
Abstract
Objectives. Many caregivers who care for their children with cancer are affected by the care burden due to the chronic nature of the disease. This study aimed to determine the burden of care level and its related factors in the caregivers of children with cancer. Methods. A facility-based, cross-sectional study was conducted at Tikur Anbessa Specialized Hospital. Children diagnosed with cancer and treated at the hospital between July 1 and August 1, 2023, and their caregivers were included. The data were analyzed using SPSS version 25. Descriptive analysis and inferential statistics were used to summarize the data and to determine the association with the dependent variable. Statistical significance was set at P < .05. Results. A total of 208 children with cancer and their caregivers were included in the study. Most children (81, 38.9%) were below 5 years of age, and 80.3% (n = 167) of the patients came from out of Addis Ababa. The most common type of childhood cancer was haemato-lymphoid cancer (n = 117, 56.3%). The mean duration of cancer care after diagnosis was 289.55 days. The median age of caregivers was 35 ± 8.7 years, most of the caregivers were parents of the child (n = 185, 88.9%), married (n = 186, 87%), had a primary level education (n = 66, 31.7), and 87.5% (n = 182) had insufficient income for the cancer treatment cost. The average caring time was 19 to 24 hours for 76.4% (n = 159) of caregivers, and more than one-fourth of caregivers (n = 57, 27.4%) intended to abandon treatment if they couldn’t get support to continue the care. The mean care burden in caregivers was 65.76 ± 14 and about, 53.4% (n = 111) and 35.1% (n = 73) of caregivers had moderate and severe care burden. Binary logistic analysis showed the factors associated with an increased care burden were the caregiver’s occupational status (P = .034, 95 % CI; AOR (0.064, 0.890)), lack of support from NGOs (P = .037, 95 % CI; AOR (1.053, 5.254), and insufficient monthly income for the treatment (P = .034; 95% CI; AOR (0.064, 0.896)). Conclusion. Most of the caregivers of children with cancer were parents and had insufficient income for the treatment. More than one-fourth had an intention to abandon the cancer treatment. Most caregivers had moderate to severe care burdens.
Keywords
Introduction
Childhood cancers are an important cause of morbidity and mortality around the world with better outcomes observed in high-income countries.1-3 Delay in the diagnosis, lack of access to treatment, abandonment of treatment, treatment-related mortality, and avoidable relapse were the reasons for lower cancer survival rates in low- and middle-income countries.2-7
Several factors related to the caregivers, healthcare professionals, and the type of cancer can cause a delay in the diagnosis and impact the burden on the caregivers.8,9 Having a child diagnosed with cancer might be a tragic phenomenon, causing many problems for the child and imposing a care burden on the caregivers, which can lead to negative health consequences.9-15
The process of childhood cancer treatment can be a stressful experience for the caregivers and their children due to the emergence of various complications associated with treatment, and the course of treatment in phases can change the patterns of family life, and the family tries to cope with the new environment, situations, and needs.9,15-17 In addition, they experience severe emotional and physiological stress during the care process, which leads to physical and mental health problems. Caregivers often feel sadness, depression, anxiety, and disappointment, which can lead to negative health consequences and poor quality of life imposing a care burden on caregivers.18-24
The socio-demographic factors that affect the amount of care burden perceived by caregivers include age, gender, marital status, patient’s age, education, occupation, and monthly income. High care burden may reduce the quality of care to children with cancer and therefore exacerbate their condition causing a vicious cycle with many physical and psychological consequences for caregivers.18,25-30
Many studies showed that caregivers of children with cancer experience high levels of care burden.18,28-35 Early identification of caregivers with care burden is important in promoting their health and improving the quality of care provided to children with chronic care.12,13,18,27,35-39
A study done at Mohammad Kermanshahi Hospital in western Iran about the “care burden and associated factors in caregivers of children with cancer” showed the mean ages of caregivers and patients were 35.7 ± 7.0 and 3.1 ± 1.6 years, respectively. Caregivers had moderate to high care burdens. The factors associated with the care burden were family relationships with the child, marital status, education, occupation, length of caring hours, and age of the child.32,40
More than half of all new cancer cases occur in low- and middle-income countries (LMICs), and sub-Saharan African countries are facing the burden of childhood cancer with a lack of adequate cancer care resources to cope with the health care needs of cancer patients.32,41-46 Considering the adverse consequences of caregiver burden, exploring the pattern of care burden and its related factors in caregivers of children with cancer is crucial for improving supportive care services. However, there are few studies in the field of care burden and related factors in parents of children with cancer in low-income countries, including Ethiopia. Our study aimed to determine the extent of the care burden in the caregivers of children with cancer and the relevant influential factors in Ethiopia.
