
Abstract
PURPOSE:
The purpose of this longitudinal study was to evaluate the internal consistency reliability and construct validity of the Adolescent/Young Adult Self-Management and Independence Scale-II (AMIS-II), an interview-based measure of self-management for youth with chronic health conditions.
METHODS:
A diverse sample of adolescents and young adults (AYA) with spina bifida (SB) (n = 64 AYA; mean 20.88; age range 18–25 years) completed an AMIS-II interview. Six years earlier, parents from 55 families completed questionnaires that assessed children’s responsibility for SB-related care (Sharing of Spina Bifida Management Responsibilities) and their ability to perform skills across condition-related tasks (The Spina Bifida Independence Survey). Parents also reported on child’s communication skills, adaptive behaviors, and independent management of finances (Adaptive Behavior Assessment System-Second Edition; Scales of Independent Behavior-Revised). Descriptive and correlational analyses were conducted to assess the construct validity and the internal consistency reliability of the AMIS-II.
RESULTS:
The AMIS-II demonstrated excellent internal consistency reliability (AMIS-II total scale α= 0.95; subscales α= 0.90 –0.91). Evidence in support of construct validity was found in associations between the AMIS-II and measures of child responsibility for SB-related care, ability to perform condition-related skills, and adaptive behaviors (r’s = 0.378 –0.777; p’s < 0.05).
CONCLUSION:
This study provides further evidence of strong reliability and validity for the AMIS-II. Additional research with this measure will facilitate a better understanding of factors related to self-management behaviors in adolescents and young adults with spina bifida.
Background
Spina bifida (SB) results from a failed closure of the neural tube during the early stages of pregnancy and is the most common congenital chronic health condition involving the central nervous system [1, 2]. This condition requires a complex daily medical regimen to manage a wide range of physical disabilities, orthopedic conditions, and bowel and bladder continence. Successful self-management of SB and its sequelae is critical, as individuals with this condition are at high risk for early mortality due to preventable complications [3]. Self-management for bladder care requires management techniques such as regular clean intermittent catheterization and medications [4]. Bowel management involves strategies such as oral medication, suppositories and enemas, digital stimulation, and colostomies. The daily regimen of care for SB requires that individuals continuously practice preventive health behaviors, such as: (a) making and attending regular appointments with health care providers; (b) monitoring for headaches, when shunted for hydrocephalus; (c) skin checks; and (d) exercise. Further, responsibility for self-management behaviors is influenced by cognitive status (e.g., IQ, executive function) [5–7] and child depression [8]. While the care needs of individuals with SB vary greatly as a function of symptom profiles and co-morbidities, self-management is always an important goal.
Adolescents and young adults (AYAs) with SB have a great deal to manage and are often lagging behind in milestone achievement relative to their typically developing peers by 2–5 years [9–11]. Such early delays translate to later delays in achievements of adult milestones and challenges with the transition to adult healthcare. For example, young adults with SB face barriers to finding accessible employment that matches their abilities and securing accessible and reliable transportation [12]. Young adults with SB are less likely at age 18–23 to achieve independent living, attend college, or obtain full-time employment than their peers [13, 14]. Understanding how young adults with SB take on skills of independent living (e.g., transportation, managing money, and household skills) is critical because such skills are necessary for a successful transition to adult healthcare and effective self-management of their condition [12, 15].
To measure independent living skills and self-management in AYAs with SB, the Adolescent/Young Adult Self-Management and Independence Scale (AMIS) was developed [16] and further revised into the AMIS-II (17 items) [17]. AMIS-II, a structured interview, was designed to assess the level of assistance required by an AYA with a chronic illness (e.g., spina bifida) to transition towards independent living in a manner that is developmentally appropriate [17]. The expanded AMIS-II, validated in a sample of 202 AYAs with SB and 129 of their parents [17], yields two subscale scores (condition self-management and independent living self-management) and an overall scale score.
Unfortunately, the majority of research on the AMIS-II has primarily been descriptive, cross-sectional, and mostly conducted with Caucasian participants. Reliability and validity in a diverse sample have not been established. SB is a condition with a high prevalence in individuals of Hispanic/Latino background (3.80 per 10,000 live births in US) [18, 19], so the lack of inclusion of diverse samples has hindered the evaluation of the generalizability of this measure. It is important to continue to evaluate this measure, particularly with more diverse samples.
There is limited and conflicting evidence regarding demographic and condition-related factors that contribute to health outcomes and self-management in SB. While there is evidence for the association between older age and better self-management [17], older age has also been associated with decreases in ambulatory status/mobility [20], higher levels of obesity [21, 22] and the presence of pressure injuries [23, 24]. This may indicate decreased personal performance of expected SB-related care such as physical activity, healthy eating patterns, and skin checks. Although females and those with higher lesion levels reported lower rates of intermittent catheterization [25], females in a national sample were more likely to demonstrate bowel and bladder continence [23], perhaps due to more parental involvement for this subpopulation. Finally, Hispanics/Latinos, when compared to non-Hispanics/Latinos, reported higher rates of bladder accidents and parents were less satisfied with both the bladder and bowel programs [26].
