
Abstract
Background:
The onset of freezing of gait (FOG) represents a turning point in the lives of patients with Parkinson’s disease (PD). FOG increases fall risk and is associated with worse physical and mental health related quality of life, thus increasing disease burden. Moreover, therapeutic studies aiming to ameliorate freezing have had limited success. In a step towards pre-emptive therapy to delay or prevent the onset of FOG, this prospective cohort study set out to uncover clinical markers of conversion to FOG.
Objective:
Investigate clinical markers of conversion to FOG.
Methods:
Sixty PD patients without FOG were followed up for two years and underwent extensive clinical testing each year. FOG classification was made with the New Freezing of Gait Questionnaire. Clinical predictors of conversion to FOG were investigated using univariate analysis and through building a multivariable model using all measured components.
Results:
Twelve patients developed FOG during the study (Incidence: 11.5% per year). Due to the large number of predictors, univariate analyses did not survive multiple comparison correction, precluding strong inference on any one predictor. Overall, the effect sizes suggested that motor deficits including difficulties with repetitive movement scaling (AUC: 0.71), coordination (AUC: 0.73) and consistency (AUC: 0.76) as well as gait asymmetry (AUC: 0.79) and variability (AUC: 0.71) were most predictive of conversion. Further, converters reported more subjective cognitive difficulty (AUC: 0.74), although their measured performance was similar to non-converters. Multivariable analyses further showed that the two components most consistently selected in the predictive model were: 1) an MDS-UPDRS component with worse axial motor, hand use and non-motor symptoms; and 2) finger tapping abnormalities.
Conclusion:
Conversion to FOG was predicted mainly by objective and clinical measures of motor dyscontrol, as non-motor disturbances were surfacing. Although based on a small cohort with limited converters, this novel finding informs future studies aimed at FOG prevention.
Keywords
INTRODUCTION
Freezing of gait (FOG) is a complex, episodic and debilitating phenomenon [1] commonly seen in advanced Parkinson’s disease (PD). Once the FOG milestone is achieved, patients are at a higher risk of falls [2], experience more anxiety [3], and have a lower quality of life [4], thereby amplifying disease burden. Prevalence rates of FOG have been reported to go from about 25% in the early stages to 80% in the later stages [5], indicating that a majority of patients will develop FOG during the course of the disease. Furthermore, FOG shows only a partial response to medication [6] and current rehabilitation [7], possibly due to limited motor learning potential in freezers [8–10]. If we are to move towards pre-emptive treatment to delay this milestone, clinical markers of the onset of FOG – conversion – are essential.
Several longitudinal studies including the DATATOP trial [11], Stavanger Parkinson Project [12], Parkinson’s Progression Markers Initiative [13], two Chinese studies [14, 15], an Israeli study [16], and an Australian study [17] have proposed various risk factors for developing FOG based on clinical data in existing data sets, using various conversion criteria. These predictors include left-sided disease onset [11], early lower limb or gait symptom onset [11, 15], worse axial symptoms including speech, bradykinesia, and rigidity [11], higher daily dose of levodopa [12, 17], an akinetic rigid subtype [14], lower education [14], more cognitive [13–15] and sleep disturbance [13, 14], poorer balance [11, 16], presence of falls, gait festination, and hallucinations [15], depression [15–17], anxiety [14, 17], and unsurprisingly, FOG severity [17]. Although highly informative for understanding global risk profiles, these studies have low clinical applicability in terms of providing specific or sensitive markers for screening patients at risk of conversion. None of these studies used objective measures to quantify performance, which seem to be more reliable and responsive compared to clinician rated measures [18]. Furthermore, it is presently unknown how these risk factors from various motor and non-motor spheres compare with each other, which is key to understanding the mechanisms of FOG and to developing an effective FOG prevention plan.
In this study, we wanted to go beyond the state of the art and prospectively follow up a group of Non-Freezers for two years, supplementing the clinical markers used in previous studies with instrumented tests to precisely measure motor control deficits such as asymmetry, movement variability, dysmetric amplitude and frequency abnormalities (or freezing indexes based on altered frequency spectra). Based on the studies mentioned above as well as previous cross-sectional work [19–24], we selected seven motor and non-motor spheres likely involved in FOG, including disease rating, cognition, affect, balance, gait (including dual tasking), turning (360° – including dual tasking) and repetitive movements of extremities. The main aim of this study was to determine which clinical markers were most predictive of conversion to FOG within the next year. We did this by assessing univariate discriminative ability as well as through building a multivariable prediction model using all motor and non-motor components.
METHODS
Participants
This prospective cohort study followed up 60 PD patients without FOG for two years and assessed them every twelve months (Baseline – first FU – second FU). Idiopathic PD (UK PDS Brain Bank criteria) patients with Hoehn & Yahr (H&Y) Stages 1– 3 were recruited from the Movement Disorders Clinic of the University Hospital in Leuven, Belgium as well as through a PD patient database. Patients who had never previously experienced FOG and were able to walk independently for 10 minutes were considered eligible. Patients with Deep Brain Stimulators, dementia (Mini-Mental Status Examination <24) or comorbidity other than PD affecting cognitive or motor function were excluded. Recruitment of patients began in August 2012 and final assessments were completed in May 2016. All measurements were performed while “OFF” medication— at least 12 hours after the last medication dose— and at the same time of day as the previous measurements. The study was approved by the Ethics Committee of the University Hospital / KU Leuven (Study number: B322201215418). Patients signed informed consent prior to participation in compliance with the Declaration of Helsinki.