Methods
All children with cancer aged <15 years who were on treatment between July 1 and August 1, 2023, at Tikur Anbessa Specialized Hospital and their caregivers were included. The study population included children with cancer and the caregivers of children with cancer being treated at Tikur Anbessa Hospital at the Pediatric Hematology-Oncology Unit during the study period.
Sample Size
Based on the results of the study of Chaghazardi et al, 40 with 95% confidence, 5% precision, and a prevalence of care burden of 84% a total of 208 participants were included in the study by convenience sampling method. A total of 208 children with cancer and their caregivers met the inclusion criteria and were included in the study.
Inclusion Criteria
Children with histologically/radiologically confirmed diagnoses of cancer, children with cancer (age 15 or younger without a lower age limit) who started treatment at Tikur Anbessa Specialized Hospital, and caregivers of children with cancer at Tikur Anbessa Specialized Hospital within the study period who signed the data release consent form were included.
Exclusion Criteria
Caregivers of children with benign hematology at Tikur Anbessa Hospital within the study period were excluded from the study.
Instrument
The Study instrument had a socio-demographic characteristic of children and caregivers, and the Novak and Guest’s Caring Burden Inventory (CBI). 44 The socio-demographic characteristics had two parts, the first part of personal information included the demography of the child; age, sex, birth order, diagnosis of childhood cancer, and duration of cancer care. The second part was about the socio-demographic characteristics of the caregivers including age, family relation with the child, educational status, marital status, occupation, monthly income, and average time of child care. The third part addressed the intention to abandon treatment and the demand for cancer support organizations. The final part assessed the level of care burden using the Novak and Guest CBI score. The CBI had 24 items and consisted of five subscales, including time-dependent (questions 1-5), evolutionary (questions 6-10), physical (questions 11-14), social (questions 15-19), and emotional (questions 20-24). The CBI score ranges from 24 to 120. The level of the care burden was classified into mild (24-47), moderate (48-71), severe (72-95), and very severe (96-120). The Amharic version of the CBI questionnaire was pilot-tested on 5% of the sample to ensure data quality. Problems highlighted during the pre-test were corrected before the start of the data collection. Each question was properly coded; the principal investigator did continuous cross-checking during the pre-test and data collection period. The collected data were checked for completeness and consistency on each day of data collection.
Statistical Analysis
Data were collected by the trained two BSc nurses using structured administered questionnaires and with principal investigator supervision. Data were analyzed using the Statistical Package for Social Sciences (SPSS) version 25. Categorical data were described in terms of frequencies and percentages. Tables and charts were created on SPSS version 25 and Microsoft Excel version 2010. Statistical significance was set at P < .05 while assessing the determinant factors.
Ethical Approval and Informed Consent
Ethical approval was obtained from the Research and Publication Committee of the Pediatrics and Child Health Department (DRCP), School of Medicine, College of Health Sciences, Addis Ababa University (REC/587/15), and Addis Ababa Medical and Business College. Written informed consent was obtained from the caregivers for data collection and publication. Confidentiality was fully maintained during data collection and analysis. Participants were anonymous during the dissemination of the results for publication.
Results
Sociodemographic Characteristics of Children With Cancer and Their Caregivers
A total of 208 children with cancer and their caregivers met the study inclusion criteria. The majority of the children (81, 38.9%) were below 5 years of age, and one-fourth (n = 52) of children were above 10 years old. Males constituted 61.2% (n = 127) with a male: female ratio of 1.6:1. The birth order ranged from 1 to 10, and the first and the third birth orders were the most commonly affected by childhood cancer, accounted for 37% (n = 77), and 26.4% (n = 55) respectively. More than three-fourths (167, 80.3%) of the patients came from out of Addis Ababa (Table 1).
