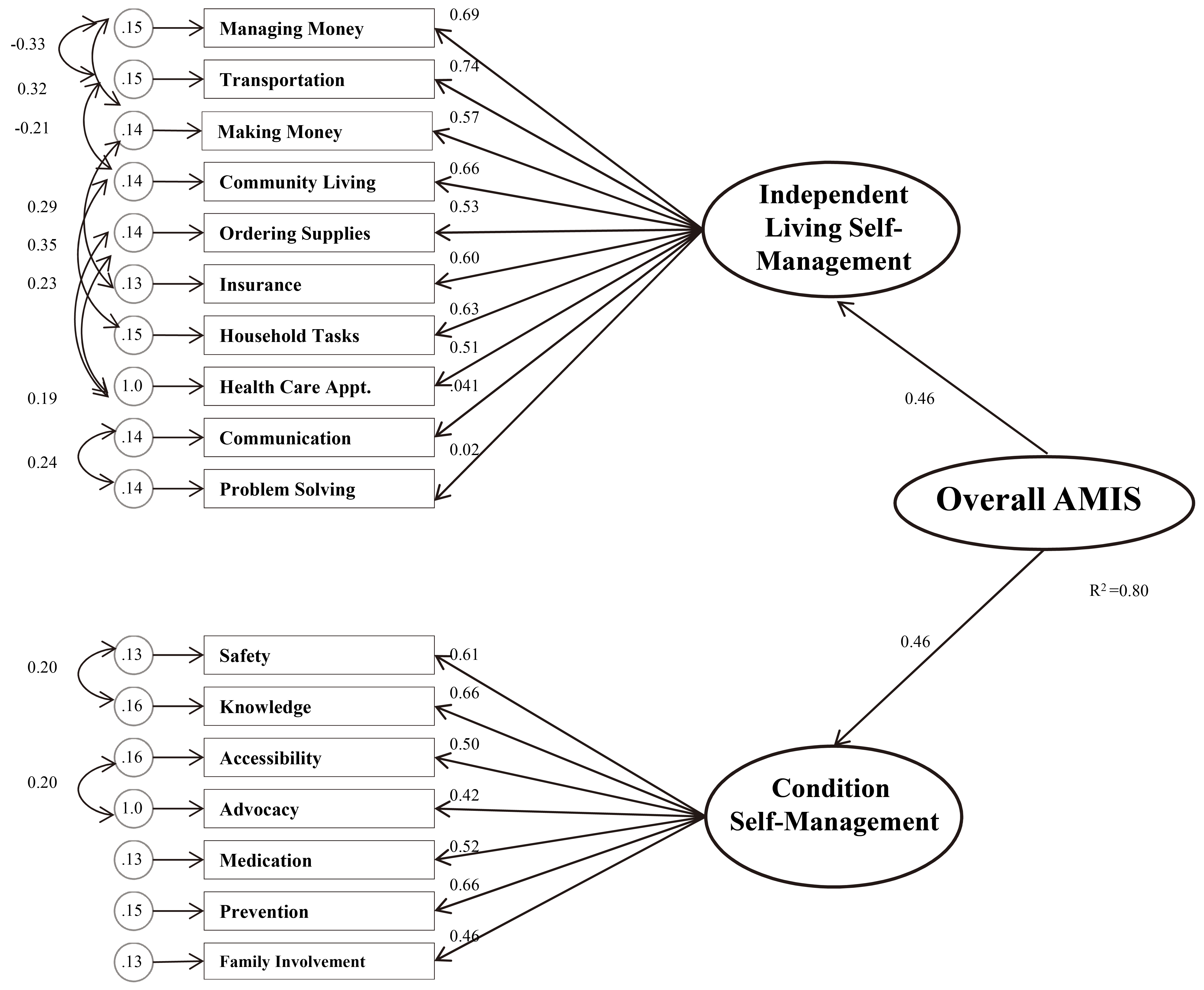
Characteristics of the sample are detailed in Table 2. The sample represents a full range of AYA ages (12–25 years of age) and was primarily Caucasian. Fifty-five percent of the AYA were females, as were the clear majority of parents interviewed. Fifty-six percent of the parents had at least some college education and 75% of female parents and 88% of male parents were employed. Just over 70% of the AYA had a shunt and 25% had thoracic, 50% lumbar, and 25% sacral lesions. All of the participants in the feasibility and adaptation samples had myelomeningocele (the most severe form of SB), while 85% of those in the transition study did. This sample is generally similar to the national data for a large number of individuals with SB. In the National Spina Bifida Patient Registry 51% were female and 79% had a shunt. In comparison to the national data, more participants in the total sample for this psychometric study had a thoracic lesion (25 vs. 18%), fewer had a lumbar lesion (45 vs. 61%), and more had a sacral lesion (28 vs. 20%) [35].