Self-management is defined as “an active daily and flexible process in which youth and their parents share responsibility and decision making for achieving control of their condition, health, and well-being through a wide range of activities and skills. The goal of this increasing responsibility is to develop skills needed for transition to adulthood and independent living” [27 p. 34, 28]. The evaluation of construct validity of the AMIS-II as a measure of self-management is limited thus far to two studies which found support for associations between the AMIS-II and age, lesion level, decision making, completion of chores, AYA responsibility for care, and self-care [16, 17]. Use of the AMIS-II in future clinical practice and research would, therefore, benefit from evidence of associations with additional measures of condition-related activities and independence skills needed for the transition to adulthood and independent living. Indeed, such additional evidence would strengthen the psychometric evidence for this measure, promoting its use in assessing and intervening on targets for a successful transition to adult healthcare and self-management in SB.
As evidence of construct validity, longitudinal data can provide information across developmental periods to identify early skills and behaviors that are expected to relate to the development of self-management, as assessed with the AMIS-II. This study uses a different and novel approach to validity, as opposed to an approach based solely on cross-sectional data or evaluating the relationship between the AMIS-II as an independent variable with outcomes assessed in the future. Specifically, we examined earlier parent reports of responsibility behaviors, self-care skills, and adaptive behavior in relation to later youth report on the AMIS-II. Additionally, items from the AMIS-II were matched with subscales of similar constructs to expand evidence of construct validity.
In a prior study, using the same longitudinal dataset when children were 8 –15 years old (Time 1) and 10 –17 years old (Time 2), children gained responsibility for their care and mastered independence skills over time [5]. Therefore, it may be that parent reports of children’s responsibility for care when the children are 10 –17 may predict later AYA responsibility for care (when the AYA is over 18 years of age). Similarly, evidence suggests that about half (55%) of AYAs began to perform skills such as catheterization at a mean age of 9.45 years (±2.97) [25]. Thus, it would be expected that parent-reported child independence in performing skills at an earlier developmental time period would be associated with later AYA mastery of condition-related skills. Moreover, at least half of adolescents with SB acquire autonomy skills such as saving money and cooking pre-packaged meals by 12 years of age, whereas skills not accomplished until about 18 years are cooking independently, doing laundry, and managing a bank account [9]. Therefore, activities or behaviors when children are 10 –17 years old such as home living skills, ability to understand the value of money, and communication skills may also predict future household skills, managing money, and social communication skills as young adults.
The current study sought to: (1) describe the association between demographic/condition-related characteristics and scores on the AMIS-II; (2) evaluate the construct validity of the AMIS-II with measures of child responsibility for SB-related care, the child’s ability to perform skills across SB-related tasks, and adaptive behaviors; and (3) determine the internal consistency reliability of the AMIS-II in a more diverse sample than in previous research. The approach included multi-informant data from youth, mothers, and fathers across two waves of data that were 6 years apart [29].
With respect to hypotheses, demographic (e.g., older age, female sex, White Non-Hispanic/Latino race/ethnicity) and condition-related severity (e.g., less severity or a higher level of gross motor functioning) were expected to be associated with the AMIS-II subscales and total scale (i.e., better self-management). We also hypothesized that greater levels of child responsibility for SB-related care, ability to perform condition-related skills, and adaptive behaviors would be associated with higher levels of independence and self-management 6 years later (i.e., AMIS-II subscales: condition self-management and/or independent living behaviors). In addition, higher levels of child responsibility and skills in specific medical domains (i.e., communication, medication, appointments, bowel management, catheterization, skin checks, and exercise) were hypothesized to be associated with higher AMIS-II scores in these same domains 6 years later.
Methods
Participants were recruited from hospitals near Chicago and through a Midwest-based SB association as part of a longitudinal study examining family, psychosocial, and neurocognitive function in youth with SB [e.g., 30]. Inclusion criteria were as follows: (a) an SB diagnosis; (b) 8–15 years old; (c) can understand English or Spanish; (d) involvement of at least one main caregiver; and (e) lives within 300 miles of the study lab for home visit data collection. The study over recruited Hispanic/Latinos (n = 42), exceeding the initial target of 28 families. A total of 246 families were recruited and 163 families agreed to participate. After initial consent, 21 families either declined to participate or could not be contacted and two families did not meet the inclusion criteria. Thus, at Time 1, the beginning of the longitudinal data collection, 140 families with children with SB participated. Youth of families who declined to participate did not differ from participants on type of SB, shunt status, or the number of shunt infections [31]. Participants were 53.3% Caucasian, 12.9% African American, 27.9% Hispanic/Latino, and 5.7% of another ethnicity [29].
Longitudinal data collections occurred every 2 years. The first timepoint (Time 1) included children 8 –15 years of age and their parents; we did not use these data in analyses since many children would be just beginning to take some responsibility for care (e.g., intermittent catheterization). Instead, Time 2, which occurred two years after Time 1, when children were 10 –17 years old, provided more appropriate data for construct validity. Also, once youth reached 18 years of age, which included 25% of the sample at Time 3, parent data were not collected; therefore, Time 2 was the last data collection that provided parent-reported validity data for the full sample. With respect to the AMIS-II, this measure was only administered to youth over 18 years of age. By Time 5, 75% of the sample was over 18 years of age; therefore, Time 5 was used for youth reported AMIS-II scores because it provided data on a larger sample of > 18 youth than the prior time points. Moreover, Time 5 also included self-reported validity variables when participants with SB were 18–25 years of age. The current analyses included those participants at Time 5 who completed the AMIS-II interview and Time 2 data from their parents (see Fig. 1).