Demographic Characteristics of Children with Cancer, Tikur Anbessa Specialized Hospital, Ethiopia, 2023 (n = 208).

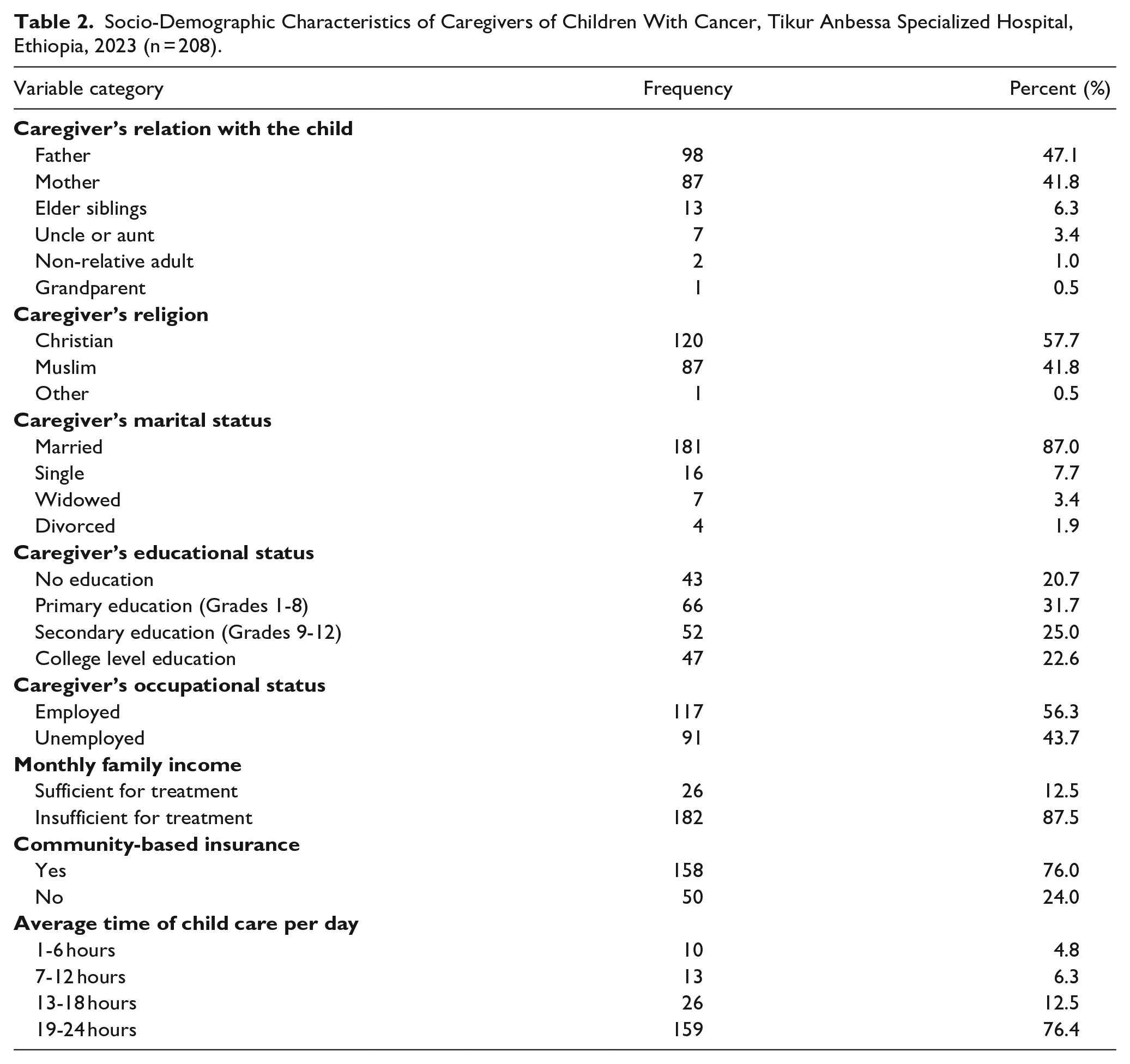
The median age of caregivers was 35 ± 8.7 years with an interquartile range of 17 to 66 years. Most of them were parents of children (n = 185, 88.9%), married (n = 186, 87%), had a primary level education (n = 66, 31.7), and 87.5% (n = 182) had insufficient income for the monthly treatment expense. More than three-fourths (n = 158, 76%) had community-based insurance. The average caring time was 19 to 24 hours for 76.4% (n = 159) of caregivers of children with cancer (Table 2). The most common type of childhood cancer was haemato-lymphoid cancers (n = 117, 56.3%), followed by soft tissue sarcomas (n = 25, 12%; Figure 1, Table 3). The mean duration of cancer care after diagnosis was 289.55 days with an interquartile range of 7 to 2920 days.
