
Abstract
The aim of this review is to examine the intersection of Parkinson’s disease (PD) with nutrition, to identify best nutritional practices based on current evidence, and to identify gaps in the evidence and suggest future directions. Epidemiological work has linked various dietary patterns and food groups to changes in PD risk; however, fewer studies have evaluated the role of various diets, dietary components, and supplements in the management of established PD. There is substantial interest in exploring the role of diet-related interventions in both symptomatic management and potential disease modification. In this paper, we evaluate the utility of several dietary patterns, including the Mediterranean (MeDi), Mediterranean-DASH Intervention for Neurodegenerative Delay (MIND), Alternative Healthy Eating Index (AHEI), vegan/vegetarian, and ketogenic diet in persons with PD. Additionally, we provide an overview of the evidence relating several individual food groups and nutritional supplements to PD risk, symptoms and progression.
Keywords
INTRODUCTION
Parkinson’s disease (PD) is the second most prevalent neurodegenerative disorder worldwide [1]. The pathogenesis of PD is thought to involve a confluence of intestinal dysbiosis, inflammation, oxidative stress, mitochondrial dysfunction, alpha-synuclein aggregation, and nigrostriatal dopaminergic neuron loss [2]. PD’s cardinal motor features— bradykinesia, rigidity, tremor and postural instability— and non-motor features can interfere with food intake and dietary composition [3]. Motor symptoms can make shopping for, preparing and eating meals, especially in social settings, challenging [3]. Deterioration of smell and taste sensation, depression, apathy, cognitive decline, changes in reward processing, and impulse control disorders can alter appetite and food preferences (e.g., increasing cravings for sweets) [3, 4]. Dysphagia, nausea, delayed gastric emptying, small intestine bacterial overgrowth, and constipation can cause early satiety and impaired levodopa absorption, as can protein-containing foods [3, 5–7]. A recent meta-analysis (n = 5,613) identified a third of persons with PD (PwP) as being at risk of malnutrition [7], which is a risk factor for worse quality of life and health outcomes [3, 9].
Observational studies have linked dietary patterns and individual food groups to PD risk, age of onset, progression, symptom severity, and mortality rates [10–18], yet there is a paucity of randomized controlled trials (RCTs) into nutritional interventions. Nutritional interventions can interact with multiple disease mechanisms simultaneously, offering the potential for disease-modification, while nutritional self-management presents an opportunity for empowerment in PwP. In this paper, we summarize the current evidence on dietary and nutritional supplement strategies in PD and suggest future directions for research.
DIETARY PATTERNS
Mediterranean diets
There is a wide range of Mediterranean (MeDi) diets, overall characterized by a predominantly plant-based diet rich in vegetables, fruits, whole grains, legumes, unsaturated fatty acids (mostly olive oil), nuts/seeds and fish/seafood, with moderate intake of poultry, and wine and low intake of red and processed meat, sweets, sugar-sweetened beverages, refined grains and saturated fatty acids [19]. Between 2020–2023 alone, several observational studies reported inverse associations between MeDi diet adherence and PD risk, age of onset and prodromal PD symptoms [20]. A single-center, cross-sectional Canadian study of 167 participants with PD found a correlation between MeDi diet scores and later disease onset, of up to 8.4 years in men, specifically (p = 0.002) [18]. A US 20-year prospective analysis involving 47,669 individuals [21] reported an inverse association between long-term MeDi diet adherence and prodromal PD features (odds ratio (OR) for 3 + versus 0 features = 0.82 (95% confidence interval (CI): 0.68–1.00)), as did a 3-year study of 1,047 adults in Greece (60–70% lower risk in highest versus lowest quartile for MeDi adherence) [22]. A 30-year study of > 47,000 Swedish women identified a reduced risk of PD among individuals with high versus low adherence to MeDi diets in middle age (hazard ratio (HR) = 0.54 (95% CI: 0.30–0.98)) [14], while the longitudinal Dutch Rotterdam Study of 9,414 adults found a similar potential, although non-significant, association (HR = 0.89 (95% CI: 0.74–1.07)) [13]. The presumed protective properties of MeDi diets against PD may stem from the anti-inflammatory and antioxidant properties of polyphenol phytochemicals and vitamins found in fruits and vegetables, neuroprotective effects of omega-3s found in fish, and/or beneficial effects of high-fiber diets on the gut microbiome [20, 23]. Japanese dietary patterns enriched in vegetables, fruits and fish were similarly associated with reduced PD risk in a case-control study of 249 PwP and 368 controls without neurodegenerative disease [24].