The KMO (0.834), Bartlett (679.32
The exploratory factor structure and the two factor correlations suggested that
a second order factor representing a total AYA self-management scale could potentially be
supported. Thus, the CFA was conducted with the two factors identified in the exploratory
factor analysis and a second order factor of overall self-management. Coefficients for the
direct paths indicated all items loaded onto the proposed factors with values from 0.41 to
0.74 (see Fig. 1). Several errors
were correlated. Results of the analysis supported the fit of the model. Model fit is
supported if the Chi Square (
Reliability analyses for parent and adolescent data yielded Cronbach alphas of 0.87 to 0.89 for the total scale, 0.86–0.88 for Factor 1 (Independent Living Self-Management), and 0.72–0.80 for Factor 2 (Condition Self-Management) (see Table 3). Frequencies (see Table 3) for the two subscales, from parent and AYA report, indicated that the AYA performed condition self-management behaviors at a higher level than independent living self-management behaviors. The stability of the instrument at 2-weeks was strong. ICC for parent total scale was 0.82, 95% CI (0.69, 0.91) and for the AYA total scale was 0.84, 95% CI (0.71, 0.92), which is between very good to excellent [34].
Frequencies and internal reliabilities for AMIS II overall scale and subscales
Frequencies and internal reliabilities for AMIS II overall scale and subscales
SM
Significant pearson correlations between total AMIS II and concurrent validity measures
*
Furthermore, the concurrent validity of the instrument was supported by its
small to moderate significant relationships to proposed variables. Higher self-management
behaviors were correlated with less severe SB (sacral lesions), better self-care, higher
decision-making participation and maturity, participation in higher number of chores, and
higher adolescent responsibility for overall condition management (Table 4). In addition, in the combined feasibility and adaptation
samples, validity was supported by the relationship of age to self-management. AYA age had
low but significant correlations with Condition Self-Management (
Given the importance of outcomes in health care delivery systems, it is essential to define and measure self-management behaviors related to health and daily functioning. The major contribution of this expanded instrument is a relatively easy to use, theory-based, outcomes measure that addresses a major issue in health care: the self-management behaviors needed for the transition of youth with chronic conditions to adulthood and independent living. Even though a previous factor analysis of adolescent AMIS II scores with a smaller sample indicated the potential of 3 factors [36], the current SEM analysis provided evidence that the parent structure was a reasonable fit for the adolescent data and yielded two clinically useful factor subscales and a total scale. The AMIS II addresses a gap identified in a review calling for an expansion of health-related outcome measures by assessing key areas of functioning and including direct involvement of youth in the instrument development [3].
The ability to perform AMIS II behaviors without assistance increases as the adolescent matures, although age norms have not been developed for this measure. It is interesting to note that for both parent and AYA, the concurrent validity analysis indicated that the total AMIS II score has a larger significant relationship to decision-making and chores than level of the lesion. The highest correlation was with decision-making participation in everyday life. It appears that participation in decision-making activities (e.g., how late AYA stays up, rules about homework, neatness of AYA room, how much allowance the AYA gets, how AYA’s spend their own money, or clothes the AYA buys and chores done around the house) can facilitate later more advanced self-management behaviors. Autonomy and independent activities may be delayed several years in AYA with chronic conditions [1, 37]. Thus, decision-making interventions may facilitate typical adolescent developmental tasks such as identity and independence from parents and be important building blocks for self-management.