Socio-Demographic Characteristics of Caregivers of Children With Cancer, Tikur Anbessa Specialized Hospital, Ethiopia, 2023 (n = 208).

Diagnosis of childhood cancers.
The Type of Cancer in Children and Disease State, Tikur Anbessa Specialized Hospital, Ethiopia, 2023 (n = 208).
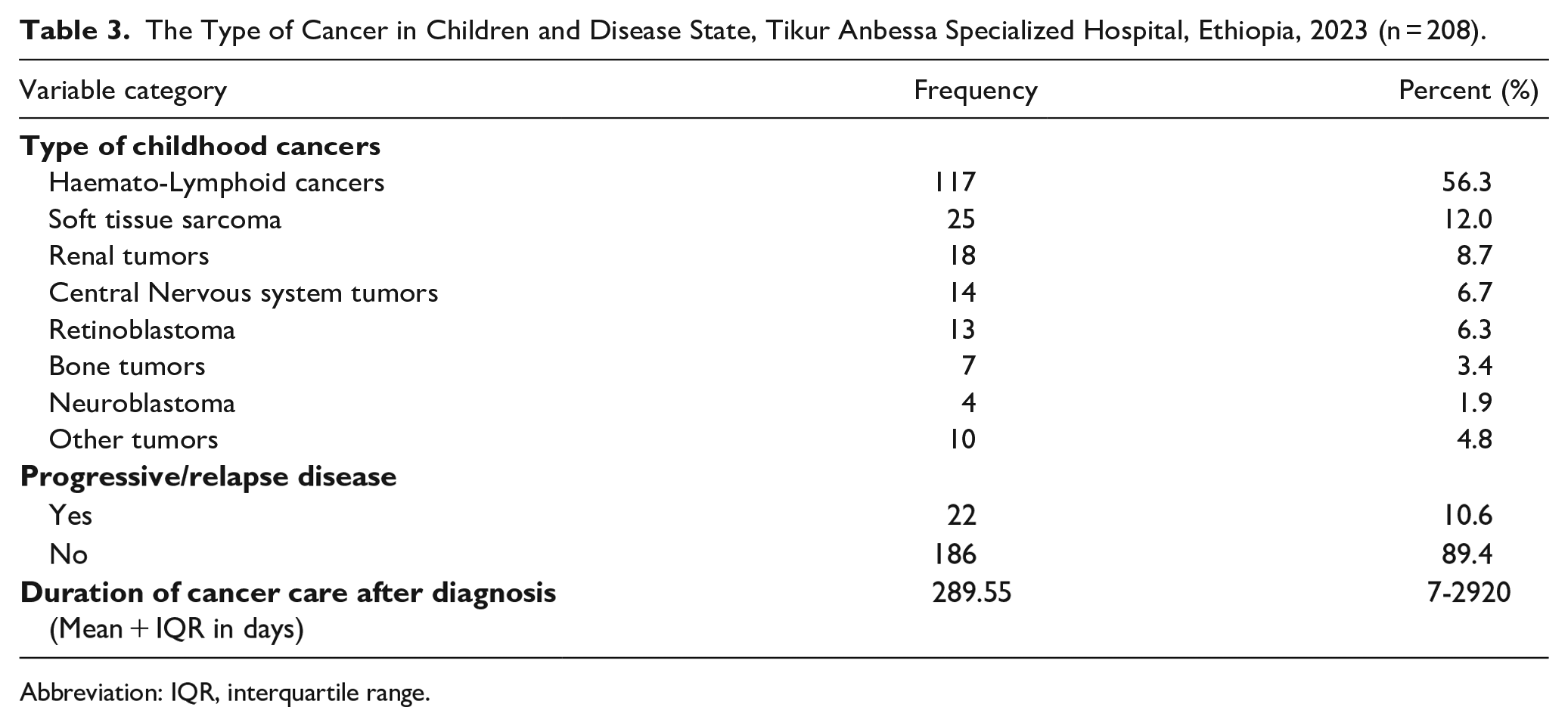
Abbreviation: IQR, interquartile range.
