A rise in pediatric patients with swallowing and feeding problems has resulted in
increased interest in multidisciplinary treatments to address these issues. This
evidence based systematic review (EBSR) examined the published evidence for the use of
common strategies used by clinicians across disciplines to treat pediatric swallowing
and feeding problems.
METHODS:
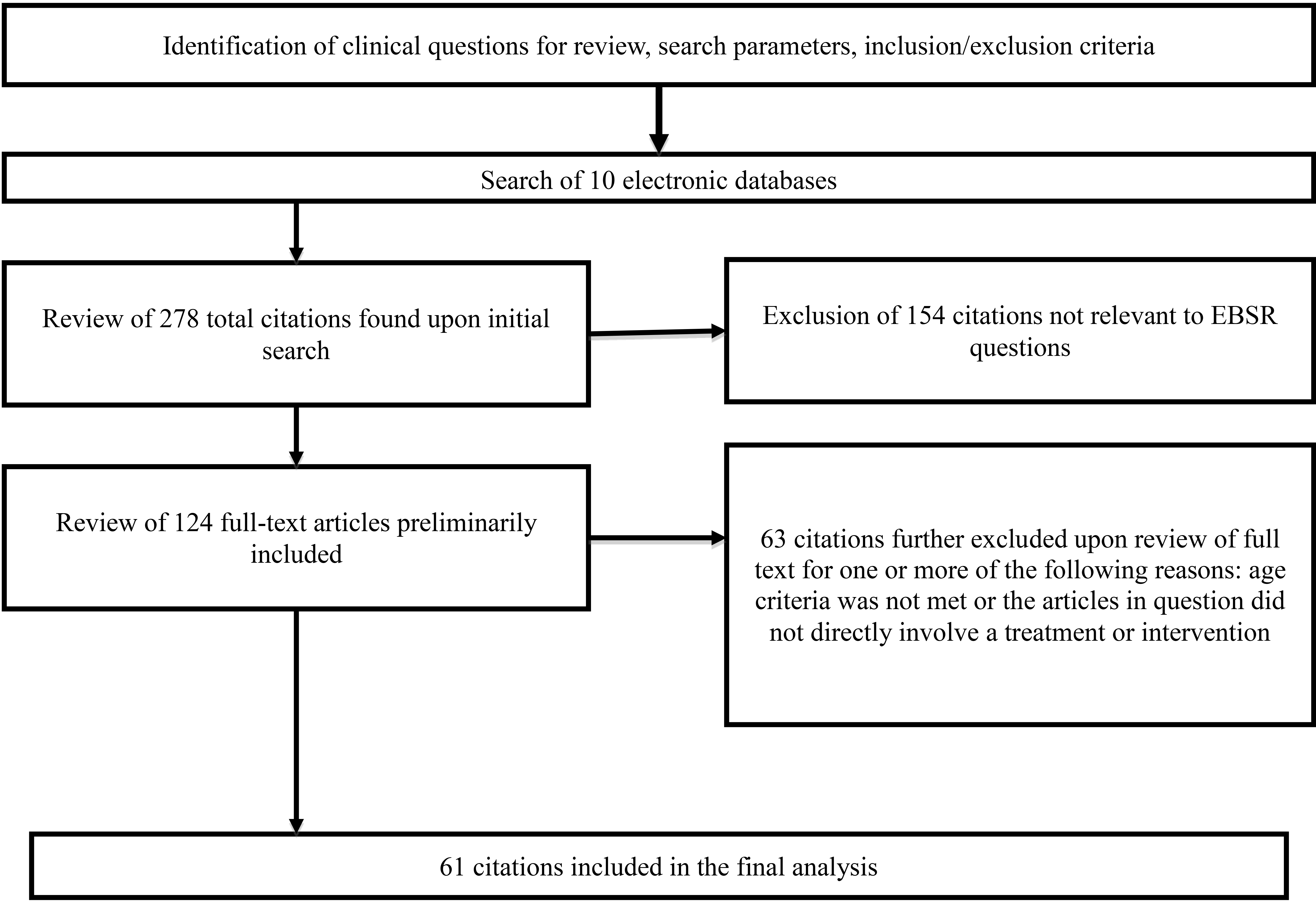
A systematic search of 10 electronic databases was completed to identify relevant,
peer reviewed literature published in English prior to December 2015 reporting original
data that addressed at least one of the five identified clinical questions.
RESULTS:
Sixty-one studies of varying methodological quality were included. The majority of the
included studies (60/61) focused on the use of behavioral therapies to remediate
swallowing and feeding disorders in children and reported mixed findings across all of
the targeted outcomes.
CONCLUSION:
There is insufficient quantity of evidence to determine the effects of oral motor,
sensory, and pharmaceutical therapies on functional feeding outcomes in pediatric
populations. A larger body of phase 1 evidence is available that establishes the
efficacy of behavioral strategies to treat some swallowing and feeding difficulties in
small cohort and single subject studies. This analysis identified limited high quality
(phase 4) research articles that establish the efficacy and benefit of joint nutrition
and behavior intervention programs and systematic desensitization and operant
conditioning behavioral therapy approaches to improve functional feeding and swallowing
outcomes in children.
Pediatric feeding and swallowing disorders have the potential for significant
morbidity and even mortality due to multiple body system involvement [1]. Successful remediation of pediatric feeding and swallowing
disorders requires a clear understanding of the contributing factors from accurate diagnosis
by a multi-disciplinary team of professionals that may include dieticians, nurses,
physicians (developmental pediatrician, gastroenterologist, pulmonologist, and/or
otolaryngologist), therapists (speech-language pathologists, occupational therapists, board
certified behavior analysts (BCBA), and/or physical therapists), psychologists, social
workers, and caregivers [2, 3, 4]. The
multidisciplinary feeding team contributes to the number of treatment modalities (oral
motor, sensory, behavioral, and pharmaceutical) recommended to address the multisystem
nature of pediatric feeding and swallowing disorders [1, 5, 6, 7].
Pediatric swallowing disorders (dysphagia) and feeding disorders have
distinctive diagnostic criteria. Pediatric dysphagia is a skill-based disorder that
interrupts the typical, coordinated actions of the swallowing mechanism. Pediatric feeding
disorders are best described with the revised classification of avoidant/restrictive food
intake disorder (ARFID) [8]. ARFID describes
children that may or may not be a normal weight, who have restricted eating patterns that
are not related to body image and whose lives and the lives of their families are
significantly impacted by their restricted oral intake [9].
Multidisciplinary swallowing and feeding teams often prescribe a number of
different treatment modalities (oral motor, behavioral, sensory, and pharmaceutical) to
address pediatric feeding and swallowing problems, once the overriding medical issues (when
present) have been ameliorated. There are also treatment programs available that utilize two
or more of the listed treatment modalities [10,
11]. While various treatment modalities are
utilized in feeding clinics, the evidence that demonstrate their efficacy and support their
use for various populations are not readily known. For these reasons, the authors felt this
study was necessary to document the levels of evidence available to support common treatment
modalities used to address feeding and swallowing problems in medically stable patients.
There have been previous evidence based systematic reviews published that
evaluated some of the treatment modalities in isolation [5, 12, 13, 14, 15]. Previous reviews of oral motor interventions on
swallowing in preterm infants [12] and
children [13] found that for preterm populations
some oral motor interventions have preliminary evidence to show limited benefit for
enhancing feeding/swallowing skills [12] and for
children there is insufficient evidence to determine the effect of oral motor interventions
on remediation of swallowing problems [13]. In
both reviews on oral motor interventions, there was specific discussion regarding the
methodological limitations of the current evidence available on this modality. Angell (2010)
reviewed treatment methods to address selective eating and tactile sensitivity and describes
them along with the limited published evidence available to support them [14]. Finally, McGrath and colleagues (2010) primarily report on the
behaviorally based treatments and the available evidence to support them for children with
severe feeding issues, children who do not eat orally, and children who are dependent upon
gastrostomy tube for nutritional support [15].
This study represents the first evidence based systematic review (EBSR) to cover all studies
on one or more of the most commonly prescribed treatment modalities: oral motor, behavioral,
sensory, and pharmaceutical.
The primary purpose of this EBSR was to examine the state of the evidence for
the use of oral motor, behavioral, sensory, and/or pharmaceutical interventions to treat
pediatric feeding problems. Specifically, the effects of the various treatment modalities on
the functional feeding outcomes of feeding behavior(s), volume of oral intake, variety of
oral intake, days to wean tube feeding dependence, weight gain, and/or growth in pediatric
populations aged six months to eighteen years were evaluated. Additionally, the goal was to
draw attention to the possible gaps in the current evidence base. In developing the clinical
questions, the impact of each treatment modality applied individually was considered. Thus,
the first four clinical questions of this EBSR were:
What is the effect of oral motor interventions on functional oral
feeding outcomes in children? Oral motor interventions included exercises and
activities that were designed to influence the action(s) of the tongue, lips, soft
palate, jaws, larynx, and/or respiratory muscles for improved strength, tone, range of
motion, or coordination during feeding/swallowing and included traditional muscle
exercises (active or passive), stretching, and/or sensory stimulation to the
articulators and related structures [13].
