
Abstract
Background:
Duchenne muscular dystrophy (DMD) is a severe neuromuscular disorder which leads to progressive muscle degeneration and weakness. Most patients die from cardiac or respiratory failure. Gene transfer therapy offers a promising approach to treating this disorder.
Objective:
Given the genetic disease burden, family size, and the high consanguinity rates in the Middle East, our objective is to address current practices and challenges of DMD patient care within two countries in this region, namely the United Arab Emirates and Kuwait, and to outline readiness for gene therapy.
Methods:
An expert panel meeting was held to discuss the DMD patient journey, disease awareness, current management of DMD, challenges faced and recommendations for improvement. Opportunities and challenges for gene therapy in both countries were also deliberated. A pre-meeting survey was conducted, and the results were used to guide the discussion during the meeting.
Results:
DMD awareness is poor resulting in a delay in referral and diagnosis of patients. Awareness and education initiatives, along with an interconnected referral system could improve early diagnosis. Genetic testing is available in both countries although coverage varies. Corticosteroid therapy is the standard of care however there is often a delay in treatment initiation. Patients with DMD should be diagnosed and managed by a multi-disciplinary team in centers of excellence for neuromuscular disorders. Key success factors to support the introduction of gene therapy include education and training, timely and accessible genetic testing and resolution of reimbursement and cost issues.
Conclusion:
There are many challenges facing the management of DMD patients in the United Arab Emirates and Kuwait and most likely other countries within the Middle East. Successful introduction of gene therapy to treat DMD will require careful planning, education, capacity building and prioritization of core initiatives.
Keywords
INTRODUCTION
Duchenne muscular dystrophy (DMD) (OMIM #300377) is a severe neuromuscular disorder (NMD) caused by pathogenic variants in the dystrophin gene which lead to progressive muscle degeneration and weakness [1]. The pooled global DMD prevalence is 7.1 cases (95% CI: 5.0–10.1) per 100 000 males and 2.8 cases (95% CI: 1.6–4.6) per 100 000 in the general population, while the pooled global DMD birth prevalence was 19.8 (95% CI:16.6–23.6) per 100 000 live male births [2].
Patients usually present between the ages of 2 and 4 years with early symptoms such as difficulty climbing stairs, a waddling gait and frequent falls [1]. The heart muscles can be affected as early as the age of 10 years [3] and most patients become wheelchair-bound during the second decade of life [4]. The diagnosis is suspected by a high Creatine Kinase (CK) level and confirmed by genetic testing. If a clinical diagnosis of DMD is not confirmed with genetic testing, then a muscle biopsy could be performed to test for the presence of dystrophin protein [5].
Despite therapeutic advances over the past 30 years, there is no effective cure for DMD [1, 6]. The focus has been on supportive care and management of complications where treatment with corticosteroids is the standard of care. However, even with optimal care, most patients with DMD die from cardiac or respiratory failure before or during their 30 s [7, 8].
Guidelines for the multidisciplinary care for DMD have been established which address obtaining a genetic diagnosis and managing the various aspects of the disease [5]. In addition, several therapies that aim to restore the lack of dystrophin protein or address secondary pathology, have received regulatory approval and many others are in clinical development [1]. However, many of these therapies, which are selective to specific gene mutations, remain suboptimal [6]. One promising approach for treating this life-threatening disease is gene replacement therapy that offers the opportunity to correct the underlying genetic defect by the introduction of a functional gene [9]. Another future treatment option is gene editing using CRISPR/CAS9 technology [10].
This paper reports the results of a survey and an Advisory Board meeting (held on 13 November 2021 and hereafter referred to as ‘meeting’) among DMD experts to explore the current practices and challenges in DMD patient care in the United Arab Emirates (UAE) and Kuwait and how to prepare for future gene therapy. Information on the prevalence of DMD in the Middle East is relatively outdated [11] however given the large family size and high consanguinity rates within the Middle East, it is expected that this region has outsized contribution to Mendelian genetic disorders, including DMD [12, 13]. It is difficult to estimate DMD incidence and prevalence for several reasons including sporadic genetic testing send out to different countries. This highlights an important knowledge gap where initiatives (such as a patient registry and centralized local genetic testing) are needed to accurately determine DMD incidence and prevalence in the region. Establishment of a national registry could improve this data gap by gathering representative, real-world data which would enable assessment of both short- and long-term patient outcomes.
The UAE, with a population of 9’991’083 people and a crude birth rate of 10 births per 1000 people, has a comprehensive, government-funded health system and a rapidly developing private health sector [14, 15]. The health care system is well-equipped and well-staffed: there are around 70 hospitals and 150 clinics. Healthcare is provided free in government hospitals; both nationals and non-nationals need to pay or rely on insurance for healthcare in private hospitals. Private hospitals outnumber government hospitals and hence the healthcare is skewed towards a private healthcare setting.
METHODS
A mixed methods approach was adopted whereby quantitative and qualitative data were collected from a written pre-meeting survey (Supplementary Table 1) and the meeting. The qualitative data included descriptive information on the overall care of patients with DMD.
