
Abstract
Background:
Vasculitic peripheral neuropathy (VPN) is caused by vessel inflammation leading to peripheral nerve injury of acute-to-subacute onset. When VPN occurs in the context of systemic disease it is classified as Systemic Vasculitic Neuropathy (SVN) and as Non-Systemic Vasculitic Neuropathy (NSVN) when restricted to the nerves.
Objective:
This study aimed to compare the clinical characteristics, biopsy findings and disease outcome in patients with VPN.
Methods:
Clinical records of adult patients with VPN diagnosed at our institution between June-2002 and June-2019 were retrospectively reviewed. Demographic characteristics, clinical manifestations, nerve conduction studies, nerve biopsies, treatment and clinical evolution were analyzed in all patients with at least 6 months follow-up.
Results:
Twenty-five patients with VPN were included (SVN, n = 10; NSVN, n = 15). No significant differences in demographic or clinical features were found between groups. The median delay between symptom onset and nerve biopsy was significantly longer in NSVN patients (10 vs 5.5 months, p = 0.009). Erythrocyte sedimentation rate (ESR) values over 20 mm/h were significantly more common in SVN patients (100% vs. 60%, p = 0.024). Nerve biopsies showed active lesions more frequently in treatment-naive patients compared to those who had received at least 2 weeks of corticosteroids (92% vs 38%; p = 0.03), with a higher proportion of definite VPN cases (92 vs 46%; p = 0.04).
Conclusions:
Although the clinical manifestations are similar, ESR is an important tool to help distinguish between both conditions. Early nerve biopsy in untreated patients increases diagnostic accuracy, avoiding misdiagnosis.
Keywords
INTRODUCTION
Vasculitic peripheral neuropathy (VPN) is caused by vessel inflammation leading to peripheral nerve injury and typically characterized by painful sensory and motor deficit of acute-to-subacute onset [1]. When VPN occurs in the context of systemic disease it is classified as Systemic Vasculitic Neuropathy (SVN), and as Non-Systemic Vasculitic Neuropathy (NSVN) when it is restricted to the peripheral nervous system [2].
To the best of our knowledge, no prior studies have been published on vasculitic neuropathy in a Latin American patient cohort providing a comparative analysis of these two etiologies, as well as limited experience regarding pathological changes in peripheral nerve biopsies after starting steroid treatment [3, 4].
MATERIALS AND METHODS
Aim and design
This study aimed to compare the clinical characteristics, biopsy findings and disease outcome in a local group of patients with VPN, in search of parameters that might help distinguish SVN from NSVN in the clinical setting. We conducted a systematic search for the terms: “vasculitic peripheral neuropathy” and “nerve biopsy” in the institutional electronic medical record database at a tertiary neurology referral center in Buenos Aires, Argentina, reviewing charts of patients treated between June 2002 and June 2019.
Study population
Patients over 18 years of age with VPN as final diagnosis were identified and divided into systemic and non-systemic etiologies, according to standard classification systems based on individual patient history, clinical findings, as well as on presence or absence of serological evidence of systemic disease [5–7].
Assessments
Prior to nerve biopsy, all patients were evaluated by two neurologists from our Neuromuscular Disorders Clinic. Muscle strength was assessed using the Medical Research Council (MRC) Scale for quantification (maximum sum score between zero (worst) and 30 (best) for upper and lower extremities) [8].
Routine blood chemistry tests were performed in all patients and included: erythrocyte sedimentation rate (ESR); anti-nuclear antibodies (ANA); anti-neutrophil cytoplasmatic antibody (ANCA); rheumatoid factor; HCV antibodies; HBV surface antigen; and HIV status. Results from nerve conduction studies (NCS) and electromyography (EMG) (both upper and lower limbs), performed at our Neurophysiology Laboratory by experienced neurophysiologists, were examined and resulting NCS patterns classified as: demyelinating, axonal, secondary axonal or normal according to pre-established criteria [9]. Neuropathy subtypes were identified as: multiple mononeuropathy, symmetric polyneuropathy or asymmetric polyneuropathy [3].