What is the effect of sensory-based interventions (exercises and
activities that are designed to promote sensory integration such as using a brushing
or vibration protocol, a weighted vest, or deep pressure in the joints) on functional
oral feeding outcomes in children [16]?
Methodology flow chart.
What is the effect of behavioral-based interventions (including
approaches that incorporate techniques with elements from operant condition- ing,
systematic desensitization, etc.…) on func- tional oral feeding outcomes in
children? [17]
What is the effect of pharmaceutical-based interventions (including any
pharmaceutical agent prescribed by a physician for the documented purpose of improving
oral intake) on func-tional oral feeding outcomes in children?
Due to the known benefits of treating pediatric feeding and swallowing
problems within a multidisciplinary team framework [18], the search criteria was expanded in the final question to include all
studies that utilized two or more of the targeted modalities (oral motor, behavioral,
sensory, and/or pharmaceutical interventions).
What is the effect of applying mixed modality interventions on
functional oral feeding outcomes in children?
Methods
A systematic search of the literature was undertaken by a multidisciplinary team
of therapists with extensive experience treating feeding and swallowing disorders in
pediatric patients, two speech-language pathology graduate students, and one speech-language
pathology undergraduate student in accordance with methodology that was previously
described [19]. All students involved in this
project were under the direct supervision of the first author. Ten different databases
(PubMed, MEDLINE (Ovid), CINAHL (Cumulative Index to Nursing and Allied Health), PsycINFO,
ERIC (Education Resource Information Center), Science Citation Index (Web of Science),
Social Science Citation Index (Web of Science), Academic OneFile, Health Source:
Nursing/Academic, & PsycArticles (NAAL)) were systematically searched between March and
August 2014 and then again in November 2015. Search terms included systematic combinations
of the following terms in order of population, disorder, and intervention: (population
terms) pediatrics, infants, toddlers, children, adolescents, (disorder terms) dysphagia,
swallowing disorder, feeding disorder/problem, volume limiting, limited variety,
(intervention) oral-motor therapy, sensory-based therapy, behavior-based therapy,
pharmaceutical therapy, mixed therapeutic interventions, and their related Medical Subject
Headings (MeSH) terms. The same search terms & systematic combinations of those search
terms were used for each database. Search terms were determined based on their relevance to
the established clinical questions, identified from review of pertinent articles, and
incorporated into the overall search strategy. To qualify for inclusion, a study had to be
written in English, published (or in press) in a peer-reviewed journal between January 1960
and December 2015, provide original data addressing at least one of the identified clinical
questions, examine infants and children from six months of age to 18 years of age with
dysphagia, feeding delay, or feeding disorder as either a primary or secondary diagnosis,
and feature an experimental, quasi-experimental, or single subject design. The date range of
January 1960 to December 2015 was chosen in order to capture the most recently published
evidence (within the last 50 years) relating to the clinical questions. Studies were
excluded if they presented only information from literature review, if the age of the
participants was outside of the specified range, or if the study reported on oral feeding
outcomes in children without a diagnosis of either swallowing and/or feeding disorder.
Inclusion and exclusion criteria were established in order to identify all of the empirical
literature that addressed one or more of the established clinical questions.
Three independent reviewers identified 61 citations for final inclusion (Fig. 1). Study eligibility agreement
between reviewers was accomplished through initial individual review of abstracts with
follow up discussion and consensus before final inclusion. The number of initial
disagreements was not documented and therefor reliability between the reviewers could not be
calculated.
Using a structured rating system [20]
three independent reviewers assessed all of the included articles to identify areas of
methodological weakness and possible bias (Table 1),
in addition to summarizing key elements (participant characteristics, treatment modality,
treatment intensity and duration, and outcomes) from each study. Table 2 provides a summary of the methodological quality for each
article included in this EBSR.
Final scoring agreement for assessment of methodological features was 100% as
all initial discrepancies were resolved through discussion and consensus and again the
number of initial disagreements was not documented and therefor reliability between the
reviewers before reaching consensus could not be calculated. Tables 3–5 summarize the quality indicators
of the included studies, the participant characteristics, key study variables and findings.
All studies, regardless of methodological rigor were included in this analysis as a stated
purpose of this EBSR was to establish the quality of evidence available to support various
treatment modalities for improving oral feeding measures in children with swallowing and/or
feeding disorders.
Results
Results are presented in order of the clinical questions posed. With regards to
Clinical Question 3 (Behavioral), results are presented with subheadings in order of
behavioral techniques utilized in the articles: positive reinforcement and extinction;
stimulus shaping and fading; caregiver involvement and education; operant conditioning and
systematic desensitization. For Clinical Question 5 (Mixed Modality), results are presented
with subheadings in order of combinations utilized in the articles: behavioral and oral
motor; behavioral and sensory; behavioral and pharmaceutical; behavioral, oral motor, and
sensory.
Clinical Question 1 (Oral Motor)
One of the 61 included studies examined clinical question one [21]. The 20 participants in this experimental,
randomized control trial study had profound intellectual disability or neuromuscular
disorders, lived in a residential care facility, and were identified by the residential
staff as being problem feeders. The authors implemented an oral motor program that
included manual intervention, direct guidance, stretches, pressure, and oral
desensitization administered 30–40 minutes daily, five times a week for nine weeks for the
experimental group ( 10). The control group continued with their previously
prescribed therapeutic plan of care. Only nine subjects from the experimental group and
two from the control group had both pre and post treatment evaluations of oral motor
functioning. Analysis of the nine experimental subjects that had pre and post treatment
oral motor function testing revealed no significant change following treatment.
Statistical analysis of the full sample ( 20) revealed no significant difference in body weight gains
between the experimental and the control group at discharge [21]. See Table 3 for
details.
Clinical Question 2 (Sensory)
None of the 61 articles included examined only sensory-based
interventions.
Quality indicators
Research design
Research protocol
Blinding
Type
of sample
For
RCTs only: Analysis by intention to treat
Evidence of treatment fidelity
value
Precision
*Randomized controlled trial Cohort Study
*Description of research protocol sufficient for replication
*Yes,
assessors were blinded
*Sample was randomized into treatment conditions with sufficient description
for replication
*Yes,
analysis by intention to treat
*Yes,
authors provide evidence of treatment fidelity
*Significance reported w/ values (or provided sufficient information to
calculate)
*Effect size AND confidence intervals were reported or there was sufficient
information to calculate
Retrospective case control or single subject design
Description of research protocol insufficient to allow for replication or not
explicitly stated
No,
assessors were not blinded or it was not explicitly stated in article
Sample
was randomized into treatment conditions but there was not sufficient
description for replication
No,
analysis not conducted by intention to treat
No,
authors do not provide evidence of treatment fidelity
Significance values not reported (no values) and there was not sufficient information
provided to calculate
Effect
size OR confidence interval reported/calculable
Case
series Case Study
Convenience sample, handpicked sample, or allocation of subjects was not
described
No
information on effect size or confidence interval was reported/calculable
Adapted from Gosa, Schooling & Coleman [19]; RCT Randomized controlled trial; * indicates highest
level of quality in each category.
Behavioral: Positive behavior support Daily eating schedule General case
programming Stimulus fading Positive contingency statement Prompting with prompt
fading Contingent praise Contingent access to preferred toy or activity Escape
extinction De-escalation procedure
Treatment 2–4 times/week Parent training 1–2 times/ week 15 sessions
Administered over 14 weeks
Volume
of intake with therapist Volume of intake with parent Generalization
Self-initiation
4
meals/day 5 days/week Duration average of 37 days (range 28–48 days)
Anthropometric data Acceptance Length of meal Grams consumed Percentage of
bites expelled Inappropriate meal time behaviors Time to wean from tube
feeding
Davis,
Bruce, Cocjin, Mousa, and Hyman (2010) [18]
9
7–48 M
27.5
NR
Dysphagia GERD Ring 21 abnormality VSD CP Trisomy 21 G tube dependency
Behavioral Pharmaceutical
3,
1-hour treatment sessions 14 weeks total time in program
Weight gain Calorie intake Time to wean from tube feedings
12
total sessions administered biweekly over 24 weeks
Reduction in tube feedings Weight percentile Volume of food and drink consumed
Selectivity Behaviors towards foods
Clinical Question 3 (Behavioral)
Thirty-seven of the 61 included studies examined clinical question
three [22, 23, 24, 25, 26, 27, 28,
29, 30, 31, 32, 33, 34, 35,
36, 37, 38, 39, 40, 41, 42,
43, 44, 45, 46, 47, 48, 49,
50, 51, 52, 53, 54, 55, 56,
57, 58]. Of 919 participants across 37 studies, a majority of participants (86%)
were between two and seven years old [22, 23, 24,
25, 26, 27, 28, 29, 30, 31,
32, 33, 34, 35, 36, 37, 38,
39, 40, 41, 42, 43, 44, 45,
46, 47, 48, 49, 50, 51, 52,
53, 54, 55, 56, 57, 58]. Overall sample sizes were small (1–13
participants) [23, 26, 27, 28, 30,
31, 32, 33, 35, 36, 37, 40,
42, 43, 44, 45, 46, 47, 49,
51, 52, 53, 54, 55, 56, 57,
58], however some studies had larger sample
sizes ranging from 24 to 490 participants [22,
24, 25, 29, 34, 38, 39, 41,
48, 50]. The majority of the reports examined the prescribed intervention’s impact
on volume and variety of oral intake as well as weight gain. The studies varied greatly in
reported frequency and duration of treatment. One study, the largest study identified by
this systematic review, did not specify the types of behavioral interventions used in
their protocol and instead assessed the impact of unspecified behavioral therapy
techniques on outcome success and cost in a retrospective chart review of 490
participants [24]. The results are presented
with subheadings in order of behavioral techniques utilized in the articles: positive
reinforcement and extinction, stimulus shaping and fading, caregiver involvement and
education, and operant conditioning and systematic desensitization.