Classification
Objective FOG detection is often compromised by false negatives [25], therefore classification of FOG at study entry and subsequently was made by patients’ response to the first question of the New Freezing of Gait Questionnaire [26]. This involved indication whether they had experienced FOG in the past month after showing them a video of different types of freezing episodes, including very mild ones. Once a patient had been classified as having developed FOG, the classification remained, irrespective of response to medication at following measurement.
Disease rating
Clinical descriptors, and the Movement Disorders Society revision of the Unified Parkinson’s Disease Rating Scale (MDS-UPDRS) were assessed by interview and examination of the patient, as well as information about daily Levodopa equivalent dose (LEDD) and non-Levodopa medication prescription. Self-reported outcomes of the MDS-UPDRS were based on how patients felt most of the time over the past week, as per the guidelines [27], thus while following their regular medication schedule.
Balance and falls
Patients maintained a falls diary in order to measure retrospective 6-month fall frequency at each follow-up (FU). The Falls Efficacy Scale [28] was completed as a measure of balance confidence while the validated and widely used MiniBEST [29] was used to measure balance performance.
Cognition and affect
An extensive cognitive battery evaluated both global cognition as well as specific executive functions. The tests included the Mini-Mental Status Examination, Montreal Cognitive Assessment (MoCA), Scales for Outcomes of Parkinson’s Disease – Cognition [30], Frontal Assessment Battery [31], Alternate Naming Test and Alternate Intake Test, Rey-Osterrieth figure, and Trail Making Test. In order to quantify affect, the Hospital Anxiety and Depression scale [32] was used.
Gait and turning with dual task
Motor tests were performed in a Movement Analysis Laboratory with a 10 camera VICON 3D motion analysis system. For gait measurements, patients were asked to walk back and forth across the lab at a self-selected comfortable pace. Segments of straight line walking without acceleration or deceleration were recorded until at least 30 steps were captured [33]. Vertical velocity components of the heel and toe markers were used to determine gait events [34] and to calculate spatiotemporal parameters of gait.
A validated auditory Stroop task was added to assess dual tasking ability [35]. For this cognitive task, the Dutch words for ‘low’ and ‘high’ were presented to the patient through headphones in either a low or a high pitch. Patients were asked to name the pitch. The task was first performed in sitting to ensure compliance and synchronized with the VICON system in order to capture the response time. A single rapid 360° turn [21] (three trials, to each side) with a narrow radius was assessed for the time and the number of steps taken to complete the turn. This was also performed with and without the auditory Stroop.
Upper and lower limb repetitive movements
Finger Tapping, i.e., alternate flexion and extension of the index finger was recorded with analog encoders (spatial resolution: 0.0001°) using previously published methods [36]. Repetitive movements of the lower limbs, namely Toe Tapping and Foot Tapping (performed similarly to the MDS-UPDRS tasks), and the Stepping in Place task, previously found to elicit freezing-like behavior [37] were also assessed. Performance of the lower limb tasks was registered through retroflective markers placed on the toe for Toe Tapping, knee for Foot Tapping, and ankle for Stepping in Place using the vertical component of their spatial signal. To prompt standardized performance, movements were initially cued for each side using an auditory metronome – 1.63 Hz for the Finger Tapping and 1.48 Hz for lower limb tasks, and uncued performance over the next 20– 25 repetitions was assessed. Cueing frequencies to prime the upper and lower limb sequences were first piloted to determine a comfortable pace.
In all of these tasks, three trials (both bimanual and unimanual) were performed with a rest period in between and non-freezing movement trials were averaged to extract the amplitude, frequency, freezing index (ratio of power spectral density in the freeze (3– 8 Hz) compared to locomotor (0– 3 Hz) bands) [38], bilateral coordination (relative phase error – degree of deviation from relative phase difference of 180°) [39] and inconsistency of movement (expressed as a coefficient of variation – SD/Mean * 100).
Data analysis
In order to have comparable time-to-event for patients that presented with FOG at the first FU (Early CONV) and second FU (Late CONV), a combined dataset was constructed using the information from the measurement before conversion to FOG, specifically using: Baseline information for Early CONV Information at first FU for Late CONV Information at first FU for non-converters (NCONV)
Univariate analysis
To evaluate the discriminative power of the markers, Area under the Curve (AUC) of 450 possible predictors from all seven spheres were assessed. The AUC represents the probability that a predictor would rank a randomly chosen positive case (in this instance CONV) higher than a randomly chosen negative case (NCONV) and is closely related to the non-parametric Mann-Whitney U [40].
In order to overcome problems of power related to missingness in the Baseline and first FU data (only 14.3% cases with no missing observations, average missingness: 4.1%, median missingness per observation: 0.9%, median missingness per measure: 1.78%), multiple imputation was applied for each measure across all time points (FOG status, baseline, first FU and second FU information included in an imputation model with no missing values for FOG status; single chain Markov Chain Monte Carlo method; 10 imputations). Emphasis is placed on the discriminative power rather than the probability values associated with the Wald test, as the objective is to evaluate performance rather than significance. Predictors with an AUC ≥0.7 are discussed in the results (AUC of 0.5 = random prediction, AUC of 1 = perfect discrimination).
