
Abstract
Background
High treatment burden is associated with poor adherence, wasted resources, poor quality of life and poor health outcomes. Identifying factors that impact treatment burden in Parkinson’s disease can offer insights into strategies to mitigate them.
Objective
To explore the experiences of treatment burden among people with Parkinson’s disease (PwP) and their caregivers.
Methods
A systematic review of studies published from year 2006 was conducted. Qualitative and mixed-method studies with a qualitative component that relate to usual care in Parkinson’s disease were included. Quantitative studies and grey literature were excluded. Data synthesis was conducted using framework synthesis.
Results
1757 articles were screened, and 39 articles included. Understanding treatment burden in PwP and caregivers was not the primary aim in any of the included studies. The main issues of treatment burden in Parkinson’s disease are: 1) work and challenges of taking medication; 2) healthcare provider obstacles including lack of patient-centered care, poor patient-provider relationships, lack of care coordination, inflexible organizational structures, lack of access to services and issues in care home or hospital settings; and 3) learning about health and challenges with information provision. The treatment burden led to physical and mental exhaustion of self-care and limitations on the role and social activities of PwP and caregivers.
Conclusion:
There are potential strategies to improve the treatment burden in Parkinson’s disease at an individual level such as patient-centered approach to care, and at system level by improving access and care coordination between services. Future research is needed to determine the modifiable factors of treatment burden in Parkinson’s disease.
INTRODUCTION
Parkinson’s disease (PD) is a common, progressive neurodegenerative disorder. It is predominantly recognized as a movement disorder with tremor, rigidity, and bradykinesia. However, people with Parkinson’s disease (PwP) experience a variety of non-motor symptoms such as bowel and bladder dysfunction, pain, fatigue, and problems with sleep [1]. There is also a high prevalence of neuropsychiatric disorders in PD such as apathy, depression, and dementia [2]. As PD progresses, PwP experience an increasing number of uncontrolled symptoms which are associated with poor quality of life [3]. Moreover, PwP are often older and have other long-term conditions such as hypertension and coronary heart disease [4, 5]. Unfortunately, there is no cure for PD. The mainstay of management in PD is to achieve symptom control, often with complex medication regimens and polypharmacy [5]. Surgical intervention with deep brain stimulation (DBS) may be suitable for a few PwP for whom medications fail to manage their symptoms [1].
Clinical experience suggests that PD is a long-term condition which may be associated with high treatment burden. Treatment burden is defined as ‘the workload of healthcare and its impact on patient well-being and functioning’ [6]. Some of the workload of managing health includes learning about a health condition, taking multiple medications, monitoring aspects of health, attending healthcare appointments and making lifestyle changes such as diet and exercise [6]. Patients may experience high treatment burden due to an imbalance between the workload of health and their ability to complete the workload with the available resources (sometimes termed ‘capacity’) [7]. High treatment burden is associated with poor adherence to treatment regimens, wasted resources, poor quality of life and poor health outcomes [8].
The majority of PwP are supported by family or friends (caregivers) who often not only assist them with activities of daily living but also help PwP manage their health and treatment-related activities such as medication taking and attending appointments [9]. Caregivers may experience treatment burden themselves as a result of looking after someone with a long-term condition as well as having to manage their own health. The treatment burden experienced by caregivers is different to the concept of caregiver burden, but may be interlinked [10]. Caregiver burden is a well-researched notion defined as ‘the extent to which caregivers perceive that caregiving has had an adverse effect on their emotional, social, financial, physical, and spiritual functioning’ [11–13]. Many tools have been validated and are widely used to assess caregiver burden [11, 15]. However, the treatment burden experienced by caregivers and its association with caregiver burden is not well understood.
Identifying the treatment burden in patients with long-term health conditions can offer insights into potential practical steps to reduce the treatment burden or enhance capacity [8]. For example, Gallacher et al. found that the quality and configuration of health and social care services influenced the treatment burden in stroke [16]. Treatment burden has been studied in other conditions such as stroke, cancer, chronic kidney disease and patients with multimorbidity but not yet explicitly evaluated in PD [16–19]. We hypothesize that PwP and their caregivers experience high treatment burden when looking after their health. The aim of this systematic review was to understand the experiences of treatment burden among PwP and their caregivers.
MATERIALS AND METHODS
We conducted a systematic review of qualitative studies following the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) approach [20]. The protocol is registered on the PROSPERO database: CRD42020172023.
Search strategy
A systematic search of the literature was conducted on five electronic databases: MEDLINE, Embase, CINAHL, Scopus and PsychInfo. A search strategy was constructed with the help of a senior librarian and is provided in the Supplementary Material. Table 1 summarizes the PICOS (Patient Intervention Comparison Outcomes Study) framework rationale for inclusion of articles.
Inclusion criteria were as follows: (i) participants were PwP and/or their caregivers; (ii) qualitative methods or mixed-method studies with a qualitative component; (iii) reported data from PwP and/or caregivers of PwP independent of other conditions; (iv) published in peer-reviewed journals. Exclusion criteria were as follows: (i) quantitative methods; (ii) qualitative data not related to usual care such as clinical trials or intervention; (iii) mixed-methods studies where qualitative data cannot be extracted; (iv) did not report data from PwP and/or caregivers of PwP independently of other conditions; (v) grey literature such as conference abstracts, book chapters, reports, commentaries and PhD theses.
