
Abstract
Background:
Although prior research has established that freezing of gait (FOG) in Parkinson’s disease (PD) is associated with anxiety, only one study to date has directly manipulated anxiety levels to induce FOG.
Objective:
The current study aimed to replicate these previous findings and evaluate whether a seated version of a ‘threat’ virtual reality (VR) paradigm could induce anxiety and provoke FOG.
Methods:
Twenty-four PD patients with FOG were assessed across various threat conditions in both a walking VR paradigm (Experiment 1) and a seated VR paradigm (Experiment 2). Both paradigms manipulated the height (i.e., elevated vs ground) and width (wide vs narrow) of the planks participants were instructed to walk across.
Results:
Across both experiments, the Elevated + Narrow condition provoked significantly greater number of freezing episodes compared to all other conditions. Higher levels of self-reported anxiety were reported during the Elevated+Narrow condition compared to all other conditions in Experiment 1, and compared to the Ground condition in Experiment 2.
Conclusion:
These findings confirm that anxiety contributes to FOG and validates the use of a seated VR threat paradigm for provoking anxiety-related freezing. This enables future studies to combine this paradigm with functional MRI to explore the neural correlates underlying the role of anxiety in FOG.
INTRODUCTION
Freezing of gait (FOG) in Parkinson’s disease (PD) is a common debilitating symptom that is characterised by a sudden episode of gait cessation and an inability to effectively generate forward movement, despite the intention [1]. It is one of the most distressing symptoms of PD, that contributes to a loss of independence, which greatly impacts quality of life [2, 3]. Previous work has highlighted a number of common triggers of FOG including turning, walking through narrow doorways, dual-tasking, step initiation and emotional stress [4]. In addition, recent evidence has suggested that the presence of anxiety may be a predictor for those patients who go on to develop FOG in PD [5].
Stress and anxiety has been suggested to ‘set the stage’ for FOG to occur [6]. Support for this conceptual model was initially shown with panic attacks being reported before and during FOG episodes [7]. Both changes in heart rate and skin conductance are widely used indicators of autonomic nervous system (ANS) activation, which can be observed when anxiety is experienced [8]. Such physiological markers of anxiety have been reported prior to and during episodes of FOG [9, 10]. Importantly, since these psychophysiological changes were observed before the occurrence of FOG episodes, one could postulate that anxiety may represent a causal factor in the phenomenon.
Despite this body of evidence, only one study to date has been conducted to investigate the causal relationship between anxiety and FOG by directly manipulating threat [11]. In this study, PD patients walked in an immersive virtual reality (VR) environment with two levels of threat. Participants were instructed to walk across either a plank that was located on the ground or an elevated plank that was above a deep pit [11]. Results from this study showed that the high threat condition (i.e., walking across an elevated plank) elicited higher self-reported levels of anxiety, elevated skin conductance levels, as well as more severe and more frequent freezing episodes compared to the low threat condition (i.e., walking across a plank on the ground). As threat was directly manipulated to induce anxiety, results from this study allowed the inference of a causal relationship between anxiety and FOG [11]. However, those investigators were not able to evaluate whether anxiety levels could be further manipulated by the width of the elevated plank. Furthermore, the design of this VR walking paradigm did not enable the investigation of the neural mechanisms that underlie this phenomenon. Thus, the first experiment in this study aimed to replicate these previous findings and to extend our understanding of the factors driving anxiety by manipulating the width of the plank (in addition to the height), in a walking VR paradigm.
The second component of the current study sought to explore the role of a seated VR ‘gait’ paradigm given the potential to combine this with functional neuroimaging (fMRI) to identify the neural underpinnings of anxiety-related FOG. Our group has previously reported the use of a validated seated VR paradigm that can reproduce the key aspects of freezing and gait disturbance allowing for a number of novel neuroimaging and neurophysiological insights [12–17]. Most significantly, the seated VR paradigm has shown correlations between the severity and duration of freezing episodes compared to actual FOG during timed-up-and-go assessments [16, 18]. However, no studies to date have investigated a threat manipulation to modulate anxiety using this approach.
Thus, the second experiment in this study aimed to evaluate whether a seated VR gait paradigm, where patients move through the environment using foot pedals, could induce anxiety and provoke freezing (as well as ‘gait’ disturbance) by manipulating threat level.
It was hypothesised that higher levels of anxiety and greater amounts of freezing would be provoked as a function of increased threat in both the walking VR experiment and seated VR experiment.
MATERIALS AND METHODS
Participants
Twenty-four patients with PD and FOG were recruited from the Parkinson’s Disease Research Clinic at the Brain and Mind Centre in Sydney, Australia. All patients met the inclusion criteria of i) a prior diagnosis of idiopathic PD by a trained neurologist (SJGL), and ii) FOG was confirmed through a history of FOG, previous clinical observation and a positive response to item 3 of the FOG Questionnaire (FOG-Q) [19]. Patients were excluded if they had other neurological disorders, severe head tremor, hearing loss or significant visual impairment that would impact their ability to wear a head-mounted display (HMD). To maximise the amount of FOG provoked in the study, all patients were assessed in their ‘OFF’ dopaminergic medication state, where ‘OFF’ was defined as withdrawing from their anti-Parkinson’s medication for at least 12 hours (and at least 24 hours for dopamine agonists). Ethical approval was obtained by the University of Sydney Human Research Ethics Committee, and all participants provided signed consent prior to participating in the study.
Participants completed a variety of anxiety measures prior to completing the experimental protocol including: i) Parkinson Anxiety Scale (PAS) [20]; ii) State-Trait Anxiety Inventory (STAI) [21]; iii) the Hospital Anxiety and Depression Scale (HADS) [22]. A trained clinician administered the Movement Disorder Society’s Unified Parkinson’s Disease Rating Scale Section III (UPDRS III), a gold standard assessment of PD’s motor symptom severity to all participants [23], as well as the Hoehn and Yahr scale [24]. The Montreal Cognitive Assessment (MOCA) [25] was also administered to assess general cognitive function.
Experiment 1: Walking virtual reality task
Experimental apparatus and protocol
Participants wore an HMD, HTC Vive (HTC Corp., Taiwan & Valve Corp., Washington, US) that delivered a virtual environment, developed onsite using Steam (Valve Corp., WA, US). The VR paradigm ran on a Dell Alienware portable computer (Dell Technologies Inc., TX, US) with a NVIDIA GeForce GTX 1080MQ graphics card (Nvidia, Santa Clara, CA, USA), streamed to the HMD in real-time (at a refresh rate of 90 Hz). The HMD weighed 470g and featured two 3.6” screens delivering a resolution of 1080x1200 full-colour pixels per eye and a 110-degree field of view. It was firmly secured on the participants’ face to prevent real-world vision; this was done to increase their immersion in the VR environment. The visual focus and eye width of the HMD was adjusted for each participant to ensure they had clear stereoscopic visual perception.