Multivariable prediction model
The main prediction model was built using the combined dataset in order to bring together Early and Late CONV. If no information at first FU was available for any measure, single imputation using baseline information was performed (this was done for 11 NCONV and 1 CONV). To avoid overfitting and to improve generalization of the prediction model, we adopted the following rigorous model building and validation approach.
The first stage of the model building involved division of the predictors into 12 domains based on the earlier mentioned 7 motor and non-motor spheres found to be of relevance [11– 17, 37]. These included Disease Rating, Cognition, Anxiety, Depression, Balance, Single-Task Gait, Dual-Task Gait, Turning, Finger Tapping, Toe Tapping, Foot Tapping, and Stepping In Place. For clinical data, individual item sub-scores were included wherever possible. For instrumented data, measures of central tendency (averages) and spread (coefficient of variation) were included. Principal Component Analysis (PCA) was used per domain to reduce the dimensionality within each domain and retain core components. The number of components to be extracted was determined by parallel analysis [41]. Forty-five factors from the 12 domains were retained; rotated (Varimax), and the regression scores were saved. In the third stage, the 45 factors were considered as possible predictors of conversion to FOG using univariate logistic regressions. Factors that were significant at P < 0.05 were examined for multicollinearity (VIF > 2.5). Those that survived this step were included in a multivariable logistic regression with backward selection (P-stay = 0.1), assuming additivity and linearity. To handle overfitting, a simple bootstrap procedure [42] was used to evaluate the performance of the model. More specifically, 200 datasets were drawn with replacement from the original dataset. In each of these datasets, a multivariable model was obtained using the approach outlined in stage three. The performance of each of these models was evaluated in the original sample and the average performance is reported.
All analyses were performed using SAS software, version 9.4 of the SAS System for Windows (SAS Institute Inc., Cary, NC, USA) and IBM SPSS Statistics for Windows, Version 24.0 (Armonk, NY: IBM Corp).
RESULTS
Study participants and dropout
60 PD patients, who had not previously experienced FOG, took part in this study (Median Age = 59.5, range 40– 77 years; Median H&Y = 2, range 1 – 3; Median Disease Duration = 5, range 1– 14 years). All participants were receiving oral Levodopa or dopamine agonist medication prescribed by a neurologist or movement disorder specialist and 64% of participants also received non-dopaminergic medication including antimuscarinics (5%), MAO-B inhibitors (45%) and glutamate antagonists (1.6%). Nine patients (15%) dropped out over the study – 4 after baseline assessment and 5 after the first year follow-up (Fig. 1). Comparing the dropouts at each time point revealed no significant differences that would indicate more severe disease or cognitive or motor decline. As the subsequent FOG status was not definitively known, the four patients that dropped out after the baseline assessments were excluded from all further analyses.
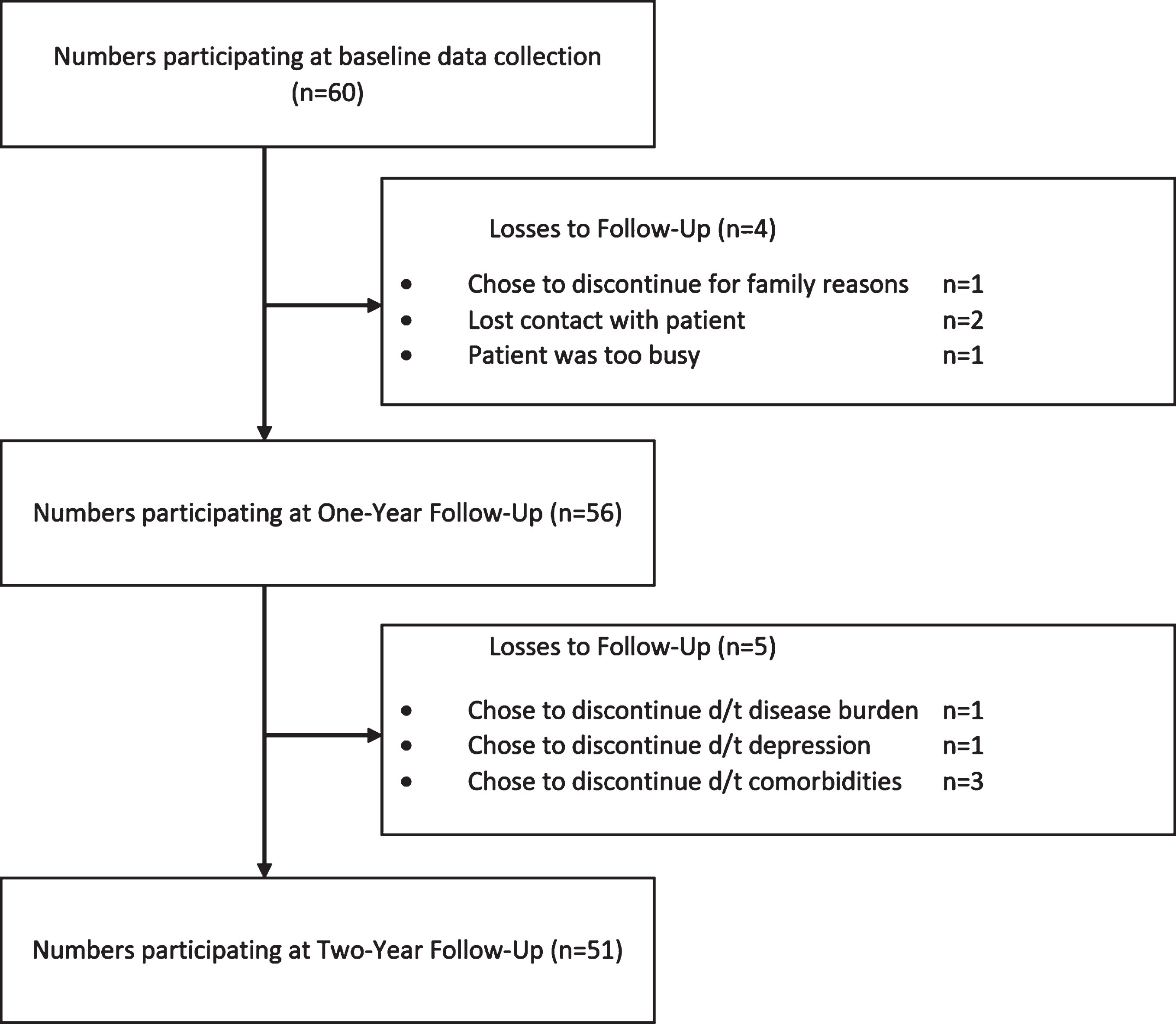
Study Outline showing number of PD participants at each Follow-Up (FU) along with reasons for dropout.
