
Abstract
Background:
Cognitive impairments are the most common non-motor symptoms in Parkinson’s disease (PD). These symptoms have a negative impact on patients’ quality of life and daily living activities. This review will focus on published articles that investigated the efficacy of cognitive rehabilitation in PD.
Objectives:
To review the existing literature on the efficacy of cognitive rehabilitation in PD and highlight the most effective form of intervention to prevent cognitive decline. This review will also point out any limitations and provide directions for future research.
Methods:
Published articles available in the Web of Science and PubMed databases up to November 2017 were reviewed for possible inclusion. We identified 15 articles that examined the effects of cognitive rehabilitation in PD and met inclusion criteria.
Results:
The main outcomes of this review indicated that, although previous studies used different cognitive rehabilitation methodologies, all studies reported cognitive improvements on at least one cognitive domain. Additionally, the most frequent cognitive domains showing improvements are executive functions and attention.
Conclusion:
This review reports the outcomes of studies that examined the effectiveness of cognitive rehabilitation in PD. It also points out the limitations of the studies indicating the limited availability of follow up data on the long-term effects of cognitive interventions. The review also highlights the fact that some of the studies did not include a PD group who did not undergo training. There remains, therefore, a need for longitudinal studies to investigate the potential long term benefits of cognitive training. In addition, future investigations should examine whether any disease characteristics such as disease stage, degree of cognitive impairment and/or the dominant side (right/left) or specific motor symptoms (rigidity/tremor) influence treatment efficacy.
INTRODUCTION
Cognitive impairments are the most common non-motor symptoms in Parkinson’s disease (PD) [1, 2]. These symptoms have a negative impact on patients’ quality of life and interfere with daily living activities [3]. It has been reported that the prevalence of mild cognitive impairment (MCI) among PD patients ranges from 17% to 53% [1]. Patients who have MCI could be at higher risk of developing dementia. The prevalence of dementia associated with the progression of PD ranges from 48% to 78% [4]. The most frequent cognitive domains affected in patients with PD are executive functions such as planning and shifting abilities, working memory [1, 6], episodic memory [6, 7], attention and visuo-spatial skills [1, 6]. There is a growing interest in research in the development of strategies to prevent more severe cognitive decline in those patients with PD who show mild cognitive impairment or in having ways to stabilise or improve cognitive dysfunctions when they occur.
Since there is no approved pharmacological treatment for cognitive decline in PD, the possibility of using non-pharmacological interventions for improving cognitive functions in this patient population was recently introduced [8]. These non-pharmacological interventions include cognitive training, physical exercise and the combination of both. So far, little is known about the efficacy of these varieties of interventions on cognitive deficits in PD, and several researchers have emphasised the need for effective techniques particularly for long-term efficacy [9].
To our knowledge there are only five review articles on this topic. One is a general review of non-pharmacological interventions in PD [10], and another included only four studies that have investigated the effect of cognitive training on a single cognitive domain (executive function) in this patient population [11]. The most recent reviews all had a specific focus. The Leung et al. [12] included only randomized controlled trials (RCT) studies, the Walton et al. [13] reviewed articles that focused only on interventions implemented late in the disease course and computer-based cognitive training techniques, while the van der Weijer et al. [14] reported on their theoretical perspective of cognitive training in PD more than performing a systematic review. In summary, most of the articles reporting the findings of studies of cognitive rehabilitation in PD have been published after the first two reviews were published [8, 15–19], while the most recent ones [12–14] had a more specific focus rather than including a thorough review of most available studies. None of the previous review articles focused on cognitive rehabilitation of PD in all disease stages, different cognitive training techniques as well as including randomized controlled trials and other methodological designs. There is, therefore, a need for an up to date systematic review of studies that have focused on cognitive rehabilitation in patients with PD and that overcomes all limitations mentioned above.
Although the testing of the efficacy of cognitive rehabilitation in patients with PD is still in the early stages, all of the previous studies have revealed a positive impact of cognitive interventions in PD patients [8, 15–27]. However, most published studies have used different methodologies including differences in patients’ characteristics and experimental design. There is a growing number of studies that has investigated the effect of various non-pharmacological interventions in PD. This review will focus exclusively on the effect of cognitive rehabilitation in this group of patients. Therefore, the aim of this systematic review was to search for all the existing literature that studied the efficacy of cognitive rehabilitation in patients with PD and to highlight which method seems to be the most effective on preventing cognitive decline. Furthermore, this review will attempt to determine which cognitive skills are more susceptible to the benefits of cognitive rehabilitation, will point out any limitations of existing approaches and will provide directions for future research.