Despite compelling epidemiologic evidence for benefits of MeDi diets in PD, RCTs have been limited. A single-center RCT from Iran involving 80 patients with idiopathic PD reported a modest increase in Montreal Cognitive Assessment and a decrease in Parts I, II and IV Unified Parkinson’s Disease Rating Scale (UPDRS) scores in response to a 10-week Mediterranean diet intervention [11, 12]. In a pilot single-arm study of eight PwP, a 5-week MeDi diet intervention reduced constipation, in association with changes in gut microbiome composition [25].
MIND diet
The MIND diet combines principles from the MeDi and Dietary Approaches to Stop Hypertension diet, originally developed to reduce cognitive decline [26]. The MIND encourages leafy greens, bean and berry consumption and discourages cheese, butter and margarine intake [27]. A longitudinal study of 706 aging American adults found that MIND diet adherence was associated with reduced incidence and slower progression of parkinsonism relative to MeDi diet adherence [28], while a Canadian cross-sectional study found that MIND diet adherence was associated with a higher age at PD onset of up to 17.4 years (p < 0.001) specifically in females [18]. A recent analysis of the Modifiable Variables in Parkinsonism Study identified an approximately two-fold decrease in severity of patient-reported symptoms associated with MIND relative to MeDi diet adherence [27]. However, the effect of the MIND diet on PD symptoms, progression and PD-associated cognitive decline has yet to be evaluated in an interventional study.
Vegetarian and vegan diets
Limited prior epidemiological studies have suggested lower rates of PD in societies mostly following vegetarian and vegan diets [29–31]. A recent UK biobank analysis found an association between a healthful plant-based diet and reduced PD risk (HR = 0.78 (95% CI: 0.61–0.99)), whereas an unhealthy plant-based diet was associated with a higher risk to develop PD (HR = 1.38 (95% CI: 1.08-1.74)) [32]. One recent trial of a 14-day ovo-lacto vegetarian diet in 16 patients with PD demonstrated significant improvements in UPDRS Part III scores [33].
Diet quality as measured by the Alternative Healthy Eating Index
The Alternative Healthy Eating Index (AHEI) is a measure of diet quality adapted from the Healthy Eating Index, which scores foods based on their association with chronic disease risk [34]. A recent analysis of the prospective Nurses’ Health Study and the Health Professionals Follow-Up Study data reported a reduced risk of prodromal PD features over two decades among individuals with higher AHEI scores [21]. In the same cohort, over the 32–34 years of follow-up, 1,251 participants developed PD, of which 942 died. Higher scores on the AHEI were associated with lower rates of all-cause and PD-specific mortality (adjusted HR, highest versus lowest AHEI quartile = 0.69 (95% CI: 0.56–0.85) for prediagnosis scores and 0.57 (95% CI: 0.42–0.78) for postdiagnosis scores) [16]. The association between AHEI scores and mortality was driven primarily by higher intake of whole grains, nuts and legumes, and lower intake of red and processed meats [16]. Additionally, the association was partially explained by higher total flavonoid intake, which was independently linked to reduced mortality in PwP [35].