The pre-meeting survey was conducted to elicit information on the challenges faced and recommendations for improvements in the management of DMD and the opportunities for innovative treatments such as gene therapy, based on collective expert opinion and experience.
The pre-meeting survey results (Supplementary Table 1) were used as a discussion guide during the meeting. The meeting was convened virtually to discuss and debate issues relating to the DMD patient demographic and the pathway from referral to diagnosis, in the UAE and Kuwait. The questions addressed different topics listed in Table 1.
Topics discussed in the meeting
Kuwait, with a population of 4’328’553 people and a crude birth rate of 13 births per 1000 people, also has a government-funded health system that is free for all nationals [16, 17]. Non-nationals who are resident in Kuwait are entitled to a health insurance card (for which they pay an annual fee) to access the public system. Private healthcare providers also run medical facilities in the country, available to members of their insurance schemes.
Hence, understanding the landscape of DMD patients’ journey in this region will provide opportunities for better care and management of these patients regionally and globally.
The specific objectives of the meeting were as follows:
To better understand the current DMD patient journey in the UAE and Kuwait To identify gaps and unmet needs of current DMD clinical practice / management To characterize the challenges and opportunities for DMD gene therapy
The participants are experts (mainly pediatric neurologists and geneticists) directly involved in the regular care of patients with DMD in the UAE and Kuwait and were selected as they are the physicians responsible for running genetic and neuromuscular services. Patients in primary and secondary care levels are referred to these physicians.
The meeting provided a real-life, clinical based platform to gather insights regarding current clinical practice, and to highlight unmet needs and challenges, based on the experience and expertise of the participants. This information is necessary to drive future clinical strategies in the management of DMD patients, with a particular emphasis on a smooth transition to DMD gene therapy.
OUTCOMES and DISCUSSION
The Current DMD Patient Journey in the UAE and Kuwait
Early signs and symptoms of DMD
In UAE, in most cases, a pediatric neurologist would typically assess a child based on a positive family history or elevated CK level, however there is no formal referral pathway. In Kuwait, any child born with a positive family history of DMD, is referred to a genetic center or to the pediatric neurologist. Children born to families with a positive history of DMD are usually diagnosed much sooner compared to a first case child in a family.
However, for patients who do not have a family history of DMD, signs and symptoms often go unrecognized. This is primarily due to poor awareness by families, primary and secondary care and the delay in referral to a paediatric neurologist.
Parents are often “falsely” reassured by family, friends, and sometimes even by primary healthcare practitioners (HCPs), that developmental delays observed in their child are within the normal spectrum. Mild delays can be ignored for quite some time as parents rarely mention this to the child’s HCP, especially if there are no other symptoms. Non-motor symptoms (e.g., speech or learning impairment) are rarely recognized as red flags for DMD. As such, patients who present initially with mild delays and non-motor symptoms are at risk of getting lost in the system.
Ultimately, many patients consult with a variety of HCPs (general pediatricians, development specialists; behavioral specialists, rheumatologists and orthopedic surgeons) and often undergo unnecessary work-up e.g., X-rays, liver investigations due to elevated transaminases, and prescribed treatment such as ADHD medication. Differential diagnoses (e.g., vitamin D deficiency, orthopedic (waddling gait / tiptoeing / slow to walk) or behavioral issues) often complicate and delay referral for DMD. Investigations such as serum CK are rarely performed which further delays the pathway to diagnosis. Experts estimate an average 1–2-year delay from onset of first symptoms to assessment by a pediatric neurologist.
DMD patient referral
There continues to be a time delay in DMD referral and diagnosis [18]. In the UAE and Kuwait, experts estimate that HCPs see on average between 2 and 5 new DMD patients per year (Fig. 1a). Children are generally referred (most commonly by pediatricians) to pediatric neurologists between the ages of 3 to 9 years (Fig. 1b and c). Muscle weakness and other motor symptoms are the most common motives for referral (Fig. 1d). Nationals account for 11.5% [19] and 30% [20] of the population in the UAE and Kuwait respectively— the majority of the population in both countries are non-nationals.