METHODS
A systematic review of published research articles that have focused on cognitive rehabilitation interventions in patients with PD was carried out. An on-line literature search of the PubMed and Web of Science databases was carried out using the term Parkinson disease with each of the following: cognitive stimulation, cognitive rehabilitation, cognitive enhancement and cognitive training. We also used the term Parkinson disease in combination with each of the above terms and with each of the following: language, executive function, memory, attention, working memory, learning and problem solving. All published papers up to November 2017 were searched. The initial search identified 791 titles and abstracts. Then 478 duplicate publications were excluded. The abstracts and complete reports were reviewed to eliminate articles according to the following exclusion criteria: (1) review articles, (2) not cognitive intervention, (3) papers that included participants with other neurological condition, (4) studies of healthy participants, (5) reports published only in abstract format, (6) non-peer reviewed articles, (7) case reports, and (8) articles written not in the English language (see Fig. 1 and Table 1). A total of 15 articles met our inclusion criteria, those articles had to: have cognitive rehabilitation/training as their main focus, be studies of cognitive rehabilitation/training even if they were not RCT, be studies that included all PD stages and used different cognitive training techniques (not only computer-based). This methodological decision was taken to give a full picture of the kind of cognitive interventional studies currently available for this patient population. These articles were assessed for scientific suitability for inclusion in the present review, by using a set of 12 criteria adapted from Welton et al. [28] (these criteria are listed in Table 2). Each article was rated from 0 to 12.
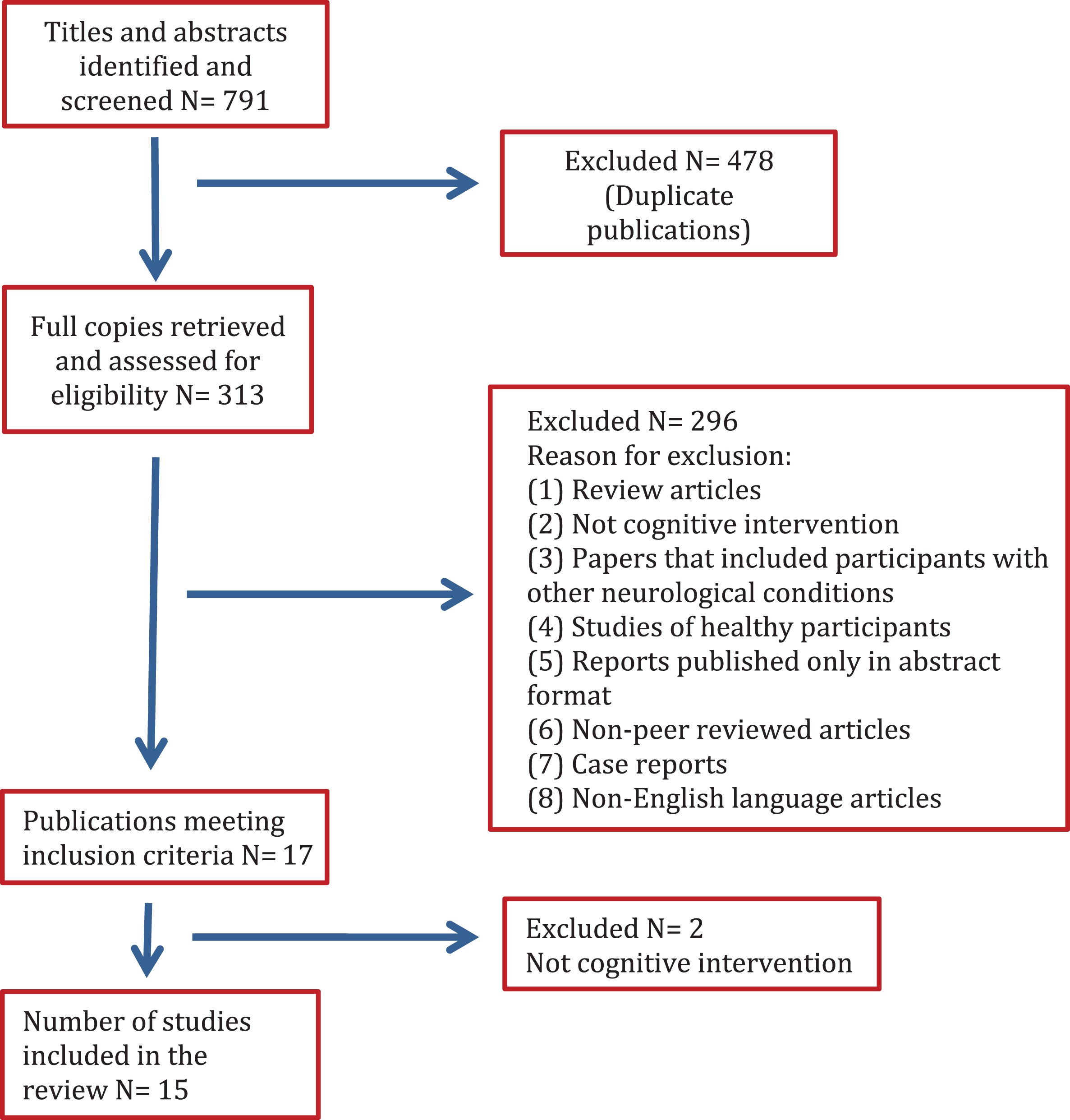
Flow chart of the study selection process.