Positive reinforcement and extinction
Eleven of the 37 studies reported on the use of escape extinction
(behavioral technique used to treat behaviors that are maintained by escaping or avoiding;
removing the possibility of escaping from the challenging stimulus) and reinforcement (the
use of any stimulus which should increase the probability of a desired response, can be
positive or negative) in single-subject and small cohort designs and their impact on
acceptance, intake, and presence of inappropriate behaviors at mealtime [23, 26,
27, 28, 30, 31, 32, 33, 36,
40]. Patel and colleagues reported that
differential reinforcement (advantages positive reinforcement to distinguish appropriate
behavior from inappropriate behavior; used to increase appropriate behavior and decrease
inappropriate behavior) alone was not effective for increased oral intake, but escape
extinction in combination with differential reinforcement did increase oral intake and
mouth clean (upon inspection, no visible food or liquid in the subject’s mouth following
intake without expulsion) in a small sample ( 3) [42]. Larue et
al. similarly found that using escape reinforcement (negative reinforcement technique,
utilizing escape) alone did not increase mouth clean or decrease inappropriate behaviors;
change in these behaviors was dependent on the application of escape extinction regardless
of the presence or absence of reinforcement ( 5) [35]. Penrod
and VanDalen corroborated the need for escape prevention in the reduction of problematic
hyper food selectivity and reported that increased acceptance of non-preferred foods
depended on escape prevention in the form of non-removal of the spoon plus re-presentation
of expelled bites ( 3) [43].
Bachmeyer et al. found participants decreased inappropriate mealtime behaviors and
increased acceptance of food utilizing an escape and attention extinction (removal of
ability to escape and removal of attention) combination ( 4) [23]. Wilkins
and colleagues also found that a chin prompt (gentle pressure applied in upward motion to
child’s chin and lower lip by the feeder/therapist) in combination with representation of
expulsion per bite decreased rates of expulsion and increased volume consumed
( 4) [57]. Pizzo et
al. examined the effects of an intensive 4–5 day behavioral intervention that included
meal and taste probing sessions with escape extinction for a small cohort ( 3) and found there was an overall increase in the volume
and variety of foods eaten and a decrease in inappropriate mealtime behaviors that was
maintained at 1-month post treatment [44]. Gale
et al. reported that non-contingent negative reinforcement (positive reinforcement not
related to the child producing the target behavior; reinforcement delivered on a
predetermined time schedule), positive reinforcement and extinction (disappearance of a
learned behavior when that behavior is not reinforced) of disruptive behavior lead to a
decrease in undesirable behavior during mealtime and an increase in volume of food eaten
in a small cohort of toddlers with autism spectrum disorder ( 3) [30].
Blisset and Harris described the effects a highly structured, behaviorally
based intervention program that integrated positive and negative reinforcement,
self-feeding, parent education, structured mealtimes, and repeated presentation of novel
foods in their case study report. Improvements in variety and volume of oral intake,
reduction in undesirable behaviors associated with feeding, improved parent-child
interactions during mealtimes and increases in both height and weight were reported after
completing the intervention and at specified follow-up points, up to three years post
treatment [27]. Volkert and colleagues
utilized reinforcement, escape extinction, and caregiver training in an outpatient
treatment program to enhance mastication and self-feeding skills for three study
participants and found mastication, mouth clean, and acceptance increased with early
swallow decrease for all subjects [56]. Rivas et
al. looked at self-feeding skills utilizing a similar therapeutic approach (reinforcement,
escape extinction, caregiver training) to enhance self-feeding skills. They reported that
although the probability of self-feeding increased for two subjects as the number of
caregiver-fed bites increased, the remaining subject did not self-feed consistently, even
when the ratio of self-fed to caregiver-fed bites was 1:5 [47]. Greer et al. conducted consecutive studies in which weight
gain and intake were monitored in both a child who had never swallowed food or liquid
secondary to dysphagia and a child who chronically refused food following application of
treatment with positive reinforcement and peer modeling. These authors reported an
increase in the volume and variety of accepted foods, as well as significant weight gain
with the participant in study one having weaned from tube feeding by two months’ post
treatment [31].
Stimulus shaping and fading
Eleven of the 37 articles reviewed examined shaping (behavior training
that uses differential reinforcement of successive approximations of the desired behavior)
and stimulus fading (initial prompting to perform behavior is gradually withdrawn,
ensuring the child does not become dependent on the stimulus) of placement, texture, taste
and quantity combined with ranging levels of reinforcement to eliminate food refusal or
discontinue tube feeding [28, 29, 32, 33, 36,
37, 46, 48, 49, 51, 58]. De Moor et al. reported generalization of oral
acceptance in their case series for a variety of food items during follow up at three to
twelve months with tube feeding discontinued in each subject ( 5) [28]. Luiselli
and Luiselli reported clear increases in oral intake with the reduction of
gastrostomy-tube feedings and addition of oral feeding meals in their case study [37]. Luiselli and Luiselli used visual cueing,
demand fading and positive reinforcement with a subject who was weaned from tube feeding
to full oral feeding and gained more than two pounds from pre-treatment [36]. In a retrospective analysis, Schadler et al.
examined the effect of positive reinforcement, escape extinction, and flooding (rapid and
excessive exposure to a feared stimulus) on oral intake with 86 ex-premature participants
with feeding disorders and found that 60% of them presented with some improvement in oral
intake [48]. Seiverling et al. found an
increased acceptance of bites (50% at baseline, at least 86% at follow up in single
subject design) and a decreased number of disruptive responses from children in their
small study ( 3) [49].
Groff et al. and Rivas et al. had similar findings assessing acceptance,
mouth clean, and inappropriate behaviors during mealtime in single subject and small
cohort designs [33, 46]. For Groff et al. acceptance was 0% during the reversal to
baseline with both a spoon and cup. During fading steps: acceptance and mouth clean
remained high and inappropriate behavior remained low ( 1) [33]. For
Rivas et al., fading plus escape extinction resulted in low rates of inappropriate
behaviors and high rates of acceptance (Study 1: 2/ Study 2: 1) [46]. Groff et
al., looked to increase acceptance and mouth clean and decrease inappropriate meal time
behaviors with extinction, syringe fading and planned ignoring in their later case study;
baseline mean for inappropriate behaviors decreased from 31 to 3.8 per minute following
extinction intervention. Acceptance and mouth clean increased to 98% given trials across
five meal blocks daily [32].
Wilkins et al., combined escape extinction techniques (including
non-removal of a spoon), bite representation, and a Nuk brush to increase mouth clean and
acceptance, and decrease packing (holding food in the mouth and cheeks) and expulsions per
bite in 12 subjects with generalized feeding complaints, developmental delays and G-tube
dependency. All participants transitioned from a Nuk brush to a spoon during either an
intensive outpatient or day-treatment admission or during outpatient follow up. Their
findings suggest that utensil manipulation during initial treatment of children with
severe feeding problems may be warranted [58].
Sharp et al. found retrospectively that using a combination including
stimulus fading and non-contingent access provided significant improvements regarding food
variety, consumption, and appropriate mealtime behaviors in a case series report
( 13). They found that all participants increased their
overall intake by at least 12 foods (relatively distributed across all food categories)
and treatment was effective in reducing mealtime stress during food presentations [51]. Dovey and Martin found that all subjects
( 24) increased in height, weight, and BMI when they utilized
a program that incorporated behavioral principles in teaching, parent education, and
concurrent presentations of preferred foods with target foods [29].
Caregiver involvement and education
Thirteen of the 37 studies focused on parent education and involvement in
combination with behavioral strategies such as reinforcement, escape extinction and
fading [22, 25, 26, 34, 39, 40, 41,
45, 50, 52, 53, 54, 55]. Half of these reported on findings from case
studies. Vaz et al. reported an increase in the intake of pureed foods and an increase in
self-feeding in a case study with eventual parent training and carryover [55], while Najdowski et al. reported an increase in
the variety of novel foods accepted when using these techniques mediated by parent
involvement and in-home therapy [40]. Similarly,
Binnendyk and Lucyshyn reported increased variety and calorie intake of previously
accepted and recently rejected foods as well as a decreased reliance on
Pediasure, a liquid nutritional supplement, with implementation of a
family-centered positive behavior support program in the home [26]. Tarbox et al. provided parent training regarding non-removal
of the meal and preparation of meals without consideration of child selectivity. This
single subject design found a significant increase in volume and variety of food
consumption following the second implementation of the intervention with a secondary
decrease in the length of meal times down to below 30 minutes at follow up [54].