Conversion to FOG
During the Two-Year study, twelve patients developed FOG – six in each year (Incidence: 11.5% per year). At study entry, no significant demographic differences were found between CONV and NCONV or between Early CONV and Late CONV (Table 1). Further, no significant differences were seen for medication prescription for any medication subclass. Converters were spread across a large range of age (Median Age = 56, IQR = 21) and disease duration (Median Disease Duration = 7, IQR = 5.8). Seven of the twelve CONV (58%) had disease onset before the age of 50. At the moment of detection, CONV reported short freezing episodes (<5 s) during turning and at gait initiation but little impact of freezing on quality of life (Median NFOG-Q = 7, IQR = 4.5).
Baseline comparison between Converters (CONV) and Non-converters (NCONV) and between converters at FU 1 (Early CONV) and converters at FU 2 (Late CONV)
Group median (interquartile range) or number (percentage) along with p-values reported. a: Mann-Whitney U for CONV-NCONV, b: χ2 Likelihood Ratio for CONV-NCONV, c: Mann-Whitney U for Early – Late CONV, d: χ2 Likelihood Ratio for Early – Late CONV.
Predictors of conversion within the following year (Univariate results)
At the measurement before conversion, the most prominent markers (AUC≥0.7) in the pooled dataset involving 12 converters were investigated within each motor and non-motor sphere. Due to the large number of predictors included, no significant probability values were found for the Wald test after correction for multiple comparisons based on the false discovery rate, thus precluding strong inference for any one predictor. However, predictors with high discriminative ability are more likely to differentiate converters from non-converters, providing useful information for future prediction work; hence, we focus only on this measure. From gait measures, gait asymmetry during Single Task Gait (AUC: 0.79) as well as during Dual Task Gait (AUC: 0.75) was found to be most discriminative, followed by swing time variability (AUC: 0.71) during Single Task Gait. Problems with repetitive movement tasks were also seen for CONV in Finger Tapping (more amplitude inconsistency AUC: 0.76, more relative phase inconsistency AUC: 0.73, smaller amplitude AUC: 0.71) and Toe Tapping (more relative phase inconsistency AUC: 0.7). CONV also had worse scores on the MDS-UPDRS non-motor sub-scale particularly on items related to cognition (AUC: 0.74), pain (AUC: 0.70) as well as on the MDS-UPDRS motor sub-score for neck (AUC: 0.71) and upper limb (0.70) rigidity. Contrastingly, performance on objective measures of Cognition, Affect, Balance and Turning was not more affected at this time (Table 2).
Univariate One Year Markers of Conversion – Top three predictors of conversion to FOG within each sphere of behavior are shown based on the Area Under the Curve (AUC). Univariate Logistic Regression Odds ratios and confidence intervals along with p-values are also reported. Measures with an AUC > 0.70 have good discriminative ability; however, none of the associated probability values survived multiple comparison correction
Multi-domain multivariable prediction model
The forty-five components representing all the measured clinical information were used to build a model for prediction of conversion to FOG. The final model had a bootstrap-averaged accuracy of 87.1% (Pcutoff: 0.5) with a sensitivity of 61.8% and specificity of 93.3%. The bootstrap-averaged AUC was 0.79 (closer to 1 is better) and Brier Score was 0.14 (closer to 0 is better) indicating that the model performance was fair to good. An MDS-UPDRS component was selected most frequently (63% of resamples) followed by a Finger Tapping performance component (40% of resamples) (Fig. 2A). Axial items from the MDS-UPDRS Part II and Part III as well as items related to hand function (Part II) and non-motor function (Part I) loaded strongly on the MDS-UPDRS component, while amplitude and rhythm inconsistency, relative phase inconsistency, and frequency and amplitude of movement loaded strongly on the Finger Tapping component (Fig. 3). Besides the two components mentioned, others that were selected in the model in more than 10% of the samples included: two Single-Task Gait components (gait variability & gait speed), two Dual-Task Gait components (gait asymmetry and step width), a Toe Tapping component (amplitude), a Stepping in Place component (amplitude inconsistency), another MDS-UPDRS component (motor upper limb + axial), a Cognitive component (Stroop response time during walking) and Depression (Fig. 2A).
