
Abstract
Background:
Limited emergency contraception (EC) use contributes to unintended pregnancies and health risks among adolescents and young adults in conflict-affected regions. In Northern Uganda’s post-conflict setting, there is a need for research on EC utilization among adolescents and young adults.
Objective:
We assessed emergency contraceptive utilization and associated factors among adolescents and young adults in Gulu East Division, Northern Uganda, following 25 years of post-conflict recovery.
Methods:
A community-based cross-sectional study was conducted among 400 adolescents and young adults in Gulu East Division using self-administered questionnaires. Data analysis involved descriptive statistics and logistic regression using STATA (StataCorp LLC) to identify factors associated with EC utilization.
Results:
Among 400 participants, 322 (80.5%) were aware of EC, but only 173 (43.3%) utilized it. Correlation analysis revealed negative correlations between age and employment status and living arrangement, and a positive correlation between education level and marital status. Multivariate analysis showed that EC utilization was significantly associated with age, education level, employment status, living arrangement, and EC service offer. Women aged 14–19 years and those not offered EC services were less likely to use EC (adjusted odds ratio (aOR) = 0.47), while women with secondary education (aOR = 3.05), employed women (aOR = 2.76), and those living alone (aOR = 9.76) were more likely to use EC.
Conclusion:
There is a gap between awareness and utilization of EC among adolescents and young adults in Gulu East Division. Targeted interventions are needed for adolescents and those with limited access to EC services to increase utilization and prevent unintended pregnancies.
Plain language summary
Emergency contraceptive utilization is an essential component in addressing the global public health issue of unintended pregnancies, especially in developing countries. For adolescents 14-19 and young adults aged 20-24, the risk of unintended pregnancy is particularly concerning due to its potential to lead to adverse outcomes such as reliance on abortion and related health consequences.
Adolescents and young adults were surveyed using an interview-based questionnaire to assess their exposure to and utilization of emergency contraceptives, as well as the factors associated with their use.
A total of 424 respondents were interviewed with a response rate of 94.3%. Results showed that most of the participants (80.5%) were aware of EC, but only 43.3% had used it, with pills being the most common method. Factors that were linked to higher EC use included age 20-24, being employed, having a history of abortion, and access to adolescent-friendly services at health facilities.
The findings highlight the need to improve EC awareness and access to prevent unintended pregnancies and reduce abortion complications in Northern Uganda.
Background
Emergency contraception (EC) is a method that can be utilized to prevent pregnancy following unprotected sexual intercourse. It provides a crucial opportunity to avoid unintended pregnancy when a regular contraceptive method fails, when no contraception is used, or in cases of coerced sex. 1 EC and unintended pregnancy are critical public health concerns, impacting women’s autonomy, reproductive rights, and family planning. Many developed countries effectively regulate EC access through robust information campaigns and supply systems, guided by international recommendations. 2
Globally, approximately 210 million pregnancies occur each year, with around 38% being unintended, and about 22% ending in abortion. 3 Emergency contraceptive pills are among the 13 essentials, underutilized, yet highly effective and affordable commodities that can significantly improve the health and survival of millions of women and children globally. 4 The burden of unintended pregnancy in sub-Saharan Africa is alarming, with more than 30% of cases ending in termination. 5 Due to restrictive laws, most women (about 77%) resort to unsafe abortions, often performed by untrained individuals or using unapproved methods, resulting in severe complications, hospitalizations, disabilities, and deaths. 6
Sub-Saharan Africa accounts for an estimated 6.2 million unsafe abortions annually, with 1.6 million women treated for related complications. The region also bears the highest burden of abortion-related deaths, with half of these deaths occurring among young people. 7 Similarly, an estimated 21 million adolescents become pregnant annually, with around 50% of these pregnancies being unintended, and approximately 55% ending in abortion, often under unsafe conditions. 8 The situation is particularly dire in conflict zones, where the collapse of healthcare systems puts women and girls at risk, leading to high rates of unplanned pregnancies, unsafe abortions, and maternal deaths, with displaced women facing significant barriers to accessing essential reproductive health services. 9
In Uganda, the situation is alarming, with unintended pregnancy rates nearly 3 times the global average, and about 145 unintended pregnancies per 1000 women aged 15 to 49. 10 The civil war that ravaged northern Uganda from 1986 to 2006 had a devastating impact on the region’s health, resulting in the worst health indicators in the country, marked by high rates of abortion and unplanned pregnancy. 11 The prolonged civil war severely hindered the delivery of health services, including family planning, in the region, while also limiting access to education and attainment of sexual and reproductive health rights due to displacement and encampment. 12 This high burden of unintended pregnancy and resultant induced abortion can be reduced by using modern contraception, including EC, which in turn can virtually eliminate harm and fatalities from unsafe abortions since most abortion-related pregnancies are unwanted. 13
Adolescent girls in Africa face significant obstacles and stigma in accessing contraception, contributing to high rates of unintended pregnancies and abortions due to low contraceptive use. 14 Policies supporting adolescents’ access to safe, affordable, and quality contraception, including clear guidelines on EC, can promote their rights, reduce poverty and drive sustainable development by enabling healthcare providers to recommend it to those in need. 15
Low- and middle-income countries Uganda inclusive continue to struggle with unmet family planning needs, even with existing family planning services. 16 The public health system in Uganda faces significant challenges, including limited and irregular availability of contraceptives, while the private sector has fewer stock-outs but high out-of-pocket costs. 17 Emergency contraceptive methods are often recommended for individuals aged 18 and older, and concerns about providing emergency contraceptive pills include misconceptions linking them to abortion and fears regarding potential side effects. 18
Despite efforts to promote better access to EC, unintended and unwanted pregnancies remain a significant risk to the health of adolescents and young women, particularly in regions with limited access to healthcare services. 19
There is limited information on the factors associated with emergency contraceptive (EC) use among adolescent and young adults in Gulu East Division, Northern Uganda, as noticed by high rates of school drop outs due to unplanned pregnancies and related complications. A lot of studies have been conducted on modern contraceptive prevalence in Uganda. However, the broader aspects of understanding the factors associated with utilization of EC, particularly in post-conflict region like Northern Uganda, remained underexplored. This highlights the need for improved scientific evidence to guide policies and programs aimed at enhancing the health of adolescents and young women. Therefore, this cross-sectional study aimed at assessing factors influencing the Utilization of Emergency Contraceptives among Adolescents and Young adults in Gulu City, Northern Uganda.