Two mounted Vive VR Base Stations (HTC Corp.) were positioned at the corners of the testing room, to capture motion tracking, which allowed real-time updates of participants’ position within the virtual environment. A 6-metre pressure sensor gait mat, ZENO™ Walkway (Protokinetics©, PA, USA), was used to record participants’ walking patterns. The walkway was mapped onto the length and location of the VR plank. A video camera was set up at the corner of the gait mat to record the entire walk, and to capture FOG episodes. A FOG episode was defined as an unintended interruption of gait where the subject did not make an effective step forward [1]. A freezing episode was considered to be finished when the subject made at least two consecutive normal steps after freezing [26]. Episodes of freezing and the average duration of freezing were identified on video, and manually annotated using ELAN™ software (The Language Archive, Nijimegen, Netherlands, [7, 8]).
Participants’ step time and step time variability (Coefficient of Variation-CV) during the walking tasks were obtained from the pressure sensitive gait mat. These temporal gait measures were recorded and processed using the Protokinetics Movement Analysis Software (PKMAS). The reason that only temporal outcome measures of gait were selected was due to the nature of the seated paradigm, which outputs footstep latency (FSL; surrogate for step time) and footstep latency variability (CV). Thus, temporal measures were examined to enable comparisons to be made between the walking and the seated VR paradigm.
The experimental protocol for the walking VR paradigm consisted of four conditions, a Ground + Wide, Ground + Narrow, Elevated + Wide and Elevated + Narrow (Fig. 1A). Each trial consisted of a 12 m walk in total, where participants walked 6 m from the starting position to the end of the plank, and then returned from the end to the starting position. They were instructed to commence walking at the sound of a tone that was elicited manually when the experimenter pressed a button. The conditions were presented randomly to the participants with a rest time of no less than 30 s given between each trial to prevent carry over effects. Each participant completed 24 trials. Upon returning to the start position after every trial, self-assessment manikins (SAM) were presented within the VR environment and participants were asked to rate their anxiety level on that trial, in keeping with previous studies [11]. The experimental conditions were selected to induce threat, as previous studies have found higher self-reports of fear, anxiety, and postural displacement when they compared elevated surface heights to ground conditions in both PD patients and controls [11, 27–29]. Other studies have found higher postural instability and gait variability when elderly and PD patients walked on a narrow surface compared to a wide surface [30, 31]. As such, the height and width of planks were manipulated to create different levels of threat.
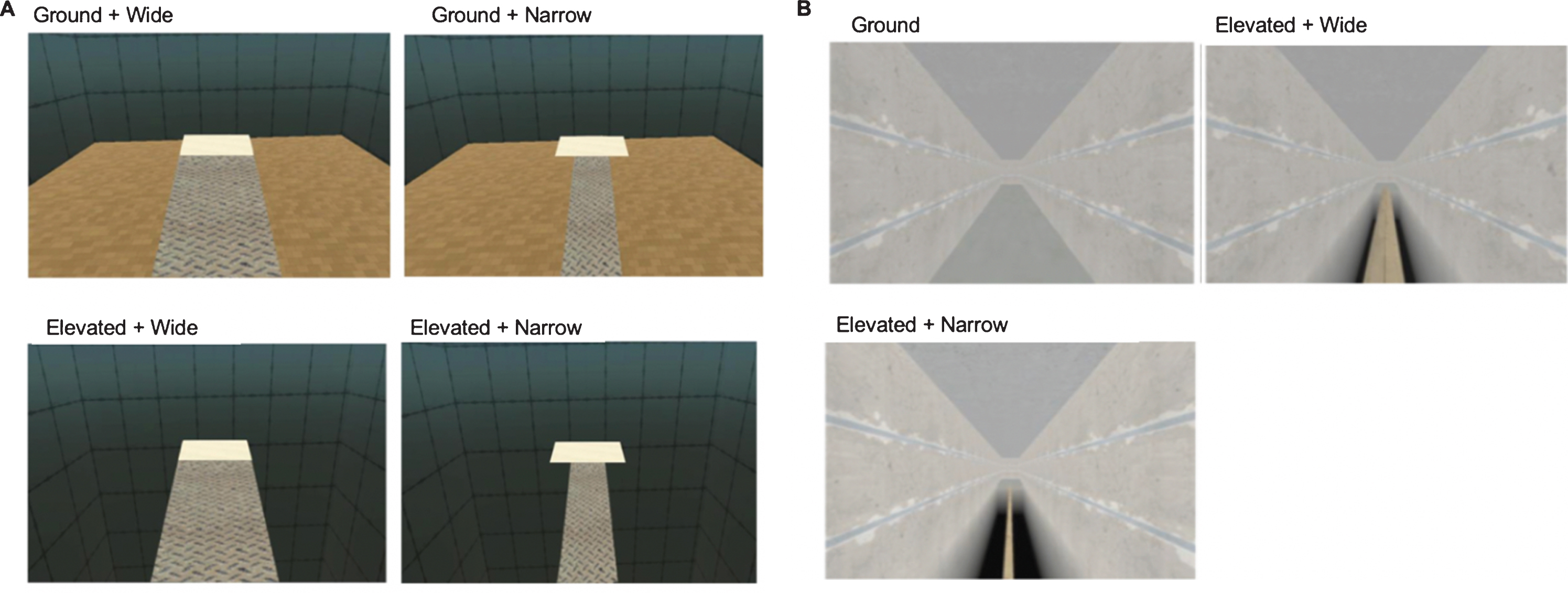
A) This figure depicts the four different threat conditions in the walking VR paradigm (Experiment 1): (i) Ground + Wide: a wide plank located on the ground, (ii) Ground + Narrow: a narrow plank located on the ground (iii) Elevated + Wide: a wide plank surrounded by a deep pit, and (iv) Elevated + Narrow: a narrow plank surrounded by a deep pit. B) This figure depicts the three different threat conditions in the seated VR paradigm (Experiment 2): (i) Ground (ii) Elevated + Wide: wide plank, (iii) Elevated + Narrow: narrow plank. Participants navigated through three different levels of threat using foot pedals. The upcoming threat condition was hidden from the participants until they had made a turn along the corridor.
Outcome measures
The primary outcome measures were the average number of FOG episodes (#FOG) provoked and the percentage of the trial spent frozen (%FOG). To verify that the threat manipulation was indeed successful at increasing anxiety in participants, levels of anxiety were reported through the use of self-assessment manikins as a secondary outcome measure. Additionally, step time and step time variability have been identified as precursors to full-blown FOG episodes, thus these gait parameters were also examined as secondary outcome measures.