Nerve biopsies were obtained under local anesthesia at our center and specimens processed using routine stains [hematoxylin-eosin; luxol fast blue; Gömöri trichrome; anti-human smooth muscle actin primary antibodies; and anti-human CD45 (leukocyte common antigen) primary antibodies] on paraffin sections, as well as epoxy resin-embedded sections stained with methylene blue.
Histopathology findings needed to fulfill all criteria and were classified as definite, probable or possible vasculitis based on pre-established definitions of active and chronic vasculitic lesions [7]. Both in SVN and NSVN cases, specimens from patients who had received at least 2 weeks of corticosteroids (CS) were compared to those from untreated patients.
Treatments and follow up
Follow up assessment at six months included evaluation of: muscle strength (total MRC sum score), pain level, sensory impairment, walking distance and treatment side-effects, evaluating the therapeutic response as “improved, worsened or unchanged” in each of these parameters.
Data handling and analysis
Patients not meeting the criteria described above, or cases missing required data were excluded. Differences in demographics, clinical features, ancillary tests and treatment responses between both groups were compared using Student’s T Test, Fisher Test and Pearson’s chi-squared test, accordingly. Software Stata V. 12 was used to perform statistical analysis.
RESULTS
General characteristics
Twenty-five patients with VPN were included: 10 SVN (eosinophilic granulomatosis with polyangiitis = 4; rheumatoid arthritis = 3; granulomatosis with polyangiitis = 2; Sjögren syndrome = 1) and 15 NSVN. Average age at presentation was 63.1 years (range 34–81 years) and male-to-female ratio was 1:1, with no significant differences between groups.
Based on clinical findings, 23 patients were diagnosed with multiple mononeuropathy, 1 with asymmetric polyneuropathy, and 1 with symmetric polyneuropathy. No significant differences were observed in relation to weight loss, fever of unexplained cause, pain, walking impairment or autonomic dysfunction. Interestingly, median delay between symptom onset and nerve biopsy was significantly longer in NSVN patients (10 vs 5.5 months, p = 0.009).
No statistically significant differences were found when initial median MRC-Sum were compared between groups.
Ancillary tests
ESR median values were significantly higher in SVN (65 vs 35 mm/h, p = 0.024), with values over 20 mm/h significantly more common (100% vs. 60%, p = 0.024) (see Fig. 1). No patient with NSVN presented ESR values greater than 100 mm/h, although no significant differences were found with respect to SVN given the low number of patients (2 of 10 only had ERS values over 100 mm/h).
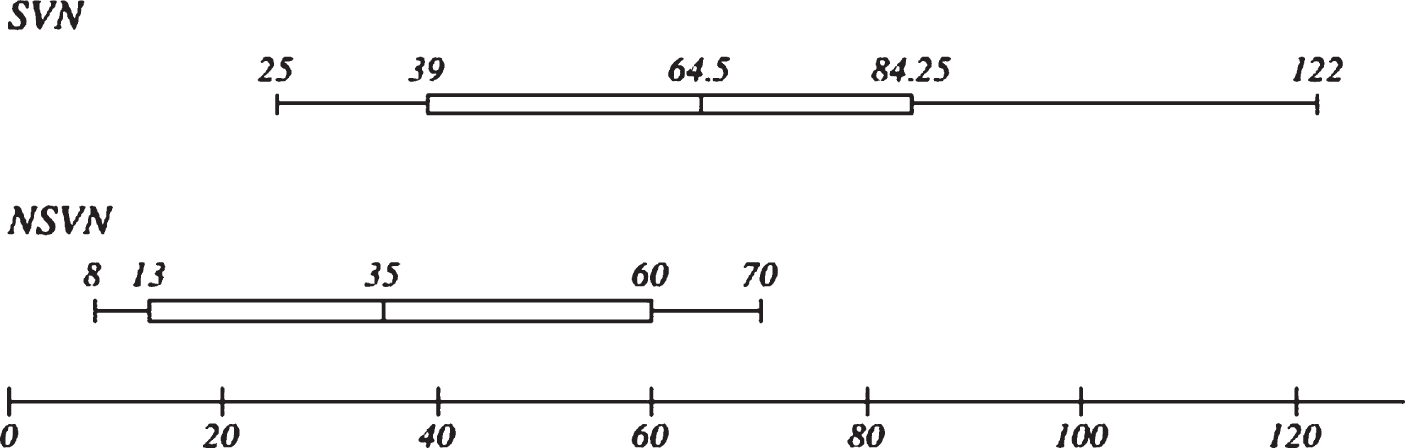
Erythrocyte Sedimentation Rate in SVN and NSVN patients. ESR measured in mm/hr.