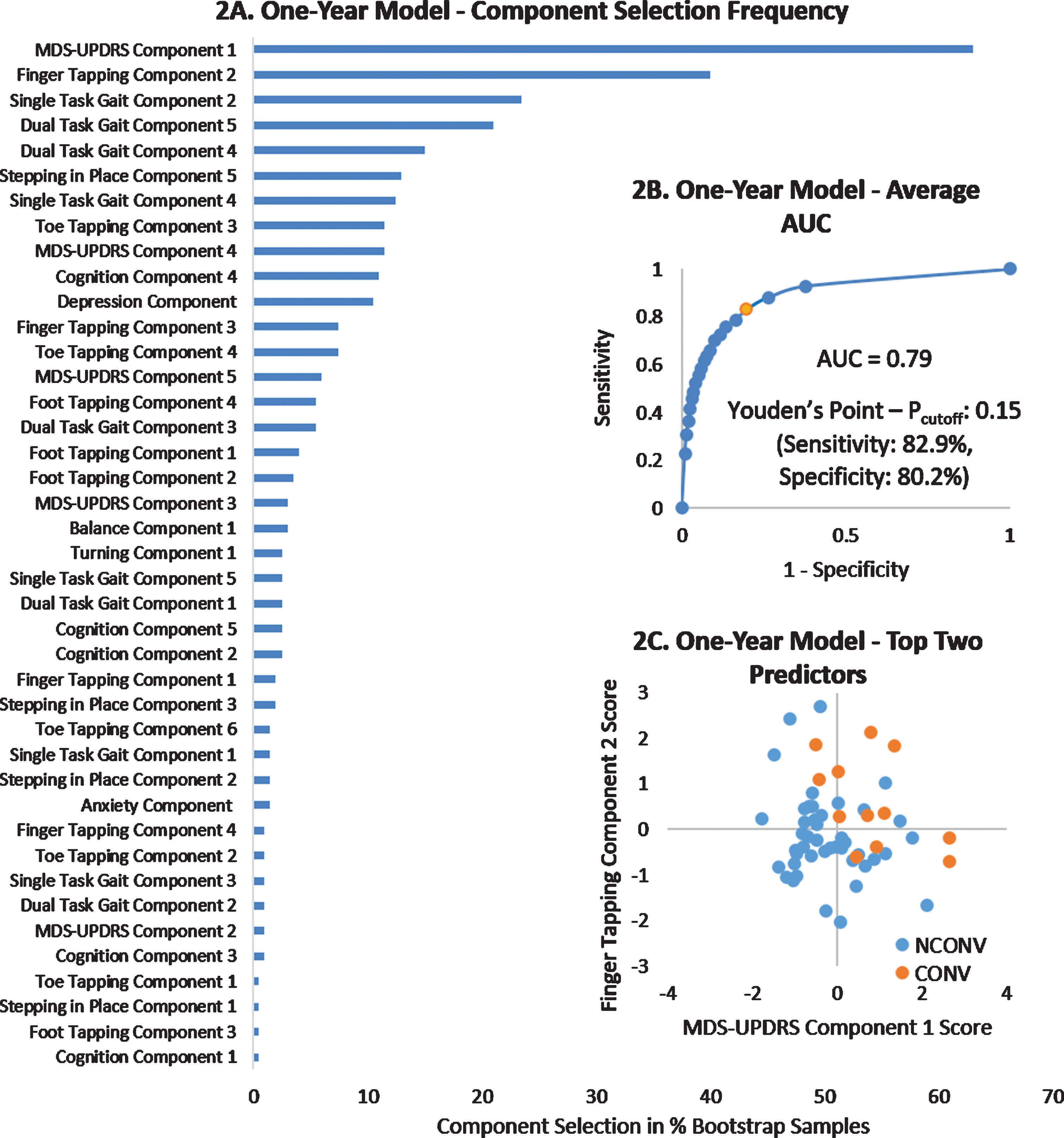
One-Year Prediction model selection and performance. Part A: Selection of variables in the final model in percent (of the 200 bootstrap models). Part B: Average Area Under the Curve (AUC) of the final model along with the predicted probability cutoff for maximum Youden’s point (in orange) indicating the classification probability cutoff (Pcutoff) for optimal model performance. Part C: Scatter plot of regression scores on the two most frequently selected measures showing that CONV had higher (worse) scores on both components.