Methods
Study design and settings
A cross-sectional study was conducted from February to April 2023 involving 400 adolescents and young adults in Gulu East Division, Gulu City, Northern Uganda. Gulu City, a newly established City, is the commercial and administrative Centre in Acholi Sub-region divided into two divisions (Gulu East and Gulu West). The city is 333 km from Kampala (the capital of Uganda), with a population of about 216,248, with approximately 34% being adolescents and young adults. Gulu East includes Laroo (32,300 people) and Pece (53,500 people), covering 10.26 and 11.72 km2, respectively. Regarding gender distribution, the overall female population are 16,500 in Laroo and 28,100 in Pece, giving a total population of about 44,600 females in Gulu East. The city comprises 16 parishes and 99 villages, with 8 and 56 villages in Gulu East. This study focused on participants from Gulu East, an urban area that experienced a prolonged civil war from 1986 to 2006.
Inclusion/exclusion criteria
The study included adolescents aged 14–19 and young adults aged 20–24 residing in Gulu East Division, with written informed assent/consent obtained from all participants. For those under 18, both written assent and parental consent were required. Exclusions included individuals with severe physical or chronic health conditions that could affect contraceptive options of study participation, as well as those who did not provide the necessary consent or assent.
Sample size
The sample size was calculated using the Kish Leslie formula at a 95% confidence interval and a 5% significance level, assuming a prevalence of 0.5. After accounting for a 10% non-response rate, the final sample size was 424 participants. However, only 400 participants were analyzed, with 24 (5.7%) excluded due to incomplete data or non-response.
Sampling procedure
Study participants were recruited into the study from their homes of residence. Administratively, the Gulu East division has 19 administrative parishes and 78 administrative villages distributed across the parishes, with an average of 4 villages per parish. A two-phase simple random sampling was performed, first to select 4 parishes from the 19, and secondly to select 2 villages from each of the 4 parishes selected in the first step, totaling to 8 villages overall. The random number generation for the simple random sampling was performed using the R software (version 4.3.0). From the eight villages, purposive sampling was undertaken to select eligible participants within the age bracket of interest (14–24 years). In cases with more than two eligible adolescents and young adults in a home, one was recruited in the study. Informed consent was obtained from study participants above 18 years, whereas those less than 18 years, parental/guardian consent was sought.
Data collection
Data were collected using structured questionnaires pretested on 25 respondents from Gulu West Division (Supplemental Appendix 1). Two research assistants were trained and taken through the study procedure by the principal investigator (FL). The questionnaire included the independent variables such as: sociodemographic characteristics, and awareness and health system factors, while, dependent variables included utilization of emergency contraceptives.
Data quality control and safety
The questionnaires were checked for completeness and consistency of the information obtained by the principal investigator at the end of each day. The hard copies of the questionnaires were stored in a lockable cabin, and the soft copies of the information were entered into a password-protected computer.
Statistical analyses
Data were analyzed using STATA version 17.0 (StataCorp LLC). Categorical data were presented as frequencies and percentages. Bivariate analysis assessed associations between variables, while logistic regression identified factors independently associated with past EC use. Both unadjusted and adjusted odds ratios (ORs) with 95% confidence intervals (CIs) were calculated, and statistical significance was set at 0.05.
Results
Sociodemographic characteristics
Table 1 presents the sociodemographic characteristics of the participants. More than half of the participants, 53.5% (n = 214), are aged 14–19 with most of them having completed primary and secondary education. A significant proportion (68%) of the participants were not employed, and the more than half (58%) lived with their parents. Additionally, 71.8% of the participants reported having a boyfriend or lover, and 66.2% had ever had sex, with a median age of first sexual activity at 17 years. In the subset of participants using EC (n = 266), the distribution across all demographic characteristics was similar to that in the entire dataset.
Sociodemographic characteristics of the participants (n = 400).