Intention to Treatment Abandonment and the Need of Cancer Supporting Organizations
Less than one-fourth of children with cancer (n = 47, 22.6%) were getting shelter and medications from childhood cancer-supporting organizations. About 10.6% (n = 22) of children had treatment discontinuation, and most of the children, 80.3% came from the regional states of the country for treatment. More than one-fourth of caregivers (n = 57, 27.4%) had an intention to abandon treatment if they couldn’t get support from governmental and non-governmental childhood cancer-supporting organizations (Table 4).
Intention to Treatment Abandonment Among Caregivers of Children With Cancer, Tikur Anbessa Specialized Hospital, Ethiopia, 2023 (n = 208).

Abbreviation: NGOs, non-governmental organizations.
The Magnitude of Care Burden in Caregivers of Children With Cancer
The mean care burden in caregivers of children with cancer was 65.76 ± 14 out of 120 with a range of 32 to 100. About, 53.4% (n = 111) and 35.1% (n = 73) of caregivers had moderate and severe care burdens respectively. About 133 (63.9%) of caregivers had mild and moderate care burden, whereas 75 (36.1%) had severe and very severe care burden as shown in Figure 2.

Magnitude of care burden in caregivers of children with cancer.
Binary logistic regression was used to assess the factors associated with the severity of cancer care burden among caregivers of children with cancer. The odds of severe and very severe cancer care burden in caregivers of children with cancer was decreased by 46.7% (COR = 0.533, 95% CI; 0.253, 1.121) among children aged above 10 years compared to children less than 5 years. The odds of severe and very severe care burden in caregivers of children were increased (COR = 2.83, 95 CI; 1.454, 5.508) in those caregivers who didn’t get support from non-governmental organizations (NGOs) (Table 5).