PICOS framework search strategy
No geographical limitations were applied. We limited our search to publications from year 2006 as this was the year of the first National Institute for Clinical Excellence (NICE) Clinical Guideline for Parkinson’s disease in the United Kingdom (UK) [21]. This also allowed us to understand the impact of current healthcare systems on the treatment burden [22, 23]. Non-English (French, Portuguese, German, Norwegian, Spanish, Persian, Japanese) full-text articles (n = 13) were excluded following full-text screening due to a lack of available translation services.
Data screening and extraction
A single researcher (QYT) screened the study titles for relevance. Two researchers independently conducted abstract review (QYT & LC/SF/KI) and full-text article screening (QYT & NJC/SERL). Any disagreements were discussed between two researchers and agreed. Data extraction were conducted by two researchers independently (QYT & KI) using a pre-defined data extraction template created by the research team. The Cambridge Dictionary defines the word ‘burden’ as ‘something difficult or unpleasant that you have to deal with or worry about’ [24]. Therefore, data related to difficult or unpleasant experiences with tasks related to looking after health mentioned by PwP and/or their caregivers were extracted, even if the term ‘treatment burden’ was not mentioned. Data were extracted from the findings or results section of the included studies as the discussion and conclusion sections would likely not present any new primary data, only additional interpretations [25]. Relevant data were extracted if they were quotations from participants (first-order construct) or interpretations of the authors (second-order construct). As the focus of this review was on treatment burden experiences, data related to symptom burden or caregiver burden in PD that did not specifically relate to the workload of health were not extracted.
Data synthesis
Framework synthesis, guided by the domains in Eton’s framework of treatment burden was used to analyze data [6]. Eton et al. developed a framework of treatment burden following interviews and focus groups with patients who had multiple chronic conditions other than PD [6, 26]. The finalized framework describe the three main themes of treatment burden as 1) the work patients must do to care for their health; 2) challenges or stressors that exacerbate felt burden; and 3) impacts of burden [6]. Framework synthesis is an iterative process widely used to synthesize qualitative research [27, 28]. It involves familiarization with the literature, identification of a thematic framework (Eton’s framework of treatment burden in this review), applying the framework to code individual studies included in the review and creating charts with distilled summaries from the evidence. The charts were used to map the range and nature of aspects related to treatment burden in PwP and their caregivers and to find associations between the themes.
Data extracted from each study were thematically coded and then these codes were mapped against the components of Eton’s framework and their sub-themes. Data were read multiple times and text coded carefully whilst keeping an open mind to identify themes or concepts in the data that may have not been described by Eton’s framework. Data were also organized and read according to first- and second-order constructs in order to understand the experiences of PwP and caregivers. Data synthesis was led by the primary researcher (QYT), closely supported by senior researchers (KI & HCR). The findings were discussed within the study team and consensus reached.
Quality rating
Quality appraisal was conducted by two researchers (QYT & NJC) independently and answers compared and discussed. The quality of studies was assessed using the Critical Appraisal Skill Programme (CASP) criteria for qualitative studies that considers the appropriateness of the research methods and whether the study findings are well-presented and meaningful [29]. The CASP consists of ten questions and is a well-established tool that is used to assess the methodological rigor of qualitative studies. Questions with ‘Yes’ responses were scored one point to give an overall quality score for each study.
RESULTS
Included articles
The number of papers screened, assessed for eligibility and included in this review are presented in the PRISMA flow diagram (Fig. 1). Thirty-nine articles were included in this review. A summary of the studies is presented in Table 2.
