
Abstract
Background:
Freezing of gait (FOG) in Parkinson’s disease (PD) has been shown to be more frequent in stressful situations, implicating anxiety. Heart rate (HR) has been shown to increase prior to a FOG episode supporting the notion that elevated stress levels may trigger FOG. However, no studies to date have investigated whether elevated HR precedes all subtypes of FOG or only those episodes that are driven by anxiety.
Objective:
The present study sought to investigate whether 1) HR increases prior to FOG episodes in nonspecific environments (Experiment 1), and if 2) HR increases prior to FOG when provoked in high but not low threat environments using a virtual reality paradigm (Experiment 2).
Methods:
In Experiment 1, 10 of 19 participants with PD and FOG (PD + FOG) experienced FOG during a series of walking trials. In Experiment 2, 12 of 23 participants with PD + FOG experienced FOG while walking across an elevated and ground level narrow plank in virtual reality. HR was collected throughout the duration of both experiments, while FOG was quantified by experts using video review and tagging.
Results:
HR significantly increased 2–3 seconds prior to a FOG episode during Experiment 1. In Experiment 2, HR significantly increased 4–6 seconds prior to a FOG episode, specifically while navigating the elevated plank. However, there were no significant increases in HR prior to FOG episodes when participants navigated the ground plank.
Conclusion:
This study extends previous work further demonstrating that increases in HR prior to FOG episodes appear linked to elevated anxiety levels.
INTRODUCTION
Freezing of gait (FOG) in Parkinson’s disease (PD) is characterized by an absence, or significant reduction in forward progression of the feet despite an intention to walk [1]. As such, patients often describe feeling as though their feet are stuck to the floor [2, 3]. The episodic nature of such gait disturbances, means that the patient is often unprepared for the event, making this symptom arguably the most burdensome for patients and caregivers, since it often precipitates falls and can lead to admission to hospital or a nursing home [4, 5].
Although an association between freezing episodes, panic attacks and anxiety was made over a decade ago [6], very little empirical work has been done to examine the relationship between anxiety and FOG. One study by Maidan and colleagues [7] posited that in theory, sympathetic activation due to stress or increased anxiety could explain the increase that had been observed in heart rate (HR) prior to and during freezing episodes. The study reported an increase of 0.7±0.2 bpm in HR in the 3 s interval closer to the initiation of FOG, compared to the 3 s interval earlier. In fact, this increase in HR observed prior to FOG was observed in 75% of the FOG episodes and was reportedly consistent across Freezer participants (N = 10). These physiological changes were consistent when examined over intervals of 3 and 10 s before the occurrence of FOG, and also distinct from changes in HR associated with voluntary stopping (which biomechanically resembles FOG). It is noteworthy that this study only included FOG episodes that occurred during turns in fast or self-paced walking conditions. Recent work has suggested that vulnerability to particular triggers (e.g., turning, doorways, dual-tasking, etc.) can subtype Freezers and explain the heterogeneity in freezing behavior across participants [8]. For example, it was found that ‘Anxious Freezers’ most commonly experience FOG in dual-task or hurried situations, whereas Asymmetric-Motor Freezers most commonly experience freezing when turning and navigating doorways. Thus, our first experiment aimed to replicate and extend previous findings by examining FOG across various situations (e.g., turning, dual-tasking, doorways, hurried shuffle) to determine whether an increase in HR prior to FOG was consistent or varied across trigger situations. A reduction in HR prior to during voluntary stopping was also verified in the current study to confirm previous findings [7]. An exploratory analysis further described the HR pattern prior to FOG across Freezer subtypes (i.e., Anxious, Asymmetric-Motor, and Sensory-Attention Freezers, as determined by the Characterising FOG Questionnaire).
Although elevated HR is an index for arousal and sympathetic activation [9], without the direct manipulation of threat, it remains difficult to infer any causal relationship between anxiety and FOG as Maidan and colleagues point out. Thus, our second experiment manipulated threat using a validated virtual reality paradigm [10] to examine whether HR changes were greater during FOG provoked by the threat condition compared to the non-threatening condition. Previous research has shown that freezing episodes are more severe and frequent when PD patients walk in anxiety-provoking virtual environments (i.e., across an elevated plank compared to a plank located on the ground) [10]. The current study will extend these findings by contrasting the HR changes prior to and during FOG episodes provoked in threatening and non-threatening environments. It was expected that if elevations in HR were driven by anxiety (or at least partially driven by anxiety), then an increase in HR before FOG would be more pronounced when the subject is more anxious during the high threat condition, compared to the low threat condition. Finally, an exploratory analysis will compare Anxious vs Non-Anxious Freezers to determine whether HR changes are more pronounced in Anxious Freezers.
METHODS
Participants
Nineteen patients with PD and FOG were recruited and tested for Experiment 1; however only 10 Freezers were included in the analysis (five participants were excluded due to poor quality HR data and four participants did not experience any FOG during the testing). For Experiment 2, twenty-three PD patients with FOG were recruited and tested with minimal overlap with the sample from Experiment 1; however, only 12 participants experienced FOG episodes in both conditions and had good quality HR data and thus were included in the analysis. Patients were recruited through the Parkinson’s Disease Research Clinic at the Brain and Mind Centre, University of Sydney, Australia. All patients were confirmed to experience FOG using the following criteria: 1) previous diagnosis of idiopathic PD by a trained neurologist and a history of FOG, and 2) a positive response to item 3 of the Freezing of Gait Questionnaire (FOG-Q), which is a reliable and valid tool to assess FOG severity and identify PD patients as “Freezers” [3]. Patients were excluded if they had other neurological disorders, severe head tremor, hearing loss or significant visual impairment. This study was approved by the University of Sydney Human Research and Ethics Committee (#2014/255) and therefore abided by the ethical standards of the 1964 Declaration of Helsinki. Written informed and signed consent was obtained from all participants prior to participation in the study.