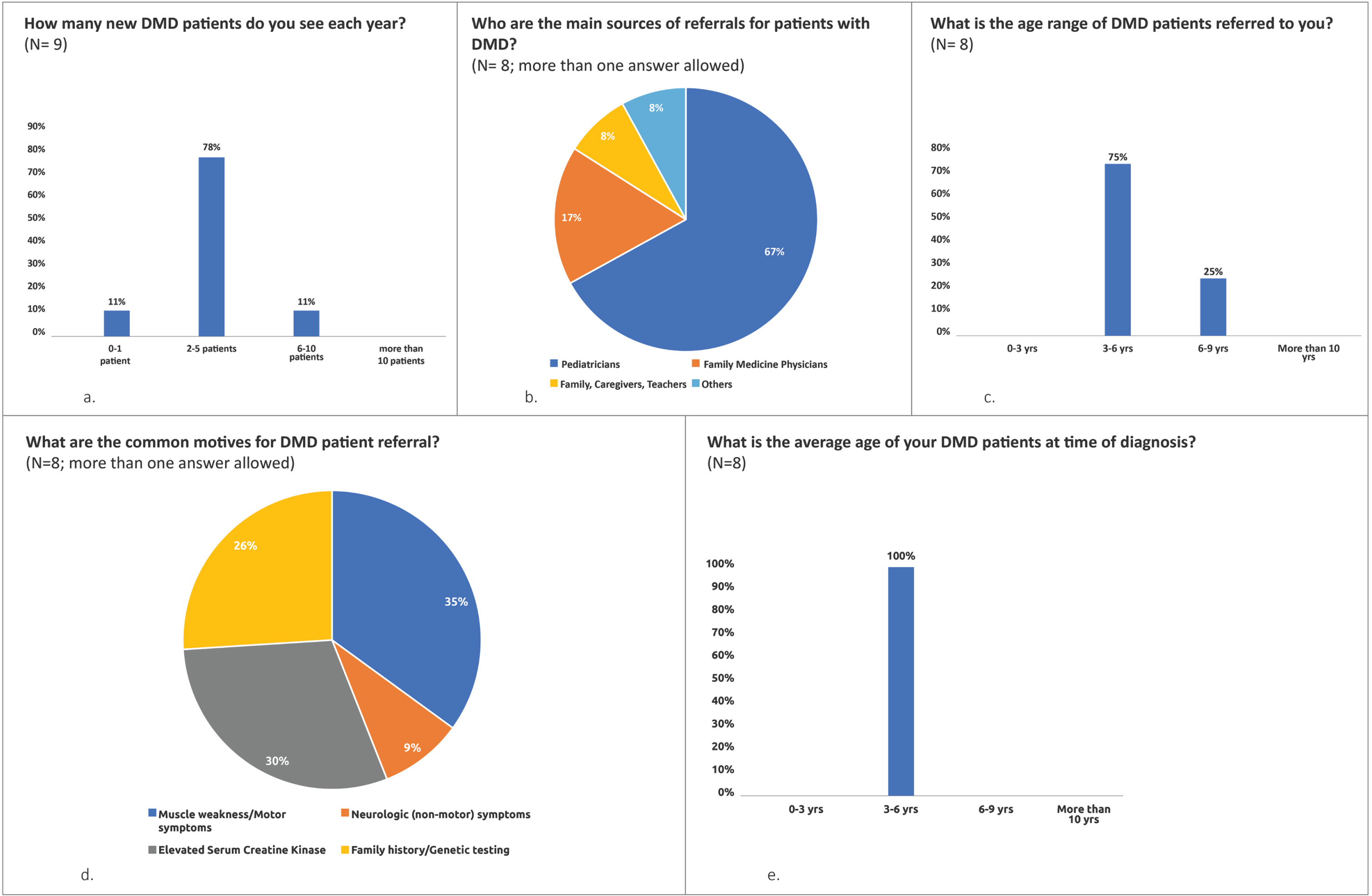
Key pre-meeting survey results. (a) to (e) indicate the percentage of respondents who selected the relevant answer to the question. N = number of respondents.
In the UAE, there is no fast-track system in place however patients are generally referred within 4-6 weeks to see a pediatric neurologist.
In Kuwait, suspicious cases are fast tracked where patients wait 2–3 weeks for an appointment with a pediatric neurologist. There are satellite clinics in hospitals to ease referral between neurology and genetics with a fast-track system for genetic testing. All genetic testing is done locally, facilitating faster results. There is no difference in the referral pathway for nationals versus non-national patients.
In the current therapeutic landscape, although referral delays do not pose a significant impact on patient management, when innovative treatments such as gene therapy become available and early initiation of treatment is vital, timeous referral might become more critical for optimal patient outcomes.
More recently, some trends have begun to reverse in the UAE, and specifically in Dubai with the announcement of the Dubai Academic Health Corporation (DAHC). All public hospitals have merged under one umbrella to facilitate patient transitions, especially between pediatric and adult care, alongside the centralization of patients’ electronic medical records. Furthermore, with the establishment of the CAP-accredited Al Jalila Genomics Center (www.genomics.ae), all genetic testing, including that for DMD, is being performed locally with a faster turnaround time and is often accompanied with appropriate genetic counseling. This new infrastructure will facilitate the early diagnosis and management of patients with DMD, especially given that (as mentioned above) most of these patients are UAE nationals and have free access to healthcare services within the DAHC.
DMD diagnosis
Currently, experts estimate that the average age of diagnosis of DMD in the UAE and Kuwait is between 3 –6 years, rarely earlier particularly when there is no family history (Fig. 1e).
Notably, the mean age at diagnosis has been reported to be 4.3 years in the UK with a delay in diagnosis averaging 2–3 years. As noted by these authors, earlier diagnosis is likely to result in better opportunities for optimized care [21].
Similarly in the UAE and Kuwait, importance is placed on early diagnosis. Early diagnosis of DMD patients not only enhances the efficacy of any treatment, mainly gene therapies but it can also cut costs by avoiding unnecessary diagnostic workup, multiple visits, and inappropriate treatment/management plans.
