
Abstract
PURPOSE:
This study examined whether certain medical complications influence the feasibility of tube removal.
METHODS:
42 subjects with dysphagia who were under the age of 2.5 years were nourished entirely through feeding tubes. Additionally, they were judged to have no aspiration. The following data about the infants were collected through a retroactive survey: age at which oral feeding training commenced, gender, and whether certain medical complications (cardiovascular, respiratory, digestive, neurological, or oral) had been present at birth. The data were analyzed to determine which type of medical complication affected the likelihood of removing the feeding tube from the infant at 3 years of age.
RESULTS:
Of the five medical complications examined, cardiovascular complications significantly affected the feasibility of tube removal (p = 0.049).
CONCLUSION:
Pediatric dysphagia patients with cardiac complications, compared to those with other complications, may take longer to transition off tube feeding.
Introduction
Medical advances have led to better neonatal survival rates. Infants increasingly survive diseases that they would have died from in the past; consequently, there are growing numbers of infants with severe dysphagia, as a sequela of such diseases [1, 2]. To meet the needs of the parents, medical teams aim for an infant’s transition to full oral feeding; however, dysphagia can make this transition problematic, and the infant might need to remain on tube feeding indefinitely. Tube feeding helps ensure that an infant is properly nourished; however, it also entails certain disadvantages. For example, the tube constrains the infant’s activities, and it imposes a physical and mental burden on the parents. It is also disadvantageous for the healthcare providers, as it necessitates having a larger number of staff on hand to maintain the tube feeding and increases medical costs. Thus, both parties (the receivers and providers of healthcare) have an interest in removing the tube.
Illingworth and Lister and Mann et al. highlighted aspiration as a predictor of the feasibility of removing a feeding tube [3, 4]. Clinical practice confirms this to be the case; when the infant is diagnosed with aspiration, the medical team will often decide to maintain tube feeding for medical reasons—that is, because oral feeding would incur the risk of aspiration pneumonia. However, even when aspiration is absent and the medical team deems it medically feasible to attempt the transition to oral feeding, the transition is not necessarily straightforward [5]. If the infant is reluctant to feed orally, for example, it might prove difficult to increase the amount of oral feeding to the point at which the tube can be removed. Thus, in order to meet the needs of parents when proceeding toward tube removal, it is necessary to consider factors other than aspiration that may influence the amount of oral feeding an infant can accept.
One such factor is the total number of medical complications [6]. Bazyk reported that a higher number of medical complications (including respiratory, digestive, neurological, and cardiac) correlates with a longer transition to oral feeding, suggesting that a number of complications predicts the prospect of tube removal [6]. However, little is known about how specific medical complications impact oral feeding progress. Accordingly, using data on infants with dysphagia who were seen as outpatients at the Division for Oral-Facial Disorders, Osaka University Dental Hospital, the present study examined the relationship between different medical complications and the feasibility of tube removal.
Methods
Subjects
The study subjects were dysphagia patients under the age of 30 months (2.5 years) who received outpatient care at the Division for Oral-Facial Disorders between January 2011 and March 2019. This study was conducted on 49 infants who, at the time of the initial medical examination, were not orally feeding at all (i.e., they were being nourished entirely through feeding tubes). All 49 were being nourished nasogastrically, and none had a gastric fistula. The parents provided informed consent, and the study was approved by the ethics committee of Osaka University’s Graduate School of Dentistry (No. H28-E18). Among 49 subjects, 7 were excluded from the study because they had been diagnosed with aspiration upon an endoscopic or videofluoroscopic swallowing test during the initial medical examination.
Survey method
The infants’ diagnostic records were examined to gather the following data: the age at which the infant commenced oral feeding training, the infant’s gender, and whether certain medical complications were present in the infant at birth. From the initial examination until age 3, each infant received the necessary care to facilitate their transition to oral feeding, including oral massage (within and around the oral cavity), positioning into a suitable oral feeding posture, and diet modification. The infants were then divided into two groups depending on the outcome of this treatment: whether the nasogastric tube could be removed (“removal-feasible” cases) or whether it remained unfeasible to remove the tube (“removal-unfeasible” cases). The authors then analyzed how each type of medical complication had affected the feasibility of tube removal at the time the infants reached 3 years of age.