To maximize the number of FOG events, all participants in both studies completed the full experimental procedure in their practically defined ‘Off’ state, having withdrawn from anti-parkinsonian medication for a minimum of 12 h prior to the study. All patients were receiving dopaminergic replacement therapy. One participant included in the analysis for Experiment 1, and one participant included in the analysis for Experiment 2, had also undergone subthalamic nucleus deep brain stimulation (DBS) in addition to taking anti-parkinsonian medication. In these cases, participants underwent the 12 h withdrawal of their medication and switched off their DBS at least 40 min prior to testing. Additionally, one participant in Experiment 2 was receiving levodopa/carbidopa intestinal gel and the pump was switched off 12 h prior to the study. It is important to note that due to the sample size in both Experiments, statistical analyses were run both with and without participants with DBS and levodopa/carbidopa intestinal gel to confirm the robustness of the significant findings reported.
Questionnaires and clinical assessment
In both experiments, prior to completing the experimental walking protocol, participants completed a set of questionnaires and examinations to assess FOG, as well as affective, cognitive and motor symptoms (see Table 1). The Characterising FOG Questionnaire (C-FOG) was employed to characterize FOG severity and subtypes (e.g., Asymmetric-Motor, Anxious, Sensory-Attention) for Experiment 1, based on contexts in which they experience greater FOG [8]. The Parkinson Anxiety Scale (PAS) assessed persistent anxiety, episodic anxiety and avoidance behavior in individuals with PD [11] and was used to striate Anxious (PAS > 12) and Non-Anxious (PAS < 12) subgroups in Experiment 2. The Modified Mini-Mental State Exam (3MS) [12], used in Experiment 1, and the Mini-Mental State Exam (MMSE), used in Experiment 2, evaluated general cognition [13]. Finally, the Movement Disorder Society’s Unified Parkinson’s Disease Rating Scale Section III (UPDRS III) assessed participants’ motor symptom severity.
Participant demographics
Data is presented as mean±SD.
Apparatus and protocol
Experiment 1
Prior to testing, participants were outfitted with the HR monitoring system (Zephyr Bioharness) that measured HR continuously for the duration of the study. A 30 s baseline standing heart rate was recorded at the beginning of the experiment. Patients were video recorded while performing a standardized series of timed up and go (TUG) tasks designed to provoke FOG, similar to previous work [14]. This protocol included 10 walking trials where participants were instructed to walk 5 meters from a chair to a 0.6 m×0.6 m target box marked on the ground and then return to the start position as quickly and as safely as possible in the following five situations: 1) 180° TUG: turn left or right (180° turn trial) in the box before returning to the starting point (chair); 2) 540° TUG: perform a one and a half turn while in the box before returning to the starting point; 3) Box: take short steps to the left or right around the taped outline of the box before returning to the starting point; 4) Dual-task (DT): perform a secondary cognitive task (e.g., recalling months of the year backwards) while completing the TUG trial; 5) Door: walk through a doorway to reach the taped box, turn left or right in the box before returning to the starting point. Each walking trial was performed at least twice to include both left and right turns. A 20-meter walking protocol was also performed where participants were given advanced instruction to immediately stop walking when hearing the word, “stop”, and to resume walking when instructed to “walk”. The entire experiment was video recorded with a tripod-mounted camera to capture the start and end times of trials, stops, as well as quantify FOG events. Video recording also served to synchronize across the various modalities for data collections.
Experiment 2
Prior to testing, participants were outfitted and familiarized with the virtual reality (VR) set-up and fitted with the HR monitoring system (Zephyr Bioharness) that measured HR continuously for the duration of the study. A 30 s baseline standing heart rate was recorded at the beginning of the experiment. The virtual environment was developed using Steam (Valve Corp., WA, USA); SteamVR is a VR software platform and the plank application was developed using the Unity game engine (Unity Technologies, San Francisco, CA, USA) and delivered to the subject using a head-mounted display (HMD), HTC Vive (HTC Corp., Taiwan & Valve Corp., WA, USA). The VR paradigm ran on a Dell Alienware portable computer (Dell Technologies Inc., TX, USA) with a NVIDIA GeForce GTX 1080MQ graphics card (Nvidia, Santa Clara, CA, USA), and was streamed to the HMD in real-time (at a refresh rate of 90 Hz). The HMD weighed 470 g and featured two 3.6” screens delivering a resolution of 1080×1200 full-color pixels per eye and a 110-degree field of view. The HMD was firmly secured on the participants’ face, preventing vision of the real-world environment around them and allowing greater immersion in the virtual environment. The interpupillary distance and visual focus of the headset display was adjusted for each participant to ensure clear stereoscopic visual perception. Two mounted Vive VR Base Stations (HTC Corp.) were placed in the corners of the testing room and tracked the movement of the HMD to allow for constant updating of the participants’ position in the virtual environment. Participants’ walking behavior was video recorded and then subsequently scored by trained experts to identify FOG episodes.
Participants were instructed to stand at one end of the pathway where a floor marking was calibrated to display the start position in virtual reality. The length of the walkway was mapped to the length of the virtual space (using the Steam based software ‘ChaperoneTweak’). Each trial consisted of walking 12 meters total (i.e., 6 meters from the starting position to the end of the plank, and then returning 6 meters to the starting position). Participants were instructed to begin walking at the sound of a tone manually elicited by a button press that was synchronized to the video and HR recording. At the end of each trial, after returning to the start position, participants were presented with a Self-Assessment Manikin scale (displayed in the HMD) and asked to provide a subjective rating of their anxiety levels during that trial. To manipulate threat, participants walked across the plank in two conditions: 1) Ground: across a narrow plank located on the ground; 2) Elevated: the ground surrounding a narrow plank descended creating a deep pit, and participants navigated the elevated plank (Fig. 1). Each participant completed 12 randomized trials (6 per condition). A standing rest period of at least 30 s between each trial was given to minimize carryover effects from the previous trial.