The most common and frequently followed screening test in DMD patients is CK testing. CK testing is simple and is recommended to be done routinely at primary, secondary or tertiary level, if DMD is suspected. The test is usually covered by insurance for those patients with access to private hospitals. If CK levels are high, the child should be referred for genetic testing. Muscle biopsy is only necessary if genetic testing is inconclusive. If muscle biopsy is performed, the sample may be sent abroad for detailed analysis as pediatric neuromuscular histopathologists are not readily available.
Genetic testing in DMD patients
In the UAE, genetic testing is conducted free of charge for nationals only however the pathway for reimbursement is changing. While this testing can be performed locally in Dubai, it is generally sent out by most other hospitals outside this Emirate (Fig. 2a). Non-nationals will either self-pay or insurance will cover the cost. In Abu Dhabi, genetic testing is either covered by insurance or patients self-pay. However, in Kuwait, it is conducted locally and is free of charge for both nationals and non-nationals. There are currently 139 DMD patients ( 93 Kuwaiti and 46 non-nationals) in Kuwait. Available genetic testing includes fragment analysis mainly by Multiplex-ligation dependent probe amplification (MLPA) for deletion and duplication analysis, and next generation sequencing (NGS) testing, in the form of targeted neuromuscular panels and whole exome sequencing, to capture both sequence and copy number variants (usually through sophisticated depth of coverage algorithms) [22–24]. MLPA is conducted first and if negative (with strong clinical suspicion of DMD), next-generation sequencing/whole exome sequencing is performed. It takes between 4–12 weeks for the results of the genetic testing to be received, depending on the test requested.
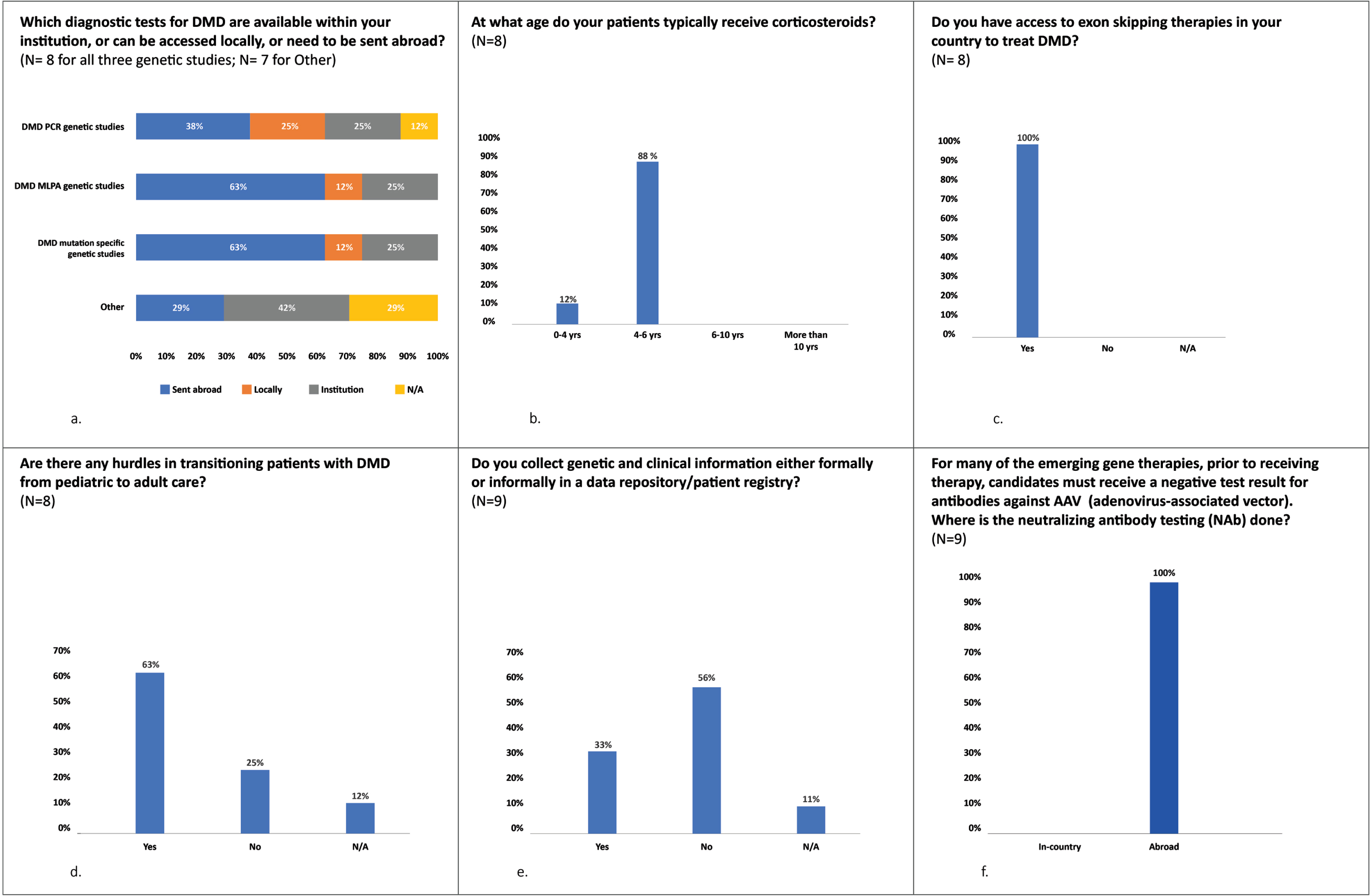
Key pre-meeting survey results continued (a) to (f) indicate the percentage of respondents who selected the relevant answer to the question. N = number of respondents.