Electrophysiological studies were abnormal in all patients, presenting similar levels of axonal neuropathy (n = 25), with no significant differences between groups. All clinical, laboratory, NCS and EMG results are detailed in Table 1.
Patients characteristics and ancillary tests
NS = not significant.
Histopathological analysis
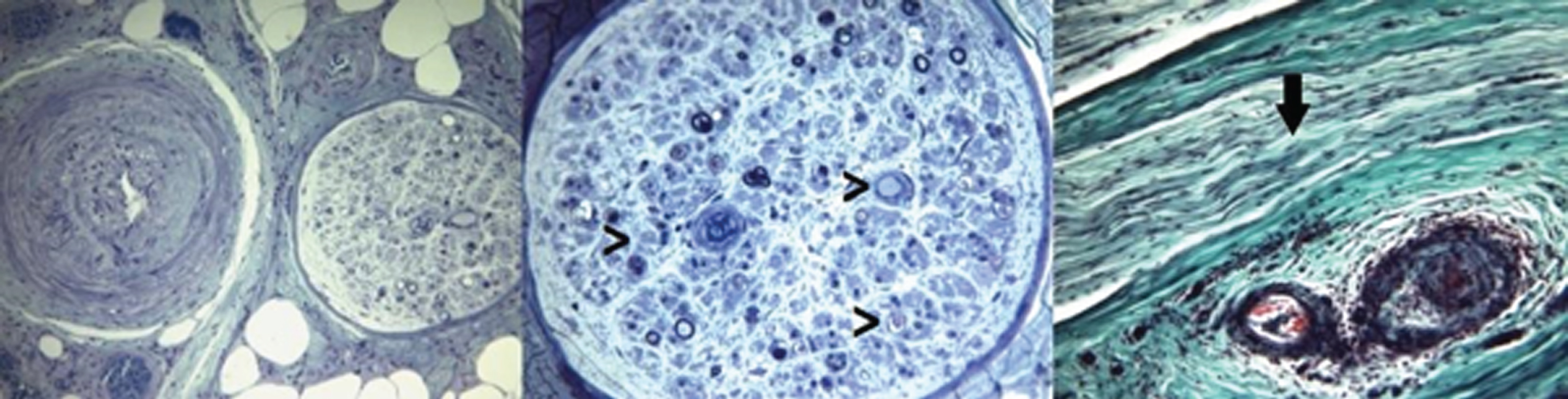
Nerve biopsy was performed in all patients (sural = 22, superficial peroneal = 2, tibial = 1). In 10, a muscle biopsy was also performed. Nerve samples revealed definite vasculitis in 17 (68%), probable vasculitis in 6 (24%) and possible vasculitis in 2 (8%) cases. No statistically significant differences were found in histopathology findings from SVN and NSVN patients, with a similar size of the vessels involved. Combined nerve and muscle biopsy did not increase diagnostic yield compared to nerve biopsy alone (see Figs. 2–7).