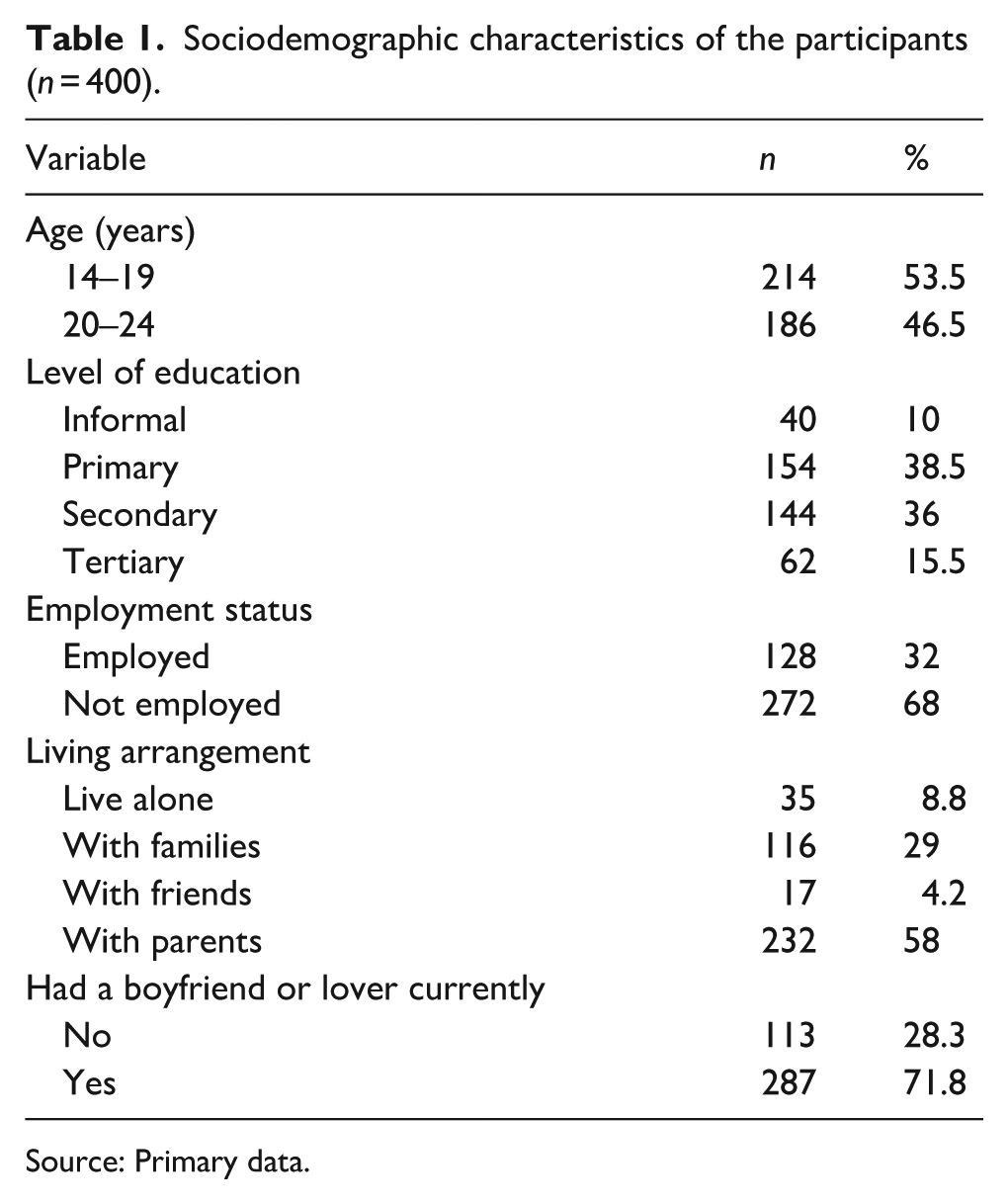
Source: Primary data.
Awareness of emergency contraception
The majority (80.5%) of the participants reported having heard of EC, but only 31.5% correctly believed it is accessible without a prescription, and 42.7% knew the optimal timing for its use. Furthermore, just 9.2% of the participants received EC training in the last 3 months, indicating limited recent education on EC as shown in Table 2.
Awareness of emergency contraception among adolescents and young adults (n = 400).