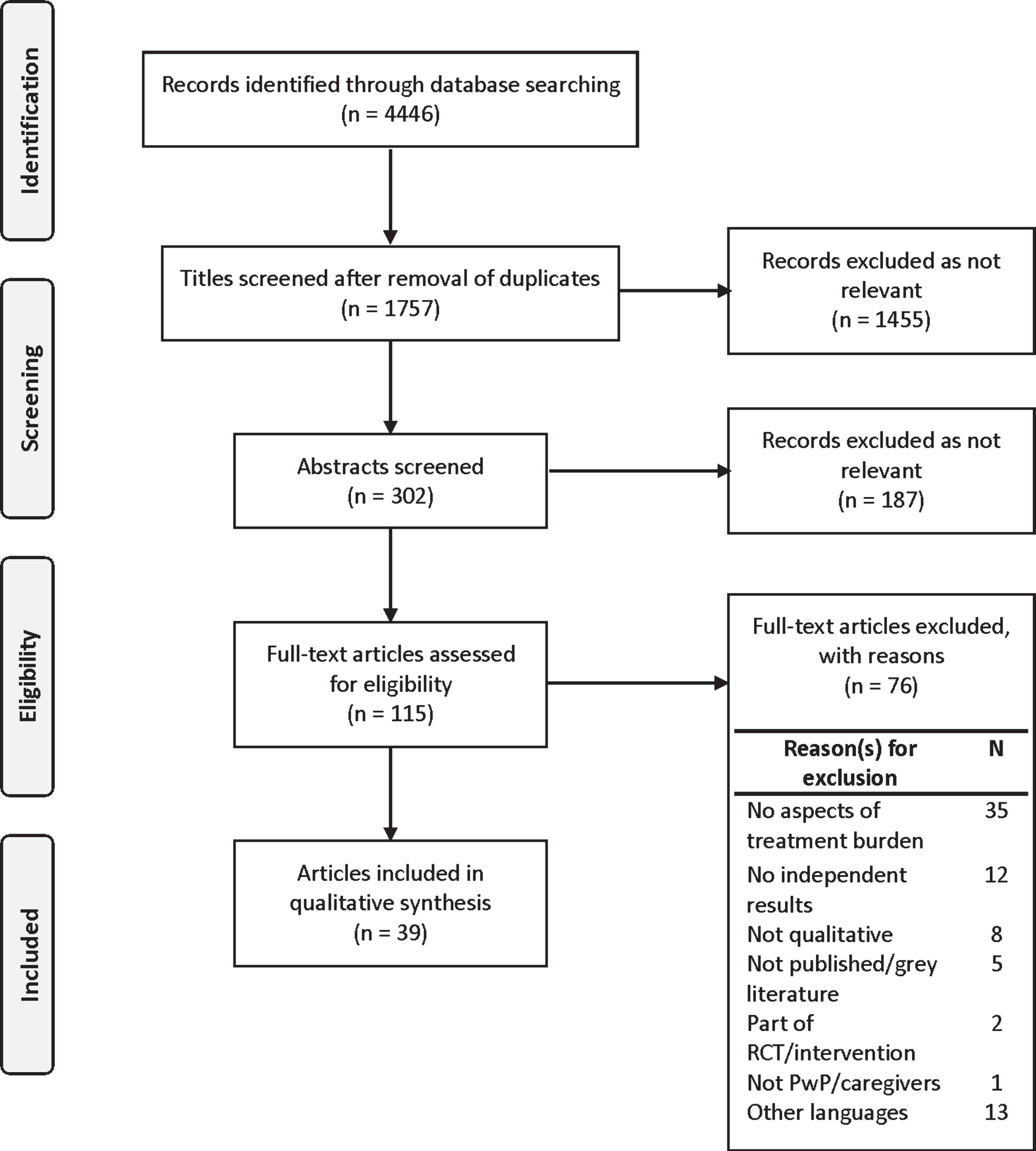
PRISMA flow diagram.
Summary of included articles
CASP, Critical Appraisal Skills Programme; DBS, Deep brain stimulation; F, Female; H&Y, Hoehn and Yahr staging; M, Male; NH, Nursing home; PD, Parkinson’s disease; PwP, People with Parkinson’s; RH, Residential home, UK, United Kingdom; USA, United States of America; Y, Year.
Studies were conducted in multiple countries including: UK (N = 10), United States of America (USA) (N = 8), Canada (N = 3), Denmark (N = 3), Netherlands (N = 3), Australia (N = 2), Brazil, (N = 1), Ethiopia (N = 1), Greece (N = 1), Indonesia (N = 1), Iran (N = 1), Ireland (N = 1), New Zealand (NZ) (N = 1), Singapore (N = 1) and Tanzania (N = 1). One international study was conducted across seven countries (Czech Republic, Italy, Netherlands, Norway, NZ, Spain, and UK). Qualitative studies were mainly conducted using interviews (N = 29), focus groups (N = 3) or both interviews and focus groups (N = 3). One study conducted secondary data analysis of interviews, one study conducted participant observation and interviews, one study conducted repertory grid methodology and one study conducted a qualitative survey questionnaire. Participants in the studies included PwP or their proxies (N = 7), caregivers (N = 16) or both PwP and caregivers (N = 16). A total of 933 participants were included in the review; 413 PwP, 435 caregivers and 85 participants where it was unclear whether they were PwP or caregivers.
Quality appraisal
Most articles (N = 34/39) were of good quality and scored seven or more points using the CASP qualitative appraisal tool (see Supplementary Material). Understanding the treatment burden in PD was not the primary aim of any of the included studies. The majority (N = 29/39) of studies failed to consider the researcher-participant relationship. As there is no consensus on assessing the quality of qualitative research, no studies were excluded based on quality.
Treatment burden in PD
Our findings support the use of Eton’s framework of treatment burden in PD and are summarized in Table 3. The subthemes within the three main themes from Eton’s framework are ordered in Table 3 based on the subtheme with the highest number of codes, with supporting quotes provided. No aspects of treatment burden identified fell outside our coding framework. We found that the main issues of treatment burden in both PwP and caregivers relate to medications, healthcare provider obstacles and information provision. The treatment burden led to physical and mental exhaustion of self-care and limitations on the role and social activities of PwP and caregivers.
Experiences of treatment burden in PwP and caregivers
GP, General Practitioner; PD, Parkinson’s disease; PwP, People with Parkinson’s.
