
Abstract
Background:
Parkinson’s disease (PD) is characterized by striatal dopamine deficiency. Since dopamine cannot cross the digestive and blood-brain barriers, its precursor, levodopa (L-DOPA), remains the mainstay of treatment. However, the significant pharmacokinetic (Pk) and pharmacodynamic (Pd) limitations of L-DOPA, combined with the severity of PD, may trigger motor and non-motor complications, for which continuous dopaminergic delivery therapies have been developed.
Objective:
The aim of this study was to review the literature on the Pk/Pd limitations of L-DOPA and how current treatments of continuous dopaminergic administration ameliorate these problems, in order to identify the need for new therapeutic avenues.
Methods:
A comprehensive literature search was carried out using PubMed and 75 articles were initially extracted. Following independent screening by two reviewers and consideration of eligibility, 10 articles were chosen for further analysis. Information concerning the Pk/Pd of L-DOPA was classified for each article.
Results:
Pk/Pd problems notably include: (i) restricted digestive and cerebral absorption; (ii) unnecessary peripheral distribution; (iii) short half-life; (iv) age- and PD-induced decline of central aromatic L-amino acid decarboxylase; (v) misdistribution in many cells; and (vii) pulsatile stimulation of dopaminergic receptors. Current treatments only slightly ameliorate some of these problems.
Conclusions:
Many Pk/Pd constraints are not resolved by existing continuous dopaminergic delivery therapies. This highlights the significant gap between these treatments and the ideal of continuous dopaminergic stimulation.
Keywords
INTRODUCTION
Parkinson’s disease (PD) is a complex neuropsychiatric condition characterized by progressive degeneration of the nigro-striatal pathway, responsible for managing automatic motor and non-motor functions [1, 2]. The degeneration of dopamine-producing neurons in the substantia nigra pars compacta leads to reduced dopamine concentrations in the striatum. Symptoms of the disease generally appear when at least 80% of the dopamine has been reduced [3]. Since its introduction in the late 1960 s, L-DOPA (L-3,4-dihydroxyphenylalanine), a precursor of the dopamine (dihydroxy-3,4-phenyl-ethylamine) has proven to be incredibly effective in managing the motor symptoms, dramatically improving the lives of many patients worldwide. L-DOPA response is now a diagnostic criterion [4–7].
L-DOPA then undergoes metabolization into dopamine, mediated by dopamine-decarboxylase (aromatic L-amino acid decarboxylase). Within adrenergic and noradrenergic neurons, dopamine can be further converted into noradrenaline via the action of dopamine β-hydroxylase. Finally, dopamine is catabolized by many enzymatic and non-enzymatic pathways, and notably the consecutive actions of two enzymes: monoamine oxidases A and B and catecholamine O-methyl transferase (COMT). Both of these enzymes are targeted by anti-parkinsonian drugs combined with L-DOPA, to extend its effects by roughly 30% (entacapone and tolcapone for COMT inhibitors) (Fig. 1).
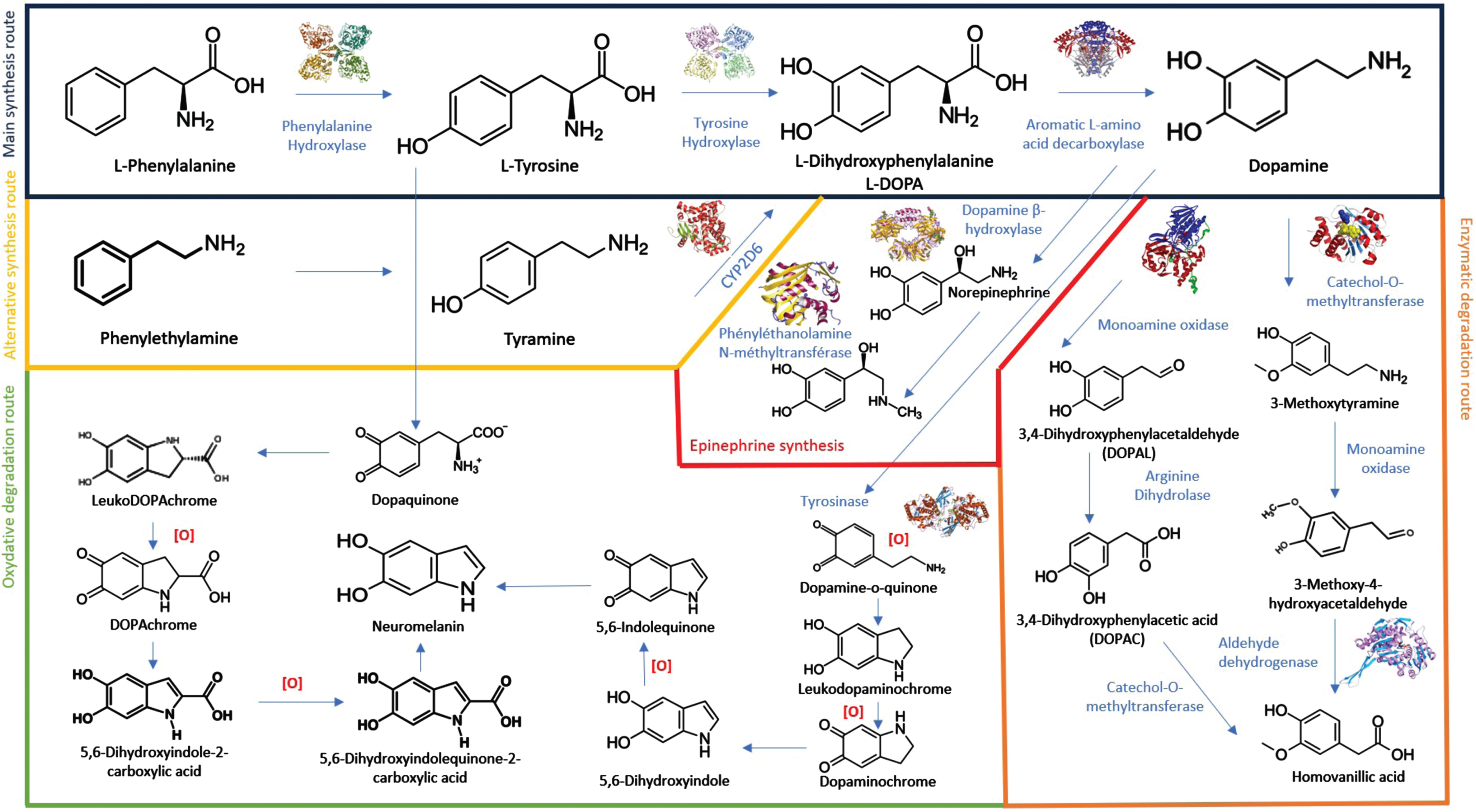
Complex metabolization of L-DOPA and dopamine through many enzymatic and non-enzymatic pathways.