Five types of medical complications were examined: cardiovascular, respiratory, digestive, neurological, and oral. According to the literature, these complications affect the amount of oral feeding the infant accepts [6]. The categorization of these medical complications accorded with Harrison’s Principles of Internal Medicine (19th ed.) [7]. The medical complications were only deemed applicable if the principal doctor determined, during the first examination, that the infant required regular examinations and/or treatment (e.g., if the physician recommended drug therapy or postoperative observation, or if the physician determined that the patient required no treatment but did require observation care). They were not deemed applicable if the infants made a complete recovery such that no more examination was required. All the infants in the study were capable of nourishment only through nasogastric feeding; although some had digestive complications, none had any dysfunction in the small or large intestine.
Statistical analysis
The two groups (removal-feasible and removal-unfeasible) were compared in terms of age of training commencement (using the Mann-Whitney U test) and gender (using the chi-squared test). The variables of removal feasibility were subjected to a univariate analysis (2-class logistic regression). All statistics were computed using IBM’s SPSS for Windows software, version 23 (IBM, 2015) with the statistical threshold set at 5%.
Results
Table 1 shows the breakdown for each of type of complication (cardiovascular, respiratory, digestive, neurological, and oral). As Table 2 indicates, following the interventions begun at the time of the initial examination, 20 of the 42 infants transitioned from tube to oral feeding by the time they were 3 years old (removal-feasible), while 22 did not (removal-unfeasible).
Breakdown of Complicationsa (n)
Breakdown of Complicationsa (n)
aSome infants had multiple complications.
Subjects’ Attributes
Table 2 and Fig. 1 present an intergroup comparison (removal-feasible vs. removal-unfeasible) of age of training commencement, gender, and medical complication status (present or absent). In the removal-feasible group, the average age of training commencement was 4.4 (±7.0) months. Half (10 out of 20 patients) commenced training at birth, and the oldest age was two years. In the removal-unfeasible group, the average age of training commencement was 5.5 (±7.3) months. The majority (17 out of 22 patients) commenced training between birth and six months, and the oldest age was two years. There was no significant intergroup difference in age of training commencement, although those in the removal-unfeasible group tended to commence training later (p = 0.29, Fig. 1). There was no significant intergroup difference in gender (p = 0.71).
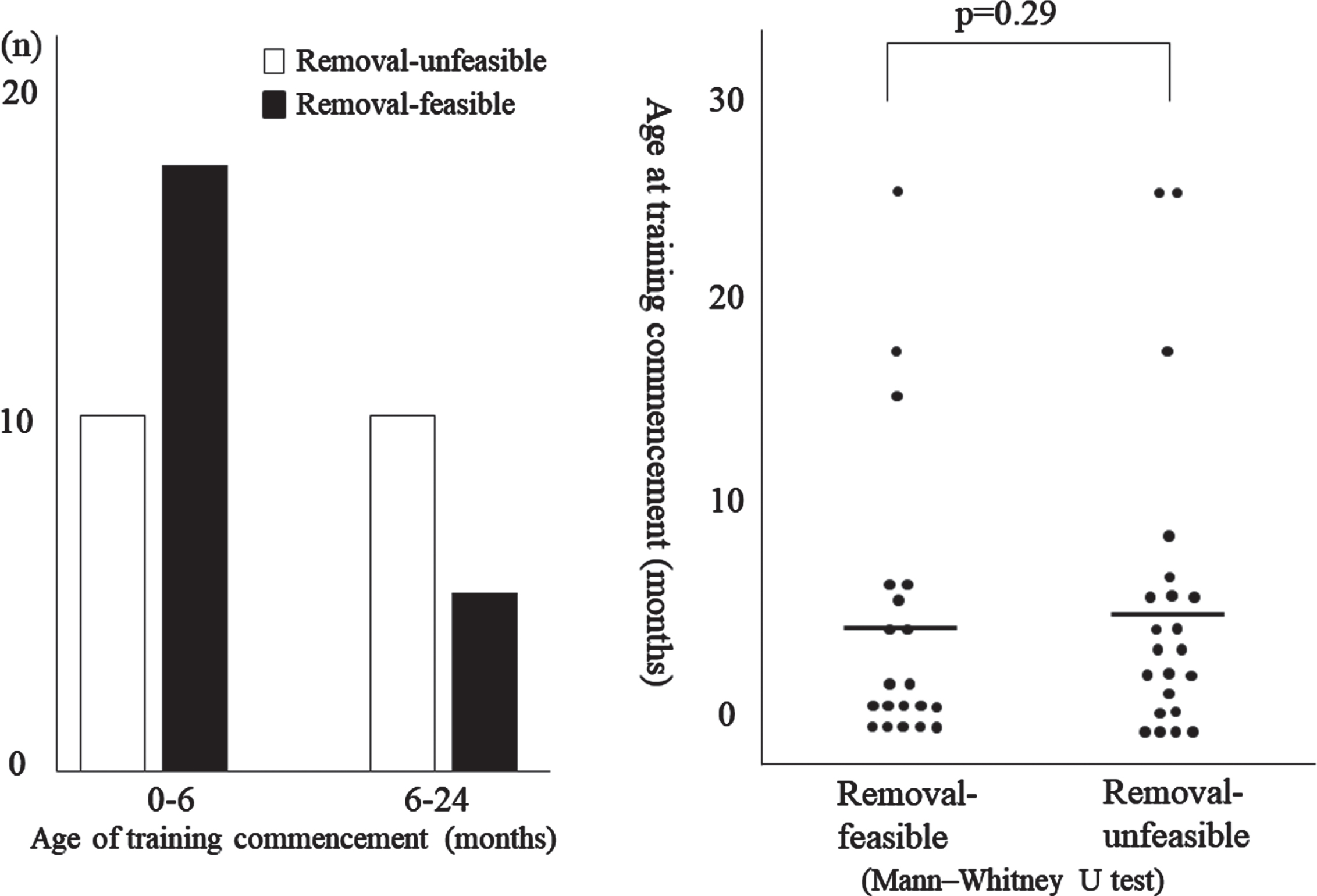
Comparison between groups (Age of training commencement).