Main issues of treatment burden in PD
Medications
PwP reported taking multiple medications at different times of the day with prescriptions being changed and adjusted regularly over time to find the right dosage to help mitigate their symptoms [30–36]. PwP were supported by their caregivers with managing and administrating medications as well as reminding them of medication times [9, 38]. The unpredictability and fluctuating symptoms of PD as well as the variability of PD medication effectiveness on a daily basis were some of the reported challenges with medication taking [35, 38–41]. PwP and caregivers monitored the response to PD medications and trialed different medication doses and timings as well as experimenting with other factors such as diet, sleep and exercise to see if this influenced their PD symptoms [33, 38]. PwP also described the ‘wearing off’ effect of PD medications causing poor control of symptoms between doses [36, 40–42]. This led to frequent changes in medications timings and doses, at times on a ‘trial and error’ basis, causing considerable confusion regarding medications [38]. Increasingly visible tremors due to the lack of medication effectiveness caused PwP to worry that the medications were not working [40]. The lack of positive symptom response observed by PwP (but not by family members) was reported as a reason for poor medication adherence [35]. Other reasons for poor adherence reported by both PwP and caregivers were forgetting to take medications, confusion about which tablets were due or being preoccupied with work or social activities [32, 43].
Other challenges with taking medications experienced by PwP and caregivers related to the precise timing of medications to avoid the return of symptoms, planning of mealtimes and diet due to PD medications and medication side-effects [32, 40–45]. PwP and caregivers described planning and scheduling activities such as exercise, shopping, meeting family or friends or clinical appointments around their medication timings [30–32, 40]. They established a daily routine around times when their medications were most effective [32, 42]. This was especially important if they had social plans to avoid any distress or embarrassment as PwP did not want their symptoms to be noticed by others [32, 40]. Some reported that the fixed schedule of medication timings interfered with their personal daily activities at times [32, 46]. There were contrasting attitudes towards medication adjustments in PwP: those who described themselves being more flexible and changing their medication times or taking extra doses around their work or daily activities to manage their symptoms [35, 42]; and those who only made changes in their medications after seeking advice from healthcare professionals [40]. Additionally, PwP and caregivers took careful consideration in planning their mealtimes and diet such as avoiding protein-rich meals to prevent drug and food interactions [30, 45]. Caregivers of PwP with swallowing difficulties also reported the need to consider how they could administer medications to the person with PD during mealtimes [47].
Managing the side-effects of taking PD medications such as compulsive behavior, frightening nightmares, hallucinations, disinhibition, dry mouth, drowsiness and insomnia were challenging for PwP and caregivers [34–36, 48]. Some PwP also reported that the medications made them feel worse rather than helped their symptoms [34, 40]. PwP described taking medications as “the lesser of two evils”, balancing the need for PD medications to help their symptoms alongside concerns of potential long-term side-effects of dyskinesia [35]. However, living with PD meant being dependent on medications, as PwP and caregivers described how they made sure they always had their PD medications with them when leaving the house [32, 40]. Furthermore, their dependence on medication increased as PD progressed and PwP described shorter time intervals between taking medications [32, 42].
Healthcare provider obstacles: Individual provider issues
PwP and caregivers described having to prepare for and attend separate appointments with doctors (General Practitioner (GP) and PD specialist), PD nurse specialist or physiotherapist [9, 49–53]. Some reported issues with transportation and the additional time spent preparing and travelling to healthcare appointments [36, 53]. Moreover, PwP and caregivers in countries across different global regions such as the UK, Netherlands and Indonesia described a lack of patient-centered care from many healthcare professionals with a predominant focus on medication needs, rather than a holistic approach that considered their social, psychological and care needs which may be more distressing [36, 54–56]. PwP and caregivers in the UK described poor relationships and unsatisfactory interactions with healthcare professionals due to lack of consulting time and infrequent follow-up appointments [9, 55]. Caregivers reported attending healthcare appointments with the person with PD they cared for as they were worried that person with PD may forget to mention certain things and not remember the consultations at the end [37]. However, they found that their views and opinions were not considered during medical appointments, despite their active role in managing PD [33, 48]. Some caregivers felt that they could not question or challenge the advice given by doctors, even if they did not fully understand the reasoning, due to the fear of being reprimanded [57]. Moreover, the predominant management of PD by specialists in the UK meant that PwP and caregivers felt that their GP lacked detailed knowledge about PD although they recognized that their GP still had an important role [9, 55]. In Australia, they described the reluctance from GPs to adjust prescriptions without input from their neurologist, causing a delay in medication changes and management of PD [41].
Healthcare provider obstacles: System issues
Attending medical appointments with multiple healthcare professionals that all focused on different medical issues was challenging [38, 58]. PwP and caregivers in Ireland, UK, Singapore and Netherlands experienced a lack of coordination, continuity of care and cohesion between the different health and social care services [9, 58]. PwP and caregivers reported a lack of clarity over the roles of health and social care professionals involved in their care, with no clear multidisciplinary approach [34, 58]. They at times experienced contradicting advice regarding their health and available support services due to the poor cohesion between services [34, 54]. In addition, caregivers perceived that the lack of coordination between services resulted in inadequate monitoring of PD symptoms and medications [9]. PwP and caregivers also described how the inflexible organizational structures of the healthcare systems influenced their interactions with health professionals and care providers [39, 59]. For example, care agency allocation of support workers based on geographical regions meant that they did not have visits from one regular support worker which prevented relationship building [59].