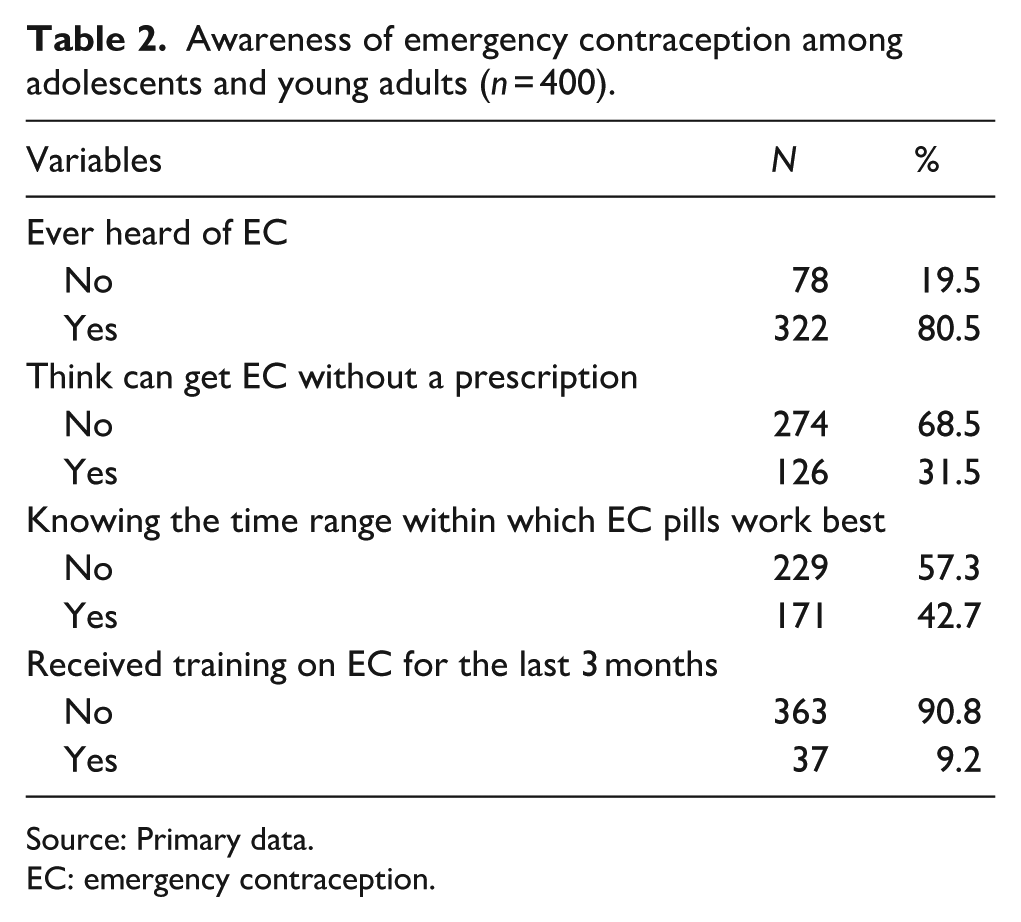
Source: Primary data.
EC: emergency contraception.
History of un-intended pregnancy
Among the 400 participants, 99 (24.8%) reported having had unintended pregnancy. Of these, 77.7% had it once, 17% had twice, and smaller proportions had three or four times. The primary cause of unintended pregnancies reported included non-use of contraception (80.6%), followed by contraceptive failure (7.1%), forced sex (5.1%), and other reasons (7.1%), such as having sex to show love, as shown in Table 3.
History of unintended pregnancy.
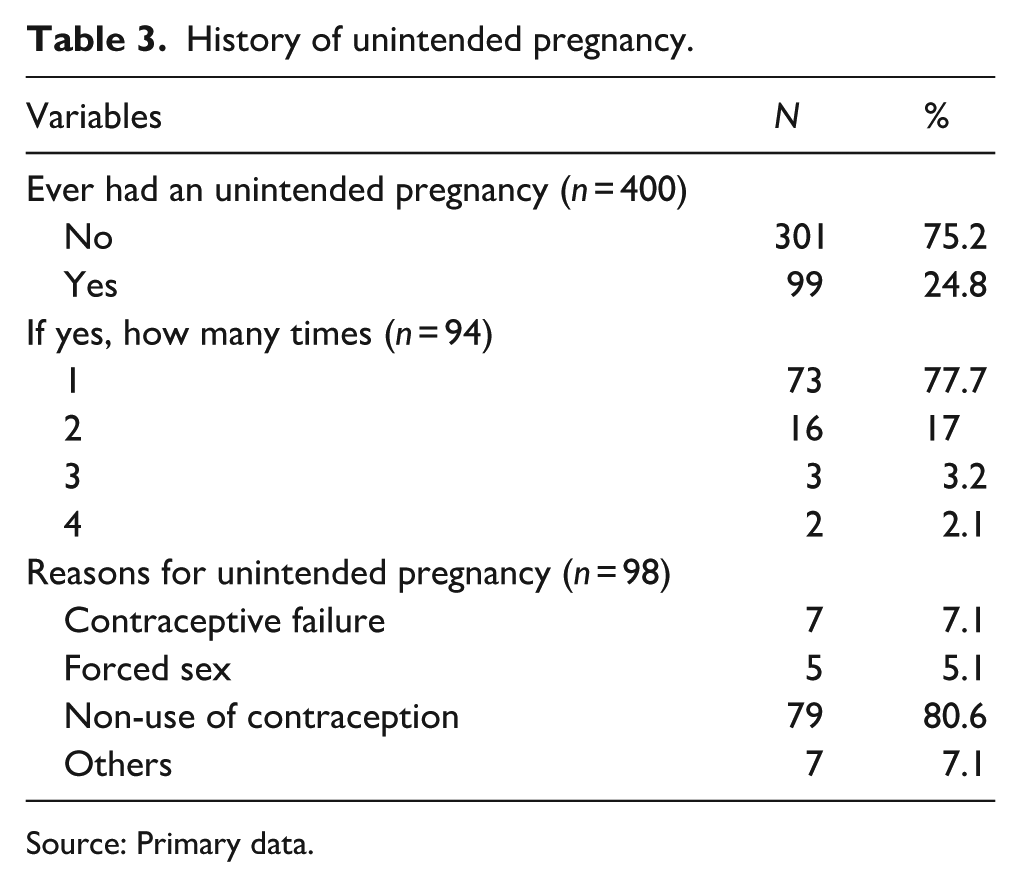
Source: Primary data.