Statistical analysis
Repeated measures ANOVAs (2 height conditions x 2 width conditions) were conducted in Experiment 1 to investigate the effect of the threat manipulation on FOG (#FOG and %FOG), self-reported anxiety, as well as step time and step time variability outcomes during the walking VR paradigm. Greenhouse-Geisser corrections were used where the data violated Mauchly’s test of sphericity. Significant interactions were investigated further with paired sample t-test post-hoc analyses. Two participants could not complete the Narrow+Elevated condition and thus were excluded from this analysis. Of these two participants, one person elected to opt out of the entire study when too much freezing occurred during the trial, while the other was able to complete the seated protocol in Experiment 2 (hence N = 23 in Table 1).
Patient Characteristics
MoCA, Montreal Cognitive Assessment; HADS, Hospital Depression Scale; PAS, Parkinson’s Anxiety Scale; MDS-UPDRS, Unified Parkinson’s Disease Rating Scale; H&Y, Hoehn and Yahr Scale; FOGQ, FOG Questionnaire.
Experiment 2: Seated virtual reality task
Experimental apparatus and protocol
The display within the seated virtual reality gait paradigm is shown in Fig. 1B. The VR paradigm was projected from a Dell laptop (Dell Technologies Inc., TX, US) onto a 55-inch Samsung Smart TV (Samsung Electronics Co., Ltd, Suwon, Korea). Participants were seated 2 m in front of the large TV that displayed the seated version of the VR paradigm and pedals were positioned beneath their feet. Alternate depression of the pedals (i.e., ‘left-right-left-right’), encoded binary information that corresponded to left and right “footsteps” in the virtual environment.
Footstep latency was calculated as the time in seconds between two subsequent depressions of the foot pedal. Previously, in the seated VR paradigm, an episode of freezing was defined as twice the modal footstep latency (FSL) [18]. However, when we applied this metric to the current data set, this definition was overly sensitive, capturing slow steps rather than freezing episodes. Upon plotting and reviewing each participants’ footstep latency histogram, we found a bimodal distribution similar to prior work. Therefore, in order to accurately capture freezing episodes, we adopted a more conservative approach, where we defined a freezing episode as any period where the time between two alternate footsteps was greater than twice the mean footstep latency of the whole trial. In our measure of footstep latency and CV footstep latency, freezing episodes were removed to provide a measurement that captured normal walking.
The experimental protocol for the seated paradigm had three conditions: Ground, Elevated + Wide, Elevated + Narrow ‘walking’ (Fig. 1B). Participants navigated through these conditions continuously with alternate depression of the foot pedals, where each condition would be visible after the participant made a turn along the corridor. Notably, participants were unable to control the position of their feet on the plank, nor their step width, step length or velocity. They only had control over the timing of their steps by depressing the foot pedals, which progressed them forward (or around a corner) in a standard manner and kept them centred in the environment. In sum, the seated VR task could be successfully completed with simply sequential foot pedal depressions. No behavioural changes were needed to navigate the threat conditions or turns.
Participants initiated their foot tapping when a ‘WALK’ cue was presented in the VR and stopped when an ‘END’ cue was given. Each trial lasted for five minutes of continuous walking and participants completed four trials in total with a minimum two-minute break between each session. The conditions were presented in a randomised order of exposure and participants encountered an average of 10 randomised conditions in each trial. To obtain a measure of subjective anxiety, patients rated their level of symptoms on self-assessment manikins every minute during each of the three threat conditions [11, 32]. To aid the participant’s immersion in the seated virtual environment, a subtle first-person mediolateral sway was added to all elevated conditions to better simulate ‘walking’ across an elevated plank, despite being seated. Since the goal of the seated paradigm was to induce anxiety and provoke FOG, conditions included were designed to elicit the most versus least amount of anxiety given the constraints that participants would be performing this task seated, and threat to posture would be severely hampered. Thus, the ground conditions were combined, and a narrow and very narrow plank were selected to manipulate threat and provoke anxiety. It is noteworthy that in the walking paradigm, no prominent differences in gait variability, FOG and anxiety were observed between the two ground conditions with different widths.
Outcome measures
The primary outcome measures for the seated VR task were the average number of freezing episodes (#FOG) and percentage of the trial spent frozen (%FOG). Anxiety levels recorded through the self-assessment manikins were used as a secondary outcome measure. Finally, step time (footstep latency) [33] and step time variability, which is the coefficient of variation (CV) of footstep latency were also examined as secondary outcome measures in keeping with our previous work utilising a seated VR gait paradigm [18].
Statistical analysis
One way repeated measures ANOVAs (3 threat conditions) were conducted in Experiment 2, to investigate the effect of the threat manipulation on freezing, self-reported anxiety, as well as ‘gait’ during the seated VR paradigms. Greenhouse-Geisser corrections were used where the data violated Mauchly’s test of sphericity. Significant interactions were investigated further with paired sample t-test post-hoc analyses. Two participants were unable to complete the seated protocol in Experiment 2 due to technical difficulties with the foot pedals, and thus were excluded from this analysis.
RESULTS
Sample characteristics
As shown in Table 1, MoCA scores were within the range of mild cognitive impairment with four patients showing no cognitive impairment. No patients satisfied diagnostic criteria for PD dementia. Depression scores on the HADS-D rating scale were within the normal range. Participants were moderately anxious, and on average reported anxiety total scores > 13, which has been previously noted as an optimal cut-off score for dichotomization of PD patients with and without an anxiety disorder [23]. All but three participants exhibited freezing of gait in the walking VR paradigm (Experiment 1) and all participants experienced “freezing behaviour” in the seated VR paradigm (Experiment 2).
Experiment 1: Walking virtual reality task
Self-reported anxiety
A significant interaction was found between height and width for self-reported anxiety using the self-assessment manikins (SAM) (F(1,20) = 28.55, p < 0.001) (Fig. 2). Post hoc tests revealed significantly higher reports of anxiety during the Elevated + Narrow condition compared to all other conditions. Participants also reported significantly higher levels of anxiety in the Elevated + Wide compared to Ground + Wide (t(20) = –4.003, p = 0.001), as well as higher anxiety reports in the Ground + Narrow condition compared to Ground + Wide, (t(22) = –4.453, p < 0.001).