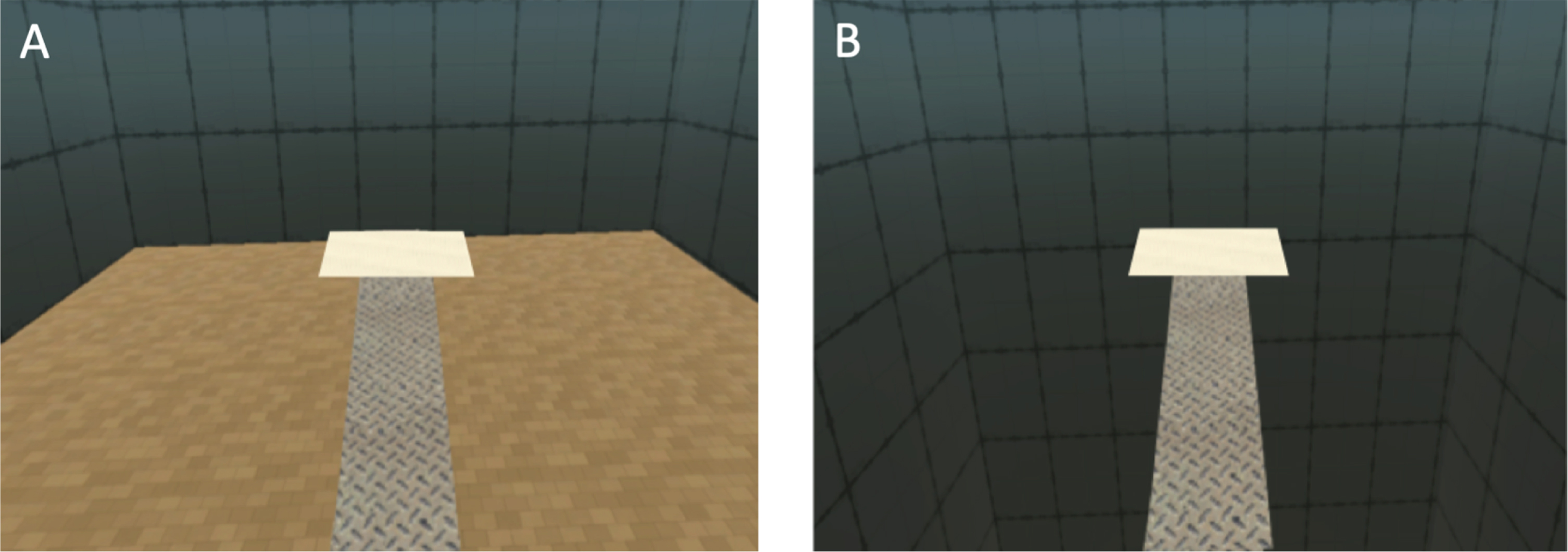
VR paradigm. Participants walked across two conditions. A) Ground: a narrow plank located on the ground. B) Elevated: a narrow plank surrounded by a deep pit.
Data analysis
Freezing of gait, stopping, and heart rate
A FOG episode was defined as an unintended interruption of gait where the subject did not make a normal and effective step forward [15]. The freezing episode finished when the subject made at least two consecutive normal steps. In both experiments, output from the video camera was manually annotated using ELAN™ software (The Language Archive, Nijmegen, Netherlands) according to recent recommendations [15]. Analysis of video playback identified FOG events during trials allowing for subsequent quantification of key outcome measures including the number of FOG episodes and the percentage of each trial spent frozen. Additionally, the onset of video recording was synchronized with the onset of the Bioharness HR monitor to overlay HR data on experimental events such as freezing and stopping. Thus, a time series of HR was developed to analyze the second-by-second changes prior to and during FOG and stopping events.
A continuous recording of HR (1 Hz) was captured by the Zephyr® Bioharness 3.0 during Experiments 1 and 2. The device is composed of a chest strap with passive sensors that detect ECG signals through conductive pads. The QRS complex from the ECG signal corresponds to the electrical activity of ventricular muscle contraction where the R-R interval was used to calculate HR expressed in beats per minute (bpm) [7]. The ECG data was filtered to automatically detect false or missing R peaks, and smoothing was automatically applied. The Bioharness calculated HR by using a moving window from the preceding 15 s of ECG signals.
Self-reported anxiety
In Experiment 2, a subjective measure of anxiety was also obtained by asking participants to rate their feelings of anxiety using a 9-point Self-Assessment Manikin (SAM) scale [16]. The SAM scale was displayed in the virtual environment at the completion of each trial.
Statistical analysis
In both experiments, only trials which provoked FOG were analyzed (Experiment 1 included 45 trials; Experiment 2 included 79 trials). For every eligible FOG episode, a 13 s HR time series composed of 10 s prior to the FOG episode, and the first 3 s of the FOG episode were extracted, normalized to the participants’ standing HR (HRt –HRstand) and compared across time in 1 s bins. Repeated measures ANOVAs were used to examine changes in HR over time (i.e., over 13 time points). Pairwise comparisons were used to evaluate post-hoc significant differences. An alpha level of 0.05 was used to determine significance. All statistical analyses were run both with and without participants with DBS and levodopa/carbidopa intestinal gel to confirm the robustness of the significant findings reported.
In Experiment 1, FOG was not experienced by all participants across all situations (e.g., turning, hurried box shuffle, dual-tasking, crossing a doorway). Thus, to examine whether HR changes prior to FOG were consistent across participants we collapsed across situations, to investigate overall HR changes (irrespective of situation) prior to FOG, similar to previous work [7]. It is noteworthy that, in Experiment 1, the amount of FOG did not differ significantly between situations. To investigate whether HR changes differed across situations, the 13 s HR time series for each individual FOG episode was normalized to the participants’ standing baseline HR (HRt –HRstand) and then grouped by situation (e.g., 180 Turn, 540 Turn, Box, Dual-task, Doorway). A mixed repeated measures ANOVA (situation×time) was conducted. To further explore the heterogeneity across Freezers, HR changes prior to FOG were examined across Freezer subtypes. In Experiment 1, there were 4 Asymmetric-Motor Freezers, 3 Anxious Freezers and 3 Sensory-Attention Freezers. Given the small number of participants in each group in Experiment 1, we opted to graph the results; however, no statistical comparisons were carried out. Finally, to determine whether HR increased prior to stopping in Experiment 1, an 8 s HR time series composed of 5 s prior to a stop, as well as the first 3 s of a stop were extracted and compared across time in 1 s bins. A two factor repeated measures ANOVA (condition [FOG vs stopping]×time) was used to examine the difference in HR changes over time (i.e., over 8 time points) between FOG and stopping.