Abortion and complications
Table 4 provides a clear picture of participants’ experiences with abortion and its complications. Out of the 400 participants, 58 (14.5%) reported having had an abortion, while the majority, 342 (85.5%), had not. Among the 58 women who had an abortion, 45 (77.6%) experienced complications, while only 13 (22.4%) did not.
Abortion and complication.
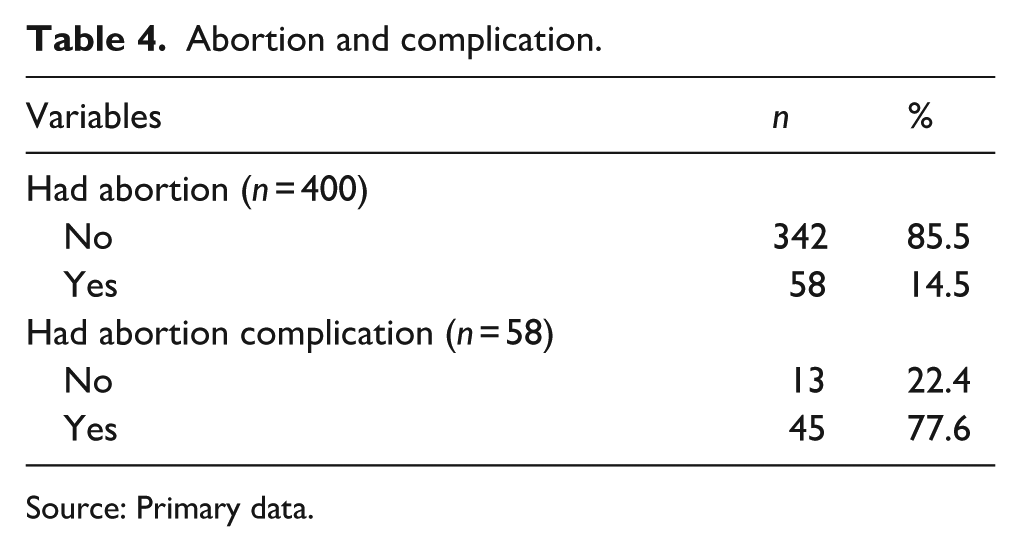
Source: Primary data.
Health system factor
The availability of EC reveals gaps in adolescent-centered services specifically, an ‘adolescent corner’ which refers to a dedicated space or area within a health facility designed to provide confidential, youth-friendly, and tailored reproductive health services for adolescents. However, 73.8% of health facilities lacked such a designated space, as reported by participants, and 77.8% did not offer EC. This limited access may hinder adolescents’ ability to obtain essential reproductive health services as shown in Table 5.
Health system factor (n = 400).
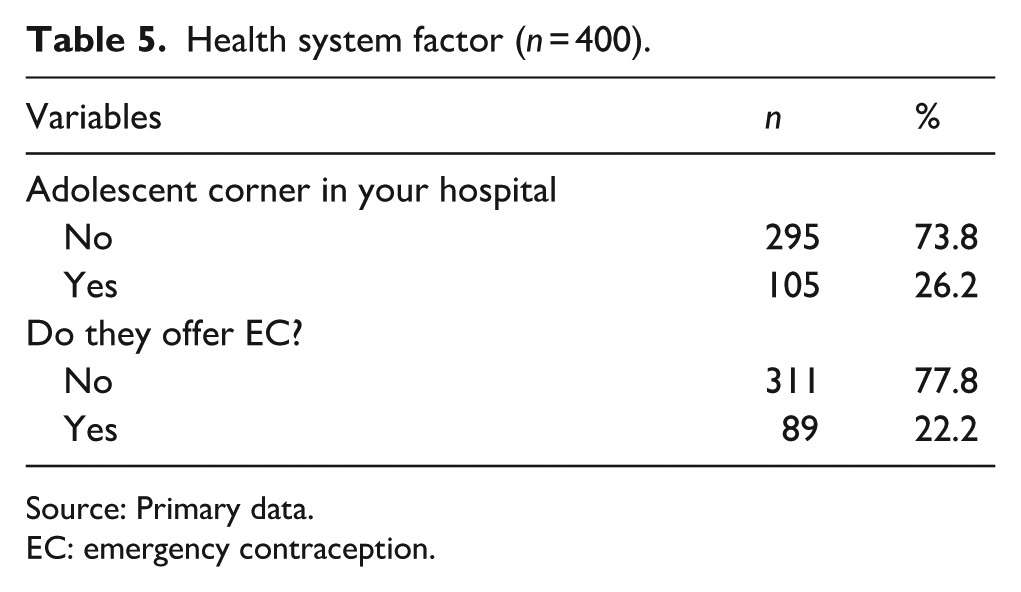
Source: Primary data.
EC: emergency contraception.
Utilization of emergency contraceptive
Among 400 participants, 43.3% (173) had used EC, and among the users (173) 92.4% opting for EC pills. Slightly the majority, 56.7% of the participant had not used EC. This group cited various reasons for non-use, primarily abstaining from sex (37.9%, with 105 participants reporting no need for EC) and lack of awareness (35.4%, with 98 participants having never heard of EC). Additional barriers included financial constraints (10.1%) and disapproval from their boyfriend (7.2%), as shown in Table 6.
Utilization of emergency contraception (n = 400).