Due to its pharmacokinetic (Pk) and pharmacodynamic (Pd) limitations, L-DOPA triggers L-DOPA-related complications (LDRC), including fluctuating efficacy such as motor fluctuations, wearing off, and L-DOPA-induced dyskinesia (LID) (1), affecting 50% of patients within 5 years and 80% of patients after 10 years of disease progression [8]. Peak-dose dyskinesia is the most common type of dyskinesia [9]. Off-period typically arises early in the morning, before the first dose of L-DOPA. Biphasic dyskinesia results from fluctuating plasma concentrations of L-DOPA and may occur 10–15 min post-dosing (Fig. 2). The earlier and more severe the degeneration of dopaminergic neurons, the more likely these complications will occur [10]. L-DOPA may also give rise to non-motor complications [11]. In older patients, the adverse effects more frequently include confusion, hallucinations, delusions, psychosis, and agitation.
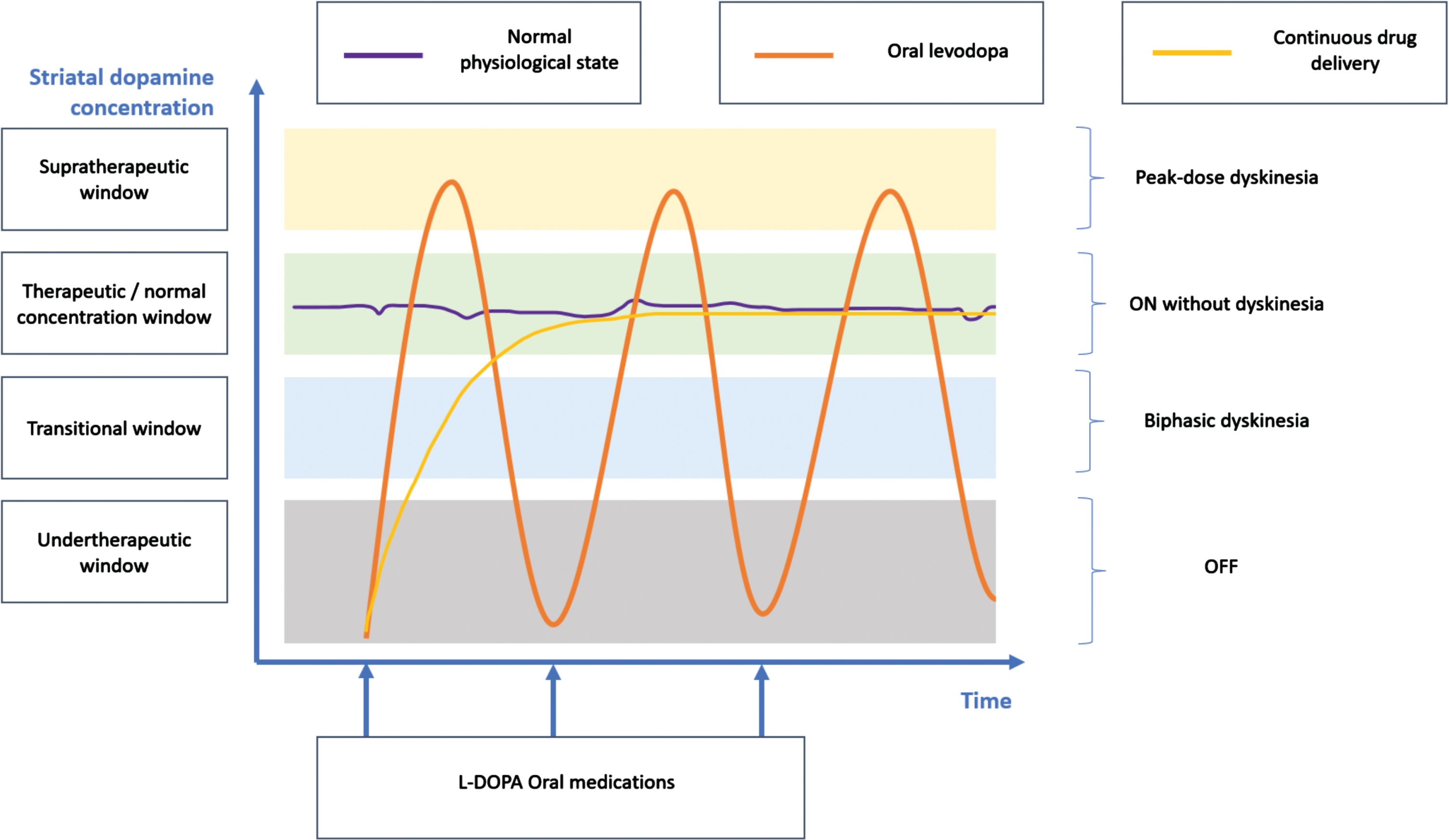
L-DOPA related complications as a function of the striatal dopamine concentration (i.e., reflecting the consequences of the pharmacokinetic and pharmacodynamic limitations). This diagram represents a patient’s diurnal period with regular medication intake.