Although the AMIS II was developed as a generic instrument, it has been primarily evaluated in AYA with SB and their parents. Some items are particularly useful for those with a physical disability (e.g., being able to access buildings or settings with stairs). However, the majority of items are broad enough to capture a wide range of self-management behaviors. Thus, the AMIS II has potential use in assessing self-management and independence behavior outcomes for adolescents with chronic health conditions that do not include a physical disability component. It is possible, however that differing conditions may have varying age-specific norms for the behaviors delineated in the AMIS II.
Additional evidence of construct validity is the performance of the AMIS II in studies of transition age young adults with SB in the literature. In a longitudinal analysis of young adults with SB, Bellin et al. [27] found that increases in self-management scores over time were associated with decreases in depressive symptoms. Similarly, Dicianno et al. [38] found that high use of a Mobile Health system (iMHere) was associated with positive changes in both AMIS II subscales. The strong relationship of parent and AYA AMIS II scores further supports the validity of the instrument. While parent and AYA reports of psychosocial concepts such as QOL are not strongly correlated [39], the high relationship of the AMIS II parent and AYA reports might correspond to the concrete behaviors tapped by this instrument that may be frequently observed by parents. Finally, both the internal reliability and the test-retest reliability or stability were supported by the data. The stability of an outcome measure is the most important reliability criteria for its use in intervention research and clinical practice [40]. It is critical to be confident that if an instrument indicates a change in behavior, the change was real rather than caused by an unstable instrument. The stability of the AMIS II supports its use in both intervention research and clinical practice.
Three generic instruments, the Transition Readiness Assessment Questionnaire (TRAQ) [16], the STARx [17], and the UNC TRxANSITION Scale [18], as well as the condition-specific Kennedy Krieger Independence Scale-SB (KKIS-SB) [19] each share some domains of interest with the AMIS II.. For example, self-management is one domain of the 10 domain 32-item TRxANSITION instrument, which also includes scales that address diet, reproductive health, school/work, and looking for new health providers. The STARx Questionnaire measures overall transition readiness with three domains: (a) transition related knowledge-communication with medical provider, (b) disease knowledge, and (c) self-management. The 20-item five-domain TRAQ scale addresses specifics of Appointment Keeping; Tracking Health Issues; Managing Medications; Talking with Providers; and Managing Daily Activities but does not capture independent performance of several higher-level community living behaviors. While the last domain, Managing Daily Activities, has questions on topics such as helping to prepare meals, keeping one’s room clean, and using neighborhood stores, the measure does not address complex behaviors such as planning, shopping and preparing the total meal, managing finances, managing transportation, managing insurance, overcoming access barriers, and social interaction behaviors measured in the AMIS II. In addition, AMIS II condition management behaviors such as prevention management or self-advocacy are not addressed. However, the self-administered instrument does allow adolescents to document their lack of knowledge about a behavior and their interest in learning how to perform the behavior. Similarly, the condition-specific KKIS-SB instrument adds useful knowledge on behaviors limited by executive function limitations. The KKIS-SB and the AMIS II share concepts, although the level of activity measured is generally higher in the AMIS II. For example, the KKIS-SB measures medication with “takes medication on time” while the AMIS II requires “knows names, dosages, and why the medication is used. Takes medications in appropriate way at appropriate time.” Additionally, the KKIS-SB addresses appointments with “writes down any new/future appointments in a scheduling book or on a calendar” whereas the AMIS II measures “Takes responsibility for making health care appointments, understands medical problem/issues that require an appointment, initiates and follows through in activities needed to make appointment (e.g., makes the phone call or makes the appointment)”. The KKIS-SB measures basic self-management skills such as “Correctly completes all of the steps of catheterization in the right order” or “Remembers to look for pressure sores on his/her body” while the AMIS II addresses consistent performance of advanced self-management behaviors such as monitoring headaches, conducting weight shifts/skin checks, increasing fluids both generally and especially with UTI, and catheterizing at the appropriate times. The KKIS-SB was developed for youth with SB as young as 10 years of age. It may be a better measure for younger youth developing basic self-management skills (e.g., doing catheterizing correctly, knowing/doing the steps of a bowel program, or checking skin on all parts of the body). In contrast, the AMIS II includes more advanced skills that the older AYA needs to achieve in order to transition effectively to adulthood. In addition, the AMIS II adds important items described above (e.g., managing money, advocacy, and insurance) and quantifies incremental progress toward independent performance.