Ketogenic diet
The KD is a high-fat, low-carbohydrate diet, which, among other mechanisms [36], may circumvent bioenergetic deficits in PD where affected neurons are unable to efficiently utilize glucose for energy production but likely continue to be able to use ketone bodies such as body beta-hydroxybutyrate, generated in response to a high-fat, low-carbohydrate diet [37]. Ketone bodies may enable neurons to feed electrons into the mitochondrial respiratory chain at complex II, bypassing PD-related deficiencies in complex I metabolism [38]. Four recent RCTs have investigated the feasibility, safety and short-term efficacy of KDs in PD [36]. In an 8-week pilot study comparing a KD to a low-fat diet in 38 participants with PD, both groups showed improvement on all four parts of the UPDRS, with the KD group showing greater improvement in Part I scores [39]. However, worsening tremor and/or rigidity was noted in the KD group 1–4 weeks into the diet intervention, leading to two participant withdrawals. In an open-label, non-controlled pilot study of 16 PD participants on a 12-week KD intervention, significant improvements were seen in UPDRS Part I and total Parkinson Anxiety Scale scores [40]. An 8-week study comparing a ketogenic (n = 7) versus high-carbohydrate (n = 7) diet in individuals with PD and mild cognitive impairment reported improvements in lexical access and memory in the ketogenic diet arm [10]. Another study of 68 participants with PD reported improvements in voice quality following three months of a ketogenic diet [41].
Protein-redistribution diets
The timing of macronutrient intake in PD can have important implications for levodopa transport and effectiveness [42]. Ten trials of protein-redistribution diets have been conducted to date [6], which typically involve limiting protein to 0–10 g at breakfast and lunch, with remaining protein intake to occur at dinner. Taken together, these studies reported 32–79% reductions in motor symptoms, 30–107 minute reductions in postprandial motor fluctuations, and reductions in disability scores in PwP on protein-redistribution diets [6, 42]. However, concerns around potential loss of weight and lean body mass on protein-redistribution diets remain [6].
FOOD GROUPS
Dairy
Early prospective studies suggested that high consumption of dairy may increase the risk of PD [43–46]. A prospective analysis of the Nurses’ Health Study (n = 80,736) and the Health Professionals Follow-up Study (n = 48,610) found that this association held only for low-fat dairy foods [17], while in the Rotterdam study, higher intake of yoghurt, fermented milk and butter, respectively, but not milk or cream intake, was associated with higher PD risk [13]. Higher consumption of ice cream, yoghurt and cheese has been associated with faster PD progression [47]. A proposed explanation for the association of PD risk with milk intake relates to the anti-uricemic effect of casein and lactalbumin found in milk, as urate’s antioxidant properties are believed to protect against PD development [48]. Anti-uricemic effects may be mitigated by saturated fats in high-fat dairy products [17]. Alternatively, some have proposed that pesticide contaminants in dairy products may contribute to PD-associated neurodegeneration [17, 49]. Overall, the association of PD risk with specific dairy products is inconclusive.
Alcohol
Evidence regarding the relationship between alcohol intake and PD risk has been mixed. A prospective study of a cohort including 694 incident PD cases found no association between alcohol consumption and PD development overall, though men reporting moderate (5–29.9 g/day) alcohol consumption were at approximately 50% higher risk for PD than those reporting light (0.1–4.9 g/day) consumption (HR = 1.58 (95% CI: 1.07–2.33) for 5–14.9 g/day and HR = 1.52 (95% CI: 1.00–2.33) for 15–29.9 g/day) [50]. However, a linear exposure-response trend was missing [50]. A recent systematic review of 11 prospective studies found a U-shaped association between alcohol intake and PD risk [51], with an overall relative risk for PD comparing any versus no alcohol intake of 0.81 (95% CI: 0.65–0.95). A meta-analysis of 52 observational studies found a negative, dose-dependent association between alcohol intake and PD risk (OR of ever drinking alcohol versus never drinking among PwP = 0.84 (95% CI 0.76–0.92)) [52] However, the authors note that the relationship between alcohol and PD may be confounded by smoking status in many of the studies included in their meta-analysis, and that results may similarly be influenced by survivor, selection and recall bias [52]. Others have suggested that moderate alcohol consumption may be associated with personality features characteristic of a more risk-taking personality, which itself is associated with reduced PD risk [53]. Alternatively, alcohol-mediated increases in levels of plasma antioxidants, such as folic acid, niacin, purine and urate, may help to explain an inverse relationship between alcohol consumption and PD up to a certain threshold [51, 53].