Stark and colleagues prospectively implemented parent education provided
by clinical psychologist, pediatric dietician, and physician with personalized nutritional
and behavioral management strategies, including relaxation strategies and token reward
system to improve feeding in three children with cystic fibrosis. Reported outcomes
included meeting calorie goals at meals and average weight gain of 0.66 kg. Utilizing
positive and negative reinforcement, relaxation techniques, and parent education that
included nutritional education and behavior management training [52], Stark et al. reported increased participant calorie intake
( 9) and significant weight gain as compared to a control
group over six weeks of treatment with generalization reported at six month follow-up
studies [53]. Powers et al. utilized a
randomized controlled design to target increased caloric intake and nutritional content
with nutritional counseling and child behavior management skills with the goal of meeting
120% recommended daily allowance (RDA) per day or greater. No one met the goal at baseline
but following treatment 100% of the participants in the experimental, behavioral group met
the goal and only 16% of the control group (randomized to a waiting list) met the
goal [45].
Sharp, Burrell, and Jacquess introduced the Autism MEAL Plan to address
caregiver training for families of children with ASD ( 19) and included didactic workshops for skill acquisition
which targeted eight key subjects of parent education: introduction, structuring meals and
monitoring behaviors, ways to increase appropriate behavior, effective communication, ways
to decrease inappropriate behavior during meals, methods of introducing foods, teaching
self-feeding skills, and monitoring and maintaining progress. Following treatment,
caregivers reported a significant reduction in overall stress and large effect sizes
( 1.1) were seen on the Parenting Stress Index short form
scores [50]. Johnson and colleagues utilized a
larger sample of families ( 14) to implement a highly structured intervention package
which included individual (not group) parent training (modeling, role play, and giving
clear instructions, mealtime plans, reinforcement, shaping and fading) with video modeling
and feedback used for caregiver skills acquisition. Reported results included
statistically significant decrease in disruptive mealtime behaviors across assessment time
points and significantly reduced amounts of reported parent stress [34].
Four of the remaining studies that examined the effects of parent training
utilized larger cohorts (combined 271) [22, 25, 39,
41]. Adamson et al. found in their randomized
control trial that parents who received intervention with their children reported
significant improvements in mealtime behavior and in their parenting styles when compared
to controls ( 96). The intensity of disruptive child behaviors, general
parenting styles, and parental efficacy were also significantly improved suggesting
generalization of program skills outside of meal time with these changes observed to be
present and reliable at a 6-month follow up [22]. Opipari-Arrigan et al. reviewed the effects of parent training on behavioral
interventions versus the effects of nutritional education alone ( 67) and found that behavioral intervention education plus
nutritional counseling (Be-In-CHARGE!) resulted in significantly greater improvements in
volume of oral intake and calories with more weight gain over 9 weeks versus nutritional
education alone [41]. Similarly, Benoit et al.
(2000) reviewed the benefits of nutritional counseling versus the benefits of behavioral
technique training in the reduction of tube-feedings utilizing a randomized controlled
trial ( 64). At the third follow-up visit, 15 (47%) of 32 patients
in behavioral therapy and none of the 32 subjects (0%) in nutritional therapy were no
longer dependent on tube feeding, indicating behavior therapy is more efficacious in
eliminating the need for tube feeding than nutritional counseling alone [25]. Morawska et al. used a controlled group
discussion and in-home workbooks to educate parents on hassle free mealtimes
( 44) and found that parents reported a significant decrease
in challenging mealtime behaviors and length of meals with an increase in volume and
variety of foods eaten at six months post education [39].
Comparison of operant conditioning approach with parent education to systematic
desensitization approach with parent education
Marshall et al. conducted a randomized controlled trial to compare the
effectiveness of operant conditioning (learning approach that utilizes consequences to
control behavior; key components include positive and negative reinforcement and positive
and negative punishment) and systematic desensitization (learning approach that engages
the patient in some type of relaxation exercise and gradual exposure to increasing levels
of an anxiety producing stimulus like food) approaches, both provided with a parent
education component, to determine their impact on specific primary outcomes of dietary
intake, dietary variety, and problem feeding behaviors. The authors found significant
improvement in all primary outcomes ( 0.05) with small to medium effect sizes when groups were
combined and compared with pre and post treatment measures; however, they did not find
significant differences in outcome measures between the two behavioral treatment
conditions.
Clinical Question 4 (Pharmaceutical)
None of the 61 articles included examined only pharmaceutical-based
interventions.
Clinical Question 5 (Mixed Modality)
Twenty-three of the 61 included studies examined clinical question
five [18, 59, 60, 61, 62, 63, 64,
65, 66, 67, 68, 69, 70, 71,
72, 73, 74, 75, 76, 77, 78,
79, 80]. Of the 395 participants across 23 studies, subjects were at various
levels of dependence and were identified for the following reasons: poor oral intake,
food selectivity, food refusal, inability to self-feed or a delay in oral-motor
skills [18, 59, 60, 61, 62,
63, 64, 65, 66, 67, 68, 69,
70, 71, 72, 73, 74, 75, 76,
77, 78, 79, 80]. A majority of participants (95%) were between the ages of
2 and 10 years old. Sample populations were identified by a variety of techniques and
included children with highly variable developmental backgrounds: Down syndrome
( 12) [64, 65, 76],
autism spectrum disorder (ASD) ( 67) [68, 69, 72,
78, 80]. Goldenhar syndrome ( 3) [61]. Rett
syndrome ( 3) [73],
cerebral palsy ( 9) [18, 68, 75],
rubella syndrome ( 1) [70], and
generalized feeding complications due to other major system impairments ( 243) [59, 60, 62,
63, 66, 67, 71, 75, 77, 79,
80]. The majority of studies
( 20, 87%) featured small sample sizes (less than 10
subjects) [18, 59, 60, 61, 62,
64, 65, 66, 67, 69, 70, 71,
72, 73, 74, 75, 76, 77, 78,
80]; however, three of the included studies
featured much larger sample sizes reporting 46, 73, and 221 respectively [63, 68, 79]. As the studies reviewed the success of mixed intervention
strategies, dosage of intervention (including frequency and duration of treatment), and
intervention techniques vary greatly. Most studies implement intervention at least 5
days a week with multiple feedings throughout the day, either reporting total number of
meals per subject or regularly timed scheduled feedings defined by predetermined
criteria [59, 60, 61, 64, 65,
66, 67, 69, 70, 73, 75, 76,
77, 80]. See Table 5 for detailed
summary.
Behavioral and oral-motor interventions
Twelve of the identified 23 studies featured a combination of behavioral
and oral-motor interventions (combined 30) [62, 64, 65,
66, 67, 69, 72, 73, 74, 75,
77, 80]. All of the studies identified utilized case study or single subject designs
to describe the effects of previously discussed behavioral techniques (such as escape
extinction, reinforcement, stimulus fading, and shaping) in combination with oral motor
principles, techniques, or tools and described their combined impact on oral feeding
outcomes in heterogeneous pediatric populations [62, 64, 65, 66, 67, 69,
72, 73, 74, 75, 77, 80].
Harding, Faiman, and Wright targeted oral versus gastrostomy tube (g-tube)
intake ( 3) with intensive parent coaching regarding textures,
desensitization, and problem mealtime behaviors and reported g-tube feedings were
significantly reduced or eliminated with an overall increase in positive parent behavior
and meal time situations in 67% of patients (two of the three subjects in the
study) [67]. Sharp et al. assessed the
reduction of problem behaviors during meals and improved ability to maintain bolus within
the oral cavity in one subject with problem feeding behavior and oral motor dysfunction
due to diagnosis of cerebral palsy [74]. Data
from their case study showed reduced rates of expulsions and increased mouth cleans with
adaptation of presentation to accommodate for existing oral motor dysfunction in addition
to escape extinction and negative reinforcement [74]. Utilizing similar approaches, Eckman et al. improved variety and texture of
food eaten in 2 male participants by implementing a structured approach to teach chewing
in combination with behavioral strategies [64].
Both participants in their report were chewing with at least 80% accuracy by discharge
from therapy [64]. In a report from Vaz and
colleagues escape extinction in the form of non-removal of the spoon and use of a
preferred food or liquid chaser following food acceptance ( 3) decreased packing and increased mouth cleans [80]. Qvarfordt et al. utilized guided eating
(including physical and verbal prompts) to successfully increase oral coordination and
participation in mealtimes in three subjects with Rett syndrome [73].
Clawson and colleagues reported on the effectiveness of the Beckman Oral
Motor Program with escape extinction, reinforcement, and parent training on food
acceptance, mouth clean, negative vocalizations, inappropriate behaviors and caregiver
interactions for eight subjects [62]. At the end
of treatment, improvements were reported for mouth opening at the presentation of food,
timeliness of managing food in the mouth, toleration of longer meals, and acceptance of
larger volumes of food per meal. Inappropriate behaviors were reduced and caregivers
demonstrated increased ability to successfully feed their children with improvement in
ideal weight seen in follow up sessions [62]. A
case study from Sheppard utilized incidental teaching and positive reinforcement to teach
oral motor concepts and improve sensory tolerances for eating with daily practice at meal
and snack times over a two year period [77]. She
reported success in the development of functional feeding skills with age appropriate
textures [77].