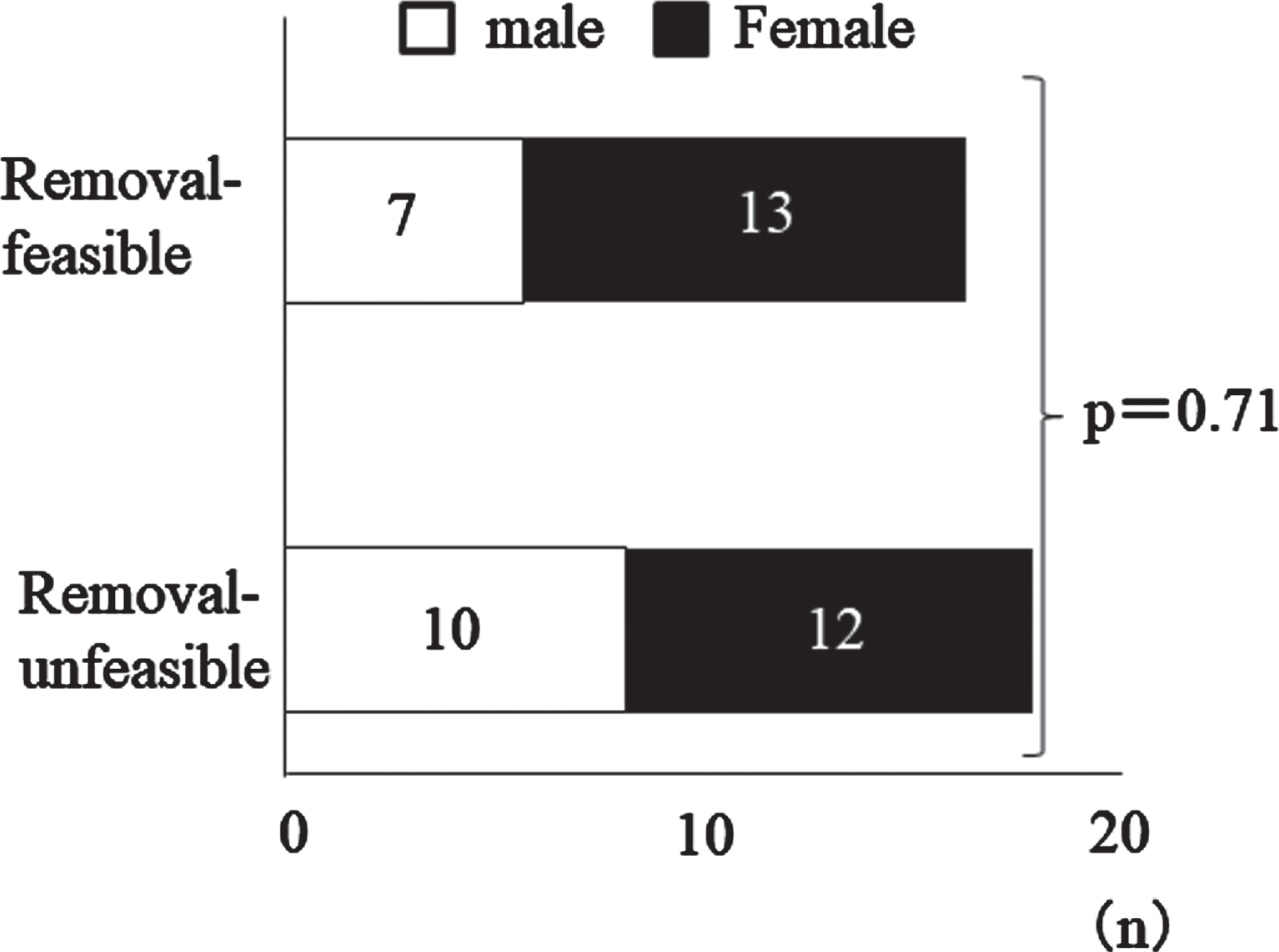
Comparison between groups (gender composition) the chi-squared test.
The data were subjected to a univariate analysis in which the objective variable was the feasibility of removing the nasogastric tube by age 3. The explanatory variables were the statuses (present or absent) of each complication type (cardiovascular, respiratory, digestive, neurological, and oral). The results of the analysis indicated that cardiovascular complications have a significant negative correlation with removal feasibility (p = 0.049). The statuses of other complications types were not found to be significantly related (see Table 3).
Complication Type and Nasogastric Tube-removal Feasibility
Complication Type and Nasogastric Tube-removal Feasibility
OR = odds ratio.
When determining whether an infant with dysphagia should commence oral feeding, it is essential to check for aspiration. The presence of aspiration increases the risk of aspiration pneumonia and thus makes it necessary to control oral intake by continuing tube feeding. If aspiration is absent, there is no need for such control, and the medical team can aim for full oral intake, allowing the infant to ingest the desired amount. In practice, however, even when aspiration is absent, it may nonetheless be necessary to administer adequate nourishment by a feeding tube owing to issues such as the patient refusing to feed orally.