In Experiment 2, paired t-tests were used to compare self-assessment ratings, number of FOG episodes and the percentage of time spent frozen between threat conditions (ground vs plank). A repeated measures ANOVA (condition×time) was conducted. Pairwise comparisons were used to evaluate post-hoc significant differences, as well as conduct a priori direct comparisons of second-by-second HR changes prior to FOG during high and low threat conditions. Finally, mixed repeated measures ANOVAs (group×condition) and (group×condition×time) were conducted to perform an exploratory analysis to examine any Freezer subgroup interactions (based on PAS responses) for self-reported anxiety, FOG outcomes as well as HR patterns prior to FOG. In Experiment 2, there were 6 Anxious Freezers and 6 Non-Anxious Freezers according to a median split on the PAS scores. This allowed us to investigate whether Anxious Freezers (compared to Non-Anxious Freezers) showed more pronounced patterns of HR and FOG across the two threat conditions.
RESULTS
Experiment 1: Freezing of gait
Of the nineteen participants recruited and tested in this study, five participants were excluded due to poor quality HR data and four participants did not experience any FOG during the testing. Therefore, ten participants were included in the analysis of HR changes prior to FOG. Notably, this remaining sample size resembled that of the previously published study [7]. During the protocol 192 FOG episodes were elicited (180° Turn: 37; 540° Turn: 16; Box: 46; Dual-task: 62; Doorway: 31) in the 10 freezers included in the study analysis. There were no significant differences in the number of FOG episodes or the percentage of trial spent frozen across the five different walking situations. However, only the first FOG episode in each trial was considered for the HR analysis to avoid carry-over effects. Thus, 45 FOG episodes (20% during 180° Turns, 13.3% during 540° Turns, 20% during the hurried box shuffle, 24.4% during dual-tasking, 22.2% during doorway navigation) were eligible for the HR analysis. See Table 1 for clinical and demographic details on the sample included in the study analyses.
Experiment 1: Heart rate changes 10 seconds prior to FOG
A significant main effect of time (F(12, 108) = 2.59, p = 0.005) was found for the HR preceding FOG (where all situations were collapsed in a similar manner to previous work [7]). Post hoc analyses showed significant increases in HR at 2–3 s (p = 0.033) prior to FOG onset and a trend that HR increases at 6–7 s (p = 0.061) prior to FOG onset (Fig. 2A). These findings remained significant when the participant receiving DBS was excluded from the analysis. In fact, upon exclusion of this participant, the increase in HR at 6–7 s reached significance prior to FOG onset (p = 0.04).
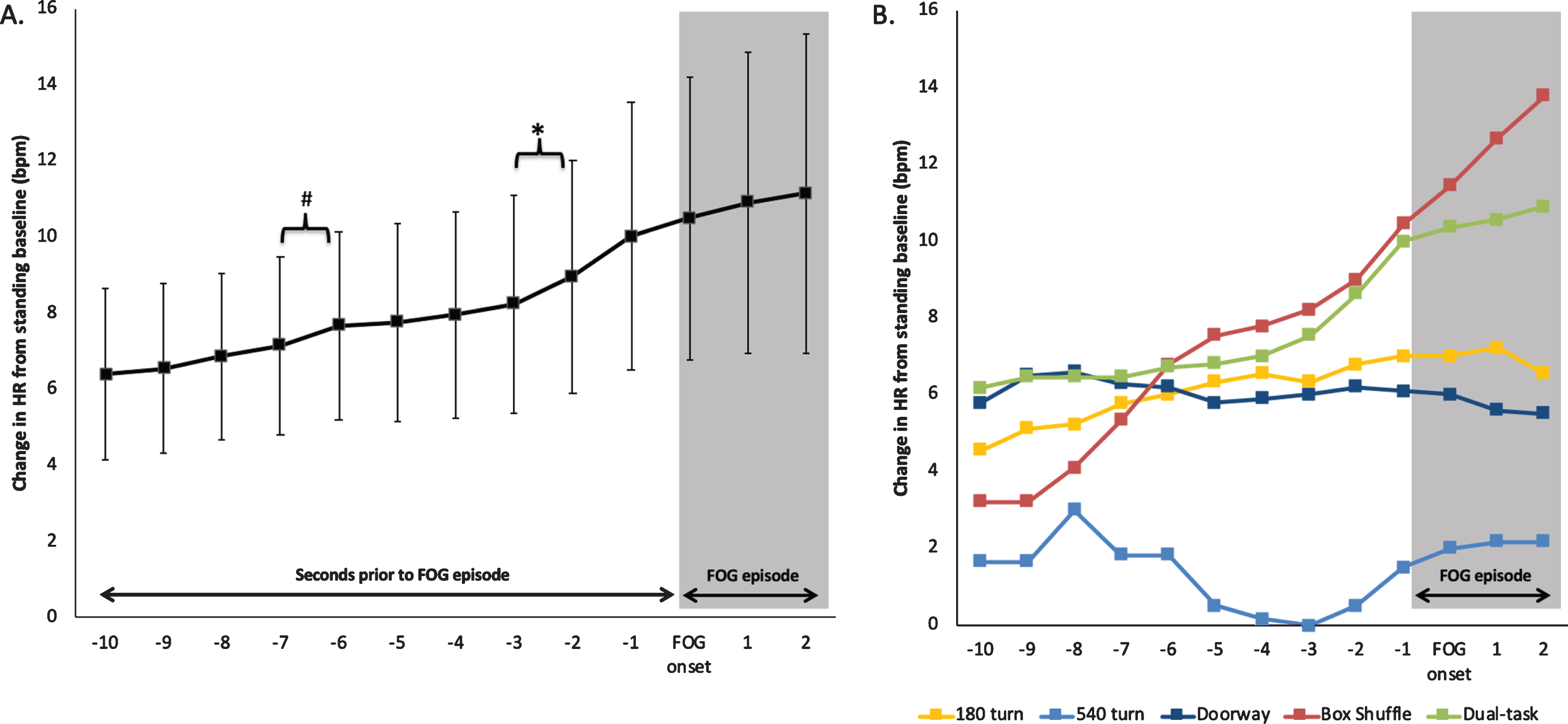
A) HR changes 10 s prior to FOG and 3 s during FOG averaged across all participants and all eligible FOG episodes in Experiment 1. B) Depicts the specific pattern of HR changes prior to and during FOG episodes averaged across the situational trigger (i.e., while performing either a 180° Turn, 540° Turn, navigating a Doorway, hurried shuffle around a Box, or Dual-tasking) to display the heterogeneity in HR changes prior to FOG. *denotes a significant increase in HR, #denotes an increase in HR that was found to reach significance upon the exclusion of one participant using DBS. Error bars represent standard error of the mean.