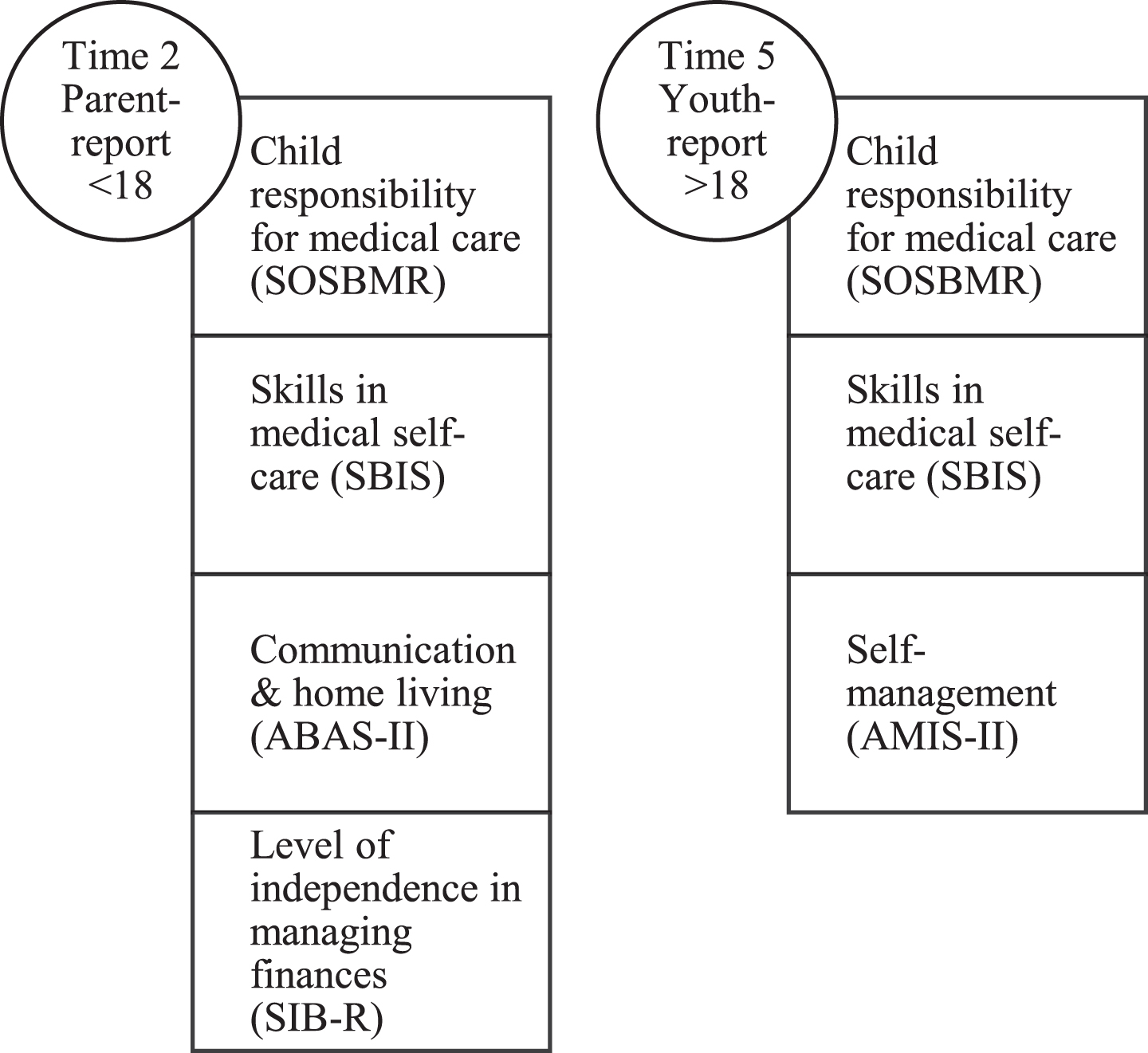
Variables by reporter and time point.
From the 140 participants with SB at Time 1, 36 were not eligible to complete the AMIS-II (i.e., under 18 years of age at Time 5), 37 did not participate at Time 5, and 3 were missing. Thus, the sample included 64 AYAs between 18 and 25 years of age at Time 5 and their parents at Time 2; either mother data, father data or both parents’ data from 55 families were available at Time 2. About half of the AYAs were female (47%), half were Caucasian (51%), 14% were African American, and 34% were Hispanic/Latino. Fifty-five AYAs (86%) had myelomeningocele. The lesion level was 34% sacral, 45% lumbar, and 17% thoracic (level of lesion was mother-reported at Time 1 and verified by medical chart review; two reports were missing and were unable to be verified). Participants were rated on their level of gross motor function using a modified version of the Gross Motor Function Classification System based on the mother’s report at Time 1. A gross motor classification scale level ranges from Level I: No braces, crutches, walker, or wheelchair (i.e., 100% unassisted walking) to Level IV: Uses wheelchair at school, long outings (i.e., < 50% walking) [32]. The gross motor functioning level mean was 2.82 (±1.03) and ranged from 1 to 4, with higher scores indicating lower levels of gross motor functioning. See Table 1 for sample characteristics.