Caffeine
Observational studies have suggested protective effects of caffeinated coffee and tea against PD risk and progression, but benefits of caffeine alone have not borne out in clinical trials involving PwP. In a 2020 meta-analysis, coffee and caffeine were associated with a reduced risk of PD onset among healthy individuals and reduced rates of PD progression among PwP [54]. Regular caffeine intake was also associated with later PD age of onset [55]. Higher plasma caffeine concentrations were linked to PD resistance among pathogenic LRRK2 gene mutation carriers in a metabolomic study [15]. The putative protective effect of caffeine may be mediated by alterations in alpha-synuclein breakdown or gut microbiome composition, or by direct neuroprotective antagonism of adenosine A2A receptors in the brain [56]. However, a RCT in participants with established PD comparing supplementation of caffeine pills (200 mg twice daily, n = 60) to placebo pills (n = 61) was terminated early due to a lack of clinical improvement in parkinsonian symptoms [57]. Additionally, authors noted a slight increase in dyskinesia and decrease in cognitive testing scores [57]. These results could be due to the isolation of caffeine, suggesting other non-caffeine components of coffee and tea may be protective against PD.
PD-specific foods based on patient-reported outcomes
Mischley et al. (2017) investigated effects of various dietary components on Parkinson’s disease progression in a web-based observational cross-sectional study of 1,053 PwP using patient-reported outcomes (PROs) as the primary outcome measure [47]. This study found that fresh vegetables, fresh fruit, nuts and seeds, non-fried fish, olive oil, wine, coconut oil, fresh herbs, and spices were associated with slower rates of PD progression, while canned fruits and vegetables, diet and non-diet soda, fried foods, beef, ice cream, yoghurt, and cheese were associated with faster rates of PD progression.
NUTRITIONAL SUPPLEMENTS
Vitamin D
Several studies have noted high rates of vitamin D deficiency in PD, associated with disease risk, motor severity, cognitive impairment and increased fall risk [58–62]. Vitamin D receptors and vitamin D synthesis enzymes are highly expressed in the substantia nigra, suggesting an important role of vitamin D in the proper functioning of these neurons [63]. A review of the four completed trials of vitamin D supplementation in PD concluded that vitamin D supplementation had no significant effect on PD severity, dyskinesia, activities of daily living or balance [62]. Of note, most studies supplemented vitamin D regardless of baseline vitamin D levels. Furthermore, this finding does not preclude potential genotype-specific benefits of vitamin D supplementation. Suzuki et al. (2013) found that 30 weeks of vitamin D3 supplementation (1200 IU/day) mitigated increases in Hoehn and Yahr stage over a 12-month follow-up period, specifically in PwP with vitamin D receptor FokI genotypes TT and CT [64]. Osteoporosis is more common in PD than age-matched healthy controls while PwP are also at increased risk of falls and fractures with significant implications for morbidity and mortality. Optimized vitamin D and calcium intake are an important part of the management of osteoporosis in PD [65].
Vitamin E and omega-3 fatty acids
Due to their antioxidant and anti-inflammatory properties, vitamin E and omega-3 fatty acid co-supplements have been suggested as potentially beneficial in PD [66]. A 12-week RCT compared supplementation with 1,000 mg omega-3 fatty acid from flaxseed oil and 400 IU vitamin E versus placebo in PD patients [67]. The intervention improved total UPDRS scores, decreased serum high sensitivity C-reactive protein (a marker of systemic inflammation) and increased total antioxidant capacity. A 30-week placebo controlled RCT (n = 40) in PD investigating a formula composed of omega-3 fatty acids, vitamin A, vitamin E and gamma-tocopherol reported significant reductions in UPDRS Part III scores in the treatment group at the 12-month follow-up [68]. Fish oil supplementation was associated with reduced rates of PD progression in Mischley et al.’s observational study (2017) [47].