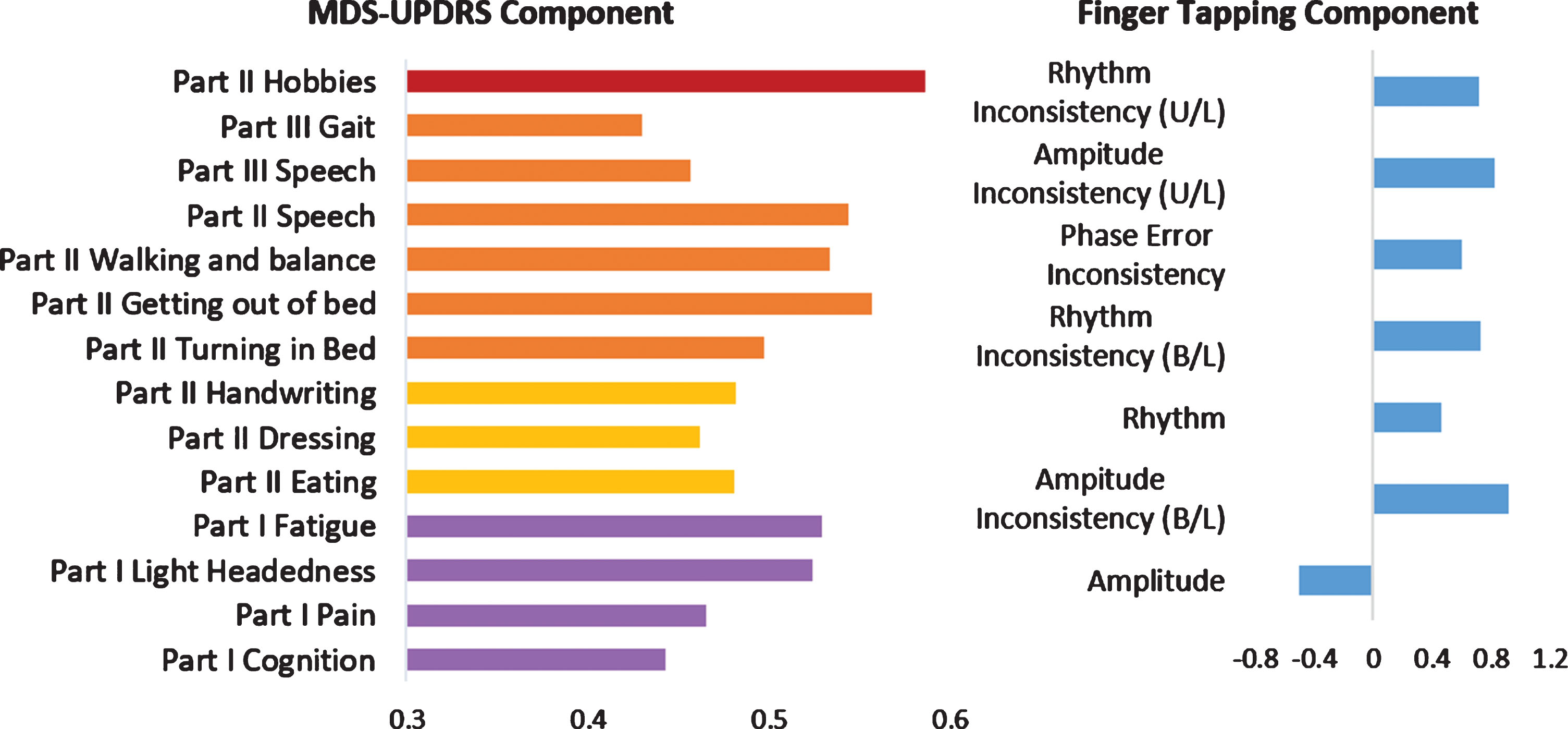
Top Two Components of One-Year model – Variable loading on MDS-UPDRS and Finger Tapping components (cutoff ±0.4). MDS-UPDRS items can be further grouped into Axial symptoms (Orange), Hand dexterity symptoms (Yellow) and Non-Motor symptoms (Purple). Positive loading indicates larger values loaded more strongly on component score, while negative loading indicates smaller values loaded more strongly on component score. U/L: Unilateral tapping, B/L: Bilateral Tapping.
DISCUSSION
In this prospective study, we used a data-driven multidimensional approach to investigate the most sensitive markers of conversion to FOG when measured OFF-medication. We found that gait asymmetry and inconsistency in both scaling and rhythm of repetitive limb movements were able to discriminate between those patients that would or would not develop FOG within the next year. We used robust methodology to build and evaluate a model of conversion within the next year and found that just two components were consistently predictive of conversion. These components were worse MDS-UPDRS based disease rating with a specific profile related to axial motor, hand use and non-motor symptoms, as well as smaller amplitude, more inconsistent and poorly coordinated Finger Tapping movements. The results of this study also show for the first time that motor dyscontrol during non-gait repetitive movement outside of freezing and festination episodes precede and predict conversion to FOG, in contrast to Delval et al., 2016 who showed a similar pattern but for episodic features [43]. In the next section, we consider the relevant findings within each clinical sphere.
MDS-UPDRS disease rating
An MDS-UPDRS component loading on speech, turning in bed and getting out of bed, hand use, walking and balance, and cognitive and autonomic dysfunction (Fig. 3) was most consistently selected in the prediction model indicating that this specific clinical profile is strongly associated with conversion to FOG. This finding is particularly encouraging, as the MDS-UPDRS is widely used clinically, and these results suggest that screening FOG conversion risk may be quickly and reliably performed in a clinical setting.