An interaction between situation and time (F(48, 468) = 2.14, p < 0.001) revealed that HR changes were not homogeneous across situations that provoke FOG, but instead most pronounced when FOG was provoked during the hurried Box shuffle and Dual-task compared to turning (both 180° and 540° Turns) and navigating Doorways (Fig. 2B).
Figure 3 displays exemplary HR traces of each FOG subtype (according to the C-FOG) on the left, while the graph on the right provides a summary of the pattern of HR changes when grouped by Freezer subtypes. It is noteworthy that no statistics were carried out; however, the ‘Anxious’ subtype of Freezers displayed the greatest increase in HR prior to FOG, compared to the other two Freezer subtypes. It is important to note that this was exploratory and remains descriptive due to the small sample size.
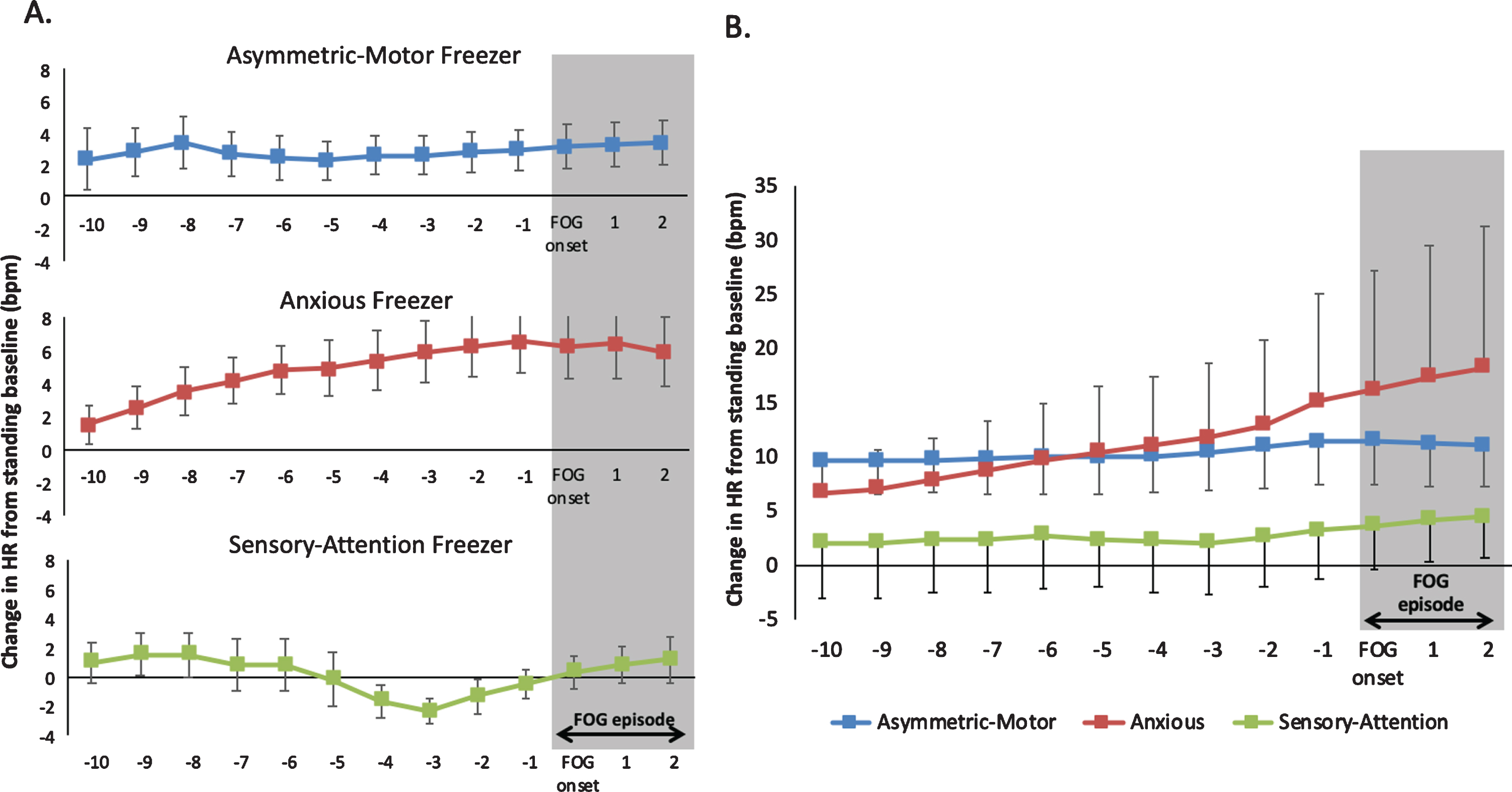
A) The average HR 10 s prior to FOG and 3 s during FOG are depicted for an individual participant of each Freezer subtype to display the heterogeneity in HR changes prior to FOG. B) Depicts the pattern of HR changes prior to and during FOG episodes averaged across Freezer subtypes (i.e., Asymmetric-Motor, Anxious, Sensory-Attention). Error bars represent standard error of the mean.