Vitamins B6, B9, and B12
Homocysteine is an alpha-amino acid intermediary product of methionine metabolism, whose role in PD was recently reviewed [69]. In brief, hyperhomocysteinemia is a common finding in PD, driven by catechol-O-methyltransferase-mediated levodopa metabolism [69]. Hyperhomocysteinemia has been associated with increased risk of cardiovascular [70], and cerebrovascular disease [71], cognitive impairment [72], and cortical structural damage [73]. Vitamins B6, B12, and B9 (folate) are cofactors in downstream pathways responsible for the metabolism of homocysteine, which can become depleted in the context of increased homocysteine generation via levodopa metabolism [69, 72]. Supplementation with vitamins B6 (< 25 mg daily), B12 and folate has been suggested for the prevention and treatment of hyperhomocysteinemia in PD although dedicated RCTs are lacking [69, 74]. Of note, in cases of PD with renal insufficiency, the standard cyanocobalamin B12 supplement should be substituted for methylcobalamin (500–100 ug per day) [69].
Vitamin B1
The role of vitamin B1 (thiamine) supplementation in PD remains relatively unexplored, although a recent study has suggested an association between thiamine deficiency and mild cognitive impairment in PD [75].
Vitamin C
There is no association between vitamin C intake and PD risk on meta-analysis [76]. However, vitamin C enhances levodopa absorption, and may confer benefit in elderly individuals with PD in whom drug bioavailability is often limited [77].
Citicoline
Citicoline (cytidine-diphosphocholine (CDP-Cho)) is an endogenous compound involved in the biosynthesis of acetylcholine, whose neuroprotective properties have been suggested by several animal and human studies [78]. A systematic review of 355 patients across seven heterogenous, small and mostly older studies found that citicoline supplementation was associated with motor and cognitive improvements in PD, facilitating a reduction in levodopa dose by up to 50% [78].
Fiber, prebiotics, and probiotics
Emerging evidence for a role of gut dysbiosis in PD has led to increasing interest in microbial-based therapies, such as probiotics. A 2023 meta-analysis of 11 RCTs reported high quality evidence for a beneficial effect of probiotics on UPDRS Part III, Non-Motor Symptoms Questionnaire, and two depression scale scores [79]. Although significant improvement in gastrointestinal motility was shown in the probiotic group compared to the placebo group, constipation symptoms and Bristol Stool Scale scores did not differ between the two groups in this meta-analysis [79]. However, two RCTs to date have provided Class I evidence in support of the use of multi-strain probiotics to treat constipation in PwP [80, 81]. In [81], the multi-strain probiotic was combined with prebiotic fiber in a fermented milk preparation. Beyond symptomatic benefits, dietary fiber may alleviate the PD-associated decrease in butyrate-synthesizing bacteria in the gut, which is thought, among other mechanisms, to reduce inflammation [82]. Two recent studies demonstrated that dietary fiber could increase butyrate production in PD participants’ stools in vitro [82, 83].
Mucuna pruriens
Mucuna pruriens is a levodopa-containing leguminous plant which grows in tropical climates, and may be considered as an alternative therapy to synthetic levodopa/carbidopa in low-resource settings [84]. A double-blind crossover study by [85] in eight patients with PD reported a faster onset of effect and longer “on” time duration with Mucuna pruriens preparation versus a standard 200/50 mg levodopa/carbidopa preparations. A double-blind, randomized, controlled crossover study with 18 PD patients, [86] found that single-dose Mucuna pruriens produced a similar motor response with a noninferior safety profile to levodopa/benserazide. A second double-blind, randomized, controlled crossover study from the same group in 14 patients with PD motor fluctuations and dyskinesias corroborated the findings of similar symptomatic control between daily Mucuna pruriens and levodopa/carbidopa over 16 weeks [87]. However, the high rate of gastrointestinal side effects and shortening “on” time in the Mucuna pruriens arm of this trial led to a 50% dropout rate [87]. Authors recommend that patients appropriately managed on synthetic levodopa/carbidopa in high-resource settings be advised against self-medicating with Mucuna pruriens due to the poor tolerability profile.