Summary of reviewed articles
N: number of participants, FAS: phonological word fluency test, WCST: Wisconsin Card Sorting Test, MMSE: Mini Mental State Examination, SD: Standard Deviation, BADS: Battery of Behavioural Assessment of the Dysexecutive Syndrome, ZVT: Zahlenverbindungstest, GNL: face-name-learning test, AKT: Alters-Konzentrations Test, MWT: test of verbal intelligence, BNT: Boston Naming Test, TMT: Trail Making Test, COWAT: Controlled Oral Word Association Test, ROCFT: Rey Osterrieth Complex Figure Test, RBANS: Repeatable Battery for the Assessment of Neuropsychological Status, TOL: Tower of London, fMRI: functional Magnetic Resonance Imaging, CVLT: California Verbal Learning Test, SDMT: Symbol-Digit Modalities Test, D-KEFS: Delis-Kaplan Executive Function Scale, TUG: Timed-Up-and–Go test, TIADL: Timed Instrumental Activities of Daily Living Tasks, MCI: Mild Cognitive Impairment, PANDA: Parkinson neuropsychometric dementia assessment, ADAS-COG: Alzheimer Assessment Scale-Cognition, SCOPA-COG: Scales for outcome of Parkinson’s Disease-Cognition, PASAT: Paced Auditory Serial Addition Test, BADS: Behavioural Assessment of the Dysexecutive Syndrome, HADS: Hospital Anxiety and Depression Scale, PDQ-39: Parkinson’s Disease Quality of life, BDI: Beck Depression Inventory, UFOV: Useful Field of View Test, CES-D: The Centre for Epidemiological Studies Depression Scale, BADS: Behavioural Assessment of the Dysexecutive Syndrome, BRB-N: Brief Repeatable Battery of Neuropsychological Tests, TAP: Test Battery for Attention Performance, WMS-R: Wechsler Memory Scale- revised.
Quality assessment of the cognitive rehabilitation studies included
RESULTS
The process of literature search is illustrated in Fig. 1. In total, 791 studies were reviewed including duplicate publications from the two databases. After we excluded duplicate papers, 313 full copies were retrieved and evaluated for eligibility. Initially, we identified 17 articles that reported intervention/rehabilitation studies in PD. However, a closer inspection of the full papers identified two articles that did not match the main inclusion criterion as they reported the findings of non-cognitive interventions and were excluded on that basis. There were 15 studies included in this review and the time span of search was from 2004 to 2017. Cognitive tests, cognitive domains targeted, techniques/design, outcome measures, duration and frequency of training and results are summarized in Table 1. Table 2 includes a quality assessment of the reviewed articles.
An in depth review of the findings of the included studies is given below. We will first focus on intervention parameters and design, domains that were studied, and then will review the studies according to outcome measures looking, in turn, at cognitive, imaging and mood, fatigue and quality of life as outcome measures.