Current Management of DMD in the UAE and Kuwait
Patients typically receive corticosteroids between the ages of 4 and 6 years (Fig. 2b). In the UAE, Deflazacort is ordinarily prescribed first, followed by prednisone (albeit many hospitals do not have Deflazacort). In Kuwait, only prednisone is available. The majority of DMD patients return for follow up / monitoring visits every 3 –6 months.
In the UAE and Kuwait, new medications for DMD are becoming available including exon skipping medications (Fig. 2c).
Although there have been some efforts to publish regional guidelines on managing DMD patients, which take into consideration peculiarities of every healthcare system, there is currently no need to develop new clinical guidelines. Nonetheless, when gene therapy becomes available, new guidelines might be needed to assist HCPs in navigating the available therapeutic options in the context of each patient’s profile.
Multidisciplinary care of DMD patients
DMD care is demanding and requires input from many HCPs. In the UAE and Kuwait, the primary HCPs that form part of the MDT include pediatric neurologists with neuromuscular expertise; physiotherapists/rehabilitation therapists; cardiologists; pulmonologists; dieticians and genetic counsellors. Spinal surgeons, orthopaedic surgeons and clinical psychologists are also part of the wider MDT.
In the UAE, DMD care can be fragmented. Services are not consistently provided in one single hospital and there is generally no structured communication between facilities. However, as mentioned above, with the transitioning into an interconnected academic healthcare system in Dubai, patients will have a more streamlined journey starting with fast diagnostics, neurology referral, and smooth transitioning between pediatric and adult care given the centralized electronic medical records within this system.
In Kuwait, MDTs are localized in each hospital but not consistent across hospitals. There are future plans to establish a new center, offering a centralized DMD MDT clinic which will lead to improved DMD patient management. A committee has been established in the Ministry of Health (MOH) for all new gene therapy treatments, which might facilitate multidisciplinary care for DMD patients.
Sustainability and continuity of multidisciplinary care is challenging with limited support in the community / local clinics, e.g., physiotherapy sessions are conducted at tertiary clinics. The availability of multidisciplinary care services is different depending on insurance approvals.
Ideally, the future management of DMD patients should be based on a hub-and-spoke model between centers of excellence for NMD with access to local genetic testing, and local centers with expertise in NMD offering care closer to home.
Transition to adult care
There are several hurdles in transitioning patients with DMD from pediatric to adult care, including a lack of services for adults, patients’ attachment to pediatric neurologists and a lack of transitional clinics. Patients are typically treated in children’s hospitals, which necessitates a referral to a general hospital. Based on our survey, the majority of experts experience difficulties in transitioning patients from pediatric to adult care (Fig. 2d).
In Dubai, the transition will be significantly mitigated with the new centralized healthcare system which will connect all public, pediatric and adult hospitals under one umbrella.
In Kuwait, experts advise that the average referral age of patients with DMD is 12 years. There is a smooth transition from pediatric to adult care with continuity of services provided by adult neurologists with experience in treating DMD in adults. Informal patient support groups are available, and parents also make collective efforts in their private capacity to support their children.
Screening, research and DMD patient registries
In the UAE, the national new-born screening program does not include testing for DMD. In Kuwait, the Kuwait Genetic Center offers screening for other NMD but not for DMD.
A major obstacle in understanding DMD disease attributes in the Middle East region, i.e., its prevalence, incidence, and the pathogenic variant spectrum, is the lack of methodologically sound and large-scale epidemiological studies [4]. There is a need for patient registries and data management. As expected, our survey shows that 56% of the DMD experts do not locally collect clinical and genetic data about their DMD patients (Fig. 2e). Most data are based on personal experiences of clinicians. Furthermore, the UAE has a fragmented healthcare system and genetic testing is sporadic: different hospitals send out genetic tests to different laboratories in Europe, US, India, etc. This highlights an important knowledge gap which needs to be addressed in the UAE. In Kuwait, however, there is a centralized system which allows for data collection.
It is estimated that the number of newly diagnosed cases of DMD is between 2-3 cases per 10000 births annually.
Key Challenges and Recommendations in the Management of DMD in the UAE and Kuwait
The key challenges and recommendations on how to improve DMD management are listed in Table 2.
Key challenges and recommendations in the management of DMD in the UAE and Kuwait
Opportunities and Challenges for Gene Therapy in DMD
Over the past 10 years, there has been a growing interest in innovative therapeutic approaches to treating DMD. In recent years, an increasing number of therapies have been studied which use different genetic techniques [4].