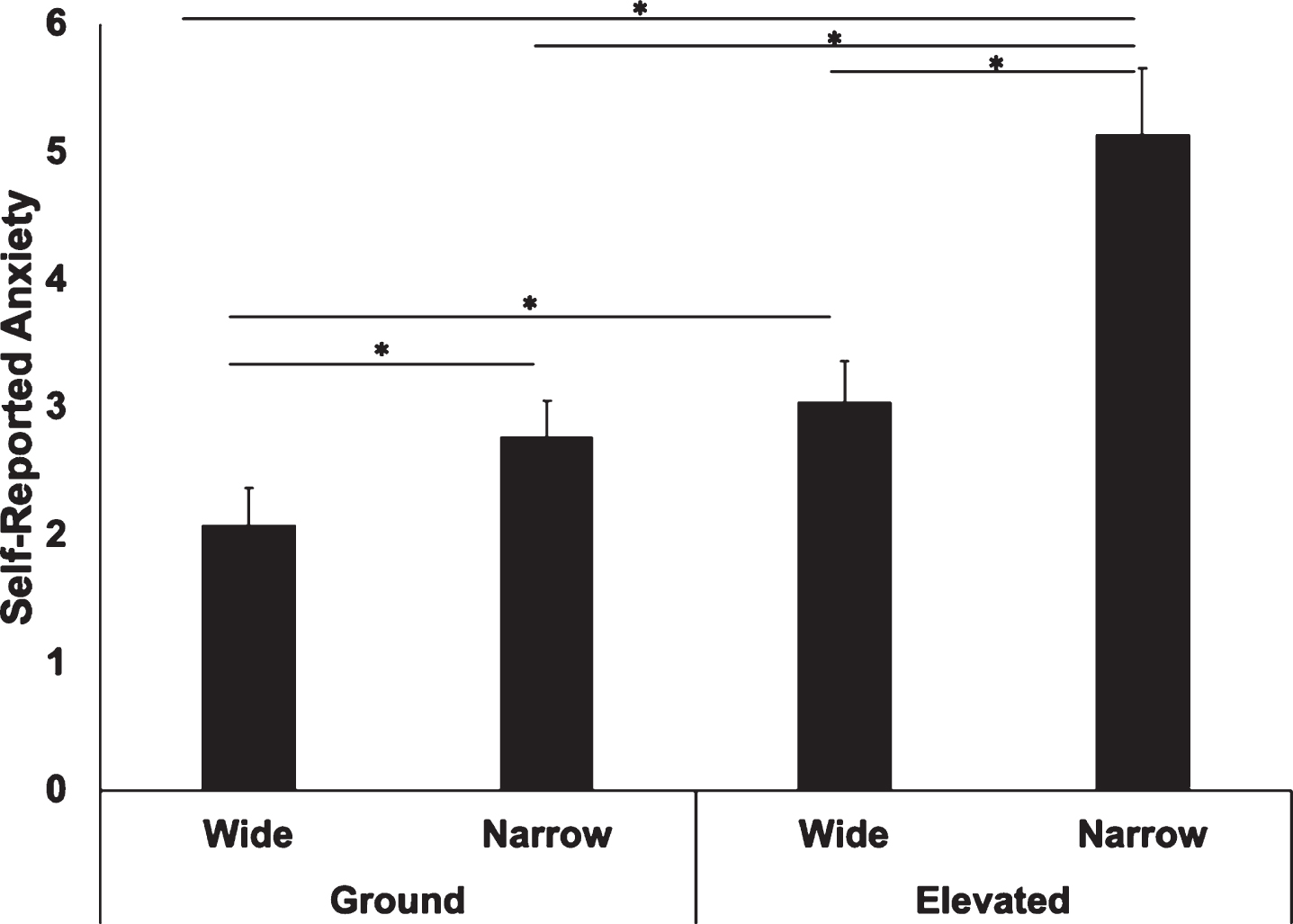
Comparison of self-reported anxiety between the four threat conditions in the walking paradigm (Experiment 1). Participants reported higher levels of anxiety using the SAM during the Elevated + Narrow plank compared to all other conditions. The Elevated + Wide condition also had higher reports of anxiety when compared to the Ground + Wide condition. *p < 0.05, error bars represent SEM.
Freezing of gait
A significant interaction between height and width was found for the number of FOG episodes (F(1,20) = 11.23, p = 0.003) (Fig. 3A). Post hoc analysis revealed that participants experienced a significantly greater number of FOG episodes during the Elevated + Narrow compared to the Elevated + Wide condition (t(20) = –4.16, p < 0.001), Ground + Narrow condition, (t(21) = –3.99, p = 0.001), and Ground + Wide condition (t(21) = –3.93, p = 0.001). A significant interaction was also found between height and width for the percentage of trial spent frozen (%FOG), (F(1,19) = 6.63, p = 0.019) (Fig. 3B). Post hoc analysis found significantly higher %FOG during the Elevated + Narrow condition compared to all other conditions (Elevated + Wide: (t(20) = –3.85, p = 0.001), Ground + Narrow: (t(20) = –3.15, p = 0.005), Ground + Wide: (t(21) = –3.46, p = 0.002)).