Experiment 1: Heart rate changes 5 seconds prior to Stopping
A significant interaction between condition and time (F(7,42) = 7.61, p < 0.001) was found for the 8 s HR time series (5 s prior to the stop/FOG and 3 s during the stop/FOG). In contrast to HR increasing prior to FOG, HR decreased before participants stopped; however, there were no significant second-to-second changes identified in the post-hoc analysis. These findings remained significant when the participant receiving DBS was excluded from the analysis.
Experiment 2: Freezing of gait
Of the 23 participants tested in this study, only 12 experienced FOG episodes in both conditions and had good quality HR data. Unfortunately, three participants could not complete the elevated plank condition due to severe freezing. Similar to Experiment 1, only the first FOG episode in each trial was considered for the HR analysis to avoid carry-over effects. Thus, HR was examined across a total of 79 FOG episodes (42% during the ground condition, 58% during the elevated condition). Participants reported significantly greater levels of anxiety after walking across the elevated plank compared to the ground plank using the self-assessment manikins (t(11) = –6.18, p < 0.001). Furthermore, FOG was also significantly more frequent (t(11) = –4.45, p = 0.001) and there was a greater percentage of the trial spent frozen (t(11) = –3.8, p = 0.0015) while navigating the elevated compared to the ground plank. These findings remained significant when the two participants receiving DBS and levodopa/carbidopa intestinal gel were excluded from the analysis.
An interaction between group and condition was found for percentage of trial spent frozen (F(1,10) = 4.93, p = 0.05). Post hoc analysis showed that Anxious Freezers spent a significantly greater percentage of trial frozen during the elevated condition compared to the ground condition (p = 0.016), whereas there was no difference between conditions in the Non-Anxious Freezers. These findings remained significant when the two participants (one receiving DBS and one on levodopa/carbidopa intestinal gel) were excluded from the analysis. A main effect of group also showed that Anxious Freezers reported significantly greater anxiety across both conditions compared Non-Anxious Freezers F(1,10) = 5.36, p = 0.043) (Anxious Freezers: Ground (Mean:4.2), Elevated (M:7); Non-Anxious Freezers: Ground (M:2.6), Elevated (M:5.4)). This finding did not remain significant; however, when the two participants (one receiving DBS and one on levodopa/carbidopa intestinal gel) were excluded from the analysis (p = 0.12). There were no interactions between group and condition for self-reported anxiety nor the number of FOG episodes.
Experiment 2: Heart rate changes 10 seconds prior to FOG
A significant main effect of time (F(12, 132) = 4.95, p < 0.001) was found for HR preceding FOG. Post hoc analyses revealed that HR significantly increased at 5–6 s (p = 0.006) and 6–7 s (p = 0.037) prior to the onset of FOG, regardless of condition (Fig. 4A). There was no significant main effect of condition (F(1,11) = 0.51, p = 0.49), nor significant interaction between condition and time (F(12,132) = 0.89, p = 0.56). However, based on our exploratory a priori hypothesis, we examined the changes in HR on a second-by-second basis across each condition separately. Significant changes were only found when all participants were navigating the elevated plank, specifically at 5–6 s (p = 0.004) prior to the onset of a FOG episode. These findings remained significant when the two participants (one receiving DBS and one on levodopa/carbidopa intestinal gel) were excluded from the analysis.
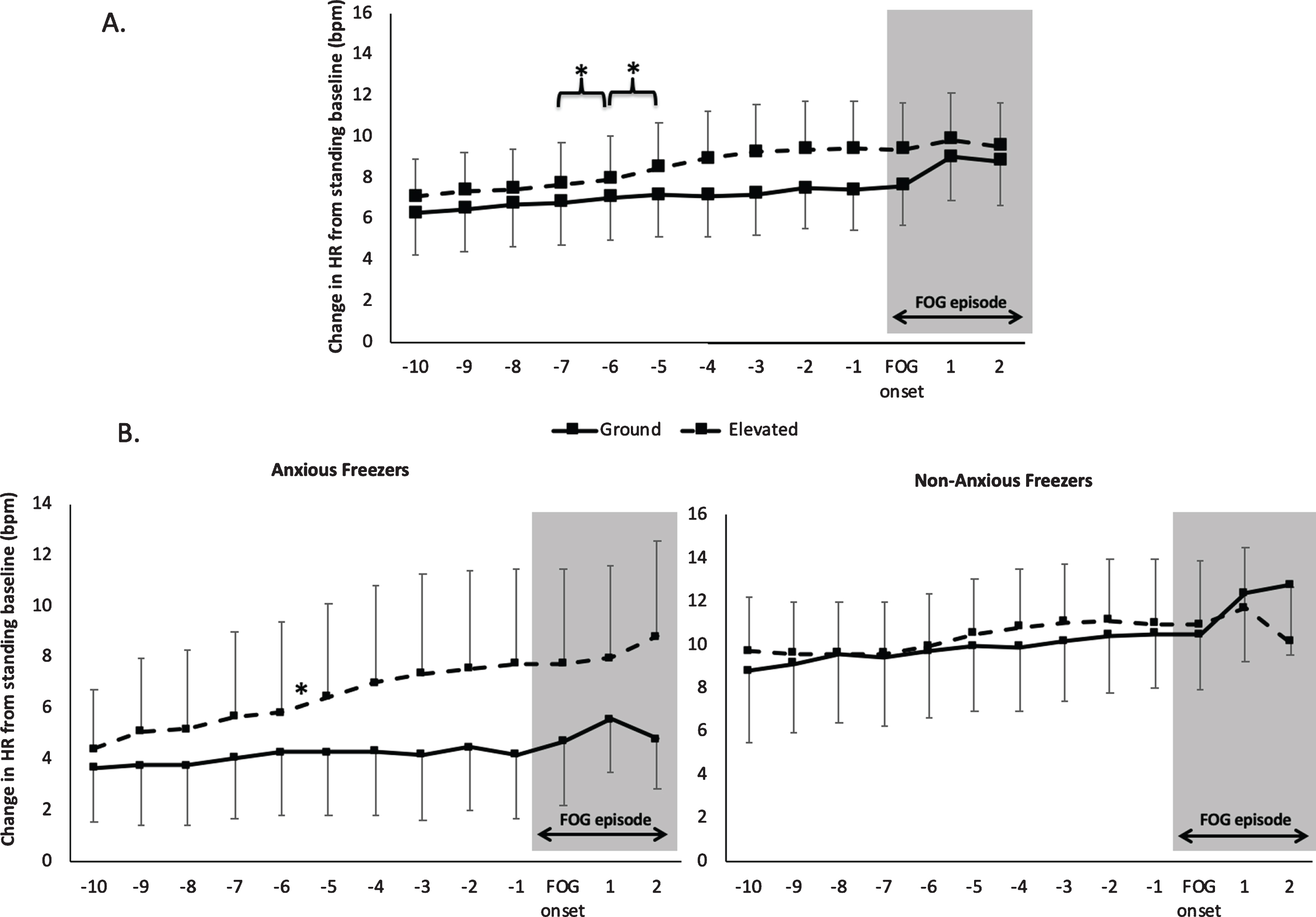
HR changes prior to and during FOG in Experiment 2 in two conditions: Ground (solid line): a narrow plank located on the ground and Elevated (dashed line): a narrow plank surrounded by a deep pit. A) Across all participants, B) Anxious Freezers only, C) Non-Anxious Freezers only. *denotes a significant increase in HR. Error bars represent standard error of the mean.