Gene therapy has the potential to provide long-lasting therapy with a single treatment [25]. Currently there are ongoing trials which differ in the type of AAV used, the parts of dystrophin selected for the micro-dystrophin versions, and the gene switch used to ensure proper expression of the micro-dystrophin in skeletal muscle and the heart [26, 27]. Compared with other therapies, AAV gene therapy shows the most promising success so far— it also has the potential of treating a large proportion of patients with DMD [6]. Other therapies such as exon skipping and stop codon readthrough may also be beneficial, although these therapies are selective to specific gene mutations and as such would only be applicable to a smaller proportion of DMD patients [6].
Key Success Factors for the Introduction of DMD Gene Therapy
Figure 3 illustrates the key success factors for introducing DMD gene therapy in the UAE and Kuwait. These factors were discussed in the meeting and are based on challenges and recommendations pertaining to expert experience and learnings in providing SMA gene therapy.
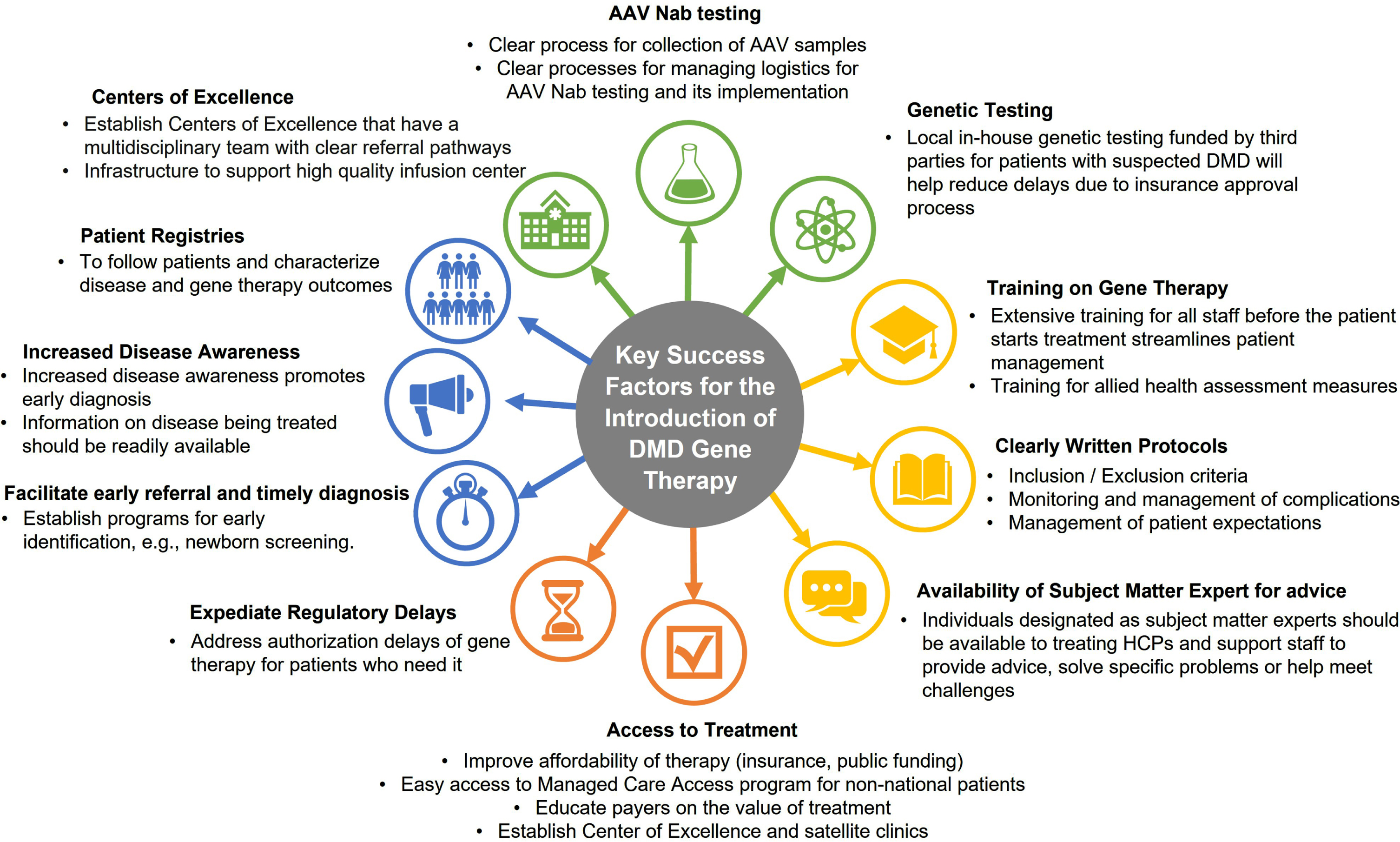
Key success factors for the introduction of DMD gene therapy.
NAb testing provides insight into the safety and efficacy of biologic therapies by assessing potential drug inhibition or neutralization through the production of anti-drug antibodies. As such, testing for NAb against AAV is an integral assessment that is conducted for eligibility prior to initial gene therapy.