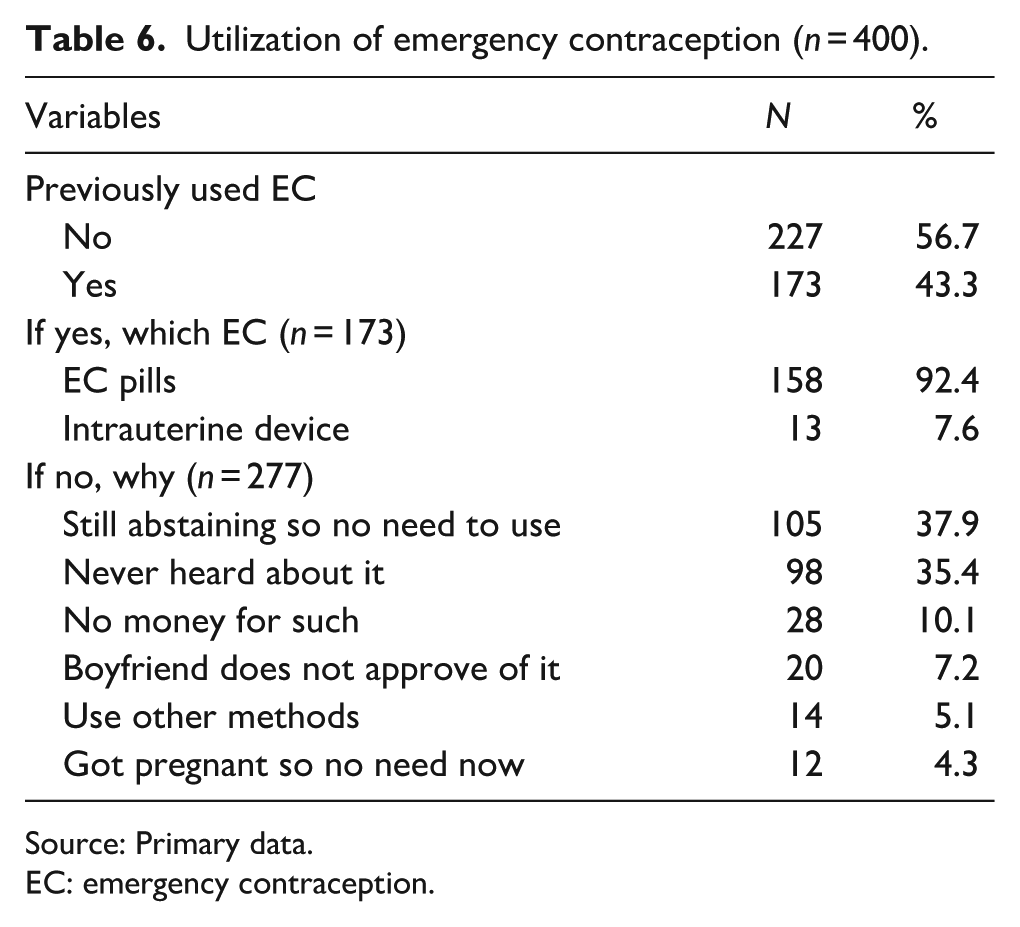
Source: Primary data.
EC: emergency contraception.
Contraceptive methods and types used
The assessment of contraception method use reveals that 63.8% of respondents (255 out of 400) are not using any family planning methods, while 36.2% (145 participants) are using family planning. Among users, condoms are the most preferred method (41.4%), followed by injectables (31%), with less frequent use of other methods like Intra-Uterine Devices (IUDs), natural methods, and pills.
Factors associated with previous utilization of EC
The bivariate analysis in Table 7 reveals several factors with significant positive associations with EC utilization among adolescents and young adults. Respondents with secondary education were more likely to use EC compared to those with tertiary education (OR = 2.40; 95% CI: 1.51–3.83; p < 0.001). Being employed was strongly associated with higher EC use (OR = 3.57; 95% CI: 2.25–5.66; p < 0.001). Living alone (OR = 15.00; 95% CI: 3.59–62.77; p < 0.001) and living with friends (OR = 6.50; 95% CI: 1.47–28.80; p = 0.014) were both positively associated with EC use compared to living with parents. Having a boyfriend was also associated with increased EC use (OR = 3.00; 95% CI: 1.09–8.25; p = 0.033). Additionally, participants who had not experienced unintended pregnancy (OR = 1.67; 95% CI: 1.22–2.28; p = 0.001) or abortion (OR = 1.51; 95% CI: 1.14–1.99; p = 0.004) were more likely to have used EC. Surprisingly, those who had not heard of EC corners (OR = 1.44; 95% CI: 1.07–1.93; p = 0.015) and those not offered EC by a provider (OR = 1.41; 95% CI: 1.05–1.90; p = 0.022) also had higher odds of EC utilization, suggesting self-initiated access.
Bivariate analysis for factors associated with utilization of previous EC.