The literature would suggest that achieving each of the AMIS II items with minimal assistance or supervision is fundamental to a successful transition to young adulthood and independent living. Choice of an instrument used to measure self-management behaviors or self-management as a part of transition readiness will depend on the type of behaviors (basic self-management behaviors/components, or advanced self-management behaviors) that the clinician or researcher is addressing as well as the specifics of the condition and the age of the child or AYA. In some situations, using both a condition-specific and generic instrument may be useful to optimally capture specific age and condition appropriate self-management behaviors.
This study is limited by 1) the geographic location of participants (mostly located in Midwest and Eastern USA); 2) the predominance of Non-Hispanic white participants in our psychometric studies when 36% of those with SB nationally are either Hispanic (24%), Non-Hispanic black (6%) or other (6%) [35]; 3) the slightly lower number of participants with a shunt (72% in the adaptation sample vs. 79% in the national study [39]); 4) the exclusion of those with intellectual disabilities; 5) the use of participants with a single chronic condition, and 6) the limited clinical and demographic data on the transition sample. Individuals with intellectual disabilities were omitted as the surveys used for concurrent validity were not appropriate for this population. However, data from this study would indicate that the parent report may be used as a proxy for understanding self-management in individuals with intellectual disability. The exclusion of those with intellectual disabilities might have accounted for the slightly lower percentage of those with a shunt. Additional analysis of a more diverse sample is indicated. Furthermore, analysis of the reliability and validity of the AMIS II in AYA who have a wide range of chronic health conditions (e.g., arthritis, asthma, epilepsy, diabetes, and congenital cardiac conditions) is underway. In addition, a generic and SB specific self-report version have recently been developed and are currently being evaluated. In the transition sample, age and severity or level of SB lesion had similar relationships to the AMIS II as they did in the combined feasibility/adaptation samples. However, they were the only concurrent validity data available. Further investigation of factors related to AMIS II behaviors in ethnically diverse and transition age young adults may be helpful.
Conclusion
Psychometric analysis supports this expanded measure of self-management for AYA with a specific chronic health condition (SB), their families, and their health care providers. Because the AMIS II quantifies actual performance of the behaviors and specific incremental achievement of items, it offers promise for use in clinical-based translational research. Further testing with AYA who have other chronic health conditions and their families is indicated.
Footnotes
Acknowledgments
The primary study (Secondary Conditions and Adaptation in Spina Bifida) was supported by a grant (RT01 2-3-002) from the Association of University Centers on Disabilities (AUCD) in cooperative agreement with the Centers for Disease Control and Prevention (CDC)’s National Center on Birth Defects and Developmental Disabilities (NCBDDD). Additionally, funding for the development of the AMIS II was provided to Dr. Sawin by the Alpha Chapter, Sigma Theta Tau, Indianapolis, Indiana. The authors would like to thank Dr. Melissa Bellin for the psychometric data from the multi-site transition study she and her colleagues carried out and Drs. Connie Buran and Thomas Webb for their contribution to the development of the instrument. In addition, the authors thank the families for their participation.
Conflict of interest
The authors have no conflicts of interest to report.