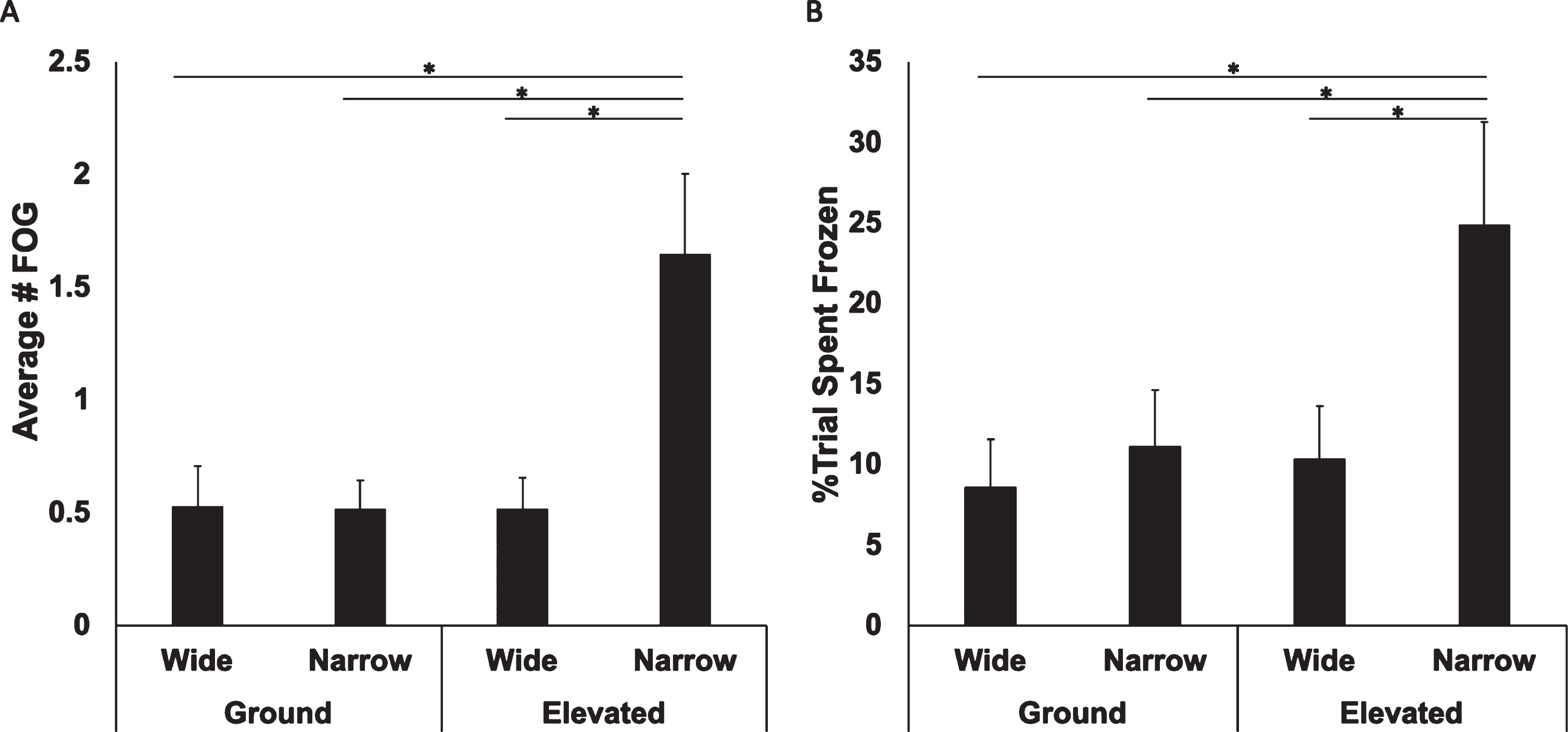
Comparison of freezing of gait between the four threat conditions in the walking paradigm (Experiment 1). A) Participants experienced a greater number of FOG episodes while walking across the Elevated + Narrow plank compared to all other conditions. B) Participants experience a higher percentage of FOG navigating the Elevated + Narrow condition compared to all other conditions. *p < 0.05, error bars represent SEM.
Gait parameters
A main effect of height was found for step time variability (F(1,18) = 7.44, p = 0.014), which showed that all patients displayed greater step time variability whilst walking across the elevated compared to the ground planks. While no significant effects were found for step time.
Correlations between SAM and FOG outcome measures
Significant correlations were obtained between the SAM scores and the Number of FOG for Ground + Wide (rs(23) = 0.61, p = 0.002), Ground + Narrow (rs(23) = 0.61, p = 0.002), and Elevated + Narrow conditions (rs(22) = 0.65, p = 0.001), as well as for %FOG for Ground + Wide (rs(23) = 0.61, p = 0.002), Ground + Narrow (rs(22) = 0.64, p = 0.001), Elevated + Wide (rs(21) = 0.47, p = 0.03), Elevated + Narrow (rs(22) = 0.73, p < 0.001) (Fig. 4). Freezing evoked in the laboratory during Experiment 1 were also significantly positively correlated with clinical measures of freezing (e.g., FOGQ total score - see Supplementary Table 1). There were no significant correlations between SAM ratings and PAS total score in Experiment 1.
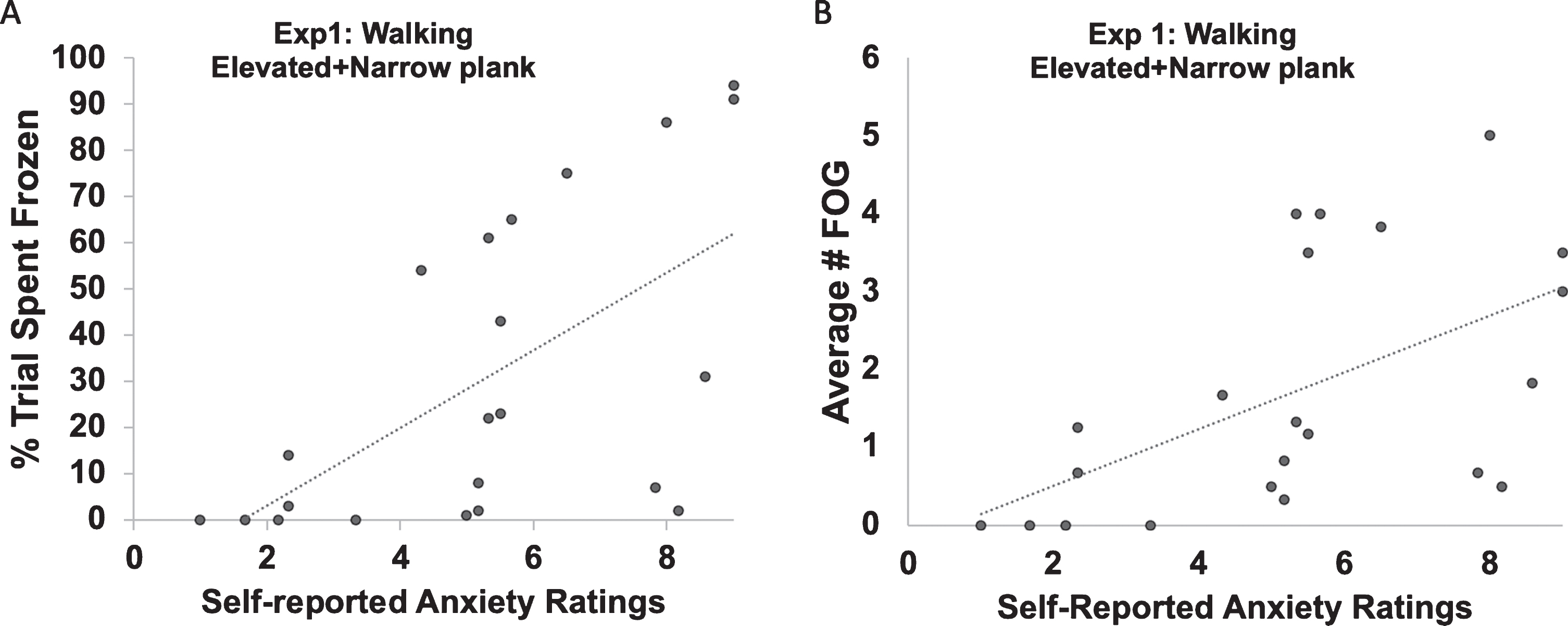
Scatterplot depicting a significant positive correlation between the Self-reported anxiety measure (SAM) in the Elevated + Narrow conditions during the walking VR task and both the (A) Percentage of trial spent frozen and (B) Average number of freezing of gait episodes.