Other issues can interfere. For example, after analyzing the data on 83 infants who underwent surgery due to congenital heart disease in their first 15 days of life, Kogon et al. reported that 45% of them had a lengthy transition from nasogastric to oral feeding [8]. In another report on infants with congenital heart disease, Vogel found that the transition from nasogastric to oral feeding can be problematic even when swallowing training is provided [9]. Similar findings have been reported concerning infants with respiratory [10, 11] and digestive complications [12, 13], suggesting that infants with these complications sometimes struggle to progress to oral nourishment. Although the above studies indicate that these medical complications increase the risk of a prolonged transition, they do not clarify whether the complications were comorbid with other conditions. One study reported on the relationship between the total number of medical complications and length of transition to oral feeding, but it did not specify the effects of specific types of complications on the outcome. Accordingly, the present study examined which types of medical complications affected the rate of oral feeding readiness, as measured by the feasibility of removing the feeding tube [6].
Intergroup comparison
Age of training commencement
Around half of the removal-feasible group commenced oral feeding training at birth, while around 70% in the removal-unfeasible group started it later, though the difference was not statistically significant. Lyu et al. reported that early commencement of oral stimulation and oral feeding increased the rate of full oral feeding (defined as the point when the nasogastric tube was removed), while delayed intervention resulted in a poorer rate [14]. Ishizaki et al. concluded that children referred for tube weaning after 3 years of age had a markedly longer treatment time than younger children [15]. Similarly, Wright et al. identified that slow or failed weaning often occurs in children 5 years and older [16].
Age of training commencement and continuation of training after intervention are sometimes delayed when the infant has severe complications for which treatment must be prioritized over oral stimulation and oral feeding; it is likely that the removal-unfeasible group included a relatively large number of infants with such complications. Thus, among cases in which the transition to oral feeding is deemed feasible early on and in which it would be desirable to effect such a transition through early intervention, the transition may nonetheless be lengthy if the infant has complications that inhibit an immediate or early transition to oral feeding.
Relationship between medical complications and feasibility of tube removal
Respiratory complications
The present study did not find respiratory complications to be a significant predictor of tube weaning feasibility. In contrast, Harris and Van Wezel-Meijler et al. reported that respiratory complications significantly predicted the outcome [10, 11]. According to Harris and Morris et al., infants with respiratory complications are prone to aspiration because they have an abnormal suck-swallow-breathe pattern, which makes it harder to increase the amount of oral feeding [10, 12]. Similarly, Smith et al. and Thoyre et al. reported that an increase in respiratory effort can interrupt the sequential nature of the swallowing process and lead to aspiration risk [17, 18].
Van Wezel-Meijler et al. suggested that the inclusion of aspiration in the category of respiration complications explains why the latter was associated with delayed oral feeding [11]. The present study, on the other hand, excluded aspiration cases (as identified by endoscopic or videofluoroscopic swallowing examination), and this might explain why respiration complications did not appear to affect the feasibility of tube weaning. In addition, Chang et al. reported that the use of thickeners may enable an infant to learn to develop a successful suck-swallow-breathe sequence [19]. In the present study, infants with respiratory complications might have moved to oral feeding without causing any problems such as aspiration since the appropriate thickness for their oral and swallowing functions was recommended.
Digestive complications
The results of the present study did not find digestive complications to be a significant predictor of tube weaning feasibility. However, other studies have found connections between gastroesophageal reflux, vomiting, and other digestive complications and problematic transition to oral feeding [12, 21]. Hyman and Rommel et al. reported that infants frequently refuse food due to unpleasant experiences involving heartburn or pain with swallowing (odynophagia) resulting from gastroesophageal reflux [21, 22].
On the other hand, Lee et al. reported that infants diagnosed with gastroesophageal reflux were treated with standard medical therapy [23]. Sixty-six per cent were able to discontinue medication within 12 months and remained well. Few children (6%) required a Nissen fundoplication for failure to respond to medical therapy. Most infants with gastroesophageal reflux disease (GERD) have an uncomplicated course. False-negative results were noted in both pH monitoring and barium meal. Up to 80% of children will improve within 12 months with therapy. In addition, Rommel et al. reported that some infants with GERD show spontaneous improvement as they grow. Indeed, in the present study, the amount of oral feeding increased in some cases following a reduction in the frequency of gastroesophageal reflux and vomiting [22]. Thus, although some of the infants had gastroesophageal reflux (as identified during the first examination) that made it difficult to increase the amount of oral feeding, improvements in their reflux symptoms over time would mean that this factor did not ultimately affect nasogastric tube removal feasibility by the time they reached 3 years of age.