To address the Pk/Pd limitations that give rise to LDRC, the concept of continuous dopaminergic stimulation has been proposed and continuous dopaminergic delivery therapies have been developed together with preclinical validation in 6 OH-dopamine rats [12] and MPTP monkeys [13, 14]. It is currently possible to administer dopaminergic therapies via two continuous administration routes, either subcutaneous or intrajejunal via gastrostomy, with two therapeutic principles: apomorphine, a dopaminergic agonist, levodopa/carbidopa prodrug (foslevodopa) or levodopa/carbidopa gel with or without entacapone.
Subcutaneous administration of apomorphine, a non-narcotic morphine derivative, enables continuous administration with an external pump and avoids the hepatic first-pass effect [15, 16]. Apomorphine administration enhances motor symptoms and quality of life [17], but does not entirely remove the need for oral treatments, and as a result, their Pk challenges persist [17–19]. Levodopa/carbidopa intestinal gel infusion (LCIG) enables continuous administration of L-DOPA into the proximal jejunum via a percutaneous gastrostomy tube. This technique can completely replace oral treatment, but is hampered by poor ergonomics (cumbersome external pump and daily replacement of L-DOPA/carbidopa cassettes), limiting its use to the most advanced patients [20–22]. An identical strategy combines L-DOPA/carbidopa gel with entacapone (Lecigon®) to reduce the dose of L-DOPA by 20% [23]. Foslevodopa/foscarbidopa (FL/FC) continuous subcutaneous infusion (ABBV-951 therapy, prodrug of L-DOPA) with an external pump has proven to be effective in a recent clinical trial [24]. A similar approach with a continuous subcutaneous L-DOPA/carbidopa delivery system has demonstrated its feasibility and safety [25].
We carried out a literature review of the Pk/Pd limitations of L-DOPA, in order to assess how these challenges might be addressed by current and emerging continuous dopaminergic administration treatments, and highlight potential areas for improving symptomatic dopaminergic therapies.
METHODS
Data source and search strategy
This review was conducted in alignment with Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines. However, certain deviations from these guidelines were undertaken due to the exclusive pharmacological focus of this literature review, for example, there was no statistical analysis or systematization of the extraction of quantitative results from the studies.
The bibliographic search was conducted using the PubMed database. While Medline and Embase were also explored, the returned articles were essentially identical to those found on PubMed.
To achieve the most effective search algorithm, multiple iterative searches were conducted incorporating key terms such as: pharmacokinetics, L-DOPA, and apomorphine. This ensured the number of articles retrieved was manageable and maintained a high degree of relevance. The final search algorithm employed was: (“pharmacokinetic” [Title] OR “pharmacokinetical” [Title] OR “pharmacokinetics” [Title]) AND (“Levodopa” [Title] OR “L-dopa” [Title] OR “Apomorphin” [Title] OR “Apomorphine” [Title]).
The literature search was conducted on November 1, 2023. Any articles published more than 20 years ago were not included in the selection. Additionally, articles in languages other than French or English were automatically excluded by the search algorithm.
Inclusion and exclusion criteria
Regarding the inclusion criteria, the selected papers needed to delineate the pharmacology, as well as the Pk/Pd of oral L-DOPA administration, LCIG infusion, or continuous subcutaneous apomorphine administration.
In terms of exclusion criteria, papers that did not primarily focus on the Pk/Pd of the aforementioned molecules were not included. Additionally, articles examining non-general cases regarding the form of the drug, administration route, patient population, or associated pathologies were disregarded. Studies involving healthy volunteers or those investigating the bioequivalence of generics were also excluded.
There were no inclusion or exclusion parameters pertaining to the type of articles, which ranged from clinical trials and literature reviews to pharmacology articles.
Selection of articles
All titles and abstracts of the identified studies were initially screened by one reviewer (AD) in accordance with the inclusion and exclusion criteria. From this preliminary screening, full texts deemed potentially eligible were obtained and independently reviewed by reviewers (AD, CM and DD). Any discrepancies encountered were discussed and resolved.
Data extraction and synthesis
One reviewer (AD) carried out the data extraction process, with a second reviewer (DD) conducting an independent reliability check. Data, including lead author, publication date, journal, abstract, and other pertinent information, were extracted systematically into a standardized form.