Experiment 2: Seated virtual reality task
Self-reported anxiety
A significant main effect of threat condition was found for self-reported anxiety levels (F(1.33,26.62) = 4.04, p = 0.044). Post hoc analysis revealed that participants reported significantly higher anxiety scores during the Elevated + Narrow (t(20) = –2.48, p = 0.022) and Elevated + Wide (t(20) = –3.08, p = 0.006) conditions compared to the Ground condition. No significant differences were found between the wide and narrow elevated planks (see Fig. 5A).
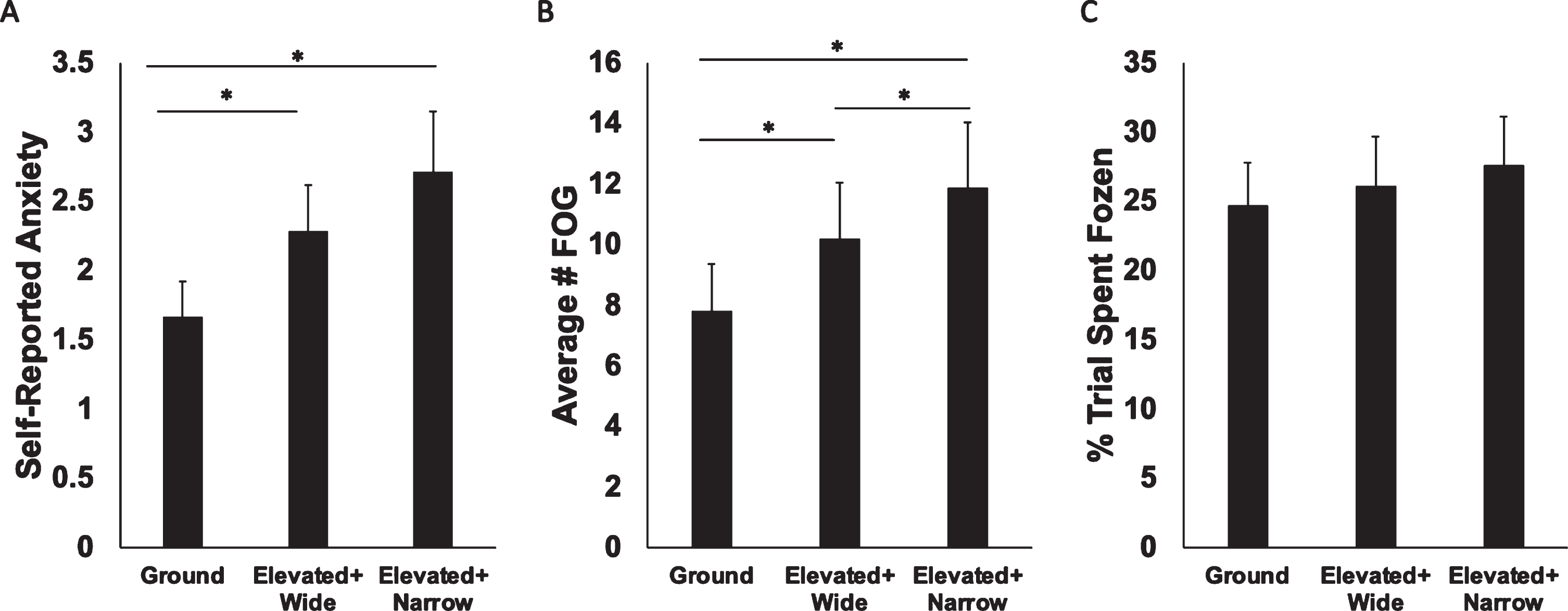
Main effect of conditions in self-reported anxiety and freezing in the seated VR paradigm (Experiment 2). A) Participants reported significantly higher anxiety levels while navigating both Elevated + Wide and Elevated + Narrow planks compared to the Ground condition. B) Participants experienced a greater number of FOG episodes while navigating both Elevated conditions compared to the Ground condition. More frequent FOG episodes were also elicited during the Elevated + Narrow condition compared to the Elevated + Wide condition. C) No significant differences were found between conditions for the percentage of trial spent frozen. *p < 0.05, error bars represent SEM.
Freezing of gait
A significant main effect of condition was found for the number of FOG episodes in the seated paradigm (F(2,40) = 10.99, p < 0.001). Post hoc tests revealed that both Elevated + Narrow (t(20) = –4.68, p < 0.001) and Elevated + Wide (t(20) = –2.42, p = 0.025) conditions elicited a significantly greater number of FOG episodes compared to the Ground condition, and Elevated + Narrow planks also elicited more FOG episodes compared to the Elevated + Wide condition (t(20) = –2.27, p = 0.034) (Fig. 5B). There was no significant effect of condition on percentage of trial spent frozen, (F(2,40) = 0.98, p = 0.39) (Fig. 5C).
Seated paradigm ‘gait’ parameters
A main effect of condition did not reach significance for footstep latency (step time) (F(2,40) = 2.87, p = 0.069). There was also no significant main effect of condition for variability in footstep latency (F(2,40) = 2.53, p = 0.093).
Correlations between SAM and FOG outcome measures
No significant correlations were found between the seated SAM and the outcomes for FOG in the seated paradigm from Experiment 2. There was a significant relationship between the freezing evoked in the lab during Experiment 2 and clinical measures of freezing. Specifically, FOGQ-3 score and %FOG were associated during the Ground condition (rs(21) = 0.547, p = 0.01), Elevated + Wide condition (rs(21) = 0.523, p = 0.015), and Elevated + Narrow condition (rs(21) = 0.556, p = 0.009) (see Supplementary Table 3 for further details). There was also a significant positive correlation between the PAS total and the seated SAM ratings during the Elevated + Narrow plank (rs(21) = 0.47, p = 0.025) in Experiment 2.
Correlations between walking and seated paradigm
As shown in Fig. 6, Spearman’s correlation revealed a positive correlation for the percentage of trial spent frozen (%FOG) between the seated Elevated + Narrow condition and the walking Elevated + Narrow condition (r s (20) = 0.427, p = 0.03).