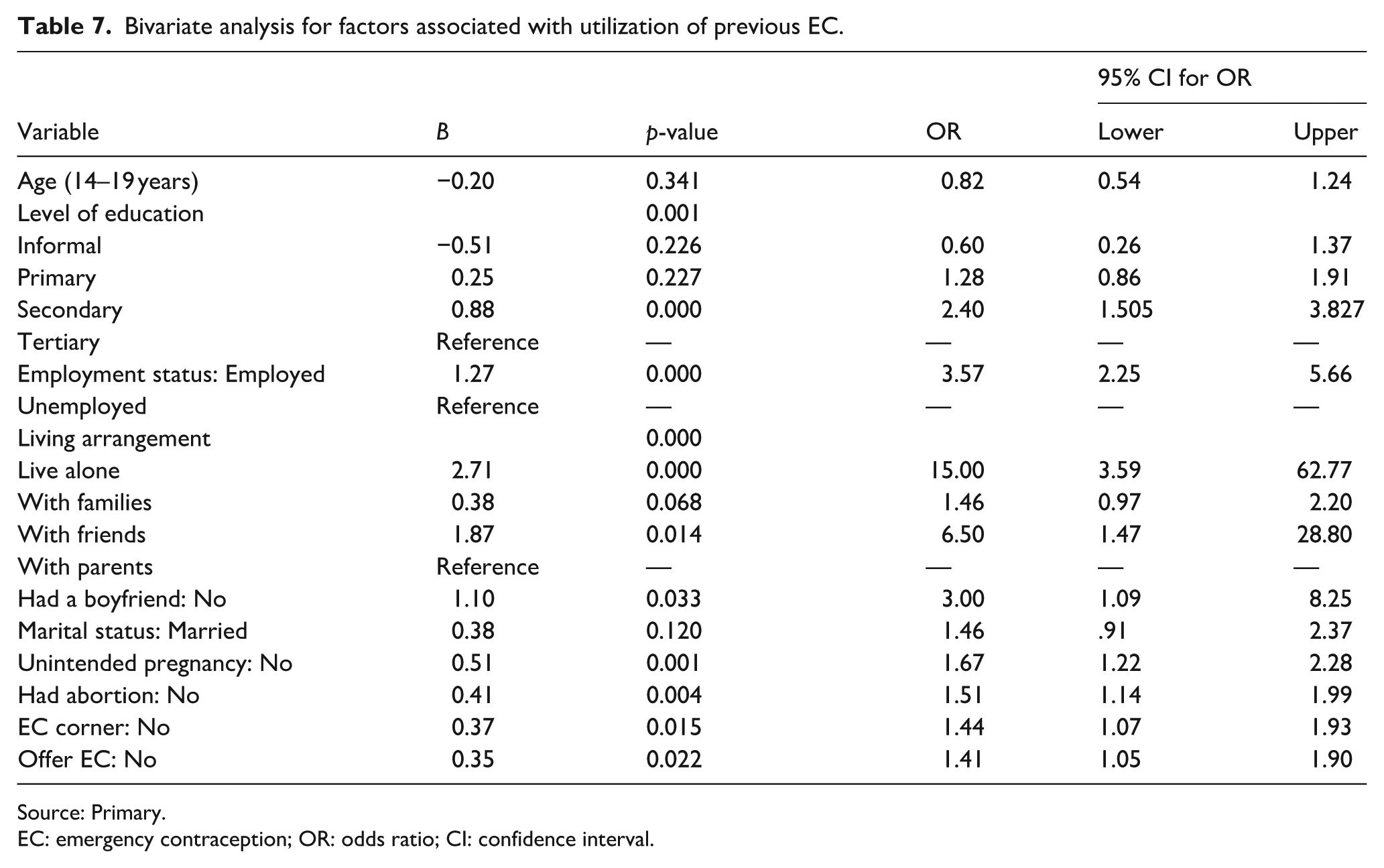
Source: Primary.
EC: emergency contraception; OR: odds ratio; CI: confidence interval.
Discussion
This study examined emergency contraceptive utilization and associated factors among adolescents and young adults. Findings revealed a significant disparity between awareness and actual utilization of this contraceptive method. This may probably be due to limited access, misconceptions, stigma, fear of side effects, lack of education, and cultural or religious beliefs, among other factors.
The study findings showed that EC use among the study participants was at 43.3%. This is slightly higher than studies reported in Ethiopia at 33.3% among the female college students. 20 The finding is also higher than 26.7% at Adama University, Nigeria Ethiopia, and Ghana.21–25 However, the findings were slightly lower than studies conducted among female students in South West Ethiopia reported at 46.3%. 26 The differences are based on the study participants, geographic locations as well as the study design and methods used. The implication to low utilization of ECs indicates a gap in family planning services, potentially leading to unintended pregnancies and abortions. Unintended pregnancies can have negative consequences for women’s health, education, and economic empowerment, and also impact maternal and child health and the economy.
Among EC users, EC pills were the predominant method used, which is consistent with previous studies in Ethiopia and similar with other studies conducted elsewhere showing EC pills were the most commonly used method.20,23,27,28 This suggests that EC pills are a widely accepted and accessible form of EC in this population. However, in contrast, a systemic review involving a search of several database showed that IUDs are a highly effective method of EC after unprotected sex, offering a safe, reliable, and cost-effective solution for most women, with the added benefit of providing long-term contraception when left in place. 29 This difference may be attributed to variations in access to different EC methods and healthcare provider training.
Regarding the non-use of EC, our study revealed several key findings including abstinences, lack of awareness, financial constraints, partner disapproval, using other methods and already pregnancy and no need. These findings are consistent with previous research,28,30–32 which shows that many different factors affect whether people use EC. The fact that lack of awareness and financial constraints were big problems highlights the need for better education and more affordable EC options. Partner disapproval was also an issue, suggesting that involving partners in reproductive health discussions could be helpful.