A significant interaction between condition, time and Freezer subgroup (F(12,120) = 2.2, p = 0.015) was also found for HR preceding FOG. Post hoc analyses revealed a significant increase in HR 5–6 s prior to FOG (p = 0.004) specifically in the elevated condition in the Anxious Freezers group only (Fig. 4B). These findings remained significant when the two participants (one receiving DBS and one on levodopa/carbidopa intestinal gel) were excluded from the analysis.
DISCUSSION
The primary aim of this study was to further understand the relationship between anxiety and FOG by exploring the heterogeneity in HR changes prior to and during FOG. In Experiment 1, we were able to replicate previous findings that HR increases prior to FOG episodes in non-specific FOG-provoking environments and also confirmed that HR changes prior to FOG were not simply due to a deceleration or coming to a halt, since HR prior to and during a stop decreased whereas HR increased prior to a FOG episode. Although we employed a second-by-second approach (rather than 3 s bins that were used to examine HR in previous work), strikingly similar results were obtained to Maidan and colleagues, such that a 0.7 bpm increase in HR was observed 2–3 s prior to FOG in the current study as well. Importantly however, our findings suggest that this characteristic increase in HR prior to FOG varied across situations that provoked FOG, as well as across individuals. HR changes prior to FOG were most pronounced when Freezers were instructed to hurriedly shuffle around a box or perform a dual-task (situations that have been previously associated with anxiety [8]) compared to turning or navigating a doorway (situations that have been previously associated with motor asymmetry rather than anxiety [8]). Furthermore, when Freezers were grouped into subtypes according to the Characterising FOG questionnaire [8], a similar pattern of results emerged suggesting that increases in HR prior to FOG may be most pronounced in ‘Anxious’ Freezers compared to ‘Asymmetric-Motor’ and ‘Sensory-Attention’ Freezer subtypes. While this descriptive data is useful for generating future hypotheses, it is noteworthy that statistics were not carried out on the Freezer subtypes in Experiment 1 due to a small sample size in each group. Thus, caution is warranted when interpreting these findings and further research is needed with larger samples before strong conclusions can be made.
In Experiment 2, where environmental threat was directly manipulated to induce anxiety, we were able to replicate the findings of Ehgoetz Martens and colleagues (2014), with both the frequency of FOG and the percentage of the walking trial spent frozen being significantly higher when participants traversed an elevated virtual plank compared to walking on a plank located on the ground. Furthermore, when split into ‘Anxious’ and ‘Non-anxious’ subgroups, only Anxious Freezers demonstrated a significant increase in percentage of trial spent frozen during the elevated condition compared to the ground condition, whereas no difference between conditions was found for Non-Anxious Freezers. These findings provide additional supporting evidence for the notion that anxiety may be an independent contributing factor to FOG. Critically, this was accompanied by increased subjective reports of anxiety during the elevated compared to the ground condition (in all participants), as well as greater subjective reports of anxiety in the Anxious Freezers compared to the Non-Anxious Freezers overall. Albeit, HR did not increase significantly during the high threat condition compared to the low threat condition as one might have expected. One possible reason for this may be because HR was only examined during the 13 s interval surrounding the FOG episode (rather than the full trial), whereas the subjective anxiety ratings were completed at the end of every trial.
Experiment 2 extended our current knowledge since it was the first to examine HR prior to and during FOG in conditions where threat was changed from low to high threat, which subsequently influenced patients’ subjective anxiety levels. Contrary to our hypothesis, our findings demonstrated that there was an increase in HR 5–6 and 6–7 s prior to a FOG episode, irrespective of threat condition. However, with a priori planned comparisons, it was revealed that a statistically significant change in HR was only found during the elevated (high threat) condition but not the low threat condition. This latter finding was more in line with our hypothesis that increases in HR prior to FOG are likely due to increased anxiety prior to FOG, supporting the notion that anxiety may be a causal factor of FOG. Furthermore, the pattern of a “climbing HR” that increased around 5–7 s prior to FOG and remained elevated (rather than simply increasing momentarily before the FOG episode) could provide insight into the nature of information prior to a FOG. Specifically, this type pattern might suggest that there is an accumulation of information processing (e.g., movement error signaling) that the system recognizes but may not be able to reset or fix. One could think of this akin to riding a bicycle down a hill. At some point, the system realizes that the bicycle is moving too fast and is out of control, and this mismatch between the skill required for the task and the individual’s skill could lead to a state of ‘sensorimotor anxiety’ (i.e., temporary panic or elevated HR). Since this remains speculative, future work should consider whether the point at which HR begins to climb correlates with increasing step-to-step variability prior to the FOG episode.