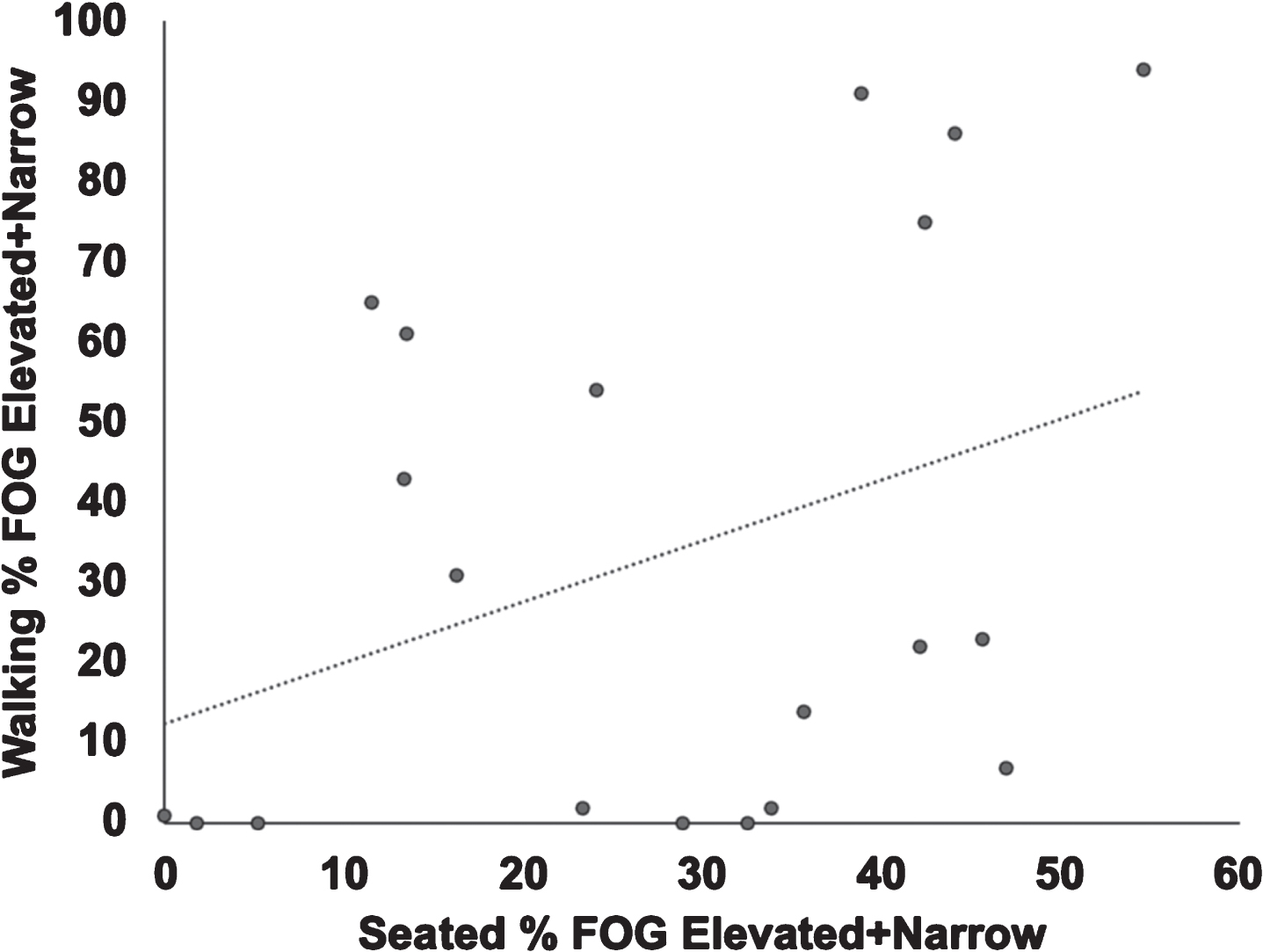
Scatterplot depicting a significant positive correlation between the percentage of time spent frozen while navigating the Elevated + Narrow plank during the seated VR task (Experiment 2) compared to percentage of trial spent frozen while navigating the Elevated + Narrow plank during the walking VR paradigm (Experiment 1).
DISCUSSION
Findings observed in Experiment 1 were consistent with previous work showing that higher levels of anxiety, more frequent and severe FOG, as well as greater step time variability were elicited when participants were asked to walk in VR across an elevated narrow plank compared to a narrow plank located on the ground [11]. To our knowledge, only one study to date has directly manipulated threat to establish this causal relationship between anxiety and FOG [11]. Thus, the current findings provide confirmatory evidence in a distinct sample of freezers, that FOG can be provoked by height-induced threat which elicits significantly greater levels of anxiety. Additionally, the Elevated + Narrow condition from the walking VR paradigm had two FOG outcome measures, namely the number of freezing of gait episodes and the percentage of trial spent frozen that were moderately correlated with the self-reported anxiety measure SAM during the Elevated + Narrow condition. This association increases the validity of the relationship between the high threat condition of the walking VR paradigm and anxiety. These results suggest that anxiety is an important contributor to FOG in PD.
We also extended this work by showing that the width of the plank contributes significantly to the threat level during the walking VR paradigm in Experiment 1, since the Elevated + Wide plank (which had not been investigated previously) did not provoke FOG beyond that of the Ground planks. One reason for this result may be that the Elevated + Wide plank simply did not provoke enough anxiety (see Supplementary Table 1 - average SAM rating: 3 out of 9) compared to the Elevated + Narrow plank (average SAM rating: 5 out of 9).
The objective of Experiment 2 was to evaluate whether elevated planks could induce greater anxiety, as well as provoke increased freezing episodes even when seated, to determine whether this virtual plank paradigm might be useful to investigate the neural underpinnings of anxiety-related FOG in future fMRI studies. Although the reported anxiety levels during the seated VR paradigm were less, given the threat to participants’ posture was minimal because they were seated, what is striking is that the differences in anxiety ratings and freezing behaviour remained significantly greater during the high threat condition (Elevated + Narrow plank) compared to the low threat condition (Ground level) even though participants were seated. Furthermore, correlational analysis revealed that the severity of freezing in the Elevated + Narrow condition of the walking VR paradigm (Experiment 1) was associated with the severity of freezing in the Elevated + Narrow condition of the seated VR paradigm (Experiment 2). It is also notable that Experiment 1 was completed prior to Experiment 2 on the same testing day. Therefore, another reason that anxiety ratings may have been less in Experiment 2 is because the seated version was performed after the more immersive walking paradigm was completed. Future research is needed to determine whether performing the seated VR paradigm in a new sample would be associated with higher anxiety ratings than in the current study. This is an important limitation which might have led to conservative reports of anxiety in the seated paradigm. Taken together, our findings suggest that the seated VR plank paradigm is capable of eliciting comparable freezing phenomena that can be provoked with the walking VR plank paradigm. This work will enable future studies to investigate the neural correlates of anxiety-related FOG with fMRI for the first time, and examine how periods of greater anxiety change brain network topology in Freezers and make an individual more vulnerable to frequent FOG.