Girolami et al. [66] and Gibbons
et al. [65] documented use of a Nuk brush in an
oral motor condition to increase tactile stimulation and escape extinction. Girolami et
al. reported that presenting and re-presenting food with the oral motor tool (Nuk brush)
was more effective in decreasing expulsions than using a spoon; however, success of the
brush may be due to negative reinforcement [66].
In contrast, Gibbons et al. attributed the weaning of gastrostomy tube feeding and the
elimination and tongue thrust in their subject to the use of the combined strategies,
oral-motor and behavioral procedures [65]. Sharp
and colleagues recruited three subjects that were all gastrostomy tube dependent and
implemented a behavioral program with variable spoon presentations to assess its impact on
reducing undesirable mealtime behaviors, mouth clean and expulsions [75]. The authors reported that the behavioral program was
effective in decreasing inappropriate mealtime behaviors and increasing acceptance of
bites; however, variable spoon presentations were necessary to reduce the level of food
expulsion and increase mouth clean [75]. Penrod,
Gardella, and Fernand found that antecedent-based strategies increased food consumption in
the absence of escape extinction for the two subjects in their study with feeding
disorders and ASD [72]. Levin et al. utilized
redistribution, swallow facilitation, and swallow chaser techniques to increase mouth
clean and decrease packing in children with ASD ( 2) [69].
Behavioral and sensory intervention
Four of the 23 studies utilized principles and techniques from sensory
integration in combination with behavioral intervention strategies [59, 63, 70, 78].
Luiselli and Gleason combined sensory reinforcement in the form of a light, rocking
motion, and texture fading to overcome chronic food refusal ( 1) [70]. Outcome
measures included acceptance and nonacceptance behaviors of solid foods; at baseline,
acceptance of solid foods was 0%. During treatment acceptance increased to above 80%.
Acceptance decreased during month follow-ups, but never fell below 80%. As Luiselli’s et
al. participant was a 4-year-old child with visual and hearing deficits, these findings
support the notion of including sensory reinforcement techniques in treating food refusal
particularly in children with documented sensory deficits [70].
Addison et al. combined individualized sensory integration therapy with
escape extinction and noncontingent reinforcement as a way to increase acceptance and
grams consumed and decrease inappropriate mealtime behaviors for two young children with
poor nutritional intake and growth [59]. Results
of functional analyses favored escape extinction plus noncontingent reinforcement for
increasing acceptance, decreasing inappropriate behavior, and increasing amount of
calories consumed [59]. Douglas and Harris
reported on a large sample ( 73) of children treated in an outpatient-feeding clinic
with a broad approach that included systematic desensitization, operant conditioning,
family therapy, positive reinforcement, appetite manipulation, sensory play, and dietary
advice to reduce the need for tube feeding, improve behavior during mealtimes and increase
weight percentiles, grams consumed, and caregiver satisfaction. The authors reported
success in outcome measures based on individualized tailoring of the vast therapeutic
approaches utilized in their clinic [63].
Most recently, Suarez retrospectively reviewed the use of sensory
integration and systematic desensitization in combination with escape extinction, positive
reinforcement, and parent training within a home therapy program ( 4) [78].
Acceptance of non-preferred foods increased. All participants showed a positive trend in
food acceptance over a relatively small number of treatment sessions (1–10) and were
discharged after caregivers reported that they were able to facilitate their child taking
at least 1 bite of every family food at every meal [78].
Behavioral and pharamceutical intervention
Two of the 23 studies reviewed the effects of pharmaceutical intervention
in combination with behavioral therapy techniques in single subject designs [18, 60].
One of the two studies looked at the use of Risperidone in three children with feeding
disorders [60]. While outcomes varied, all of
the subjects ( 3) showed improvement in oral intake with at least partial
reduction in calories administered via tube feeding [60]. Similarly, Davis et al. utilized pharmaceutical treatment (Gabapentin
and/or amitriptyline, megesterol) plus hunger provocation to assess weight gain and
percent of oral intake ( 9) [18]. Eight of
the nine subjects maintained weight and never required additional tube feedings following
treatment [18].
Behavioral, Oral Motor, & Sensory interventions from multidisciplinary
teams
Five of the 23 articles reviewed intervention techniques that involved a
multidisciplinary approach to improving feeding outcomes [61, 68, 71, 76,
79]. Clawson and colleagues utilized a large
team of providers including occupational therapy, speech therapy, feeding technicians,
dieticians, nutritionists, gastroenterologists, nursing staff, and a social worker to
target four main components during the prescribed intervention that included oral motor
exercises, structured meals, behavioral interventions and caregiver training [61]. In this small study of three children with
Goldenhar Syndrome, the authors reported a 36% increase in acceptance of food and drink,
16% decrease in the incidence of expulsion during mealtime, approximately 88% increase in
mouth clean, and a 56% decrease in inappropriate mealtime behaviors following discharge
from this multidisciplinary feeding program [61].
Trabi et al. retrospectively examined the impact of a program that
utilized hunger promotion by reduction of tube feeding in a supervised setting, including
an intensive, noninvasive monitoring of the child’s medical condition and full support of
the child’s capacity for autonomous food exploration and self-regulated intake on the time
to wean from tube feeding in 221 long-term feeding tube dependent participants [79]. The program included occupational, speech, and
psychodynamic therapy in addition to nutritional counseling for the participants and their
families. Following treatment, approximately 92% of the subjects weaned completely from
tube feeding and none of the subjects returned to tube feeding after completing
treatment [79].
Mckirdy et al. reviewed oral intake for two subjects enrolled in
school-based interdisciplinary intervention programs with a team of professionals that
consisted of school based speech therapists, consultative medical speech therapists,
classroom teachers and aides, physical therapists, occupational therapists, school nurses,
program administrators, and caregivers [71]. At
the end of treatment, one participant consumed all medications and liquids by mouth but
remained on a self-restricted diet. The other participant achieved 100% oral intake and
removal of nasogastric tube following treatment [71].
Shaw et al. retrospectively examined the oral intake of solid foods,
weight gain, duration of meals, and percentage of self-feedings in a six-year-old boy with
Down syndrome following participation in a program that combined oral motor techniques
(including the Beckman Oral Motor Program) speech therapy, and occupational therapy with
behavior modification including reinforcement and punishment as well as stimulant
medication [76]. At discharge, the subject was
reportedly eating thick soup-based mixtures with some texture added from mashed
vegetables, meats and noodles, and yogurt with fruit pieces. There was an increase in
lingual range of motion, but oral feeding skill was still limited to munching. Variety and
duration of intake improved, and the subject was able to adequately maintain a healthy
weight without the use of a high calorie supplement. At a six-month follow up, weight had
increased in accordance with developmental expectations [76].
Five-phase model of clinical-outcome research in speech-language pathology
Level of evidence
Purpose
Examples
Phase 1
To
determine if a therapeutic effect exists and determine its magnitude
Case
Studies Single-subject studies Pre and post studies of small groups
Retrospective analyses
Phase 2
To
determine the total dimensions of a therapeutic effect and implement the
necessary steps for clinical trial
Single-subject studies to test specific hypotheses Small group within-subject
studies Case-control Small-group cohort-control Estimates effect size
Phase 3
To
test efficacy of treatment strategies in clinical trials (establish internal
validity)
Parallel-group designs
Phase 4
To
determine the effect of a treatment strategy in clinical practice (establish
external validity)
Pre
and post studies of larger cohorts Parallel-groups Some hypothesis driven
single-subject studies
Phase 5
To
establish the benefits of the treatment strategy for specific populations and
determine the cost of that treatment
Laud et al. retrospectively reviewed a variety of dependent variables
including acceptance, refusal behaviors, negative vocalizations, grams consumed, caregiver
measures, food variety inventories, and caregiver satisfaction scores in a large sample of
subjects ( 46) with diagnoses of ASD with or without co-occuring
morbidity [68]. Behavioral and oral motor
therapy implemented by an occupational therapist and a speech therapist included
systematic meal sessions with individualized behavior protocols involving antecedent and
consequence manipulation. Oral motor therapy was conducted to determine safety while
eating and to perform eating and non-eating oral motor exercises. Significant differences
were found in percentages of acceptance, refusal behaviors, negative vocalizations, and
grams consumed from admission to discharge. Specifically, acceptance, refusal behaviors,
and grams consumed increased significantly while negative vocalizations significantly
decreased from admission to discharge. At three years following discharge, only 63% of the
original sample could be contacted and 100% of those who could be contacted reported a
significant increase in food acceptance and extinction of the structured therapeutic
protocol [68].
Study quality
Clinicians providing treatment to children with feeding and/or swallowing
disorders should be aware of the levels of evidence available to support the various
treatment modalities used in their recommended programs. The search strategy utilized for
the current EBSR did not reveal any published literature that examined the effects of
sensory therapies (exercises and activities that are designed to promote sensory
integration such as using a brushing or vibration protocol, a weighted vest, or deep
pressure to the joints) or pharmaceutical therapies (including any pharmaceutical agent
prescribed by a physician for the documented purpose of improving volume of oral intake)
applied singularly (clinical questions two and four) in a therapeutic environment on
functional feeding outcomes (i.e. volume of intake, variety of intake, days to wean tube
feeding, weight gain, or growth). This is not to imply that there is not clinical or
anecdotal evidence to support the use of these modalities to improve functional feeding
outcomes, but this EBSR establishes that the current level of evidence to support these
types of treatments applied singularly to treat pediatric feeding and/or swallowing
problems is phase I research (least robust level of evidence, see Table 6 for hierarchical levels of evidence) [81]. All of the quality features are summarized in Table 2 for each article included in this EBSR.