DISCUSSION AND FUTURE PERSPECTIVES
The role of nutrition in PD is of interest among clinicians, researchers and PwP alike, given strong epidemiological evidence implicating dietary patterns and malnutrition in the disease process [20]. However, few high-quality randomized controlled dietary intervention trials have been conducted in PD to date [20]. Randomized controlled nutrition intervention trials are challenging to conduct due to a variety of reasons including variability in baseline dietary factors and nutrient status [88], the necessity for substantial behavioral changes on the part of the participant and their household members, the risk of high attrition rates and suboptimal adherence, blinding and treatment standardization [89]. Reliable and convenient capture of dietary intake presents a further challenge as does variability in nutrient content in a given food, although the advent of biomarkers of food intake, or biomarkers of food intake (BFIs, e.g. of specific flavonoids) may prove to be an increasingly valuable tool in these regards [90]. In PD, added complications include long follow-up times required to ascertain a disease modifying effect, and the lack of reliable biomarkers to both identify patients with early disease who may optimally benefit from such interventions and to track interventional outcomes [20]. While consensus recommendations around a particular diet have yet to be developed for PD as a result, this paper sought to provide a comprehensive review of evidence in the field, and we will conclude with suggestions for future directions. Figure 1 illustrates the complex relationships between dietary patterns and food choices, socioeconomic factors, quality of life, PD-related malnutrition, symptoms and disease pathophysiology, highlighted in this review.
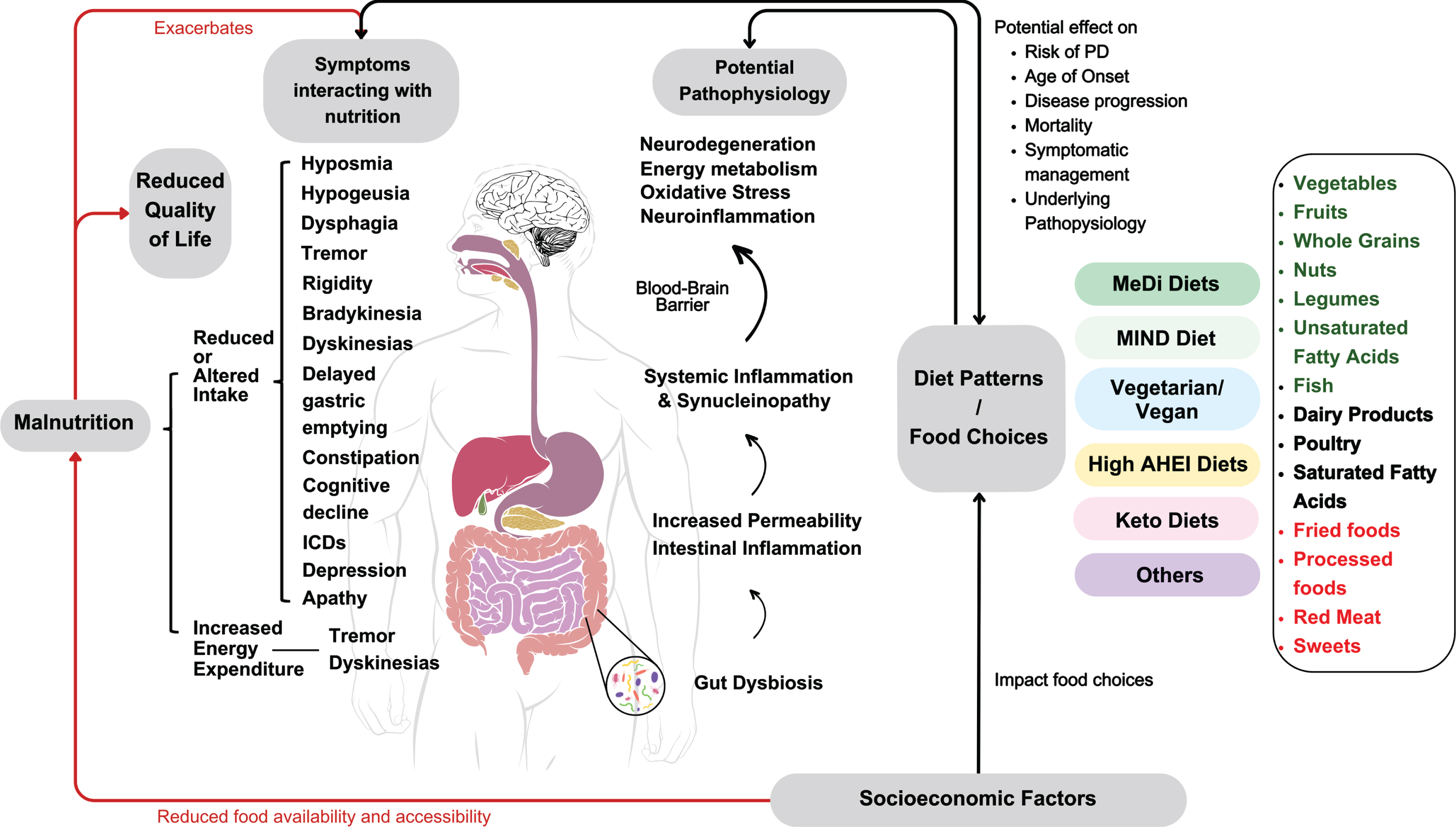
Summary of the complex interactions of dietary patterns and food choices with socioeconomic factors, PD-related malnutrition, disease pathophysiology, symptoms and quality of life.
Where dietary patterns are concerned, the strongest evidence supports adherence to mostly plant-based, MIND and MeDi-style diets in PD, whereas the potential role of ketogenic diets is still unclear. While RCT data is limited, MIND and MeDi diets are believed to be generally safe and beneficial for overall health, and their adherence predicts reduced risk of prodromal and manifest PD [22, 28], older age of onset [18], reduced disease severity [11, 12], progression [28], and self-reported symptom burden in PD [27]. Higher scores on the related AHEI are strongly associated with lower mortality in PD [16]. Preliminary, short-term evidence suggests potential benefits of