In general, AAV NAb testing is a streamlined process. All blood samples for AAV NAb testing are sent abroad (USA or Europe) (Fig. 2f). It takes 1 –2 weeks for the results to be received by the neurologist (Supplementary Table 1). Gene therapy must be infused within 1 month of NAb testing otherwise the test needs to be repeated (this is the current experience with gene replacement therapy used to treat SMA). The requirements of health authorities regarding blood shipment abroad include (but are not limited to): The laboratory or manufacturer needs to take care of the logistics, including assuming full responsibility for the shipment of the samples and completion of all the health authority paperwork A declaration of a medical sample for testing is required Approval of laboratories via a central laboratory is required
Preparing for DMD gene therapy
Insights on the readiness for gene therapy
Education on DMD and gene therapy for medical faculty, nursing and support staff; staff training in preparation and safe administration and post-infusion follow-up of gene therapy; rationale for patient selection and patient risk stratification; information on DMD and gene therapy for patients / families; management approval of gene therapy; early accessible genetic testing and resolution of reimbursement and cost issues are considered the top priorities to improve readiness for the introduction of gene therapy for DMD in the UAE and Kuwait. Based on our survey, 88% (n = 7) of the experts already have experience with other gene therapies (Supplementary Table 1).
Facilities and resources for the preparation and safe administration of gene therapy, including logistical set-up for the supply and storage of gene therapies are also required.
Insights on educational needs: Who should learn what?
Each person involved in the management of a patient with DMD should be well informed about the disease and the management thereof. Table 3 illustrates the educational needs of clinicians, families and caregivers, and payers.
Educational needs of people involved in the care of patients with DMD
Clinicians should be well trained on trial and safety-like clinical data of gene therapies indicated for DMD. It is further important that families and clinicians alike have a clear understanding of the risk-benefit ratio and cost of treatment, as well as realistic expectations of gene therapy, i.e., that gene therapy is not a cure and that patients would still require MDT care to manage their condition.
In addition to the specific training needs, it is also important that other stakeholders such as rehabilitation teams, procurement departments, health insurers and Revenue Cycle Management (RCM) are educated on the clinical benefits and cost-effectiveness of gene therapy.
Practical considerations of gene therapy in DMD patients
Figure 4 illustrates the priorities and recommendations for DMD gene therapy.
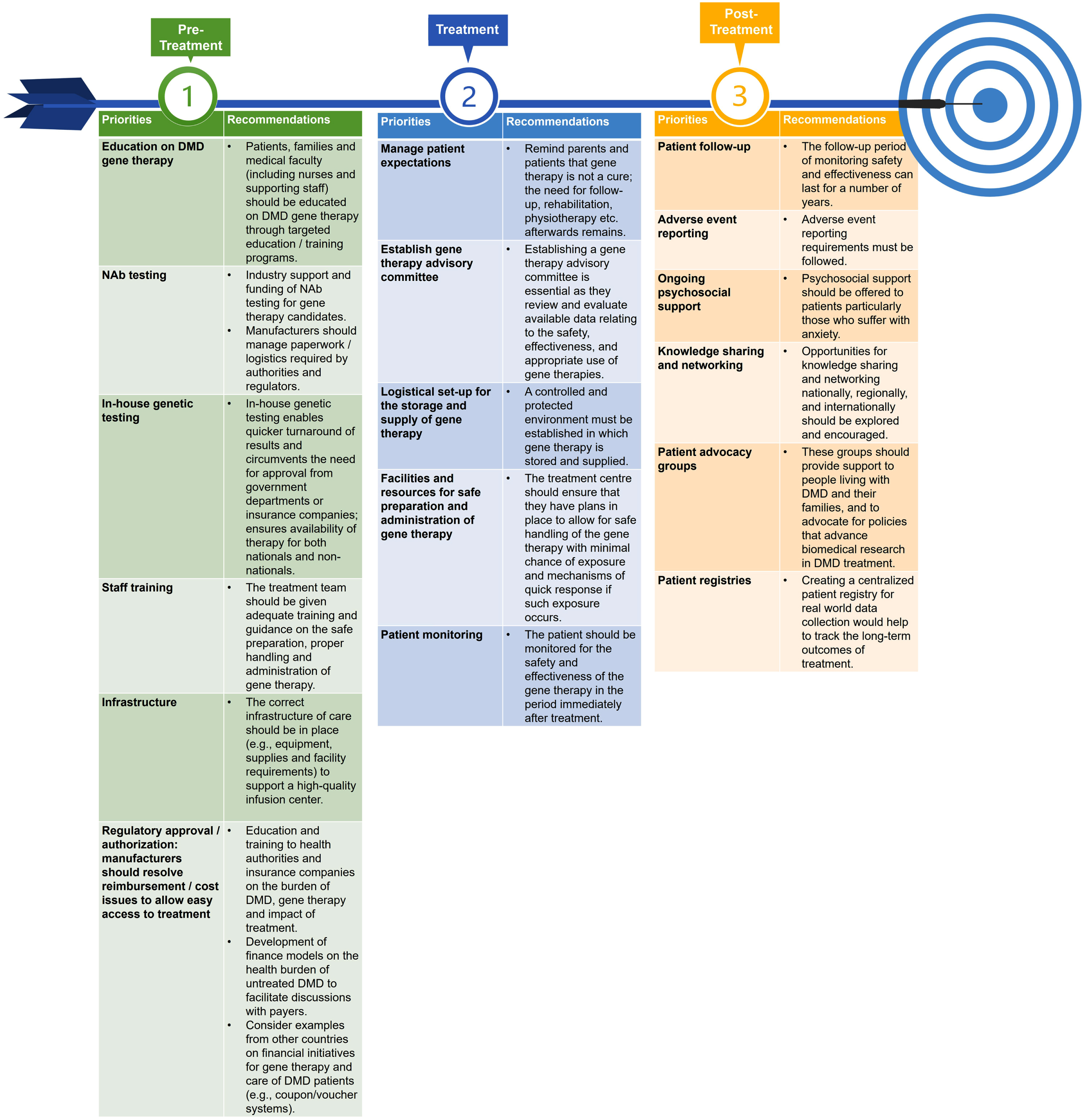
Priorities and recommendations for DMD gene therapy.