Characteristics of the Sample
Characteristics of the Sample
Note. The sample included 64 adolescent/young adults. †Youth age range. 18 –25 years old; Gross motor functioning range low (I) to (IV) severe.
Youth completed questionnaires and the AMIS-II interview during a home visit at Time 5 conducted by trained undergraduate- and graduate-level research assistants. Parents completed questionnaires during home visits at Time 2. Informed consent from parents and assent from youth were obtained at Time 2 and AYAs > 18 years old were consented as adults at Time 5. Mothers and fathers completed questionnaires separately at Time 2. The longitudinal study was approved by university and hospital-based IRBs.
At Time 5, AMIS-II interviews were audio-recorded by a research assistant during the home visit. Participants were first provided with a definition or description of each item, then asked the interview questions. Follow up questions and/or prompts for each item were also used, as described in the administration instructions.
Measures
In addition to the AMIS-II, four instruments were used to evaluate the construct validity of the AMIS-II from multiple reporters.
Adolescent/Young Adult Self-Management and Independence Scale (AMIS-II)
The AMIS-II was developed as a clinical interview for parents of participants (or other significant adults in an AYA’s life) or for AYAs [33]; in this study, the AYA was the only respondent. Each of the 17 items on the AMIS-II (e.g., condition: complication prevention; self-management: medication, making health care appointment; transportation; social communication; problem-solving) is scored on a seven-point Likert scale (i.e., 1 = total assistance: AYA does little or none of the activity [less than 25%] to 7 =complete independence: AYA does activity independently 100% of the time; score of 8 is assigned when item is “not applicable”). For the AMIS-II, if a score of 8 was recorded, the item was omitted from the subscale score. The AMIS-II total and subscales were calculated only if no more than 2 items were missing from the scales. An individual’s subscale or total scores were based on the mean of all items that were not scored as “not applicable.” See Table 2 for a complete list of items. Based on past research, internal consistency reliability for the subscales (α= 0.70 –0.83) and the total score (α= 0.87 –0.89) was satisfactory for both AYA with SB and parent reporters (Buran et al., 2006). The internal consistency in the most recent psychometric study was also satisfactory (α= 0.80 –0.89) [17].
AMIS-II subscales and corresponding items
AMIS-II subscales and corresponding items
Note. Item 17 on family involvement has two components: (a) independence score, (b) satisfaction score. Only the independence score is used to compute the condition management subscale and the total score.
In the current study, we had two coders for each interview to assess for scoring reliability; two research assistants independently scored the Time 5 audio-recorded interviews. Intraclass correlation coefficients (ICCs; e.g., inter-rater reliability between coders of the AMIS-II interviews) were computed at the item and the scale level. Guidelines for interpreting ICCs were 0.90 = excellent; 0.80 = very good; and 0.70 = adequate [34]. The inter-rater reliability at the item level was adequate to excellent; ICCs were 0.77 –0.95. ICCs for the subscales and the total scale were excellent (0.95 –0.97).
Parents (Time 2) and youth (Time 5) reported on the SOSBMR, which was adapted from the Diabetes Family Responsibility Questionnaire. The SOSBMR instructs respondents to rate each item on a three-point Likert scale (i.e., 1 = parent responsibility to 3 = child responsibility; score of 4 is assigned when item is “not applicable” if the task is not part of their care). Higher scores indicated greater child responsibility (but did not assess the level of competence at completing the task). The SOSBMR consists of 34 SB-related responsibilities. The current study employed subscale scores of child responsibility for communication, medication, appointments, and SB-related care across four dimensions (bowel management, catheterization, skin care, and exercise) as well as total scores for child responsibility (mother and father report at Time 2; youth report at Time 5). Due to the use of “not applicable” responses, the internal consistency of the total scores could not be computed because the reliability algorithm only computes values for participants who provide a response to all items. Internal consistency reliabilities could be computed for the subscales, which were high for youth report (α= 0.84 –0.97), mother report (α= 0.75 –0.93), and father report (α= 0.79 –0.96). An exception was the low internal consistency reliability of the father-reported medication subscale (α= 0.55). This scale was retained in the analyses because the mean and standard deviation of father’s report were similar to those based on the mother’s report, and the mother’s report was reliable.
Spina Bifida Independence Survey (SBIS)
This measure was adapted for youth with SB from the Diabetes Independence Survey [36], a brief measure of the parent’s evaluation of the child’s growth and development of diabetes knowledge and skills among children and adolescents with diabetes. Participants respond “yes”, “no”, “not sure”, or “not applicable” to each item of the SBIS. A parent version (Time 2) and a youth self-report version (Time 5) were completed. For analyses, a ratio score was created based on the total number of “yes” responses over the total number of “yes” and “no” responses. This ratio provided information about the degree to which youth had mastered SB-related tasks (e.g., remembered to complete catheterization every 2–4 hours; conducted daily skin checks). Mastery of a skill indicates when youth are able to perform a skill, not what they actually do. Ratio scores ranged from 0 to 1, with a 1 indicating that a youth had mastered all of the skills. As was the case for the SOSBMR, the internal consistency of the SBIS could not be calculated because data for those participants who responded “not sure” or “not applicable” on any single item would be removed when conducting reliability analyses (due to listwise deletion).