ketogenic diets in PD [10, 40], the safety and feasibility of these high-fat low-carbohydrate diets have yet to be adequately studied in PD, though. In practical terms, KD may be challenging to follow due to its restrictions on grains, sweets, and fruits. Therefore, ketone supplements and precursors, such as medium-chain triglyceride supplements, may be used to promote ketosis without rigorous limitations on carbohydrates. Intermittent fasting has been proposed as an alternative strategy to target bioenergetic deficits in PD; however, no interventional trials have yet been published to examine their safety, feasibility or efficacy to date [91]. Regardless of the dietary pattern followed, protein-redistribution diets may help to minimize motor fluctuations, though the safety of these diets with respect to weight maintenance and lean muscle mass preservation is an active area of investigation [6, 42].
Evidence for the effects of particular food groups on PD incidence, progression and symptomatology is similarly mixed, with the majority of work involving longitudinal observational studies. Such studies often report differences in PD incidence over several decades based on stratification according to dietary factors at baseline. One limitation in the interpretation of these studies is thus the possibility that participants’ dietary composition may have changed substantially over the follow-up period from their baseline state, which would reduce the strength of associations. Once PD is manifest, adherence to a healthy diet such as the AHEI is associated with reduced mortality during follow-up and a diet based on PROs is associated with slower disease progression, respectively [16, 47]. Several epidemiological studies have linked higher dairy consumption to an increased risk of PD, though it remains unclear whether this applies to all dairy products or specific groups only [17, 43–47]. Findings regarding the relationship of alcohol with PD risk are inconclusive, where the consumption of some alcohol compared to abstinence is potentially beneficial, and the moderate consumption of wine is frequently part of the MeDi [47, 52]; however, the possibility of reverse causation cannot be excluded, as reduced alcohol/drug consumption may represent a feature of a more risk-averse personality type associated with PD [92]. There are differences between food groups included in different MeDi diets and the role of items such as poultry, or potatoes remains to be further explored. In addition to applying existing dietary rating instruments originally developed for other conditions to PD cohorts, data-driven approaches should identify dietary patterns associated with better PD outcomes.