RESULTS
Selection of articles
The selected articles are in the Table 1. As depicted in Fig. 3, the search of the PubMed database returned a total of 87 articles. Among those not selected, 31 were related to the Pk/Pd of L-DOPA in conjunction with other drugs, primarily COMT inhibitors. 15 articles were related to L-DOPA administration methods other than those under review, while nine articles compared the Pk of different oral L-DOPA formulations, such as conventional and sustained-release forms. Four articles investigated the influence of environmental factors on L-DOPA Pk, including the dietary intake of the subjects. Two articles analyzed the impact of genetic polymorphisms, particularly in relation to genes encoding enzymes involved in the conversion of L-DOPA to dopamine. Another four articles focused on healthy subjects, two were unrelated to L-DOPA Pk or the apomorphine molecule, and one article explored patients with another pathology concomitant with PD. One article compared the Pk profiles of a generic and a brand name oral L-DOPA formulation. Lastly, one article was not available; the initial selection was based solely on the article’s title and abstract.
Main results of the pharmacokinetic and pharmacodynamic analyses of L-DOPA in the selected articles (articles about CSAI, LCIG, and other continuous dopaminergic stimulation are also included)
PD, Parkinson’s disease; L-DOPA, levodopa; L-AADC, L-amino acid decarboxylase; COMT, catechol-O-methyl transferase; LCIG, levodopa-carbidopa intestinal gel; LNAA, large neutral amino acids; SIBO, small-intestinal bacterial overgrowth; TDC, tyrosine decarboxylase; TOPA, 2,4,5-trihydroxyphenylalanine; Pk, pharmacokinetics; Pd, pharmacodynamics; LDRC, L-DOPA-related complications; QoL, quality of life; CSAI, Continuous Subcutaneous Apomorphine Infusion; SD, standard deviation; DBS, deep brain stimulation; RCT, randomized controlled trial; BMT, Best Medical treatment; MPTP, 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine.
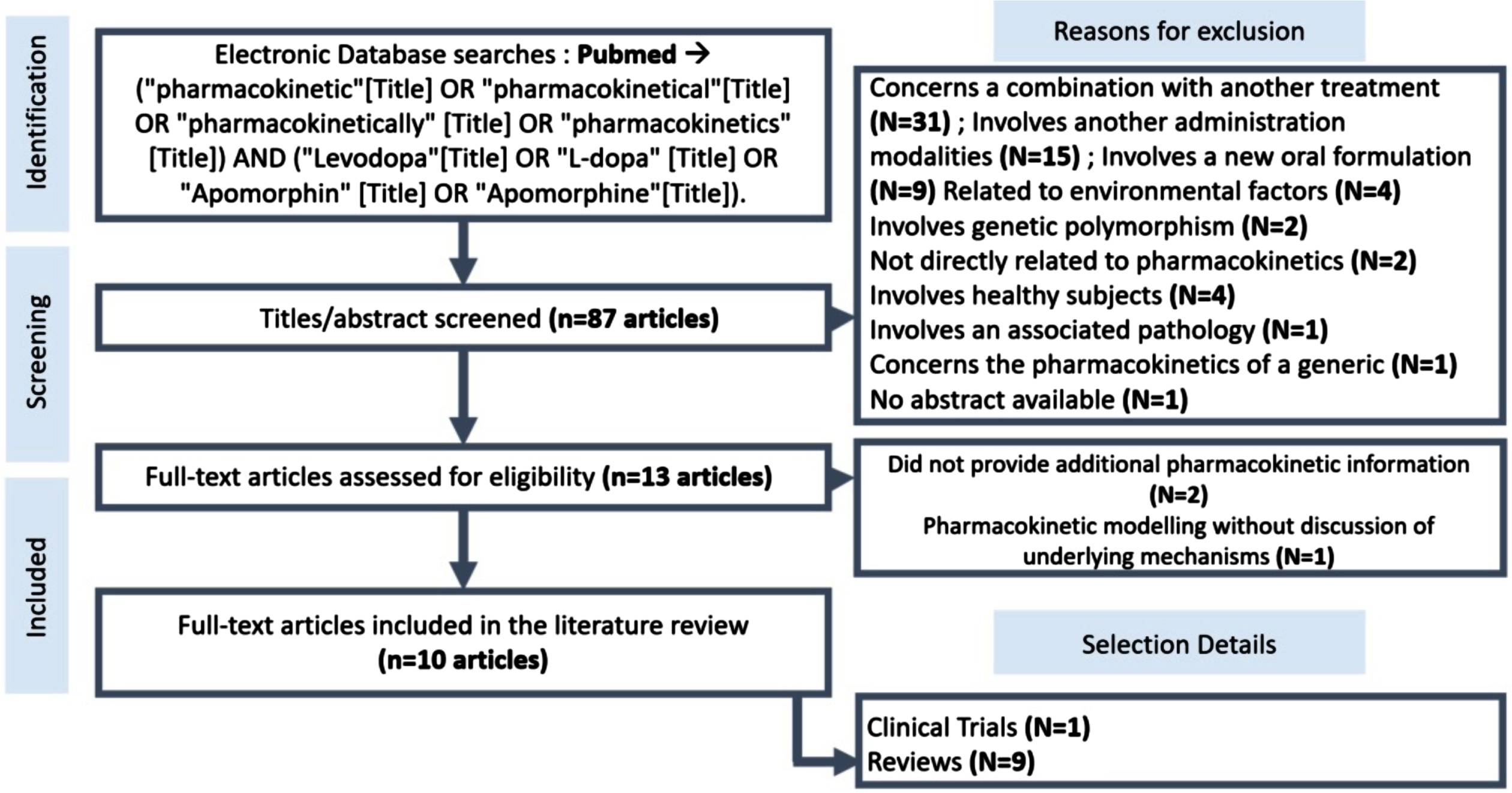
Flowchart showing the search for articles in the PubMed database.