Scales of Independent Behavior-Revised (SIB-R)
The SIB-R was used to assess an individual’s level of functioning in several areas of adaptive behavior (e.g., Fine-Motor, Money and Value) and areas of maladaptive behavior. Parent-reported data from the Adaptive Behavior Subscale of Money and Value of the SIB-R at Time 2 were included in these analyses. This subscale was selected to assess construct validity with youth report on the AMIS-II item that focused on managing money (item 9; Time 5 youth report). Items on the SIB-R are rated on a four-point Likert scale (i.e., 0 = never or rarely [even if asked] to 3 = does very well [always or almost always, without being asked]). The subscale score was the sum of the items. In the current sample, the internal consistency reliabilities were high (α = 0.93 - 0.95).
Adaptive Behavior Assessment System-Second Edition (ABAS-II)
Subscales from the ABAS-II were completed by parents (Time 2) to assess additional dimensions of a youth’s adaptive behavior. The measure includes several subscales; communication and home living were selected to assess the construct validity of youth report (Time 5) on relevant AMIS-II items focused on social communication (item 14) and household skills (item 12), respectively. Items were rated on a four-point Likert scale (i.e., 0 = is not able to 3 = always when needed). The subscale scores were the sum of the items. In the current sample, the internal consistency reliabilities for these subscales were high (α = 0.93 - 0.97).
Analyses
Preliminary analyses examined variables for outliers and skewness. To evaluate the associations between demographic/condition-related characteristics and the AMIS-II, Pearson correlations were run between continuous variables. Independent samples t-tests were used to assess differences on the AMIS-II by sex and ethnicity (i.e., Hispanic/Latino background vs non-Hispanic/Latino). Differences by multiple categories of race/ethnicity were further examined using one-way ANOVAs. The internal consistency reliabilities of the AMIS-II total scale and subscales were reported using the coefficient alpha for Time 5 data. The internal consistency reliabilities were also computed for the AMIS-II total scale and subscales in a subsample of Hispanic/Latino participants. To evaluate the construct validity of the 2 subscales and the total scale of the AMIS-II, Pearson correlations were run between the AMIS-II subscales/total score and the total scales of child responsibility for SB-related care (SOSBMR) and the child’s ability to perform skills across SB-related tasks (SBIS). The validity of the AMIS-II independent living subscale was further assessed with the adaptive behaviors subscales (i.e., communication and home living subscales of the ABAS-II and money and value subscale of the SIB-R).
Corresponding validity measures were also identified for 3 items from the condition management subscale of the AMIS-II and 4 items from the independent living subscale of the AMIS-II. Specifically, Pearson correlations were calculated between 4 AMIS-II items (Condition: Knowledge, Self-management: Ordering medication/supplies, Self-management: Making health care appointment, and Condition: Complication prevention) and several measures of child responsibility for SB-related care (i.e., subscales on communication, medication, appointments, bowel care, bladder care, skin checks, and exercise). Correlations were also calculated between 2 AMIS-II items (Social communication, Household skills) and 2 adaptive behavior subscales of the ABAS-II (communication, home living). Finally, a correlation was computed between the AMIS item for managing money and the relevant subscale of the SIB-R (money and value). See Table 3 for AMIS-II items and corresponding validity variables.
AMIS-II Items and Corresponding Validity Variables
AMIS-II Items and Corresponding Validity Variables
Note. Sharing of Spina Bifida Management Responsibilities (SOSBMR); Adaptive Behavior Assessment System (ABAS-II); Scales of Independent Behavior-Revised (SIB-R)
Several analyses were conducted: attrition analyses, preliminary analyses (i.e., data screening and inter-rater agreement), internal consistency reliability analyses, descriptive statistics, and construct validity analyses.
Attrition analyses
While the majority of families participated at Time 2 and Time 5 of the study, not all participants from Time 1 completed subsequent visits (ineligible because not 18 + years old: NTime5 = 36, 26%; declined at Time 5: NTime5 = 37, 26%). Cases included in the analyses were based on completion of the AMIS-II interview (NTime5 = 64, 63% of those eligible to complete the AMIS in the sample). Parent data at Time 2 were included in the analyses if the corresponding cases had complete data on the AMIS-II at Time 5. Chi-squares and independent samples t-tests were used to identify significant differences in characteristics of the sample between those who were included and those who were excluded from the analyses. No significant differences were found between these groups on age, sex, race/ethnicity, SES, level of lesion, gross motor functioning (p’s > 0.1).
Preliminary analyses
All variables were examined for outliers. Several measures contained 1-2 outliers, as determined by scores greater than±3 standard deviations from the mean. For this reason, the following outlier scores were not included: two youth reports and one mother report on the SBIS, two youth reports on the SOSBMR total score, one mother and one father report on the SOSBMR appointment subscale, and two mother reports on the ABAS-II communication subscale. Subsequently, all variables were also evaluated for skewness determined by values greater than±2. The highest skewness value was –2.136 for the youth-reported catheterization subscale of the SOSBMR. All other skewness values were below 2.0. Thus, data transformations were not conducted.