Limited RCTs suggest that dietary supplementation with vitamin E and omega-3 fatty acids may reduce the risk of PD, while citicoline may reduce motor and cognitive symptoms. Vitamin C, B6, B12 and folate supplementation may be of benefit in patients who are on levodopa [42, 93] although there is a paucity of RCTs. There is insufficient evidence for the potential role of vitamin D and B1 [62, 75]. Future studies into vitamin supplementation should take baseline levels into consideration and target those with baseline deficiencies in a move towards personalized medicine.
There are potential safety concerns regarding the use of Mucuna pruriens as an adjuvant therapy [87] but in low-resource settings, Mucuna pruriens might be a valuable alternative to levodopa.
Summary of current evidence for nutritional interventions in Parkinson’s Disease
Two RCTs have established multi-strain probiotics as useful therapies for the treatment of PD-associated constipation [80, 81] and emerging evidence from a 2023 meta-analysis suggests that probiotics may reduce depression, motor and non-motor symptoms in PwP [79]. However, findings must be interpreted in light of significant heterogeneity in the bacterial strains, dosages, treatment durations and methods of administration between included trials. Most current probiotics consist of Bifidobacteria and Lactobacillus strains [94], which are elevated in PwP [95]. It is unclear whether single- or multi-strain probiotics offer greater benefits [96], and how the mode of delivery (ex. tablets, capsules, powdered sachets, yoghurts, and fermented milk drinks) affects bacterial stability, viability and subsequent colonization in the gut [97] and how concurrent diet might influence probiotic efficacy. Six trials of probiotics targeting depression, anxiety, gut health, constipation, and disease severity in PD are currently registered as active in on clinicaltrials.gov (NCT04871464; NCT05576818; NCT05146921; NCT04293159; NCT03968133; NCT05568498). The results of these trials will provide critical information regarding the indications for probiotic supplementation and their efficacy in PD.
Nutritional interventions are of great interest to PwP, as they provide an opportunity for self-management and empowerment, are generally low-risk, and can be beneficial for the treatment and prevention of a wide range of health conditions [98]. However, several barriers to dietary modification in PD need to be addressed: cultural considerations may require adjustment of MeDi-style diets [99], financial constraints can limit access to healthy foods, sex-specific effects of different dietary regimens need to be further investigated, and individualization of dietary regimens is often required to suit the requirements of patients and their care partners/families [98]. Physicians receive limited nutrition education in medical school curricula [100], and dietitians are rarely members of a PwP’s team.
CONCLUSION
PD intersects with nutrition on numerous levels, including pathophysiological mechanisms, motor and non-motor symptoms, medication interactions, disease course, quality of life and socio-economic determinants of health. Observational studies of Mediterranean-type dietary patterns suggest benefits for the risk to develop parkinsonism or PD, age of onset of PD, progression and survival, but RCTs of dietary patterns are urgently needed. The symptomatic management of nutrition-related complications in PD including the significant risk of malnutrition, requires an interdisciplinary team and evidence-supported strategies such as protein-redistribution diets. Nutritional guidelines in PD, training in nutrition for medical students [100] and physicians and access to dietitians trained in PD are necessary steps to integrate nutritional strategies into routine PD care while empowering PwP with a generally low-risk but potentially crucial self-management tool.
ACKNOWLEDGMENTS
The authors thank the following for their support: SAC is supported by the Marg Meikle Professorship in Parkinson’s Research (Pacific Parkinson’s Research Institute (PPRI)). KNT is funded by the Canada Graduate Scholarships Master’s (CGS-M) program. JSTL is supported by a Parkinson Canada Graduate Student Award. YNW and JSTL are supported by grants from the Weston Family Foundation. AC is supported by a grant from the Jack and Darlene Poole Foundation.
FUNDING
No external funding was received for this study.
CONFLICT OF INTEREST
The authors report no conflicts of interest in relation to the content of this manuscript. SAC has received grant funding from the Weston Family Foundation and the Pacific Parkinson’s Research Institute to study nutritional interventions in Parkinson’s disease.