Intervention parameters and design
The length of all cognitive rehabilitation/training interventions ranged from 3 weeks to 6 months, with the number of sessions varying from 4 to 180. The frequency of these training sessions was from once a week to every day over a period of 6 months. Only two studies tested the long-term effects of cognitive intervention: one study had a follow up after 6 months, whereas the other had a follow up after one year. Furthermore, there was heterogeneity and variations of the intervention strategies between studies. Most of the studies used computerized based training programs, whereas other forms of treatment included different strategies such as the use of paper-and-pencil methods or multimodal cognitive rehabilitation. Moreover, in four studies cognitive training was compared to other active treatments (e.g., specific versus non-specific or structured versus unstructured). For instance, Zimmermann et al. [19] compared two different computerized cognitive rehabilitation programs, specific cognitive training (CogniPlus, 19 patients) versus non-specific computer sport games with motion-capturing controllers (Nintendo Wii, 20 patients). This study aimed at finding a possible positive effect in five cognitive domains (attention, working memory, executive functions, visuo-construction and episodic memory) as measured with neuropsychological testing before and after training. All patients received a 40-minute training session three times per week over four weeks, either with the specific or non-specific training programs. The CogniPlus rehabilitation program included four modules: FOCUS, that trained focused attention; NBACK, that trained working memory; PLAND, that trained planning and action skills, and HIBIT, that trained response inhibition (last two modules trained executive functions), whereas the Nintendo Wii training was a game console with movement-capturing controllers. This training included four sports games: Table Tennis, Swordplay, Archery, and Air Sports. The results showed that greater improvement in attention skills was triggered by the nonspecific training (Nintendo Wii) rather than by the specific training (CogniPlus). No positive effects were found on tests assessing other cognitive skills. Furthermore, another study by Petrelli et al. [18] examined the effect of different computerized cognitive group trainings: a structured training program (NEUROvitalis) with sessions targeting specific cognitive functions (attention, memory and executive functions) was contrasted with an unstructured training program (Mentally fit) similar to brain jogging. All treatment groups (22 patients in the structured training groups and 22 patients in the unstructured training group) had a 90-minute session twice a week over 6 weeks whereas a third PD group had no training at all (N = 21). The results revealed that compared to the no training control group, patients in the structured training groups improved in short-term memory and working memory. In addition, the “NEUROvitalis” group improved significantly in working memory compared to the “Mentally fit” group. Petrelli and colleagues [8] conducted a one-year follow up with these groups of patients. However, 18 patients from the original samples could not be re-assessed due to difficulties in contacting them. The one year follow up, therefore, was available only for 16 patients in the structured training group, for 17 patients in the unstructured training group and for 14 in the no training control group. The findings showed that, compared with the no training control group, both training groups maintained better overall cognitive functions as assessed by the DemTect. However, only the structured training group appeared to maintain their cognitive level when assessed with the MMSE. This study also concluded that cognitive training might prevent cognitive decline or onset of MCI in PD.
Cognitive domains targeted by rehabilitation
Most of the studies targeted one or more specific cognitive domains (N = 13), whilst two studies used a non-specific method of cognitive rehabilitation. The majority of the studies focused on improvements of executive function and attention. For instance, although studies that focused on executive functions used different duration and frequency of sessions, all results showed improvements in this specific cognitive domain. The evidence from these studies, therefore, suggests that all cognitive intervention programs targeting executive functions were effective in treating some component of executive abilities in PD. Furthermore, another cognitive domain that seemed to benefit from non-specific cognitive intervention was attention. Zimmermann et al. [19] demonstrated that a nonspecific training program (Nintendo Wii) improved attentions skills more than a specific one (CogniPlus). In addition, Petrelli et al. [18] found that a structured cognitive training program improved short-term memory and working memory skills in patients with PD.
Measures of cognition as outcome measures
All investigations focused on cognitive outcomes and reported improvements, although there was diversity in the cognitive domain/s targeted and the duration of each intervention. Only one study, that of Petrelli et al. [8], intended to follow up the training groups after one year of intervention and they found that the training groups maintained their overall cognitive functions better than the control group. Most of the studies were carried out with non-demented patients (N = 10), three studies included patients with MCI, whereas, two studies did not state the overall cognitive status of their samples. In terms of severity of disease, nine out of 15 studies included patients who were in the mild to moderate disease stages; two more studies included patients who were in the mild to severe disease stages, whereas the remaining four studies did not specify the disease severity stage of their samples. As for the type of intervention, there was a considerable diversity among studies and all appeared to focus on different cognitive domains. For instance, four studies focused their intervention on executive functions; one study focused on non-specific multiple skills, one study focused on cognitive processing speed, another study focused on shifting ability, while the other studies targeted different cognitive domains such as attention (in four studies), working memory (in four studies) and verbal fluency (in two studies). Other domains were mentioned at least once in different studies including: abstract reasoning, visuospatial, sustained, selective, alternating and divided attention, mental flexibility, episodic memory, mental speed, verbal and visual memory and short/long term memory.