Clinical question one identified one published article that addressed the
effect of oral motor interventions on functional oral feeding outcomes in children. [13, 21].
Although it was designed as a randomized controlled trial it was underpowered and suffered
from significant loss of subjects to follow-up, making post treatment assessments
impossible for nine subjects (only 55% of the subjects had both pre and post treatment
analysis). As a result, the authors did not find significant differences between the
control and experimental groups on the outcomes of weight gain or change in oral motor
function and this study does not offer any direct support for oral motor therapy to
benefit functional oral feeding outcomes. Based on the results of this EBSR, oral motor
therapy applications are phase I research. Significant limitations of this study included
inadequately described study protocol, values neither reported nor calculable, and no effect sizes
or confidence intervals reported or calculable (see Table
2) [21].
Of the 37 articles that addressed clinical question three, the majority
(32/37) were determined to be phase one research reporting either 0/8 [27, 28, 37, 44],
1/8 [23, 24, 29, 30, 31, 36, 46,
48, 49, 55], 2/8 [26, 32, 33, 34,
35, 40, 41, 42, 43, 47, 51,
52, 54, 56, 57, 58], or 3/8 [50, 53]
quality indicators. Limitations of the articles determined to be phase one research
included small sample numbers (single subject or case controlled trials), with
inadequately described protocols (insufficient detail for replication), utilizing
convenience samples with inconsistently described evidence of treatment fidelity, and
inconsistent reports of significance precision (effect size). The five remaining articles
relevant to clinical question three were randomized controlled trials and determined to be
phase four research [22, 25, 38, 39, 45].
None of the randomized controlled trials provided 8/8 quality markers, please see Table 2 for complete summary of included features.
The 23 studies identified by this EBSR relevant to clinical question five
can be described as phase one research with all of them reporting two or less quality
markers (seven studies reported 0/8 quality markers [18, 60, 71, 76, 77, 78,
79], five reported only 1/8 quality
markers [59, 61, 62, 64, 75],
and 11 reported 2/8 quality markers [63, 65, 66,
67, 68, 69, 70, 72, 73, 74,
80]. Only three of the 23 articles relevant to
mixed modality interventions reported on the statistical significance of their
findings [63, 68, 73].
Discussion
This EBSR summarized the published evidence to support common treatment
modalities for children with feeding and/or swallowing disorders. The results bring to light
the lack of published evidence to support the singular use of oral motor interventions (one
of the 61 included articles) [21], sensory-based,
and pharmaceutical interventions (zero of the 61 included articles) to remediate pediatric
feeding and/or swallowing problems. Additionally, it highlights for the reader the moderate
amounts of published evidence to support the use of behavioral interventions (37 of the 61
included articles) [22, 23, 24, 25, 26,
27, 28, 29, 30, 31, 32, 33, 34, 35,
36, 37, 38, 39, 40, 41, 42, 43, 44,
45, 46, 47, 48, 49, 50, 51, 52, 53,
54, 55, 56, 57, 58], the use of mixed method
interventions (23 of the 61 included articles) [18, 59, 60, 61, 62, 63, 64, 65,
66, 67, 68, 69, 70, 71, 72, 73, 74,
75, 76, 77, 78, 79, 80] and the various levels of evidence available to support the use
of behavioral (32/27, 86% were found to be phase one research) and combined treatment
options (all phase one research with extensive methodological limitations [18, 59,
60, 61, 62, 63, 64, 65, 66, 67, 68,
69, 70, 71, 72, 73, 74, 75, 76, 77,
78, 79, 80]) for children with feeding and/or
swallowing disorders. The clinical utility of the findings from question one (oral motor
interventions) [21] and question five (mixed
method intervention strategies) [18, 59, 60,
61, 62, 63, 64, 65, 66, 67, 68, 69,
70, 71, 72, 73, 74, 75, 76, 77, 79,
80] is limited due to the limitations of the
methodologies employed in these studies and the primarily descriptive data reported. The
lack of scientific evidence available on the singular use of oral motor interventions,
sensory-based interventions, and pharmaceutical interventions does not allow clinicians to
draw any valid conclusions about the efficacy of these methods when applied for improving
functional feeding outcomes in pediatric populations. However, the moderate amount of
published, phase one evidence on mixed method interventions does call for further
investigation of these strategies with greater scientific rigor to establish the full
dimensions of the therapeutic effect and ultimately determine the internal and external
validity of these treatment options as an initial therapeutic effect has been
established.
From this EBSR, clinicians recognize the importance of behavioral therapy
techniques for remediating feeding disorders and must ensure that members of the
multidisciplinary team are trained in the appropriate application of the various behavioral
therapy techniques. Sixty of the 61 articles identified utilized behavioral therapy
techniques within the prescribed therapeutic plan and reported various levels of improvement
in functional feeding outcomes including increased dietary intake, variety, and reduction in
inappropriate mealtime behaviors [18, 22, 23,
24, 25, 26, 27, 28, 29, 30, 31, 32,
33, 34, 35, 36, 37, 38, 39, 40, 41,
42, 43, 44, 45, 46, 47, 48, 49, 50,
51, 52, 53, 54, 55, 56, 57, 58, 59,
60, 61, 62, 63, 64, 65, 66, 67, 68,
69, 70, 71, 72, 73, 80]. Five of the sixty identified articles that reported on
behavioral feeding therapy approaches were randomized controlled trials and met the criteria
of phase four evidence [22, 25, 38, 39, 45].
One study randomized young patients with cystic fibrosis to either a wait list
(control group) or a behavioral and nutrition intervention (experimental group) and found
that the combination of behavioral and nutrition intervention led to an increase in energy
intake as compared to wait list [45]. Two [22, 39] of
those five articles reported on a specific program (Hassle Free Mealtimes Triple P) of
behavioral parent training to remediate difficult mealtime behaviors in children and improve
parent variables related to those behaviors in otherwise healthy, typically developing
children [22, 39]. One utilized the full program [22]
and the other utilized an abbreviated version of the program [39]. Both reported significant improvements in mealtime behaviors
following treatment with the parent behavioral training program [22, 39].
The remaining two randomized controlled trials identified were designed to
compare the effectiveness of two different approaches one to wean children from tube
feedings [25] and the other to increase dietary
intake, variety, and decrease problematic mealtime behaviors [38]. Benoit and colleagues compared the effectiveness of
nutritional training with nutritional training with the added component of extinction and
found that the nutritional training with the extinction component was significantly more
effective in weaning the use of tube feeding dependency in children with a mean age of 17.2
months [25]. Marshall et al. compared the
effectiveness of systematic desensitization and operant conditioning approaches to improving
dietary intake, variety and decreasing problematic mealtime behaviors and found no
significant differences in any of the primary outcomes between participants in the two
groups [38]. Marshall and colleagues well
designed randomized controlled trial highlights that tenants of both behavioral approaches
(operant conditioning and systematic desensitization) were effective in significantly
improving dietary intake and variety, and reducing problematic mealtime behaviors when
administered to a protocol by reliably trained professionals [38].
Across all of the studies, methodologies for evaluating the treatment modality
in question were inconsistent and there was wide variability among patient populations
studied (including children with ASD, medically and non-medically complex histories, genetic
syndromes, etc.…) which in combination with the relatively small numbers of subjects
enrolled in the majority of the studies included in this review, limits the generalizability
of the results to broad clinical populations. Clinicians are aware that there are three
tenants to evidence based practice: external scientific evidence, clinical
expertise/opinion, and client/patient/caregiver perspectives and desires. Whenever possible,
clinical care should be based on the best available evidence, but when there is insufficient
quantity and/or quality of evidence available in the literature, clinicians must determine
what is best practice based on the limited available evidence, clinical opinion, and the
needs/desires of their patients and their families. Further, clinicians must focus on
functional feeding outcomes for their clients, document client progress, and adjust
treatment modalities used to fit the individual needs of each client.
Limitations of the current EBSR included the inclusion criteria of exclusively
peer-reviewed literature published only in English. This design feature may have contributed
to a publication bias in this EBSR. Due to the limited resources available for this EBSR,
limiting inclusion to only articles published in English was a necessity; however, the
authors acknowledge that this may have introduced bias and ultimately limited the number of
articles identified. Additionally, reliability of reviewers could not be determined, but the
three reviewers independently reviewed all of the articles before inclusion and then used
discussion and consensus to resolve any discrepenancies.
Conclusion
This EBSR contributes to clinicians’ knowledge of the published literature on
the use of various treatment modalities available to treat pediatric feeding and swallowing
disorders including oral motor, sensory, behavioral, pharmaceutical, and mixed method
intervention strategies. It is yet to be established whether or not oral motor, sensory, or
pharmaceutical interventions applied singularly or in combination can be used to
successfully aid in achieving functional feeding outcomes for pediatric patients. There is
phase four research from randomized controlled trials that establishes the following:
A program that incorporates behavioral and nutrition intervention for young
children with cystic fibrosis leads to greater increases in energy intake as compared to
usual care [45].