Cardiovascular complications
The results of this study indicated that cardiovascular complications significantly affected the feasibility of tube removal. This finding is consistent with two existing studies that found that infants with heart disease have lengthy transitions from nasogastric to oral feeding [24, 25]. According to these studies, such infants are prone to exhaustion during the breastfeeding process, which forces them to stop the swallowing action to catch their breath, and that they struggle to coordinate the swallow-breathe sequence. In another study involving infants with heart disease, Hartman et al. found that some infants presented digestive conditions with symptoms such as vomiting and nausea [26]. According to the reports of Morris et al. and Ferry et al., digestive problems may lead to a loss of appetite due to unpleasant postprandial experiences such as vomiting and gastroesophageal reflux [12, 20]. Of the cardiovascular cases analyzed in the present study, four infants exhibited repeat instances of vomiting and gastroesophageal reflux for unknown reasons. Despite the absence of any functional issues, these four infants lacked appetite and refused oral feeding, which inhibited their progress. In addition, Wolf et al. described decreased endurance, early satiety, and poor growth in infants with congenital heart disease [27]. Cardiac patients are at the mercy of their physiologic status since all of their resources are focused on survival. In this state, the slightest increase in stimuli may be overwhelming. Thus, medical professionals should bear in mind that cardiovascular complications will render tube removal more problematic than it would otherwise be.
Summary
Parents may believe that if their infants show no sign of aspiration, they will have an uncomplicated oral feeding readiness. Therefore, parents may experience mounting frustration when the transition proves to be more complicated than they expected. In this respect, parents, as well as medical teams, would benefit from the ability to predict the feasibility of tube removal and the length of the transition. The results of the present study indicated that the transition from nasogastric feeding was more problematic for infants with cardiovascular complications than for other infants. This finding implies that the parents of such infants should be briefed in advance about the potential difficulties. Medical teams should advise these parents to proceed with oral feeding but also consider other means of nourishment, including gastric feeding.
The results of this study imply that respiration complications do not inhibit the transition from tube feeding provided that the symptoms do not lead to an increase in aspiration frequency.
Provided that symptoms such as gastroesophageal reflux and vomiting ease, the results of this study suggest that infants with digestive complications will proceed smoothly to oral feeding and have a reasonable prospect of coming off tube feeding.
Study limitations
Although this study examined which types of medical complications affect infants’ transition from tube feeding, as a retrospective study, it was unable to examine or account for differing severity levels of each disease. Additionally, many of the subjects had multiple medical complications, and the study did not examine differences between subjects with a single complication and those with multiple complications. Thus, further research with larger samples is required. Also, this study was conducted at a hospital specializing in patients with dental-related complaints, specifically infant patients with oral-facial disorders. Further research of infant patients in general hospitals might yield different findings.
Factors influencing the transition to oral feeding include medical complications, oral dysfunction [28, 29], low appetite [30], low birth weight [22], and preterm delivery as well as the presence or absence of appropriate training [31]. There are cases in which it is difficult to wean from tube feeding due to the complex intertwining of these factors; therefore, it is necessary to understand the trends of each medical complication and consider them in relation to other factors.
Conclusion
This study analyzed infants diagnosed with dysphagia at the Osaka University Dental Hospital to determine the types of medical complications that affect the feasibility of removing a feeding tube by the time the infant reached three years old. The study revealed that cardiovascular complications significantly inhibited the feasibility of tube removal. This finding implies that parents of infants with dysphagia and cardiovascular complications should be informed that the infant may take longer to transition away from tube feeding and that oral feeding may remain problematic even as the infant grows. Practitioners need to consider appropriate therapeutic non-nutritive and oral care strategies that can maximize the infant’s health and functional oral motor skills as well as support the family’s quality of life.
Conflict of interest
The authors have no conflict of interest to report.