Agreement between mother and father report on all subscales and total scales was evaluated using inter-rater reliability analyses. ICC coefficients between parents were 0.40 –0.87. The lowest agreement was found for the SOSBMR subscales of child responsibility for appointments (0.40), communication (0.45), skin checks (0.57) and medications (0.60); therefore, all findings for mother and father data were reported separately.
Internal consistency reliability analyses
Overall, the AMIS-II demonstrated adequate internal consistency reliability. Internal consistency reliabilities for the AMIS-II total scale and subscales were high (α= 0.90 –0.95). In the Hispanic/Latino subsample, the internal consistency reliabilities were also high for the AMIS-II total scale (α= 0.94) and the subscales (α = 0.88 –92).
Descriptive statistics
Descriptive statistics for the AMIS-II are reported in Table 4. With the AMIS-II scores ranging from 1 to 7, the means for the current sample were as follows: total scale 3.71 (±1.33), independent living self-management subscale 3.43 (±1.35), and condition self-management subscale 4.11 (±1.45). The two subscales were highly correlated (r = 0.823, p < 0.001). The item-to-total correlations for the total scale were r’s=0.563 –0.828. The item-to-total correlations for the independent living subscale were r’s = 0.443 –0.803 and, for the condition subscale, they were r’s = 0.617 –0.772. The items with the lowest item-to-total correlations for the total scale were self-management of medication (item 3, r = 0.566) and social communication (item 14, r = 0.563). Similarly, the lowest item-to-total correlations for the subscales were also self-management of medication (item 3, r = 0.617) and social communication (item 14, r = 0.443).
Descriptive Statistics for AMIS-II
Descriptive Statistics for AMIS-II
Age was not associated with the AMIS-II subscales or the total AMIS-II self-management score (r’s = –0.087 –0.114, p’s > 0.05). Independent samples t-tests revealed no differences in the AMIS-II subscales and overall AMIS-II scale by sex or ethnicity (Hispanic/Latino vs. non-Hispanic/Latino). One-way ANOVAs examining differences in the AMIS-II subscales and overall AMIS-II scale between Caucasian, African-Americans, and Hispanic/Latinos were nonsignificant. Gross motor functioning at Time 1 was significantly associated with the AMIS-II subscales and overall scale in the expected direction; more severe gross motor function was associated with less independence (r’s = –0.249 to –0.346, p’s≤0.05).
This section reports correlations between AMIS-II subscales/items and the construct validity variables. All bivariate correlations between the validity measures (e.g., SOSBMR total, SBIS ratio, ABAS-II communication and home living, and SIB-R money and value) and the two subscales of the AMIS-II were significant. See Table 5.
Bivariate Correlations of Subscales by Multiple Reporters
Bivariate Correlations of Subscales by Multiple Reporters
Note: Pearson correlations reported. **Significant at the 0.01 level. *Significant at p < 0.05.
Parent-reported (Time 2) child responsibility for communication, appointments, bowel management, catheterization, skin checks, and exercise were also associated with the corresponding Time 5 AMIS-II items (see Table 6 bivariate correlations with parent report) (r’s = 0.302 –0.817; p’s < 0.05). However, parent-reported child responsibility for medication management was not significantly associated with the AMIS-II medication item (mother report r = 0.159, p = 0.315; father report r = 0.229, p = 0.208). The correlation between parents’ report of the child’s communication and home living skills at Time 2 (ABAS-II subscales) and youth-report on social communication and household skills at Time 5 (items 12 and 14 of the AMIS-II) were significant when the former were reported by mothers (r’s = 0.514 –0.543, p’s < 0.01) and fathers (r’s = 0.414 –.518, p’s < 0.05). The correlation between parents’ report of the child’s management of finances at Time 2 (SIB-R- money and value) and youth-report on managing money more independently at Time 5 (item 9 of the AMIS-II) was significant when reported by mothers (r = 0.543, p < 0.01) and fathers (r = 0.352, p < 0.05). AYA reported (Time 5) responsibility for communication, medication, appointments, bowel management, catheterization, skin checks, and exercise were associated with the corresponding Time 5 AMIS-II items (r’s = 0.477 –0.730, p’s < 0.01; see Table 6).
Bivariate Correlations of Youth-Reported AMIS Items and Subscales of SOSBMR, ABAS-II, and SIB-R by Multiple Reporters
Note. Pearson correlations. **Significant at p < 0.01. *Significant at p < 0.05.
This study supports the internal consistency reliability and the construct validity of the AMIS-II in a diverse sample of youth with SB with longitudinal, multi-informant data. This study also provides evidence of an association between condition severity and the AMIS-II, but there were no significant associations between demographic characteristics and the AMIS-II.
The demographic characteristics were not significantly associated with the subscales of the AMIS-II, which was unexpected. Age was not associated with better self-management (i.e., AMIS-II subscales and total scale); although, in previous work that employed the original 10-item version of the AMIS, age was positively associated with self-management (i.e., AMIS total scale) among individuals with SB (r = 0.68) [15]. In addition, in a recent psychometric study of the 17-item version of the AMIS-II, age was associated with self-management (i.e., a small but significant correlation with youth-report on the AMIS-II condition self-management subscale, r = 0.30; a larger correlation with youth-report on the AMIS-II independent living subscale, r = 0.54) [17]. Importantly, these earlier studies had a broader age range (12 –25 years) than the current study (18 –25 years). Perhaps less variability across the age range and the older ages in the current sample may explain these discrepancies across studies. Indeed, it is possible that differences across age on self-management are more likely to be present when comparing adolescents to young adults as opposed to within a cohort of young adults only.