Parent-training programs are successful in reducing problematic feeding
behaviors in otherwise healthy and typically developing children [22, 39].
Nutritional intervention in combination with behavioral therapy (extinction
technique) is more effective in weaning young children from tube feeding dependency than
nutritional intervention alone [25].
Both systematic desensitization and operant conditioning behavioral therapy
approaches are effective in improving dietary intake, variety, and decreasing problematic
mealtime behaviors in children with ASD and those with non-medically complex histories when
administered to a protocol by trained professionals [38].
Funding
There was no funding source for this study.
Footnotes
Acknowledgments
The authors acknowledge the technical contributions of Kayla C. Mizell, Madison Hatchett,
and Jill Rogers and thank them for their assistance with this project.
Conflict of interest
The authors declare there are no financial or non-financial conflicts of interest.
References
1.
TutorJD, GosaMM.
Dysphagia and aspiration in children.
Pediatric pulmonology. 2012;
47(4): 321-337.
2.
ArvedsonJC.
Evaluation of children with feeding and swallowing
problems. Language, Speech and Hearing Services in
Schools. 2000; 31(1):
28-41.
3.
ArvedsonJC.
Assessment of pediatric dysphagia and feeding disorders: clinical and
instrumental approaches. Developmental disabilities
research reviews. 2008;
14(2): 118-127.
4.
RudolphCD, LinkDT.
Feeding disorders in infants and children.
Pediatric clinics of North America.
2002; 49(1):
97-112, vi.
5.
ArvedsonJ.
Treatment Efficacy Summary on Pediatric Feeding and Swallowing
Disorders. Rockville, MD2008.
6.
ArvedsonJC.
Management of pediatric dysphagia.
Otolaryngologic clinics of North America.
1998; 31(3):
453-476.
7.
Lefton-GreifMA.
Diagnosis and management of pediatric feeding and swallowing disorders:
Role of the speech-language pathologist. In: Tuchman DN, Walter RS, eds.
Disorders of feeding and swallowing in infants and
children. 1 ed. San Diego: Singular Publishing Group;
1994: 97-113.
8.
AssociationAP.
Diagnostic and Statistical Manual of Mental Disorders:
DSM-5. ManMag; 2003.
FishbeinM, CoxS,
SwennyC, MogrenC, WalbertL, FrakerC. Food
chaining: a systematic approach for the treatment of children with feeding
aversion. Nutrition in clinical practice: official
publication of the American Society for Parenteral and Enteral
Nutrition. 2006; 21(2):
182-184.
11.
BoydKL. The
effectiveness of the Sequential Oral Sensory Approach group feeding
program. Colorado School of Professional Psychology;
2007.
12.
ArvedsonJ, ClarkH,
LazarusC, SchoolingT, FrymarkT.
Evidence-based systematic review: effects of oral motor interventions on
feeding and swallowing in preterm infants. American
journal of speech-language pathology/American Speech-Language-Hearing
Association. 2010;
19(4): 321-340.
13.
ArvedsonJ, ClarkH,
LazarusC, SchoolingT, FrymarkT.
The effects of oral-motor exercises on swallowing in children: an
evidence-based systematic review. Developmental Medicine
& Child Neurology. 2010;
52(11): 1000-1013.
14.
AngellA.
Selective eaters and tactile sensitivity: A review of classification and
treatment methods that address anxiety and support a child’s need for a sense of
control. ICAN: Infant, Child, & Adolescent
Nutrition. 2010; 2(5):
299-303.
15.
DavisAM, BruceA,
CocjinJ, MousaH,
HymanP.
Empirically supported treatments for feeding difficulties in young
children. Current gastroenterology
reports. 2010; 12(3):
189-194.
16.
DonnellanP.
Sensory integration therapy. Kids with
Tubes News. 2001: 2-3.
DavisAM, BruceA,
CocjinJ, MousaH,
HymanP.
Empirically supported treatments for feeding difficulties in young
children. Current Gastroenterology
Reports. 2010; 12(3):
189-194.
19.
GosaM, SchoolingT, ColemanJ.
Thickened liquids as a treatment for children with dysphagia and
associated adverse effects: A systematic review. ICAN:
Infant, Child, & Adolescent Nutrition. 2011:
1941406411407664.
20.
CherneyLR, PattersonJP, RaymerA, FrymarkT, SchoolingT.
Evidence-based systematic review: Effects of intensity of treatment and
constraint-induced language therapy for individuals with stroke-induced
aphasia. Journal of Speech, Language, and Hearing
Research. 2008; 51(5):
1282-1299.
21.
OttenbacherK,
ScogginsA, WaylandJ.
The effectiveness of a program of oral sensory-motor therapy with the
severely and profoundly developmentally disabled. OTJR:
Occupation, Participation and Health. 1981;
1(2): 147-160.
22.
AdamsonM, MorawskaA, SandersMR.
Childhood feeding difficulties: A randomized controlled trial of a
group-based parenting intervention. Journal of
Developmental & Behavioral Pediatrics. 2013;
34(5): 293-302.
23.
BachmeyerMH, PiazzaCC, FredrickLD, ReedGK,
RivasKD, KadeyHJ.
Functional analysis and treatment of multiply controlled inappropriate
mealtime behavior. Journal of Applied Behavior
Analysis. 2009; 42(3):
641-658.
24.
BandstraNF, CristWB, Napier-PhillipsA,
FlowerdewG.
The impact of behavioral feeding intervention on health care
utilization. Children’s Health Care.
2011; 40(4):
282-296.
25.
BenoitD, WangEE,
ZlotkinSH.
Discontinuation of enterostomy tube feeding by behavioral treatment in
early childhood: A randomized controlled trial. The
Journal of pediatrics. 2000;
137(4): 498-503.
26.
BinnendykL, LucyshynJM.
A family-centered positive behavior support approach to the amelioration
of food refusal behavior: An empirical case study.
Journal of Positive Behavior Interventions.
2008; 11(1):
47-62.
27.
BlissettJ, HarrisG. A
behavioural intervention in a child with feeding problems.
Journal of Human Nutrition and Dietetics : The official journal of the
British Dietetic Association. 2002;
15(4): 255-260.
28.
de
MoorJ, DiddenR, KorziliusH.
Behavioural treatment of severe food refusal in five toddlers with
developmental disabilities. Child Care Health
Dev. 2007; 33(6):
670-676.
29.
DoveyTM, MartinCI. A
quantitative psychometric evaluation of an intervention for poor dietary variety in
children with a feeding problem of clinical significance.
Infant Mental Health Journal. 2012;
33(2): 148-162.
30.
GaleCM, EikesethS, RudrudE.
Functional assessment and behavioural intervention for eating
difficulties in children with autism: A study conducted in the natural environment using
parents and ABA tutors as therapists. Journal of Autism
and Developmental Disorders. 2011;
41(10): 1383-1396.
31.
GreerRD, DorowL,
WilliamsG, McCorkleN, AsnesR.
Peer-mediated procedures to induce swallowing and food acceptance in
young children. Journal of Applied Behavior
Analysis. 1991; 24(4):
783-790.
32.
GroffRA, PiazzaCC, VolkertVM, JostadCM.
Syringe fading as treatment for feeding refusal.
Journal of Applied Behavior Analysis.
2014; 47(4):
834-839.
33.
GroffRA, PiazzaCC, ZelenyJR, DempseyJR.
Spoon-to-cup fading as treatment for cup drinking in a child with
intestinal failure. Journal of Applied Behavior
Analysis. 2011; 44(4):
949-954.
34.
JohnsonCR, FoldesE, DeMandA, BrooksMM.
Behavioral parent training to address feeding problems in children with
autism spectrum disorder: A pilot trial. Journal of
Developmental and Physical Disabilities. 2015;
27(5): 591-607.
35.
LaRueRH, StewartV, PiazzaCC, VolkertVM, PatelMR, ZelenyJ.
Escape as reinforcement and escape extinction in the treatment of feeding
problems. Journal of Applied Behavior
Analysis. 2011; 44(4):
719-735.
36.
LuiselliJK.
Cueing, demand fading, and positive reinforcement to establish
self-feeding and oral consumption in a child with chronic food refusal.
Behavior Modification. 2000;
24(3): 348-358.
37.
LuiselliJK, LuiselliTE.
A behavior analysis approach toward chronic food refusal in children with
gastrostomy-tube dependency. Topics in Early Childhood
Special Education. 1995;
15(1): 1-18.
38.
MarshallJ, HillRJ,
WareRS, ZivianiJ, DodrillP.
Multidisciplinary intervention for childhood feeding
difficulties. Journal of Pediatric Gastroenterology and
Nutrition. 2015; 60(5):
680-687.
39.
MorawskaA, AdamsonM, HinchliffeK, AdamsT.
Hassle Free Mealtimes Triple P: A randomised controlled trial of a brief
parenting group for childhood mealtime difficulties.
Behaviour Research and Therapy. 2014;
53: 1-9.
40.
NajdowskiAC, WallaceMD, DoneyJK, GhezziPM.
Parental assessment and treatment of food selectivity in natural
settings. Journal of Applied Behavior
Analysis. 2003; 36(3):
383-386.
41.
Opipari-ArriganL,
PowersSW, QuittnerAL, StarkLJ.