CONCLUSION
There are several challenges facing the management of DMD patients in the UAE and Kuwait and most likely other countries within the Middle East with less resourced healthcare systems. This paper offers insights based on expert opinion on how to improve on current practice. Furthermore, it highlights gene therapy as a promising approach to treating DMD in the future. Efforts to successfully implement AAV/ micro-dystrophin gene therapy in the UAE and Kuwait will require careful planning, education, capacity building and prioritization of core initiatives. These include setting up a patient registry, hospital collaborations, formulating a unified care approach and local guidelines, establishing training programs for paediatricians and primary healthcare physicians and assistance in genetic confirmation tests. Establishing a timeline for the action plan would be heavily dependent on the priorities, readiness and collaborative work between many different entities to set up a country plan. Such entities would include Ministries of Health, healthcare authorities, hospitals, physicians, societies etc. Complexities of healthcare systems, such as that in the UAE, which is mainly private driven, could pose an additional challenge in the implementation of gene therapy according to a defined timeline.
The recommendations provided are intended to assist HCPs, payers and regulators to better understand the current DMD management landscape in the UAE and Kuwait and to assess the potential opportunities and challenges for gene therapy. Given the expectedly high genetic disease burden in the Middle East, it is important to streamline DMD patient diagnosis, management, and treatment for better outcomes in this region, and for overall understanding of the natural history of the disease and efficacy of DMD gene therapy.
LIMITATIONS
There were a small number of respondents to the pre-meeting survey which could be considered a limitation however, these experts are directly involved in the regular care of patients with DMD in the UAE and Kuwait and were selected as they are the physicians responsible for running genetic / neuromuscular services. Patients in primary and secondary care levels are referred to these physicians. As such, although there were few respondents, the quality of their responses (based on their extensive experience) is high.
Summary points
•DMD is a severe, progressive genetic childhood disorder that results in functional decline, loss of ambulation and early death due to cardiac or respiratory failure.
•This paper reviews the current practices and challenges in the management of DMD in the UAE and Kuwait and how to prepare for gene therapy, based upon local expert opinions and recommendations.
•Awareness issues for referral are similar in the UAE and Kuwait, and for nationals compared to non-nationals.
•Education to increase awareness of DMD is the mainstay of achieving an earlier diagnosis. As such, there is a great need for awareness and educational campaigns for both HCPs and the public.
•The value and simplicity of CK testing should be emphasized.
•In the UAE: establishing early accessible in-country genetic testing for DMD diagnosis is crucial to collect phenotype and genotype data.
•Support is needed to establish MDT clinics that provide universal care (irrespective of insurance coverage) to all DMD patients.
•Training to unify DMD patient assessment is needed especially for physiatrists and physiotherapists
•Ideally, DMD management should be in a centre of excellence and involve a multidisciplinary approach.
•The top three collaborative activities considered to be of value include research, education, and awareness / advocacy.
•Financial models are needed for reimbursement and access discussions with health authorities and insurance companies to educate them on the health economic burden of untreated DMD patients and the direct and indirect cost savings derived from early treatment.
•Gene therapy offers a promising approach to treating DMD however careful planning, education, capacity building and prioritization of core initiatives are required.
Footnotes
ACKNOWLEDGMENTS
The DMD Advisory Board meeting was sponsored by Pfizer Gulf FZ LLC. The authors wish to thank Dr Helen Miller-Janson and Dr Ilanca Fraser from VI Research FZ LLC for medical writing support in the preparation of this manuscript, with funding from Pfizer Gulf FZ LLC. All authors contributed to the discussions and preparation of this manuscript and met the authorship criteria of the International Committee of Medical Journal Editors.
CONFLICTS OF INTEREST
HE, WF, VM, MI, AAAT, SC, LB, OI and AT received an honorarium for participating in the Advisory Board Meeting and other work outside of the submitted manuscript. Neither honoraria nor payments were made for authorship. IR is a full-time employee of Pfizer Gulf FZ LLC.