The poor availability of health and social care services increased the treatment burden for PwP and caregivers [9, 61]. In countries such as Australia, Canada, Ireland and UK, PwP and caregivers described long waiting times and lack of access to specialist PD doctors and allied health professionals such as physiotherapists and speech and language therapists, specialist palliative care or hospice services [38, 57]. The deteriorating mobility of the person with PD as the disease progressed meant PwP and caregivers experienced difficulty accessing healthcare and social services due to the limited availability of home visits from those services [39, 44]. Some PwP reported being discharged from specialist clinics to community services as they were physically unable to attend appointments, whilst other PwP made an active decision not to attend clinics as the difficulties of attending appointments and limited consulting time did not have any justifiable benefits as their PD progressed [44, 45]. PwP and caregivers also experienced poor access to social support and funding for home care support, home modifications and access to supportive equipment [9, 57]. Consequently, PwP and caregivers in UK with a publicly funded National Health Service reported making private payments for trained carers and respite as well as purchasing equipment individually due to the long waiting times for private carers and equipment [9]. Similarly in Australia, the inequitable funding system and limited access to home modifications added to the frustration and financial burden to PwP [53].
PwP and caregivers also faced specific challenges with looking after their health in care home or hospital settings, particularly with medications [39, 43–45]. The multiple levels of systemic administration in healthcare caused delays of medication changes for one care home resident with PD as the prescription had to be passed from the hospital specialist to the GP, to the pharmacy before finally arriving at the care home [39]. Wrong instructions, delays in medication administration, a lack of awareness and knowledge regarding medication administration and contraindications for specific drugs including dietary requirements by staff were described by PwP in care homes or hospitals [39, 43–45]. The fixed schedules in care homes or hospitals meant that PwP and their caregivers found that they were unable to administer medications at their usual recommended specific time [41, 45]. This inflexibility led to a loss of autonomy that not only impacted their medication schedules, but also their usual routine for personal care and meals [44].
Information
PwP and their caregivers reported that after being diagnosed with PD, they had to learn about PD, how PD progresses, other health conditions, medications, medication side-effects and available resources and services [30, 62]. However, PwP and caregivers across different countries and healthcare systems reported receiving inadequate information from healthcare professionals on topics such as dietary requirements, managing the progression of PD and prognosis of PD [9, 62]. Due to the lack of information provided, PwP and caregivers reported searching for information themselves from the internet or support groups [9, 57]. However, some PwP and caregivers found unhelpful information that was not relevant to their situation which instead caused distress and made them feel worse about living with PD [9, 57]. Other PwP and caregivers actively chose not to search for information and avoided support groups as it reminded them of their inevitable deterioration with PD [40]. Some PwP and caregivers also described their confusion about medical information provided to them, with contradicting information from different healthcare professionals, at times feeling that they have been sent from “pillar to post” [34, 56].
Due to the lack of information regarding the progression and poor prognosis of PD, PwP and caregivers reported that they were unable to prepare for the advanced illness, plan for the future or make decisions about their health [9, 54]. PwP and caregivers across multiple countries including Canada, Denmark, Ireland, Netherlands, Norway, Spain and UK also reported a lack of guidance on relevant healthcare and social services or support that may be available [9, 54–57]. Consequently, they were unable to access help from the appropriate services even though it may be beneficial [9, 56]. Furthermore, caregivers reported a lack of certainty on whether the symptoms of the person they cared for related to the PD or side-effects of medications [38]. They were uncertain about what changes in health circumstances constituted a need to seek help outside of their routine appointments [38]. Caregivers also commented on the lack of preparation and were unsure about what to do during emergency situations such as falls, resuscitation and psychosis due to the lack of information provided from healthcare professionals [48, 54]. Some caregivers described feeling responsible for obtaining information on their own due to the lack of regular appointments and contact with healthcare professionals [62].
Financial challenges
The financial challenges reported by PwP and their caregivers living in different countries with different healthcare systems related to the costs of travel, healthcare appointments, medications and treatments on top of the potential loss of earnings due to PD or caring for someone with PD as well as consideration of living expenses [35, 64]. Furthermore, the costs of private carers and the potential costs of care homes as PD progresses added to their concerns about financial stability [9, 38]. Studies conducted in Africa (Ethiopia and Tanzania) described a lack of medication supply with PwP and caregivers having to source medications themselves and then paying high medications costs [61, 63]. They also described how treatment decisions were made based on affordability of treatment, rather than medical need [63]. The financial burden of medications were also experienced by PwP and caregivers living in developed countries such as the USA, where they described additional high costs for medications despite already paying for medical health insurance cover [35, 48].
Other aspects of treatment burden in PD
Other aspects of treatment burden in PD include the loss of independence, impact of other long-term conditions, lifestyle changes as well as issues related to DBS. Some of these aspects correlate to the subthemes described by Eton’s framework of treatment burden and are highlighted in this section. As their PD progressed, PwP described frustrations due to
Looking after their health with PD meant PwP attended
Impacts of burden
Role and social activity limitation
PwP and caregivers described how their role in life had changed and was spent managing their PD and health, with symptoms and medication efficacy that could be difficult to predict on a daily basis [31, 40]. PwP and caregivers reported how their daily lives were dictated by the schedules of medications and appointments of the person with PD [30]. Having to take medications at different times of the day as well as the variable medication efficacy and side-effects impacted their ability to plan or attend social activities outside of the home [32, 46]. PwP reported increasingly relying on others for help as PD progressed, whilst family members or friends of the person with PD found themselves taking on the role of a caregiver [33, 65]. Caregivers described a loss of independence as their lives now revolved around the PwP with unpredictable symptoms and medication schedules impacting their social activities [46, 51]. Some patients with DBS described how malfunction of the device could prevent them from engaging in new activities or disrupt their usual routine although others enjoyed the spontaneity that DBS gave them, no longer having to plan activities between medication timings [31].