Differences by race/ethnicity on AMIS-II total scale and subscales were expected, but not found in this sample (where 34% were Hispanic/Latino). However, internal consistency reliability in the subsample of Hispanic/Latino participants was high. Therefore, findings support the use of the AMIS-II in diverse samples, specifically Hispanics/Latinos.
Also, unexpectedly, the means of the AMIS-II total and condition subscales in this study (total scale 3.71±1.33; independent living subscale 3.43±1.35; condition subscale 4.11±1.45) were slightly lower than cited in previous work (total scale 3.92±1.37; independent living subscale 3.38±1.52; condition subscale 4.70±1.46) [17]. We expected that the older age range in this sample would yield more rather than less advanced self-management. As they mature, perhaps AYAs with SB report their self-management more realistically as they gain more experience; for example, participants in a bladder and bowel management intervention rated their own performance poor after training [37]. Another explanation may be the diversity of the sample, although race/ethnicity was not significantly related to the AMIS. It is possible that parents of Hispanic/Latino ethnicity, known to perceive their child with SB as being more vulnerable [29], may provide more assistance in the youth’s care. Also, in the current study, youth of all IQ levels were included, which may have lowered the overall level of the AMIS-II scale scores.
The significant association between gross motor function and overall self-management (AMIS-II total scale) is similar to the significant association found between lesion level and overall self-management in a psychometric study by Sawin et al. (2018) [17], although the current sample has a slightly higher proportion of individuals with sacral lesions (34% versus 28%). The current longitudinal sample (17% thoracic, 45% lumbar, 34% sacral) also has somewhat fewer participants with lumbar lesions and more with sacral lesions than the clinic-based sample from the National Spina Bifida Patient Registry (15% thoracic, 55% lumbar, and 30% sacral) [38].
Overall, associations were found between the skills in communication/home living/money and the independent living subscale of the AMIS-II. Construct validity of the AMIS-II was supported by associations with these basic living skills. Higher levels of communication and home living skills translated to better social communication and independent household skills 6 years later. Although construct validity was found, social skills (i.e., social communication) are challenging for youth with SB due to their neurocognitive profile [39]. Youth reported a mean of 4.19 on the AMIS-II social communication item (range 1 to 7) indicating a self-identified need for some assistance and prompting. It is possible that parent reported skills at younger ages may not be associated with later mastery if there are executive functioning difficulties that are observable in their child at an older age. Parents may perceive and possibly report the necessary level of support differently as the youth ages.
It is also possible that the wording of questions in the different scales impacted how parents or youth reported on the level of independence. Across instruments, respondents were asked about responsibility, mastery, ability, frequency, and performance of behaviors. Specifically, respondents were asked to report on taking or sharing responsibility (SOSBMR), if they had mastered a skill (i.e., able to do, not what they actually do; SBIS), how well they were able to do a task (SIB-R), and how often a behavior was correctly performed without help (ABAS-II). The latter measures were collected using questionnaires. The AMIS-II asks about what the individuals do, while assessing their required level of assistance to perform a behavior using a tiered interviewing strategy with follow-up questions. In contrast to data collection with questionnaires, the interview process provides an opportunity for probing and clarification.
Youth at Time 5 tended to rate themselves as requiring minimal assistance/prompting or needing some supervision for medication self-management. This finding may indicate either that youth need parents to physically prepare and organize their medication in some way or that youth take their medication as recommended but know little about these medications. The age of the children at the time that the parent data were collected in this study may be an explanation for why parent-reported self-management of medications was not related to later youth-reported responsibility for medications on the AMIS-II. Medication use is certainly a target for ongoing education in clinical practice since any missed medications can have an effect on health status (e.g., bladder and/or bowel complications). It may be helpful for clinicians to educate AYAs on developing their own reminder system for medication self-management. Interventions using mHealth (such as iMHere) now exist to facilitate this process for youth with SB [40]. Feasibility testing of this intervention showed an increase in self-management behaviors over time; this is a promising intervention to support care for youth with this complex medical regimen, most of whom have cognitive difficulties.
For AYA with specific executive functioning abilities, the AMIS-II provides a measure of performance of behaviors even when youth are dependent on assistance. If the AYA is monitored over time and scores are consistently low, it offers health care providers information about gaps in self-management behaviors or the need to support family self-management. As AYA transition to adulthood, monitoring self-management independence remains important to identify needs for additional caregiver resources to mitigate risk of lapses in condition management.
The evidence of internal consistency for the AMIS-II was high (α= 0.90 –0.95) and the subscales of the AMIS-II were highly correlated (r = 0.823). This latter finding is inconsistent with an earlier report of psychometric evidence where the correlation between subscales was moderate (r = 0.44) [17]. This finding may be explained by the age range of the sample in the current study, 18 –25 versus 12 –25 years of age in Sawin et al.’s sample [17]. Indeed, a large association between individual-level change scores of the AMIS-II subscales (r = 0.71) over a 15 month period was also found in Bellin et al.’s (2012) sample of young adults with SB (19 –26 years of age) [41]. The larger associations in the current study and in Bellin et al.’s study may reflect a closer, more overlapping relationship between condition self-management and independent living behaviors in older youth.