DISCUSSION
The Pk/Pd challenges stemming from oral L-DOPA administration are outlined alongside the effects of the two commercially available continuous dopaminergic delivery therapies, namely LCIG and the apomorphine infusion pump. The various Pk limitations of L-DOPA and how continuous delivery therapies can address them are summarized in Table 2.
Pharmacokinetic problems with oral L-DOPA and the value of continuous dopaminergic administration therapies in resolving these problems
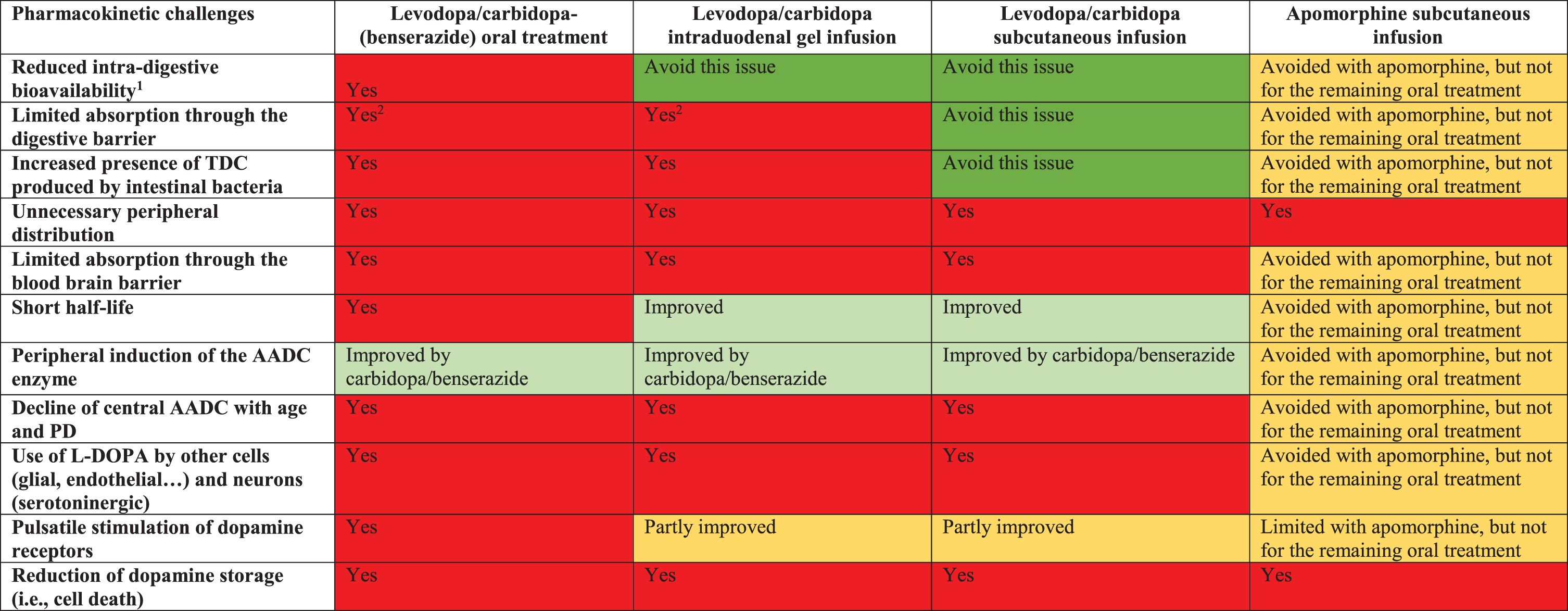
The color code represents the degree of impact of pharmacological bias (essentially pharmacokinetic) on the dopaminergic strategy. Red: significant impact; orange: partial impact (because 50–70% of the oral treatment is maintained), with a light vs. dark gradation if it is significant; green: therapeutic strategy not affected, with a light vs. dark gradation if it is significant. PD, Parkinson’s disease; TDC, tyrosine decarboxylase; AADC, amino acid decarboxylase.
Short half-life of L-DOPA
L-DOPA has a half-life of about 90 min [26], requiring patients to take doses very frequently (every 2–3 h) throughout the day to maintain consistent control over motor symptoms. The intermittent intake of L-DOPA requires the neurons in the substantia nigra to store the compound. As the disease advances, the number of these neurons diminishes, reducing this storage capacity. This progression compels patients to decrease the intervals between doses, creating greater Pk inconsistencies and resulting in motor fluctuations. The short half-life, combined with the increased dosing frequency leads to abnormal, large-scale, and intermittent activation of dopaminergic neurons.
The Pk challenges arising from the short half-life of L-DOPA are significantly alleviated by LCIG and FL/FC due to its continuous delivery mechanism. Additionally, the subcutaneous infusion of apomorphine mitigates this issue by lessening the dependence on oral L-DOPA administration.
Variable intragastric bioavailability
One of the challenges with oral L-DOPA administration is its variable intragastric bioavailability, which can be influenced by several factors.