While in bivariate analysis, the factors independently associated with EC utilization were age, education level, employment status, living arrangement, and being offered EC. Younger adolescents (14–19 years) were less likely to utilize EC compared to young adults (20–24 years), which is consistent with previous studies. However, in contrast to the above findings, a study conducted in Ethiopia showed that females aged 20 or less were more likely to utilize EC compared to those older than 20 years. 23 The less utilization could be due to lack of awareness, social and cultural barriers, fear of stigma and judgment, and limited financial independence. Women with secondary education were more likely to utilize EC, supporting previous research.33–35 This could probably indicate that higher education increases EC awareness, use, and empowering students on decision-making. Employed women were also more likely to use EC, as noted with previous studies that have reported higher EC utilization rates among employed women.36,37 Similarly, being in school and receiving monthly allowances was associated with EC utilization as supported by other studies.36,38 These suggest that financial independence may facilitate access to healthcare and EC utilization. Furthermore, the study found that living arrangements were associated with utilization of EC which is supported by other literatures.39,40 This suggests that living alone provides greater autonomy and reduced external influences. Lastly, women not offered EC were less likely to use it, and this is consistent with other studies.19,41–43 This suggests that prior information and awareness campaigns may contribute to the offer of EC, emphasizing the importance of education and awareness efforts.
A multivariable model was not developed from the available factors (age, education level, employment status, living arrangements, and offer of EC) due to significant correlations identified among several variables. Correlation analysis revealed notable relationships between demographic characteristics and EC utilization. For instance, a positive correlation was observed between age and education level; education level was also positively correlated with marital status. Additionally, both employment status and marital status were correlated with living arrangement. These interrelationships indicated a high degree of collinearity among the variables. Only two pairs – marital status with employment status, and living arrangement with employment status – showed relatively low correlations (i.e. correlation coefficients below 0.3). However, in joint evaluation of these minimally correlated variable pairs, statistical significance was not achieved for both variables within any given pair. As a result, and to avoid the risk of multicollinearity affecting the validity of the findings, the study retained univariate analysis as the final approach for evaluating the factors associated with EC utilization.
Strengths and limitations
The study’s strengths lie in its well-designed sampling method and rigorous data quality control, which enhance the representativeness and reliability of the findings. However, it is limited by its cross-sectional design, potential biases in purposive sampling, limited generalizability, and reliance on self-reported data, which may introduce social desirability bias. Despite these limitations, the study offers valuable insights into EC utilization among adolescents and young adults.
Conclusion
EC utilization among adolescents and young adults was found to be relatively low. Although several factors were associated with EC use, high correlations among them limited multivariable analysis, so univariate results were retained. Strengthening education, raising awareness, and improving access to EC are key strategies to enhance utilization and support better reproductive health outcomes for young people.
Recommendations
We recommend enhancing awareness and education on EC, particularly among sexually active adolescents aged 14–19 and those with limited education. EC services should be made more accessible and affordable, especially in facilities lacking adolescent-friendly care. Further research is needed to identify additional factors influencing EC use and to inform strategies for improving uptake.
Supplemental Material
sj-docx-1-whe-10.1177_17455057251374498 – Supplemental material for Emergency contraceptive utilization and associated factors among adolescents and young adults in Gulu East Division, Northern Uganda
Supplemental material, sj-docx-1-whe-10.1177_17455057251374498 for Emergency contraceptive utilization and associated factors among adolescents and young adults in Gulu East Division, Northern Uganda by Florence Laker, Jerom Okot, Francis Williams Ojara, Franceska Akello, Derick Amone, Pebalo Francis Pebolo, Silvia Awor, Pamela Atim and Felix Bongomin in Women's Health
Supplemental Material
sj-docx-2-whe-10.1177_17455057251374498 – Supplemental material for Emergency contraceptive utilization and associated factors among adolescents and young adults in Gulu East Division, Northern Uganda
Supplemental material, sj-docx-2-whe-10.1177_17455057251374498 for Emergency contraceptive utilization and associated factors among adolescents and young adults in Gulu East Division, Northern Uganda by Florence Laker, Jerom Okot, Francis Williams Ojara, Franceska Akello, Derick Amone, Pebalo Francis Pebolo, Silvia Awor, Pamela Atim and Felix Bongomin in Women's Health
Footnotes
Acknowledgements
We would like to acknowledge the study participants and express our gratitude to the Dean and Deputy Dean of the Faculty of Medicine at Gulu University for their support. We also thank the Pre-Publication Support Service (PREPSS) for assisting in the manuscript preparation through author training, pre-publication peer review, and copy editing. Additionally, we extend our appreciation to the local leadership in Gulu City and the community members who willingly participated and contributed to the success of this research.
Ethical considerations
The study protocol was approved by the Gulu University Research Ethics Committee (GUREC-2022-433). All ethical guidelines outlined in the Declaration of Helsinki were observed.
Consent to participate
Assent was obtained from adolescents who were less than 18 years of age.
Consent for publication
Not applicable.
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Center for International Reproductive Health Training at the University of Michigan (CIRHT-UM). The funder had no involvement in the study design, data collection, analysis, interpretation or manuscript preparation.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data and materials used in this study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.