Alternatively, the differences in the correlations between the two subscales across the current study and the Sawin et al. sample may also be due to the composition of samples, as they appeared to differ by type of SB. A descriptive study of participants in the National Spina Bifida Patient Registry found that those with myelomeningocele differed from others with SB on most clinical variables [42]. The current study had 55 participants (86%) with myelomeningocele, which is similar to Bellin et al.’s (2012) sample of young adults (85.5% myelomeningocele); as noted above, the subscale correlations were similar for the current study and Bellin et al.’s study. Whereas other studies using the AMIS-II had samples with myelomeningocele only and did not report correlations [e.g., 43, 44], Sawin et al. (2018) reported that participants had SB but did not delineate the SB type [17]. Clearly, delineating the type of SB in future samples and analyzing data by type of SB when possible may further the understanding of the interrelations between the AMIS-II subscales.
Additionally, the sample reported in Sawin and colleagues’ psychometric study and most other studies using the AMIS-II, have been clinic-based, whereas individuals in the current sample were participating across multiple occasions in a longitudinal research program. Participation in an ongoing research project may have triggered awareness and adoption of self-management behaviors, thus potentially increasing the association between the subscales. It is also possible, with the high alpha for the total score and the high Pearson correlation between scales in this study, that the AMIS-II is a unidimensional scale in some populations. Regardless of the reason for the differences in subscale correlations across studies, further evaluation of the AMIS-II factor structure is needed.
Limitations and future research
While the AMIS-II appears to be a highly reliable and valid assessment of self-management in youth with SB, data collection does require an interview as well as coding decisions. Generic and SB-specific self-report versions of the AMIS-II have been developed but are not yet tested [45]. It is recommended that the self-report versions be evaluated psychometrically in future research. Given the high internal consistency values, it appears that the measure could be shortened without compromising internal consistency. Unfortunately, the current psychometric analysis was conducted on a small sample of 64 youth; thus, insufficient power prevented more in-depth analyses such as a factor analysis. A factor analysis in a larger sample of young adults would be a useful addition to the literature. Further psychometric testing could also evaluate the possibility that the AMIS-II measures multiple different constructs.
The association between gross motor functioning at Time 1 and the AMIS-II 10 years later, while significant, may be confounded by a decline in motor functioning with age. Evaluation of motor functioning at the same time as self-management is important but was not conducted in this study. The lack of parent-report on the AMIS-II at Time 5 also limited our ability to evaluate known differences between parent and youth report of self-management. Another limitation of our study is that we did not include measures of cognitive functioning in our analyses; therefore, the potential impact of cognition on the associations between the AMIS-II and the validity measures was not tested. Further, we did not analyze the differential predictive utility of child responsibility for care (SOSBMR), independence in medical tasks (SBIS), and overall self-management (AMIS-II) for salient outcomes in individuals with SB (e.g., the transition to adult health care, clinical health outcomes). These outcome variables were not yet available in this longitudinal dataset. Future research should assess the unique contribution of the AMIS-II above and beyond other related measures as a predictor of future health complications and secondary conditions.
Further evaluation of the AMIS-II is warranted to understand the high correlation between the two subscales. Although, the item-to-total correlations were satisfactory when evaluating the AMIS-II total scale (r’s > 0.56), the lowest item-to-total correlations for the AMIS-II subscales were found for the medication and social communication items (item 3, r = 0.62; item 14, r = 0.44); thus, these items might need to be modified for emerging adults and tested in future studies.
Conclusion
This study supports the internal consistency reliability and construct validity of the AMIS-II with a relatively diverse and longitudinal sample. For youth with SB, responsibility for SB-related care, the ability to perform skills across SB-related tasks, and independent living behaviors (i.e., communication, home living, finances) appear to be related to self-management behaviors (independent living and condition self-management) as measured by the AMIS-II. Thus, the AMIS-II appears to be an appropriate method for monitoring the “achievement” of self-management over time and may identify components of self-management behaviors that are predictive of future health outcomes for individuals with SB.
Footnotes
Acknowledgments
This research was supported in part by grants from the National Institute of Nursing Research and the Office of Behavioral and Social Sciences Research (R01 NR016235), Eunice Kennedy Shriver National Institute of Child Health and Human Development (R01 HD048629), and the March of Dimes Birth Defects Foundation (12- FY13–271). This study is part of an ongoing, longitudinal study. Dr. Stiles-Shields is also supported by a fellowship from the Cohn Family Foundation. Dr. Sawin is a consultant for the Spina Bifida Association, on the Board of MetaStar (a quality improvement organization), and a funded investigator at the Wisconsin site on the National Spina Bifida Patient Registry Project (funding from Centers for Disease Control and Prevention).
The authors thank the Illinois Spina Bifida Association as well as staff of the spina bifida clinics at Ann & Robert H. Lurie Children’s Hospital of Chicago, Shriners Hospital for Children-Chicago, and Loyola University Medical Center. We also thank the numerous undergraduate and graduate research assistants who helped with data collection and data entry. Finally, we would like to thank the families who generously participated in this study.
Conflict of interest
The authors have no conflict of interest to report.