Dysphagia, characterized by difficulty in swallowing saliva, liquids, or solid food, becomes prevalent with the progression of certain diseases. It is primarily caused by bradykinesia of the posterior region of the tongue and the jaw. Such a condition can result in aspiration, potentially leading to pulmonary infections. Additionally, it can cause dehydration and malnutrition. Importantly, dysphagia can also influence the response to oral medications, causing phenomena like “delayed-on” (a prolonged latency in response to a dose) and “no-on” (total dose ineffectiveness). Various clinical cases have identified instances where patients experience drug retention in the esophagus or the epiglottic vallecula. This retention can lower the peak plasma concentration of L-DOPA. However, reports in the literature have shown that treating dysphagia effectively, including through speech therapy, can revert to a more standard Pk profile for oral L-DOPA [27].
Currently available continuous dopamine delivery therapies offer solutions to these challenges. LCIG and FL/FC directly bypass the issues arising from dysphagia, ensuring more consistent drug bioavailability. Subcutaneous infusion of apomorphine provides a partial solution by diminishing the need for oral treatments, thus reducing the complications associated with dysphagia.
Gastrointestinal transit disturbances [28]
Constipation stands out as a prevalent non-motor symptom in PD, affecting more than 80% of patients [29, 30]. Often, this symptom is attributed to impairment of the autonomic nervous system, resulting in reduced digestive tract motility. Interestingly, constipation can manifest up to a decade before the emergence of motor symptoms. Various factors influence intestinal mobility and the movement of its contents, such as neurohumoral influences, an imbalance in the intestinal microbiota, with evidence suggesting the efficacy of probiotics as a therapeutic approach [31], intestinal inflammation, medication effects, and overall lifestyle habits.
Beyond the pronounced effect on a patient’s well-being and quality of life, gastroparesis, and its consequent delay in gastric emptying, hampers optimal absorption and the efficacy of orally administered drugs, like L-DOPA [32–34]. This results in increased pre-systemic decarboxylation, further diminishing the drug’s therapeutic potential.
LCIG and apomorphine improve this challenge. FL/FC overcomes this challenge.
Alterations in the gut microbiota and the role of tyrosine decarboxylase (TDC) production
It is important to highlight the changes in composition of the gut microbiota when discussing the Pk challenges of L-DOPA. Beckers et al. [35] reviewed multiple studies that indicated an elevated presence of specific bacterial genera in PD patients, notably Akkermansia (observed in 12 studies), Lactobacillus (10 studies), and Bifidobacterium (four studies). This increased bacterial presence could be attributed to the compromised intestinal motility inherent to PD. Interestingly, certain bacteria within these genera, specifically Enterococcus faecalis, Enterococcus farcium, Lactobacillus brevis, and Providencia rettgeri are known to produce tyrosine decarboxylase (TDC). While TDC primarily facilitates dietary tyrosine digestion, it also has the capability to decarboxylate L-DOPA. Intriguingly, there is a positive correlation between jejunal expression levels of TDC encoding genes and the required daily L-DOPA dosage for symptom control in PD patients. Conversely, there is a negative correlation with circulating plasma L-DOPA levels.
LCIG is not entirely exempt from these challenges but, compared to oral treatments, its susceptibility is diminished. The administration of apomorphine subcutaneously sidesteps gastrointestinal absorption, thus ameliorating, to a degree, the Pk challenges, although residual oral treatments might still present complications [36].
FL/FC overcomes this challenge.
Selective absorption challenges of L-DOPA in the digestive system
Absorption of L-DOPA is selective and intricate. The molecule depends on sodium-driven active transport mechanisms for its passage across both the digestive and blood-brain barriers. Furthermore, the transport of neutral L-amino acids, like L-DOPA, is restricted to a specific segment, primarily the duodenum and the initial portion of the jejunum. These unique Pk traits lead to an absorption rivalry between certain dietary components, specifically L-neutral amino acids from dietary proteins and orally administered L-DOPA [37]. As a result, after consuming a meal, patients might experience motor blockade episodes or notice variations in the Pk of their oral medications based on the composition of their meal. Given these challenges, the common recommendation is for patients to ingest their L-DOPA dose at least 45 min prior to eating, which reduces but does not eliminate the lower biodistribution.
LCIG does not overcome this challenge. The administration of apomorphine subcutaneously sidesteps gastrointestinal absorption, thus ameliorating, to a degree, the Pk challenges, although residual oral treatments might still present complications. FL/FC overcomes this challenge.
Peripheral distribution
The majority of orally-administered L-DOPA undergoes first-pass hepatic metabolism or is distributed in the skeletal muscle [26]. This molecule exhibits a pronounced peripheral distribution, as various organs and tissues, including the stomach, liver, kidneys, and even endothelial cells of blood vessels, possess dopaminergic receptors. Such widespread distribution has dual implications. On the one hand, it triggers side-effects such as nausea or hypotension (the latter results from the activation of D1-like receptors causing vasodilation). On the other, it significantly restricts the amount of L-DOPA reaching the blood-brain barrier. Highlighting the scope of peripheral L-DOPA decarboxylation, it is notable that nearly 45% of the body’s total dopamine is synthesized within the epithelial cells of the gastrointestinal tract. L-DOPA is routinely co-administered with a COMT inhibitor, which plays a role in converting L-DOPA to 3-O-methyldopa. In clinical scenarios, this inhibitor is believed to extend the effect of L-DOPA by approximately 20–30 min per dose. As noted previously, peripheral dopa decarboxylase activity inhibitors like carbidopa or benserazide are also employed to enhance the bioavailability of L-DOPA.