Physical and mental exhaustion of self-care
PwP and caregivers reported that their day was filled with medications, appointments, therapy, diet and exercise; constantly reminding them of their life with PD and increasing recognition that they may not go back to living a normal life [9, 50]. The lack of contact with healthcare professionals meant that PwP and caregivers felt ‘alone’ when managing their PD [54]. Caregivers of PwP found themselves responsible for the health of the person with PD, particularly as PD progresses and the capacity for self-care decreases [9, 33]. Caregivers described how the lack of information and uncertainty of what to expect with PD and having to make decisions about the care of their loved ones with PD was very stressful [48, 54]. The lack of information and access to available support services meant caregivers felt physically and mentally worn out [33, 55]. The inevitable progression of PD and increasing dependence of PwP on their caregivers, who may themselves have a worsening health condition may eventually lead to the person with PD moving into placement to help manage their care [30].
DISCUSSION
To the best of our knowledge, this is the first systematic review to explore the treatment burden in PwP and their caregivers. None of the included articles in this review explored the concept of treatment burden as the primary outcome. Using Eton’s framework of treatment burden, our findings suggest that the main issues of treatment burden in PwP and caregivers relate to: 1) the workload and challenges of taking medications, 2) healthcare provider obstacles at individual and system level and 3) learning about health and poor information provision regarding PD and available resources. Although Eton’s framework was useful in identifying the issues of treatment burden in PD, it was challenging to separate the three themes (workload, challenges, and impact) as described in Eton’s framework. Indeed, these constructs of treatment burden have been shown to correlate with one another in studies involving patients with multiple long-term conditions that have used a patient-reported outcome measure for treatment burden based on Eton’s framework [68, 69]. The main issues that impact the treatment burden in PD appear to be closely interlinked, as shown in Fig. 2.
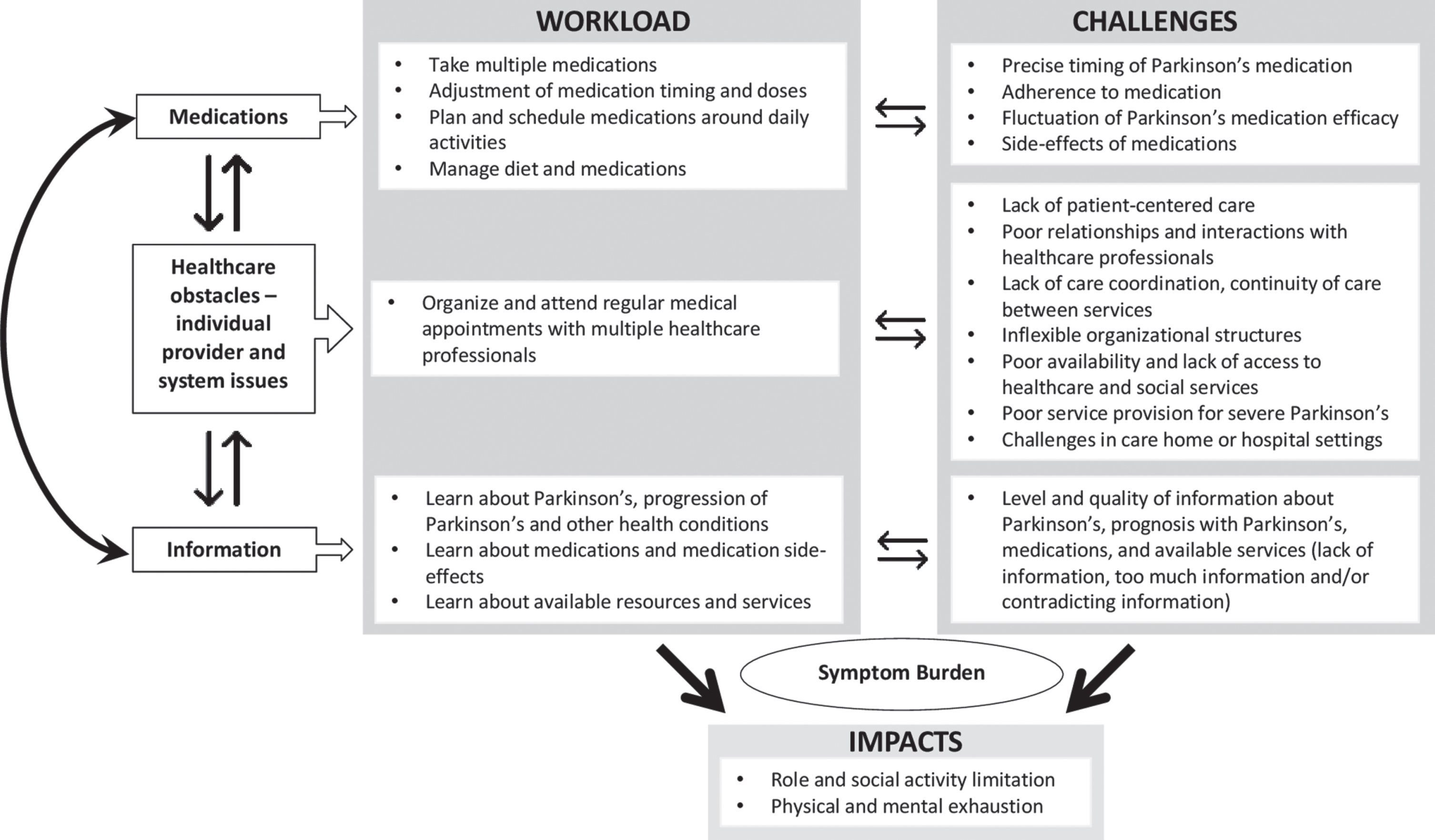
Main components of treatment burden in Parkinson’s.