The axial motor findings confirm previous work [11, 14] and might reflect a greater striatal dopaminergic deficit in these patients, supported by PET results from the PPMI cohort [44]. Items related to hand use loaded strongly on the component, possibly reflecting topographic spread from the face to the hands, as the disease progresses ventrally. The arrangement of the motor homunculi in the striatum [45] and findings from prodromal PD with REM sleep behavior disorder [46] corroborate this pattern of progression in conversion to FOG. Apart from motor symptoms, self-reported non-motor symptoms were also found to be affected, as also reported in other studies [13–15]. These non-motor symptoms might reflect spread of the synucleinopathy to non-dopaminergic neurotransmitter systems giving rise to the cognitive [21, 47– 50], affective [3, 51], and postural [22] deficits later seen in Freezers.
Cognition and affect
Seemingly contrasting results were found for cognitive outcomes – in that, while converters did not perform worse on any of the cognitive tests, they did report more cognitive difficulties compared to non-converters prior to conversion. Further, a cognitive component was selected in the prediction model, which loaded strongly on the auditory Stroop response time while walking and turning (fluctuating attention). These findings suggest that cognitive reserve is declining in this population, which is only evident during challenging dual task situations.
In line with previous studies [11, 52], we found that a depression component was selected in the prediction model in 10% of the bootstrap samples and might indicate involvement of serotonergic systems prior to conversion. Contrary to other work [17], anxiety did not predict conversion in this cohort, and might surface as an early consequence of experiencing FOG [3].
Repetitive movements
We found evidence of widespread spatiotemporal motor dyscontrol by way of smaller amplitudes, amplitude and rhythm inconsistency, higher freezing index as well as bilateral coordination deficits during repetitive movements before conversion. These deficits were witnessed in multiple tasks involving upper and lower limbs, particularly Finger Tapping and Toe Tapping and during unimanual as well as bimanual tasks. All of these measures have been found to be affected in Freezers [36]. However, the extent of these deficits suggests that altered movement generation during repetitive movements is central to FOG.
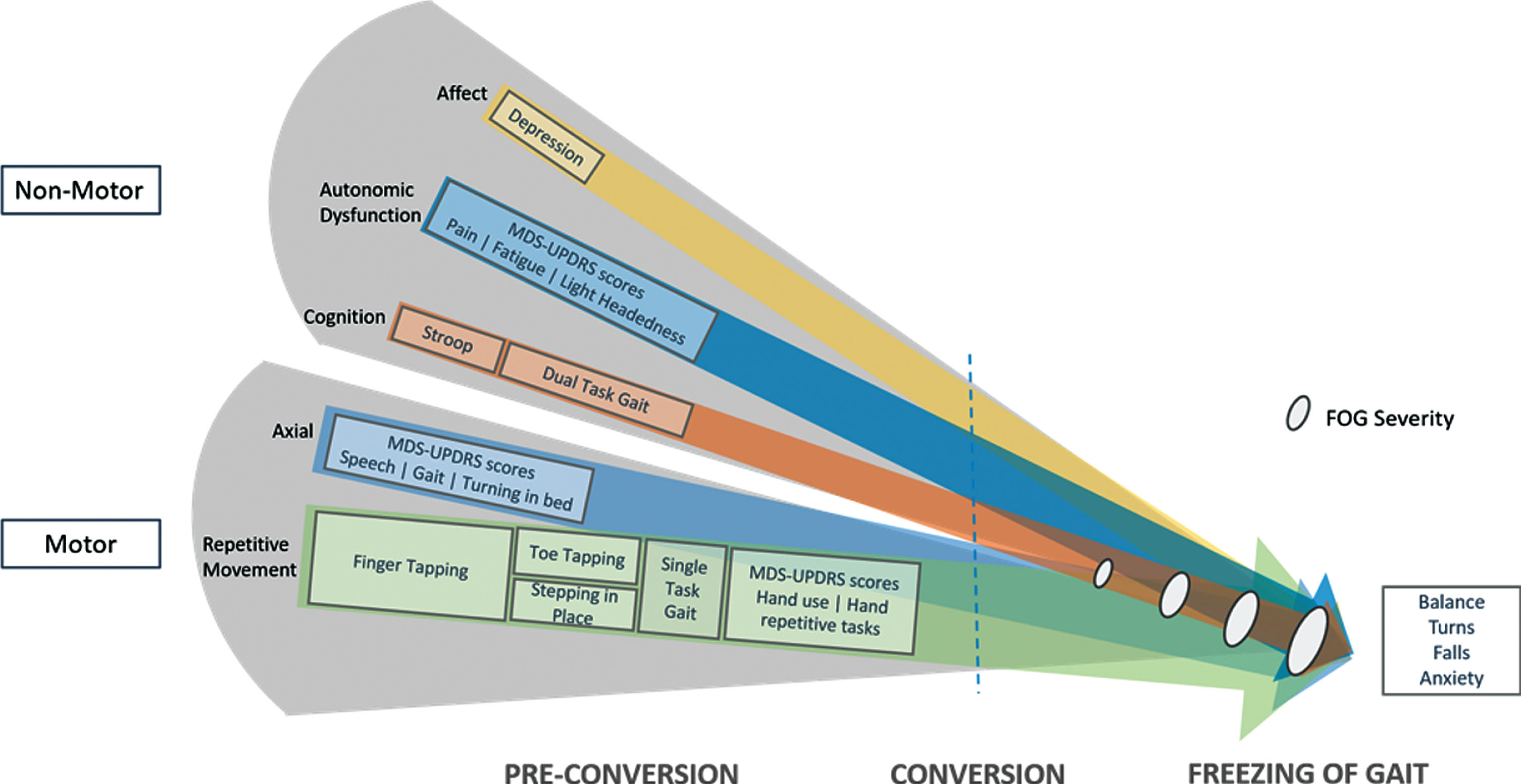
Conceptual Road to Conversion to FOG – Various aspects of behavior found to be more affected pre-conversion are represented by colored arrows. Components selected at least 10% in the multivariable model in this study are shown as rectangles sized approximately to selection frequency, overlaying the spheres of behavior captured by the component. Some components capture multiple aspects of behavior and are represented separately. The blue dashed line symbolizes a critical threshold reached in the interplay between already deteriorated motor control and progressive deterioration in affective, autonomic and cognitive function. This likely results in the onset of Freezing of Gait and may further progress to balance loss, turning difficulties, falls and anxiety, which were not found to be predictive in this study. FOG: Freezing of Gait.