LCIG, FL/FC and apomorphine do not overcome this challenge.
Peripheral induction of the amino acid decarboxylase enzyme
One of the challenges with the Pk of oral L-DOPA stems from activation of the aromatic L- amino acid decarboxylase (L-AADC) enzyme. Triggered by decarboxylase inhibitors, this activation prompts the early conversion of L-DOPA to dopamine peripherally. This, in turn, significantly diminishes the bioavailability of L-DOPA in the brain. Studies indicate that when administered alongside peripheral AADC inhibitors such as carbidopa or benserazide, the bioavailability of oral L-DOPA increases threefold [38]. It is noteworthy that while the apomorphine pump reduces issues related to peripheral distribution, it does not fully eliminate them. Likewise, LCIG, despite its broad peripheral distribution, which is not needed for its neurological effects, presents similar challenges [39].
LCIG and FL/FC do not overcome this challenge. The administration of apomorphine subcutaneously ameliorates this challenge, although residual oral treatments may still cause complications.
Stimulation of different dopamine receptors
Dopamine, which is stimulated by the administration of L-DOPA in PD patients, can bind to various receptors. The five types of dopamine receptors differ in their central and peripheral locations, genes coding for their protein, affinity for dopamine, and the nature of the response their stimulation elicits. They are divided into two categories: D1-like receptors and D2-like receptors, depending on the type of G protein to which they couple. Stimulation of D1 and D5 receptors, which belong to the D1-like category and are located exclusively at the postsynaptic level, results in the production of cyclic AMP and depolarization of the neuronal membrane due to their association with the Gs protein. Conversely, D2-like receptors, which can be both presynaptic and postsynaptic, reduce the amount of cyclic AMP produced and induce hyperpolarization when activated, leading to a decrease in the number of neurotransmitters released.
While apomorphine is categorized as a dopamine agonist, it exhibits characteristics that differentiate it from other oral dopamine agonists. Its catechol moiety enables apomorphine to interact with a broad spectrum of D1- and D2-like receptors, including D1, D2 S, D2 L, D3, D4, and D5 [5, 40]. However, the mechanisms by which apomorphine and dopamine influence dopaminergic neurotransmission are not identical. Dopamine neurons can oscillate between two distinct activity states: slow tonic firing and phasic burst firing [41]. While apomorphine can partially reinstate slow tonic firing through the stimulation of postsynaptic receptors, it lacks the capability to be taken up by the dopamine transporter. This means that, unlike dopamine, apomorphine does not enhance presynaptic dopamine availability and cannot potentiate phasic dopamine signals, a mechanism crucial for memory functions [42].
Variability and constraints of L-DOPA absorption across the blood-brain barrier
Similar to its interaction with the digestive barrier, the passage of L-DOPA through the blood-brain barrier depends on a saturable sodium-dependent transporter. This setup places L-DOPA in competition with other L-neutral amino acids that originate from protein degradation and various dietary amino acid sources. As a result, access of L-DOPA to the brain is both constrained and unpredictable [26].
LCIG and FL/FC do not overcome this challenge. The administration of apomorphine subcutaneously ameliorates this challenge, although residual oral treatments may still present complications.
Distribution of L-DOPA in serotoninergic neurons, astrocytes, and endothelial cells
After entering the central nervous system, L-DOPA is taken up by various cell types other than dopaminergic neurons through the L-type amino acid transporter [43]. These cells, which include serotoninergic neurons, glial cells, and endothelial cells, express L-AADC, enabling them to convert L-DOPA into dopamine and store it within vesicles [44]. Notably, these cell types lack the dopamine transporter DAT, rendering them incapable of reuptake of the synthesized dopamine, resulting in unregulated dopamine production. Research has indicated a link between serotoninergic neurons and L-DOPA-induced dyskinesia. Specifically, experiments employing 5,7-dihydroxytryptamine, a selective neurotoxin targeting serotonergic neurons, have led to the cessation of these L-DOPA-triggered side-effects.
LCIG and FL/FC do not overcome this challenge. The administration of apomorphine subcutaneously ameliorates this challenge, although residual oral treatments may still present complications.
Decline of central L-AADC with advancing age and PD progression
As PD progresses and with increasing age, there is a notable decline in the activity of L-AADC within dopaminergic neurons. This decline results in decreased conversion of L-DOPA into dopamine over time. While some research suggests that, even in the later stages of the disease, the activity of the enzyme remains sufficiently robust for L-DOPA to dopamine conversion [26], other studies have highlighted potential therapeutic avenues. For instance, gene therapy aimed at enhancing the expression of L-AADC has been shown to improve Parkinson’s symptoms [45].
LCIG and FL/FC do not overcome this challenge. The administration of apomorphine subcutaneously ameliorates this challenge, although residual oral treatments may still present complications.