Factors Associated With the Magnitude Care Burden in Caregivers of Children With Cancer by Binary Regression (N = 208).
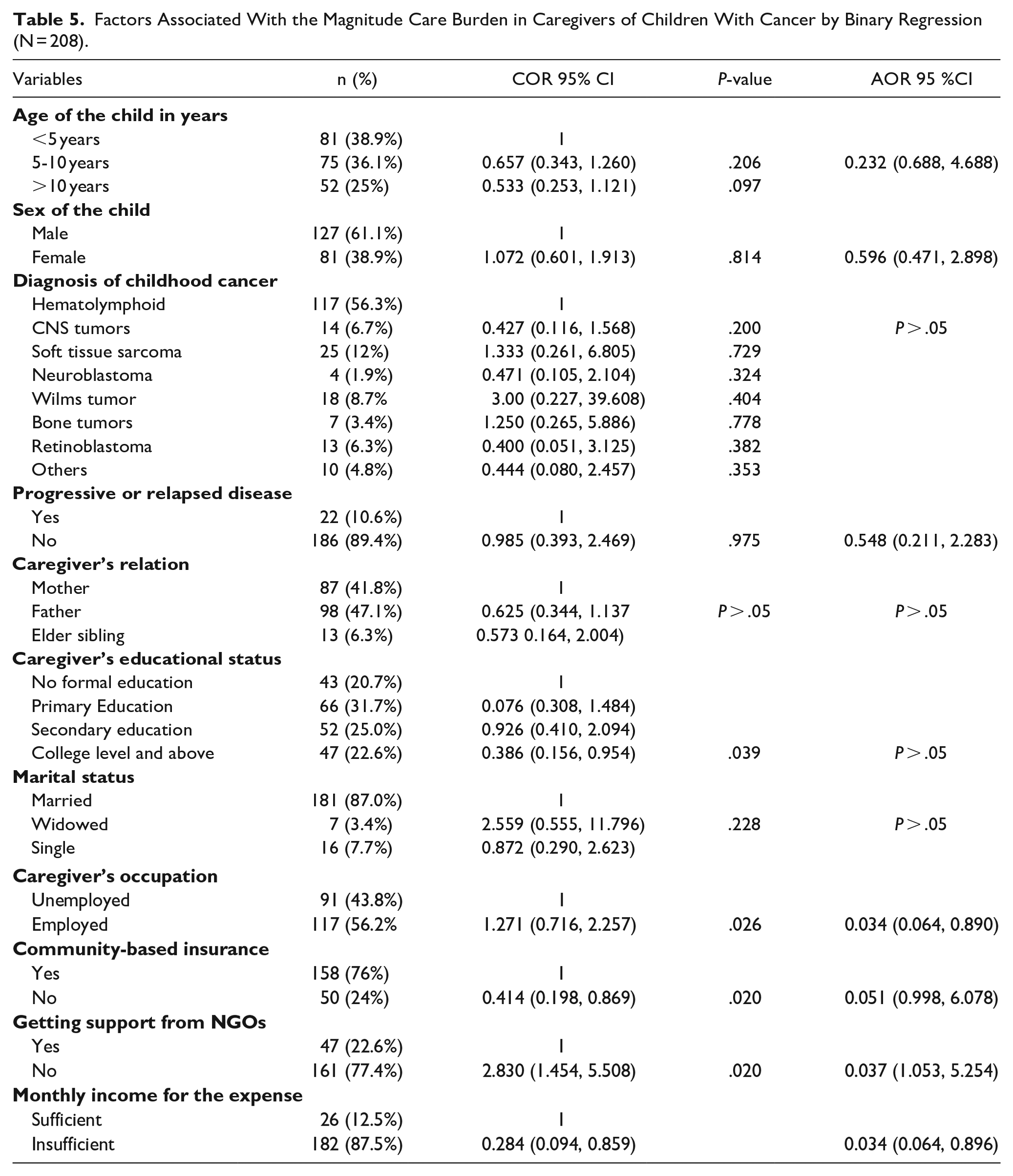
The factors associated with increased care burden were the caregiver’s educational status (P = .039), caregiver’s employment status (P = .026), community-based insurance ( P = .020), support from non-governmental organizations (P = .002), and monthly income for the medical expense (P = .034). Adjusted odd ratio (AOR) was done to control the predictors and showed the factors associated with an increased care burden were the caregiver’s occupational status (P = .034, 95% CI; 0.064, 0.890), lack of support from NGOs (P = .037, 95% CI; 1.053, 5.254), and insufficient monthly income for the treatment (P = .034; 0.064, 0.896).
Discussion
This study was conducted in one of the largest tertiary referral hospitals in Ethiopia serving as the only center for pediatric cancer patients until recently. This cross-sectional study was conducted to assess the level of care burden and associated factors in caregivers of children with cancer in Ethiopia. The median age of caregivers was 35 years with an interquartile range of 17 to 66 years, and most of the caregivers were parents of the child (89%). More than a third-fourth of caregivers had insufficient income for the monthly treatment expense. The average caring time was 19 to 24 hours for most caregivers of children with cancer. These findings are similar to the previous studies done on different continents.27,28,32,35,38,39
Having a child with cancer can fundamentally change the family life, putting parents in a difficult and stressful situation and making them experience a lot of care burden. Haemato-lymphoid cancers were the most common type of childhood cancer followed by soft tissue sarcomas followed by soft tissue sarcomas (n = 25, 12%).