Firstly, the workload and challenges of medications in PD were closely related. The workload of medications experienced by PwP and caregivers may be increased by challenges such as strict medication timings, variable medication efficacy, medication side-effects and issues with medication adherence. For example, the variable medication efficacy led to frequent changes in medication doses and timings. Similarly, managing the side-effects of medications meant that they took more medications which added to their workload. Secondly, the work of organizing and attending medical appointments was challenging due to the healthcare obstacles faced by PwP and caregivers. At an individual provider level, PwP and caregivers experienced poor relationships with healthcare professionals and a lack of patient-centered care when attending healthcare appointments. They reported a predominant focus on medications or symptoms rather than psychosocial factors that may be more distressing in PD. At a system level, the lack of access to services and lack of coordination between services meant that PwP and caregivers experienced a lack of information or conflicting information about their health. In some cases, this meant that they had to seek out information themselves, increasing the workload. Finally, the work and challenges with information provision added to treatment burden in PD. PwP and caregivers described learning about PD, how it progresses, medications, side-effects and how to access healthcare services. Yet, they experienced poor information provision and difficulty getting suitable levels of information. This meant that they looked for information themselves from support groups or the internet, increasing their workload. Furthermore, poor information provision meant that PwP and caregivers reported a lack of access to health and social care services as they were unaware of the available services to them. Both the workload and challenges of treatment burden impact the lives of PwP and their caregivers and led to limitations in their role and social activity as well as physical and mental exhaustion of self-care. Our review has also highlighted PD-specific issues of treatment burden such as fluctuation of PD medication efficacy, impact of PD symptoms and progression of disease on treatment burden, lack of PD prognostic information, lack of service provision for severe PD, challenges faced in hospital or care home settings with PD and issues related to DBS.
The medications aspect of treatment burden was a recurring issue in PD. This is not surprising given the predominant management of PD with medications. Polypharmacy, complex medication regimes, medication side-effects, coordinating medications, associated stigma and interference of medications on daily activities have been reported as important factors that increased the treatment burden in patients with a chronic illness, multimorbidity (two or more chronic conditions) and heart failure [70–73]. Patients with heart failure experienced the constant changes or adjustments in medications which increased their treatment burden, similar to experiences of medications in PD [70, 73]. Deficiencies of healthcare providers at both individual and system level have also been described as important factors that increased the treatment burden in other long-term conditions [16, 74]. Poor communication, lack of trust and lack of continuity between patients and healthcare professionals have been found to increase the treatment burden in patients with multiple chronic conditions [26, 72]. A study exploring the treatment burden in stroke reported how healthcare provider issues at a system level such as the lack of communication between services led to confusion about medication prescriptions, which resonates with our findings that these issues are closely interlinked in PD [16]. Although PwP and caregivers had various sources of information available, issues with getting appropriate levels of information regarding PD and available services appear to impact on the treatment burden in PD. The lack of information provision is similar to previous literature on treatment burden in stroke, heart failure and chronic kidney disease [73–75]. Similar to our findings, patients with heart failure and chronic kidney disease also reported the lack of prognostic information and unpredictable future faced [18, 77].
Furthermore, caregivers of PwP reported how their daily lives were dictated by medications, appointments and lifestyle changes whilst seeking information about PD and learning how to successfully navigate the healthcare system. They reported that the treatment burden led to changes in their role, loss of independence, feeling isolated due to the lack of support, and being physically and mentally exhausted. Even though we were careful not to extract data related to caregiver burden, our findings suggest that treatment burden experienced by caregivers in PD may be associated with caregiver burden. This is similar to findings from Sav et al who reported that caregivers of people with a chronic condition may experience treatment burden which can lead to distress, frustration and caregivers neglecting their own life and needs, including their health and well-being [10]. The relationship between treatment burden experienced by caregivers and caregiver burden has not been fully explored, and further research is needed.