Pd issues with the pulsatile stimulation of dopamine receptors
One of the core challenges faced in the treatment of PD stems from the pulsatile stimulation of dopamine receptors [46, 47], which can be attributed to the short half-life of L-DOPA and the Pk challenges associated with its oral, and to a lesser extent, enteral administration. Such unpredictable and uneven stimulation from L-DOPA often results in motor complications, including peak dose fluctuations, biphasic dyskinesias, the wearing-off phenomenon, and circadian off periods [48]. This has given rise to the idea of “continuous dopaminergic stimulation” aiming for steady L-DOPA administration to achieve more consistent dopamine receptor activation. Yet, a more precise term might be “continuous dopaminergic administration” because the treatments do not genuinely offer uninterrupted stimulation. Moreover, the stimulation of dopamine receptors is complex and multiple with at least a low and continuous tonic stimulation (i.e., inhibition) and a phasic one (i.e., activation). The inherent nature of L-DOPA and its misdistribution to cells other than dopaminergic neurons remain a significant hurdle, irrespective of administration continuity. Only direct dopamine administration could possibly sidestep this misdistribution challenge.
LCIG, FL/FC and apomorphine do not overcome this challenge.
Decline in dopamine storage due to neuronal death
As PD advances, the gradual death of dopamine neurons significantly impacts the Pk of L-DOPA. Imaging studies have indicated that with disease progression, there is a heightened release of dopamine in the brain following a L-DOPA dose, potentially explaining L-DOPA-induced dyskinesias. This can be attributed to multiple factors: the diminished capacity for vesicular dopamine storage, a decrease in dopamine reuptake sites due to vanishing DATs, and the unintended utilization of L-DOPA by non-dopaminergic cells. Continuous dopaminergic administration may reduce the impact of this problem on treatment pharmacokinetics. However, being only symptomatic treatments, LCIG, FL/FC, and apomorphine do not overcome this challenge.
How can continuous dopaminergic delivery therapies be improved?
While continuous dopaminergic delivery therapies can address some of the Pk challenges posed by oral L-DOPA, they cannot address many pharmacological challenges. This may explain why pivotal therapeutic trials showed only a 1.9-h improvement in On without troublesome dyskinesias compared to the placebo group with LCIG (22) or an apomorphine pump (18), and 1.7 h with FL/FC [24]. In fact, there was an improvement of around 2 h in the placebo group and less than 2 additional hours in the treated groups in patients who had an average of 6 h of non-control LDRC. It therefore appears that these therapeutic strategies, while clearly effective, offer only an incomplete solution to LDRC. Interestingly, brain stimulation does not improve the situation any further, with 3.25 h without placebo group (i.e., it was also around 4 h including the placebo effect for continuous dopaminergic delivery therapies). This may be explained by the fact that more than 50% of the oral treatment is maintained under subthalamic stimulation [49, 50]. This underlines the importance of progressing towards innovative continuous dopaminergic treatments, whether through new molecules, formulations, or administration methods, while taking these Pk/Pd challenges into account.
One of the most obvious explanations is that these LDRCs are intimately linked to L-DOPA use, and that as long as L-DOPA is used, it causes dyskinesias, even if LDRC and dyskinesias are less pronounced with continuous administration, they persist due to all the Pd mechanisms involved. Interestingly, there is one therapeutic innovation that could potentially overcome these mechanisms, namely the direct administration of dopamine at the intracerebral level. This strategy has never been developed previously, for fear of rapid and major oxidation of dopamine. However, a dopamine that is synthesized, stored, and administered anaerobically (A-dopamine) has recently been developed. This continuous cerebral infusion of A-dopamine involves surgical implantation of a thin catheter in the 3rd ventricle just proximal to the bilateral striatum, connected to a programmable pump under the abdominal skin. This telemetry-controlled pump continuously delivers an anaerobic solution of dopamine hydrochloride directly into the cerebrospinal fluid, enabling doses to be precisely adapted to circadian needs. Preclinical results in 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine (MPTP) lesioned mice, 6 OH-dopamine lesioned rats, and MPTP lesioned monkeys demonstrated that intracerebral administration of A-dopamine induced a strong and continuous motor improvement. The most astounding preclinical finding was that even at very high doses of dopamine, no dyskinesia was observed in any of the three models. Conversely, oral L-DOPA induced dyskinesia even with the smallest effective dose [51, 52]. A Phase I/IIB clinical trial involving 12 patients is in progress (ClinicalTrials.gov ID: NCT04332276) [53]. Although clinical data and further Pk analysis are required, it is consistent to hypothesize that central administration of A-dopamine could limit peripheral and central Pk problems and Pd issues (i.e., pulsatile stimulation and dopamine misdistribution).
Conclusion
L-DOPA, combined with an AADC inhibitor, has improved the lives of millions of patients suffering from PD and remains a pivotal treatment. However, the many Pk/Pd limitations of L-dopa have a major impact on the lives of patients with the induction of severe LDRC. We have seen that most L-DOPA formulations and delivery strategies retain the many Pk/Pd limitations. This should encourage researchers and manufacturers to develop new dopaminergic stimulation strategies without L-DOPA, such as dopamine administration.
Footnotes
ACKNOWLEDGMENTS
We would like to thank Everpharma for its financial support and Val Hopwood, BSc, PhD, for proofreading the manuscript.
FUNDING
This review was funded by EverPharma.
CONFLICT OF INTEREST
AD is a former employee of InBrain Pharma. DD and CM are co-founders of InBrain Pharma and InVenis Biotherapies, in which they have an equity stake. CM is CMO of Feetme. DD and CM have provided consulting services or served on the scientific boards of Abbvie, Alterity, Orkyn, Air Liquide, Apopharma, Lundbeck, EverPharma, and Boston Scientific.
DATA AVAILABILITY
All data is available on request by e-mail from david.devos@chu-lille.fr.