More than one-fourth of caregivers (n = 57, 27.4%) had an intention to abandon treatment if they couldn’t get support from governmental and non-governmental childhood cancer-supporting organizations.
Our study showed that the majority of caregivers of children with cancer have a moderate to severe care burden (89.4%). Multiple factors can cause a care burden for the caregivers of children with cancer, including the challenges associated with cancer treatment, financial problems, lack of information about the course of the disease, feelings of inadequacy, worries about the future of the child, and disorganized family life.28,32 Binary logistic regression analysis showed the factors associated with the severity of cancer care burden among caregivers of children with cancer. The odds of severe and very severe cancer care burden in caregivers of children with cancer was decreased by 46.7% (COR = 0.533, 95% CI; 0.253, 1.121) among children aged above 10 years compared to children less than 5 years. This might be due to the fact children become more independent as age increases, this finding is supported by the previous studies. 32
The odds of severe and very severe care burden in caregivers of children were increased (COR = 2.83, 95% CI; 1.454, 5.508) in those caregivers who didn’t get support from non-governmental organizations (NGOs).
The factors associated with increased care burden were the caregiver’s educational status (P = .039), caregiver’s employment status (P = .026), community-based insurance (P = .020), support from non-governmental organizations (P = .002), and monthly income for the medical expense (P = .034). Adjusted odd ratio (AOR) was done to control the predictors and showed the factors associated with an increased care burden were the caregiver’s occupational status (P = .034, 95 % CI; 0.064, 0.890), lack of support from NGOs (P = .037, 95% CI; 1.053, 5.254), and insufficient monthly income for the treatment (P = .034; 0.064, 0.896). In this study, we report the magnitude of the care burden in caregivers of children with cancer in Ethiopia. The stage of cancer in children and the time to diagnosis can affect the magnitude of the care burden on caregivers, which was not considered in the current study. The other limitation of this study is related to the nature of cross-sectional studies. In these studies, it is not possible to determine the cause-and-effect relationships between the studied variables, and the current study is no exception to this limitation.
Conclusion and Recommendations
This study demonstrated that most parents of children with cancer suffered from a moderate to severe care burden. These findings underscore the need for healthcare providers to plan and implement holistic interventions to reduce the care burden among parents of children with cancer and to improve the care quality of children. These might include prioritizing the efficient use of national resources in a way that assures equity in cancer care, adapting the governmental and non-governmental organization of childhood cancer care and the pediatric oncology workforce to promote full population coverage of high-quality comprehensive cancer services, including geographic accessibility through establishing satellite clinics in the nearby, strengthening regional and national partnerships for childhood cancer treatment, as well as international collaborative projects addressing the care burden in the cancer care. The cancer care should provide long-term care needs of all children with cancer, and their caregivers. It should also assure patients have enough insurance coverage for adequate cancer care, which plays a major role in decreasing the financial toxicity and distress among the caregivers. In addition, the development of comprehensive supportive care to improve the quality of life of children and their caregivers is needed. Future prospective studies are recommended to determine the causal relation with the magnitude of cancer care burden.
Supplemental Material
sj-docx-1-gph-10.1177_2333794X241275258 – Supplemental material for The Magnitude of Care Burden and Associated Factors in Caregivers of Children with Cancer at the Country’s Largest Tertiary Referral Hospital, Ethiopia: A Cross-Sectional Study
Supplemental material, sj-docx-1-gph-10.1177_2333794X241275258 for The Magnitude of Care Burden and Associated Factors in Caregivers of Children with Cancer at the Country’s Largest Tertiary Referral Hospital, Ethiopia: A Cross-Sectional Study by Gashaw Arega, Abdulkadir M. Said, Sosina Workineh, Kedir Hussien and Kassahun Ketema in Global Pediatric Health
Footnotes
Acknowledgements
We thank the Addis Ababa Medical and Business College and Addis Ababa University for allowing us to conduct this study. We express our deep gratitude and respect to the patients and their attendants, who passed through their treatment course and disease state challenges.
Author Contributions
All authors (GA, AM, SW, KH, and KK) made a significant contribution to the, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Availability of Data
Data are available upon reasonable request from the corresponding author.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.