Imaging parameters as outcome measures
Only one study has investigated the role of neuroimaging techniques in the assessment of the effects of cognitive rehabilitation in PD. Nombela and others [23] examined whether cognitive training improved cognitive dysfunction and they also assessed whether any cognitive changes were correlated with changes in any measure of brain function. One easy level of Sudoku was used (4-by-4 grid with 2-by-2 blocks). These authors measured cortical activation tested in response to a modified version of the Stroop test performed while participants were in a functional magnetic resonance imaging (fMRI) scanner. There were 10 patients with PD and 10 healthy controls; half of the PD patients had 6 months of cognitive daily training based on Sudoku exercises that mainly focused on working memory and attention skills. The results revealed that the training program improved cognitive performance in the Stroop task of the trained PD group during fMRI (in terms of reaction time, and of correct and missed answers). Furthermore, in the untrained PD group, there were reduced cortical activation patterns similar to the patterns of activation that were observed in the controls. Therefore, from this study it appears that neuroimaging techniques might provide evidence of the positive impact of cognitive rehabilitation in PD. Further investigations with larger samples are needed, however, to confirm this finding.
Mood, fatigue and Quality of Life assessments as outcome measures
There is evidence that the cognitive deficits experienced by patients with PD have a negative impact on their quality of life [3]. The majority of the cognitive rehabilitation studies also evaluated other important non-cognitive factors such as depression (N = 7), fatigue (N = 2), anxiety (N = 2), and quality of life (N = 3). However, some studies evaluated these aspects only at the baseline stage (depression N = 2, anxiety N = 2, fatigue N = 1). The outcomes of these studies were inconsistent. For instance, out of five studies, two found improvement in depressive symptoms after cognitive rehabilitation. In addition, out of three studies, two found improvement in quality of life. Due to the small number of studies that evaluated these factors, it is very difficult to draw any firm conclusion as to the impact of cognitive intervention on quality of life and on neuropsychiatric symptoms in PD. Furthermore, the difference among the results of different studies might be explained by the use of different methodological approaches. For example, Adamski et al. [20] concluded that depressive symptoms assessed by a general depression scale were improved in PD patient after cognitive intervention, whereas fatigue that was assessed by the Fatigue Scale for Motor and Cognitive Functions did not improve. Edwards and colleagues [17] used the Center for Epidemiological Studies Depression Scale to assess depression and found no improvement in the PD group following cognitive training. Furthermore, Paris and others [24] found no improvement in depressive symptoms in PD after cognitive rehabilitation. This latter study used the Geriatric Depression Scale to assess depression. From the review above, it appears that the various studies that assessed the effect of cognitive training on depression used different tools to measure depression that may explain the inconsistency in outcomes. In addition, based on prior investigations, it seems that type of cognitive intervention, duration and frequency of training have no influence on improving depression in PD. Further studies to examine the effect of cognitive rehabilitation on quality of life and other neuropsychiatric symptoms are needed.
CONCLUSIONS AND FUTURE DIRECTIONS
The previous review by Hindle et al. [10] was a more general review of the effect of a variety of forms of non-pharmacological interventions in PD. The search strategy for this previous review included terms that were not exclusive to cognitive interventions such as physical activity, exercise and motor. Although the review by Hindle and others [10] found that many studies reported positive outcomes for executive function in particular, the findings of our review indicate that several studies of cognitive training reported a positive impact on executive functions and attention. For the second review by Calleo and colleagues [11], their work focused on only one cognitive domain that was executive function. Unlike our review they did not include terms such as attention, language, memory, working memory, learning and problem solving in their search strategy, potentially missing effects on other cognitive domains. Overall, converging evidence of the benefit of cognitive rehabilitation on executive functions is reported both by the previously published reviews and our own. Our review, however, given the broader search including other cognitive domains, also highlights the benefits on attention, a finding that was missed both by the Hindle et al. and the Calleo et al. reviews. The newly published reviews showed different findings based on their research focus. For instance, Leung et al. [12] looked at only RCT studies (7 papers) and they found that cognitive training resulted in improvements on measures of working memory, processing speed and executive functions. Whereas Van de Weijer et al. [14] review was focused on the late stage of PD and they provided limited evidence of effectiveness of cognitive training. The results indicated improvements in non-demented patients in HY-stage 3-4, but not in HY-stage 5 and they did not state which cognitive domains were improved. Walton et al. [13] discussed the theoretical perspective of cognitive training in PD; they illustrated cognitive training as a potential therapeutic technique and the efficacy of cognitive training in general not only in PD. They also reported some results from the previous studies to provide evidence of the efficacy of cognitive training in PD without reaching any conclusion on which cognitive domains appeared to benefit more from cognitive training.