Mealtime problems predict outcome in clinical trial to improve nutrition
in children with CF. Pediatric
Pulmonology. 2010; 45(1):
78-82.
42.
PatelMR, PiazzaCC, MartinezCJ, VolkertVM, ChristineMS.
An evaluation of two differential reinforcement procedures with escape
extinction to treat food refusal. Journal of Applied
Behavior Analysis. 2002;
35(4): 363.
43.
PenrodB, VanDalenKH.
An evaluation of emerging preference for non-preferred foods targeted in
the treatment of food selectivity. Behavioral
Interventions. 2010;
25(3): 239-251.
44.
PizzoB, WilliamsKE, PaulC,
RiegelK.
Jump start exit criterion: Exploring a new model of service delivery for
the treatment of childhood feeding problems. Behavioral
Interventions. 2009;
24(3): 195-203.
45.
PowersSW, JonesJS, FergusonKS, Piazza-WaggonerC,
DainesC, ActonJD.
Randomized clinical trial of behavioral and nutrition treatment to
improve energy intake and growth in toddlers and preschoolers with cystic
fibrosis. Pediatrics.
2005; 116(6):
1442-1450.
46.
RivasKD, PiazzaCC, PatelMR, BachmeyerMH.
Spoon distance fading with and without escape extinction as treatment for
food refusal. Journal of Applied Behavior
Analysis. 2010; 43(4):
673-683.
47.
RivasKM, PiazzaCC, RoaneHS, et al.
Analysis of self-feeding in children with feeding
disorders. Journal of Applied Behavior
Analysis. 2014; 47(4):
710-722.
48.
SchädlerG, Süss-BurghartH,
ToschkeAM, Von
VossH, Von
KriesR. Feeding
disorders in ex-prematures: Causes-response to therapy-long term
outcome. European Journal of Pediatrics.
2007; 166(8):
803-808.
49.
SeiverlingL, WilliamsK, SturmeyP, HartS.
Effects of behavioral skills training on parental treatment of children’s
food selectivity. Journal of Applied Behavior
Analysis. 2012; 45(1):
197-203.
50.
SharpWG, BurrellTL, JaquessDL.
The Autism MEAL Plan: A parent-training curriculum to manage eating
aversions and low intake among children with autism.
Autism. 2013: 1362361313489190.
51.
SharpWG, JaquessDL, MortonJF, MilesAG. A
retrospective chart review of dietary diversity and feeding behavior of children with
autism spectrum disorder before and after admission to a day-treatment
program. Focus on Autism and Other Developmental
Disabilities. 2011;
26(1): 37-48.
52.
StarkLJ, KnappLG, BowenAM, et al.
Increasing calorie consumption in children with cystic fibrosis:
replication with 2-year follow-up. Journal of Applied
Behavior Analysis. 1993;
26(4): 435.
53.
StarkLJ, MulvihillMM, PowersSW, et al.
Behavioral intervention to improve calorie intake of children with cystic
fibrosis: treatment versus wait list control. Journal of
Pediatric Gastroenterology and Nutrition. 1996;
22(3): 240-253.
54.
TarboxJ, SchiffA, NajdowskiAC.
Parent-implemented procedural modification of escape extinction in the
treatment of food selectivity in a young child with autism.
Education and Treatment of Children.
2010; 33(2):
223-234.
55.
VazP, VolkertVM, PiazzaCC.
Using negative reinforcement to increase self-feeding in a child with
food selectivity. Journal of Applied Behavior
Analysis. 2011; 44(4):
915-920.
56.
VolkertVM, PetersonKM, ZelenyJR, PiazzaCC. A
clinical protocol to increase chewing and assess mastication in children with feeding
disorders. Behavior Modification.
2014: 0145445514536575.
57.
WilkinsJW, PiazzaCC, GroffRA, VazP.
Chin prompt plus re-presentation as treatment for expulsion in children
with feeding disorders. Journal of Applied Behavior
Analysis. 2011; 44(3):
513-522.
58.
WilkinsJW, PiazzaCC, GroffRA, VolkertVM, KozisekJM, MilnesSM.
Utensil manipulation during initial treatment of pediatric feeding
problems. Journal of Applied Behavior
Analysis. 2014; 47(4):
694-709.
59.
AddisonLR, PiazzaCC, PatelMR, et al.
A comparison of sensory integrative and behavioral therapies as treatment
for pediatric feeding disorders. Journal of Applied
Behavior Analysis. 2012;
45(3): 455-471.
60.
Berger-GrossP,
ColettiDJ, HirschkornK, TerranovaE, SimpserEF.
The effectiveness of risperidone in the treatment of three children with
feeding disorders. Journal of Child & Adolescent
Psychopharmacology. 2004;
14(4): 621-627.
61.
ClawsonE, PalinskiK, ElliottC.
Outcome of intensive oral motor and behavioural interventions for feeding
difficulties in three children with Goldenhar Syndrome.
Developmental Neurorehabilitation.
2006; 9(1):
65-75.
62.
ClawsonEP, KuchinskiKS, BachR.
Use of behavioral interventions and parent education to address feeding
difficulties in young children with spastic diplegic cerebral palsy.
NeuroRehabilitation. 2007;
22(5): 397-406.
63.
DouglasJ, HarrisB.
Description and evaluation of a day-centre-based behavioural feeding
programme for young children and their parents. Clinical
Child Psychology and Psychiatry. 2001;
6(2): 241-256.
64.
EckmanN, WilliamsKE, RiegelK, PaulC.
Teaching chewing: A structured approach.
American Journal of Occupational Therapy.
2008; 62(5):
514-521.
65.
GibbonsBG, WilliamsKE, RiegelKE.
Reducing tube feeds and tongue thrust: Combining an oral-motor and
behavioral approach to feeding. American Journal of
Occupational Therapy. 2007;
61(4): 384.
66.
GirolamiPA, BoscoeJH, RoscoeN.
Decreasing expulsions by a child with a feeding disorder: Using a brush
to present and re-present food. Journal of Applied
Behavior Analysis. 2007;
40(4): 749.
67.
HardingC, FaimanA, WrightJ.
Evaluation of an intensive desensitisation, oral tolerance therapy and
hunger provocation program for children who have had prolonged periods of tube
feeds. International Journal of Evidence-Based
Healthcare. 2010; 8(4):
268-276.
68.
LaudRB, GirolamiPA, BoscoeJH, GulottaCS.
Treatment outcomes for severe feeding problems in children with autism
spectrum disorder. Behavior
Modification. 2009.
69.
LevinDS, VolkertVM, PiazzaCC. A
Multi-Component Treatment to Reduce Packing in Children With Feeding and Autism Spectrum
Disorders. Behavior Modification.
2014; 38(6):
940-963.
70.
LuiselliJK, GleasonDJ.
Combining sensory reinforcement and texture fading procedures to overcome
chronic food refusal. Journal of Behavior Therapy and
Experimental Psychiatry. 1987;
18(2): 149-155.
71.
McKirdyLS, SheppardJJ, OsborneML, PayneP.
Transition from tube to oral feeding in the school
setting. Language, Speech, and Hearing Services in
Schools. 2008; 39(2):
249-260.
72.
PenrodB, GardellaL, FernandJ. An
evaluation of a progressive high-probability instructional sequence combined with
low-probability demand fading in the treatment of food selectivity.
Journal of Applied Behavior Analysis.
2012; 45(3):
527-537.
73.
QvarfordtI, EngerströmIW, EliassonA-C.
Guided eating or feeding: Three girls with Rett syndrome.
Scandinavian Journal of Occupational Therapy.
2009; 16(1):
33-39.
74.
SharpWG, HarkerS, JaquessDL.
Comparison of bite-presentation methods in the treatment of food
refusal. Journal of Applied Behavior
Analysis. 2010; 43(4):
739-743.
75.
SharpWG, OdomA,
JaquessDL.
Comparison of upright and flipped spoon presentations to guide treatment
of food refusal. Journal of Applied Behavior
Analysis. 2012; 45(1):
83-96.
76.
ShawRJ, GarciaM, ThornM,
FarleyCA, FlanaganG.
Treatment of feeding disorders in children with Down
syndrome. Clinical Child Psychology and
Psychiatry. 2003; 8(1):
105-117.
77.
SheppardJJ.
Using motor learning approaches for treating swallowing and feeding
disorders: A review. Language, Speech, and Hearing
Services in Schools. 2008;
39(2): 227-236.
78.
SuarezMA.
Multicomponent treatment for food selectivity in children Description and
Case Report. Nutrition in Clinical
Practice. 2014: 0884533614553638.
79.
TrabiT, Dunitz-ScheerM,
KratkyE, BeckenbachH, ScheerPJ.
Inpatient tube weaning in children with long-term feeding tube
dependency: A retrospective analysis. Infant Mental
Health Journal. 2010;
31(6): 664-681.
80.
VazP, PiazzaCC, StewartV, VolkertVM, GroffRA, PatelMR. Using
a chaser to decrease packing in children with feeding disorders.
Journal of Applied Behavior Analysis.
2012; 45(1):
97-105.
81.
RobeyRR. A
five-phase model for clinical-outcome research. Journal
of Communication Disorders. 2004;
37(5): 401-411.