When the HR patterns were probed further, in Experiment 2, by splitting participants into ‘Anxious’ and ‘Non-Anxious’ subgroups, a significant interaction between group, condition and time showed that only the ‘Anxious’ Freezers had a significant increase in HR 5–6 s prior to FOG, particularly during the elevated condition. It is important to note that these subgroup findings should also been interpreted with caution, since each group only consisted of 6 Freezers (due to exclusions of participants that did not freeze (or froze too much) and/or had poor data quality). While further work is certainly needed, this is the first study to consider HR patterns across different FOG subtypes, and these exploratory findings provide preliminary evidence of potentially different mechanisms underlying FOG that may be at play in different Freezers. Although, anxiety may indeed be driving an increase in HR prior to some FOG episodes, it is important to consider that perhaps not all FOG episodes are preceded by an increase in HR or triggered by anxiety. These findings have important implications for developing biotechnology that can predict FOG.
How may anxiety cause FOG?
In contextualizing the role of HR in the current study, it is important to first note that HR can demonstrate changes in autonomic system activity and can therefore indirectly index threat processing and anxiety [17]. At the center of this ‘defensive’ system is the amygdala, which is involved in both processing threat stimuli and the expression of it [18]. Via a range of projections, the amygdala and other limbic structures are essential in mediating the response to threat processing, such as the somatic response mediated by the midbrain (i.e., periaquedactal gray) and activation of the hypothalamic-pituitary-adrenal axis, which results in release of cortisol from the adrenal cortex [19]. Pertinent to the present study is output from limbic structures that can process threat to activate the autonomic system, namely through the hypothalamus [20]. With regards to the cardiovascular response to threat processing, it has been shown that sympathetic innervation to cardiac pacemaker tissue increases HR and conduction velocity via elevated levels of primary neurotransmitter, noradrenaline. While activation of the autonomic system can be mediated by a range of factors [17], it is reasonable to assume that elevated HR prior to a FOG episode may be contributed to by the limbic system’s interaction with the autonomic system.
Neural projections from limbic structures, such as the amygdala, to the basal ganglia are key to the interaction of threat processing with motor output [21]. Indeed, pathology due to PD may cause dysfunctional limbic processing, which can subsequently manifest as FOG. During states of fear in healthy individuals, neuroimaging studies reveal heightened connectivity between the right amygdala and the putamen (part of the dorsal striatum of the basal ganglia). In a healthy state, temporary heightened connectivity in the context of perceived threat provides an evolutionary advantage, facilitating a state of readiness to respond to the threat [21]. However, sustained heightened connectivity becomes pathological, as demonstrated by similar patterns in individuals with anxiety disorders [22]. Notably, this same pattern of abnormal connectivity has been identified in individuals with PD and FOG during resting state [23]. Furthermore, a recent fMRI study revealed more pronounced connectivity between the limbic network and the striatum when participants experienced freezing episodes on a virtual walking task using foot pedals, compared to normal walking on a virtual walking task using foot pedals [24]. Interestingly, connectivity between the limbic network and striatum was independent of FOG severity suggesting that it may represent the fundamental network signature of FOG [24].
Dysfunctional top-down regulation of limbic regions can also result in abnormal activity and may be involved in precipitating FOG [23]. The modulatory role of higher cortical regions in influencing activation of limbic regions and thus regulating the emotional response to threat is in line with a post-attentive stage of processing threat-stimuli [18]. Bishop and colleagues [25] found that the response of the amygdala to unattended (outside current focus of attention) and attended threat-related stimuli (within current focus of attention) was also modulated by anxiety. Specifically, low-anxious subjects only demonstrated an increase in amygdala response to attended threat-related stimuli, whereas high-anxious subjects demonstrated elevated amygdala responses to both attended and unattended threat-related stimuli. Diminished output from a pre-attentive threat evaluation system, thereby results in a greater probability that threat stimuli will capture attention [26]. Given that anxiety disorders are one of the most common non-motor symptoms in PD [27], it is not surprising that a similar pattern of connectivity between higher cortical regions and the amygdala is evident in patients with FOG [23]. Taken together, it could be postulated that abnormal activity of the amygdala and other limbic regions, due in part to irregular or dysfunctional control from higher cortical centers may contribute to FOG.
Limitations and considerations
We acknowledge that the main limitation of this study was the small number of participants that were included in the final analysis either because they did not experience any FOG episodes during testing or being excluded due to poor quality HR data. It should be emphasized that since the sample size was limited, the statistical findings should be interpreted with caution. Furthermore, the resultant small sample size also meant that statistical analyses could not be performed on Freezer subtypes in Experiment 1. Future studies are needed to confirm these findings in a larger cohort.
Conclusion
In conclusion, these results provide supporting evidence that anxiety is involved in precipitating FOG. Moreover, increases in HR prior to a freezing episode, particularly in anxiety-provoking situations, further implicates anxiety as an important contributor to FOG. Future studies should consider tracking other psychophysiological measures when studying FOG behavior to further understand the complex sequelae that generates FOG episodes. The findings from this study suggest that physiological markers of anxiety may help to predict anxiety-related FOG episodes in real time, which if combined with biofeedback could form the basis of a novel treatment strategy to reduce freezing. Furthermore, the role of anxiety treatment strategies should be contemplated in the management of this challenging symptom.
CONFLICT OF INTEREST
The authors have no conflict of interest to report.
Footnotes
ACKNOWLEDGMENTS
We warmly acknowledge the assistance of the team and patients at the ForeFront Parkinson’s Disease Research Clinic, Sydney for their contribution to this research. We would also like to acknowledge Gabriel Wainstein and Joseph Phillips for their assistance with computer programming, Matthew Georgiades for the assistance in recruitment and data collection, as well as Monique Masling for data extraction and organization.
This work was supported by the University of Sydney –Brain and Mind Centre Early Career Development Grant (KEM). Parkinson Canada also supported KEM with a Postdoctoral Fellowship. SJGL is supported by NHMRC-ARC Dementia Fellowship (#1110414). NHMRC Dementia Team Grant (#1095127) supported work performed at the University of Sydney.