This review aimed to examine the effects of cognitive rehabilitation in PD, describe the present situation in this field and provide directions for future research. From this review it is evident that most of the articles were published in the last decade. Thus, this research area can be considered in its early stages of investigations. The main outcomes of this review indicate that, although previous studies used different cognitive rehabilitation methodologies, all studies revealed cognitive improvements on at least one cognitive domain. Additionally, the most frequent cognitive domains showing positive effects were executive functions and attention. Therefore, it seems that cognitive interventions have a positive impact in patients with PD irrespective of methods, duration and frequency of training.
Due to the use of various cognitive rehabilitation techniques, we cannot draw any firm conclusion on which method might trigger the largest improvement in cognition, mood, fatigue and quality of life. However, cognitive improvements were observed even in the studies that included a small sample size. This finding might be explained by the inclusion of patients in the early stages of the disease, as well as by the inclusion of non-demented patients.
This review has also pointed out the limitations of previous studies. The main shortcoming appears to be the absences of long term follow up data, the absence of a control group of patients with PD who did not undergo training. Some cognitive training programs included other elements such as psycho-education, physical exercise, medications or unspecific conversations that make it difficult to determine which specific elements had more influence on the training results. Thus, more studies are needed to have a clearer picture of which techniques are more effective to improve cognitive abilities in PD.
Only two studies included follow up of their samples after cognitive interventions to see the long-term effects on cognitive functions. Sinforiani et al. [27] found that after a 6 month follow up PD patients maintained their improved performance and no changes were observed on the neuropsychological tests scores. A second study by Petrelli et al. [8] reported that after a one year follow up the trained groups maintained their overall cognitive function levels. However, this study did not do an extensive cognitive assessment at the follow up stage (after one year) as they did immediately after cognitive training, but applied only some limited testing, a strategy that limits our knowledge about the long term effects of the training programs on specific cognitive domains. Therefore, longitudinal studies are needed to investigate the potential benefits of cognitive training long term. In addition, future investigations should also examine whether any disease characteristics such as disease stage, degree of cognitive impairment and/or the dominant side (right/left) or specific motor symptoms (rigidity/tremor) influence treatment efficacy.
Furthermore, only one neuroimaging study by Nombela et al. [23] examined whether the potential cognitive improvement might be correlated with neural alterations in PD. The results showed that training improved cognitive performance on the Stroop test during fMRI. Specifically, trained PD patients showed alterations in activation patterns that involved the left precentral gyrus, left medial frontal gyrus, right precuneus, and left inferior parietal gyrus when compared with the control group. Further imaging studies could provide a better understanding of these neural changes and more clear evidence of the efficacy of cognitive rehabilitation in PD.
While some studies concluded that neuropsychiatric symptoms such as depression were not responsible for the different treatment outcomes, other studies reported that depression had an effect on the cognitive rehabilitation findings. Also in this case more investigations with improved design and more comprehensive outcome measures are needed to provide clearer evidence of the role of depression and other neuropsychiatric symptoms on the effects of cognitive rehabilitations in PD.
Despite some reports finding an association between improvement of cognitive functions and quality of life, other investigations found no significant benefit of cognitive interventions on quality of life. Of course, cognitive training should result in improved daily live activities to have a significant impact on improvement of quality of life. Therefore, future research may investigate whether the improvement in cognitive skills can be transferred to improve daily life activities and consequently quality of life in this patient population.
Overall, cognitive rehabilitation in PD is still in its infancy stage. No firm conclusion can, therefore, be drawn at this stage. However, future research should take into account the shortcoming and unanswered questions highlighted in this review to design better trials. Future studies should also investigate whether PD patients may benefit more from a cognitive rehabilitation strategy that involves intervention on multiple cognitive domains or from one focused on only one cognitive skill.
CONFLICT OF INTEREST
The authors declare that they have no conflict of interest.
Footnotes
ACKNOWLEDGMENTS
King Fahad Medical City, Riyadh, Saudi Arabia for supporting this project. This is a summary of independent research carried out at the NIHR Sheffield Biomedical Research Centre (Translational Neuroscience). The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health.