Considerations and limitations
Importantly, whilst the Elevated + Narrow plank condition was able to reliably elicit higher levels of anxiety and freezing compared to the other threat conditions, two participants were unable to complete this condition in the walking VR paradigm, and one of these particiapnts elected to opt out of the entire study when too much freezing occurred during the trial. In contrast, most participants were able to complete the Elevated + Narrow condition during the seated VR paradigm, which highlights that although the paradigm was successful in provoking anxiety and FOG episodes, it does not elicit the same level of postural threat nor have the same implications for falling. Thus, especially for severe freezers, the seated VR paradigm represents a valid alternative to the walking VR paradigm, as there is no actual risk of falling down and participants are more willing to try out higher threat inducing conditions. This observation offers potential benefits to future fMRI studies as well as potential safe rehabilitation strategies.
It should be noted that the first-person mediolateral sway of 3 degrees was added only to the elevated conditions of the seated VR paradigm to create a more immersive experience that mimics actual walking on an elevated plank. However, this sway was not added to ground conditions and could therefore potentially be a confounding factor that contributed to the increase in freezing of gait instead of the anxiety elicited from the threat condition. Further research assessing sway during ground walking in the seated VR paradigm should be considered to determine the role of sway in FOG.
The current results showed that both height and width played a role in eliciting varying degrees of anxiety in participants during the walking VR paradigm. Although the Elevated + Narrow condition during the walking VR paradigm reliably obtained significantly higher levels of self-reported anxiety ratings, as well as a greater number of FOG episodes and more severe FOG (measured by %FOG) compared to all other conditions, this was not the case for the seated VR paradigm. Walking across the Elevated planks, regardless of the width (Narrow vs Wide), led to increased levels of self-reported anxiety and a greater number of freezing episodes. One reason for this is that we opted for relatively narrower plank widths in the seated condition, in an effort to maintain the feeling of threat given the absence of true postural threat when performing the task seated. Therefore, in the seated VR paradigm, height was the main driver of threat, where elevated heights elicited more anxiety and freezing episodes regardless of width.
Despite the similarities across paradigms, some other differences were also noted. In the seated VR paradigm, no effect of condition was found for foot step latency variability. However, in the walking VR paradigm, there was a significant main effect of height, where the elevated conditions elicited greater step time variability than the ground conditions. Indeed, participants showed an increase in foot step latency during the elevated narrow condition compared to the ground, similar to that found in the walking VR paradigm, however this was not statistically significant (See Supplementary Tables 1 and 2). One possible explanation could be that step time variability stems from dynamically controlling movement. As dynamic control of walking was reduced when performing the seated version of the VR paradigm the effect on step time variability (i.e., variability in footstep latency) was reduced.
Another difference was observed in the percentage of trial spent frozen, where participants in the walking VR paradigm spent a greater percentage of the trial frozen when navigating the Elevated + Narrow compared to the Ground + Wide condition. However, in the seated VR paradigm, percentage of trial spent frozen did not significantly differ between conditions, despite the elevated conditions having more frequent FOG episodes than the ground condition. One consideration that may explain this difference, is that discrete trials were carried out in the walking VR paradigm, whereas participants ‘walked’ continuously in the seated VR paradigm, encountering various threat conditions en route. This difference in protocols was to optimise an event-related design for future fMRI studies that could utilise the seated VR paradigm. It is possible that continuous compared to discrete trial durations may have washed out these effects. It is worth noting that during the seated VR paradigm, participants displayed strikingly similar %FOG when navigating the Elevated + Narrow (27.7%) as they did when navigating the Elevated + Narrow plank during the walking VR paradigm (24.9%) (See Supplementary Table 2). Moreover, it should be emphasized that the %FOG during the seated VR task was correlated with the %FOG during the walking task. Thus, significant differences were not detected in the seated VR paradigm because of the high amount of FOG during the Ground condition at baseline. This may have been caused by carry over effects of previous anxiety-provoking trials, which were eliminated with the 30 s breaks during the discrete trials. Future research using the seated VR paradigm should consider monitoring physiological changes such as heart rate or skin conductance to determine whether anxiety levels drift throughout the continuous trials. Furthermore, staggering the conditions further apart in time may also reduce these carry-over effects, albeit at the cost of less events over time or by implementing longer scan times.
Implications and future directions
Overall, the height-induced threat manipulation in the seated VR paradigm was successful at inducing anxiety and provoking FOG. Whilst previous fMRI studies have drawn links between increased striato-limbic connectivity in conjunction with deterioration of top-down control by the frontoparietal network (FPN) over the amygdala in freezers at rest [34], as well as increased striato-limbic connectivity during episodes of freezing [12], no studies to date have directly manipulated anxiety to examine the neural underpinnings of anxiety-provoked FOG. Therefore, future studies could now pair this seated VR paradigm with fMRI to further explore how anxiety might ‘set the stage’ for FOG to occur. This understanding may also inform mechanistic explanations for other anxiety-worsened motor symptoms such as PD tremor and dyskinesia [35, 36].
The seated VR paradigm could also be used in psychotherapy for anxiety treatments with older adults (i.e., exposure therapy, graded introduction to higher levels of anxiety inducing contexts), where they could offer exposure to anxiety-inducing conditions without the actual risks of falling [37]. In addition, given that visual feedback is an aspect that has been found to reduce FOG, future studies could incorporate visual feedback into the VR paradigm to investigate the relationship between visual feedback and freezing of gait through cueing.
CONCLUSION
Overall, the threat manipulations were successful in both paradigms, whereby walking across an elevated narrow plank elicited higher levels of anxiety and more frequent freezing compared to less threatening conditions. The seated VR paradigm and the walking VR paradigm both impacted FOG and anxiety measures overall, suggesting that the seated VR paradigm may be a valid substitute for the walking VR paradigm, which in conjunction with functional MRI could explore the neural correlates of anxiety provoked FOG.
CONFLICT OF INTEREST
The authors have no conflict of interests to report.
Footnotes
ACKNOWLEDGMENTS
We would like to thank Mr Simon Wadsworth of Turambar Software for his assistance in developing the virtual reality paradigm and would like to extend our gratitude and appreciation to the patients who participated in our study.
KAEM is supported by a New Investigator Award from Parkinson Canada and the University of Sydney, Brain and Mind Centre Early Career Researcher Development Grant; Professor Lewis is supported by a National Health and Medical Research Council Leadership Fellowship (#1195830).