Whilst we specifically did not extract data related to symptom burden in the review, our findings suggest that the symptom burden in PD may impact the treatment burden and capacity in PwP and caregivers due to the myriad of motor and non-motor symptoms associated with PD. Although symptom burden is a separate concept on its own, changes in disease severity, disease control and co-morbidities are closely linked to treatment burden and capacity [7, 78]. Higher levels of symptom severity is associated with higher levels of treatment burden in studies conducted in older adults with multimorbidity and people living with HIV [79, 80]. However, the impact of symptoms burden on treatment burden in PD has not been researched.
Although a large cohort study found that 31%of PwP have more than five co-morbidities (physical and mental conditions) compared to 13%in patients without PD, aspects of treatment burden associated with long-term health conditions other than PD were mentioned less often than we anticipated in our review [5]. This may be because PwP and their caregivers predominantly experience treatment burden related to PD as they must manage the symptoms and complications of PD on a daily basis compared to other long-term health conditions. A previous study developing and validating the Multimorbidity Treatment Burden Questionnaire (MTBQ) as a measure for treatment burden showed that high treatment burden is associated with higher number of long-term conditions, depression and dementia [81]. All these factors are commonly found in PwP, further supporting our hypothesis that they are a population at risk of experiencing high treatment burden.
Implications
Our findings suggest PwP with high medication burden, those who navigate through multiple healthcare services, as well as those with inadequate information provision may experience high treatment burden. It is equally important for healthcare professionals to be aware that caregivers of PwP may also experience similar issues with treatment burden when helping to support the health of someone with PD. Healthcare professionals need to recognize PwP and caregivers who may have high treatment burden as they are potentially at risk of treatment non-adherence and subsequent poor health outcomes. Establishing patients’ and caregivers’ priorities with good communication and a move towards patient-centered care with a holistic approach by healthcare professionals can play a role in improving the treatment burden in PD [8, 82]. Perhaps reframing healthcare delivery using ‘Minimally Disruptive Medicine’, an approach that considers the impact of the workload of healthcare for people with long-term conditions and moves away from disease-centered guidelines may potentially be beneficial [83–85]. Further research is needed to understand the factors at both an individual and system level that can reduce the treatment burden or enhance the capacity of PwP and caregivers.
Strengths and limitations
Our review included 32 studies that involved caregivers of PwP. This is a strength as a recent systematic review by Sheehan et al. highlighted the lack of research exploring treatment burden experiences in caregivers, with only six studies doing so [86]. These studies involved caregivers of older adults, caregivers of older adults with multimorbidity, caregivers of patients with lung cancer and chronic obstructive pulmonary disease, older adults or caregivers of patients with at least one chronic condition such as diabetes, cardiovascular disease or cancer [10, 87–89]. The use of specific search terms in Sheehan et al.’s systematic review may have led to the exclusion of studies exploring caregiver burden that contained experiences of treatment burden in caregivers. In our review, the broad search terms used led to the inclusion of multiple studies involving caregivers and allowed the interpretation of treatment burden experiences in caregivers of PwP. Data synthesis was conducted using framework synthesis guided by Eton’s framework of treatment burden, although other frameworks such as the Normalization Process Theory and Cumulative Complexity Model have been used for qualitative synthesis of treatment burden experiences [71, 74]. Our review has several limitations. Firstly, none of the studies explored treatment burden as the primary aim. Although we did find various aspects of treatment burden from the included articles, we did not extract data from the original interview transcripts of studies. However, data extraction was conducted by two researchers independently and discussed to increase rigor. Secondly, we included papers published from year 2006 onwards to identify the current experiences of PwP and caregivers following the introduction of the NICE UK PD guidelines, which may be different to PD guidelines in the other countries included in this review. However, exploration of the current experiences will help inform the development and changes to health services and/or policy for service users [23, 74]. Exclusion of grey literature and non-English articles may also be a limitation. However, we did not apply any geographical exclusion in order to capture important experiences across different countries and healthcare systems. Whilst we were careful to include all aspects of treatment burden during data extraction, prior knowledge of Eton’s framework may have influenced data extraction. However, Eton’s framework was created with patients with multimorbidity and therefore suitable for this study as PwP can be considered an exemplar for patients with multimorbidity [5].
CONCLUSIONS
We have explored the experience and influences on treatment burden among PwP and their caregivers which have offered an insight into potential strategies to reduce the treatment burden. Eton’s framework of treatment burden is a robust tool that can be used to understand treatment burden in chronic diseases including PD. Medications, healthcare provider obstacles at individual and system level as well as information provision appear to increase treatment burden in PD. Future research is needed to focus on treatment burden as the main outcome for PwP and their caregivers and identify the potentially modifiable factors that may improve their experiences.
Footnotes
ACKNOWLEDGMENTS
We would like to thank Paula Sands of University of Southampton Health Services Library for her assistance with developing the search strategy.
QYT and LC were also supported by the University of Southampton National Institute for Health Research (NIHR) Academic Clinical Fellow training programme. SERL was supported by the University of Southampton NIHR Academic Clinical Lecturer programme. QYT, SERL, SF, HCR and KI are supported by the NIHR Applied Research Collaboration Wessex; and NJC, HCR and KI by the NIHR Southampton Biomedical Research Centre. The views expressed are those of the authors and not necessarily those of the National Health Service, the NIHR or the Department of Health and Social Care.
CONFLICT OF INTEREST
The authors have no conflicts of interest to report.