Gait
Measuring gait also provided useful information about conversion to FOG, as both Dual Task and Single Task Gait components were selected in the prediction model. While Single Task Gait was more variable, addition of a cognitive secondary task led to more asymmetric and broad-based gait in the Converters. Furthermore, within a year of conversion, higher gait asymmetry was the strongest univariate predictor of conversion. Gait asymmetry has previously been shown to be highly attention-dependent when gait is less automatic [53] and might be related to impaired inter-hemispheric connectivity [54]. This increase in gait asymmetry and variability might thus reflect failing attentional control of less automatic gait, predisposing the patients to develop FOG.
Balance and turning
Balance measures on the MiniBEST may have suffered from a lack of sensitivity, with larger deficits only being picked up closer to conversion as previously shown in a subgroup of this cohort [55]. Posturography using inertial sensors might provide more sensitive measures of postural control. Similarly, we did not find any measures of turning that were predictive of conversion. Perhaps more sensitive measures of turning performance are required, taking into consideration trunk dissociation and variability in turning performance [56].
Conceptual model of conversion to FOG and implications
This is the first study to examine multiple motor and non-motor domains using objective, as well as clinical measures in relation to conversion to FOG. We summarize the important results of this study in a multidimensional model of conversion to FOG (Fig. 4). The results of this study unequivocally show that motor dyscontrol apparent in repetitive gait and non-gait tasks such as finger tapping, toe tapping and stepping in place, is central to, and underlying the development of FOG. Converters also showed greater axial disease burden, which corroborates the difficulty in generating internally driven motor programs in multiple effectors including speech. Further, decreased cognitive reserve evident in Stroop performance during dual tasking gait as well as autonomic symptoms like pain and fatigue, and affective symptoms like depression suggest that extra-nigral pathologies [57] are advancing. This likely results in reduced compensatory external control of movement, resulting in movement breakdown during the complex situations in which FOG occurs. This interplay between motor automaticity and cognitive control of movement is also supported by results of motor and cognitive interventions that have shown promising results on freezing [58, 59], suggesting that early delivery of similar interventions may delay the onset of FOG.
Limitations and recommendations
In this study, we took a broad approach to investigating predictors of conversion to FOG, in order to capture the complex multifaceted nature of FOG. Although this study was underpowered to detect individual predictors of FOG, these findings provide insight for future work with narrowed hypotheses. The incidence of FOG over the two year study period (11.5% per year) was close to that previously proposed (12.4% per year) [12]. This figure reflects a representative PD sample, as we made no attempt to enrich our cohort with patients who we thought were more likely to develop FOG. This also resulted in a rather small number of events for building a predictive model. However, towards improving external validity, we adopted a rigorous internal validation technique, using a bootstrapping method including all model building steps to minimize overfitting our data and overoptimistic predictions. As with most prospective studies, dropout further affected our analysis sample. We performed careful analysis of missing data and dropout, and used unbiased multiple imputation methods. For the multivariable prediction model, we did not have a pre-specified hypothesis and so multiple imputation was not possible. Single imputation thus provided conservative estimates.
Unlike the other cohort studies, we used the validated NFOG-Q with video for classifying patients as converters, which due to its reliance on self-report may have missed subtle freezing. Furthermore, the exact time of conversion was difficult to determine since follow-ups were one year apart. Future studies should consider using sensor-based measures of free-living gait to improve the sensitivity of FOG detection and quantification.
Conclusions
Through this prospective study, we investigated and compared a wide range of objective and clinical markers of conversion to FOG using a data-driven approach, albeit determined in a small cohort with a limited number of converters. A clinical profile with speech, hand use and cognitive and fatigue complaints was consistently predictive of conversion. Importantly, we found that repetitive motor dyscontrol during gait and non-gait movements were strong predictors of conversion, while non-motor symptoms including cognitive deficits and depression were surfacing. These findings, which need to be validated in an independent cohort, present specific markers for novel interventions to investigate whether the onset of FOG can be delayed or prevented in patients found to be at risk of conversion.
CONFLICT OF INTEREST
The authors declare no financial conflicts of interest.
Footnotes
ACKNOWLEDGMENTS
We would like to thank all subjects for their motivated and enthusiastic participation in this study. Support for this study was provided through a grant from the Special Research Fund of KU Leuven, Belgium (contract OT / 11/ 091), Research Foundation Flanders (FWO) [grant number G.0867.15]. W.V. is a Senior Clinical Investigator of the FWO. We also thank Mr. Jean Heymans for his generous contribution and support of this study.