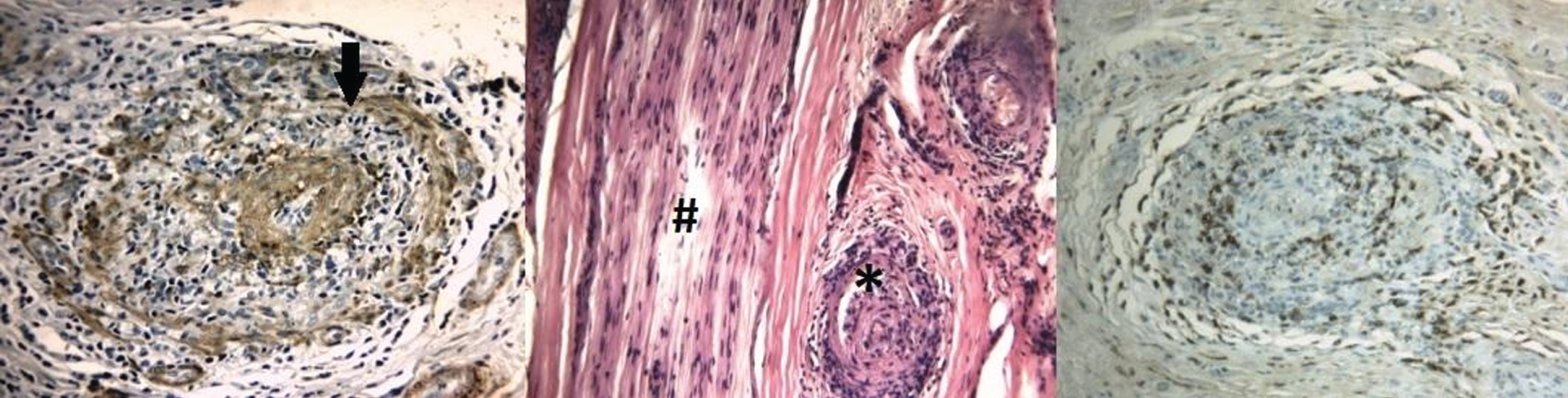
Sural nerve biopsy. Fig. 2: Anti-human smooth muscle actin antibodies show fragmentation of the vascular wall (arrow). Fig. 3: Hematoxylin-eosin illustrates nerve damage on the left (#) and vascular sub-occlusion on the right (*). Fig. 4: Anti-leukocyte common antigen (CD 45) presents inflammatory infiltrate in the arteriolar wall. Scale bars: 30μm (2 and 4), 100μm (3). Fig. 5 and 6: Epoxy resin-embedded sections stained with methylene blue show severe depletion of myelinated fibers (small arrows). Fig. 7: Gömöri’s trichrome, axonal degeneration is appreciated with formation of digestion chambers (arrow). Scale bars: 200μm (5), 100μm (6–7).
Diagnostic accuracy was greater in untreated patients, with a higher proportion of definite VPN cases (92 vs 46%; p = 0.04). Active lesions (defined by a high density of inflammatory cells in the vessel wall, loss of the endothelium, fragmentation of the internal lamina and signs of acute thrombosis) were significantly more frequent in the treatment-naive group (92% vs 38%; p = 0.03) (see Figs. 8 and 9). No other significant differences were observed (Table 3).
Sural nerve biopsy before and after treatment (Hematoxylin-eosin). Fig. 8 (Pre-treatment): Active lesions showing collection of inflammatory cells in the vessel wall, with loss of the endothelium, fragmentation of the internal lamina and signs of acute thrombosis. Fig. 9 (Post-treatment): Chronic lesions with signs of repair showing collection of few mononuclear inflammatory cells in vessel wall, intimal hyperplasia and thrombosis with recanalization. Scale bars: 30μm (8–9).
Treatment and follow up
All patients were treated initially with steroids, while 17 out of 25 (68%) required combined therapy (azathioprine = 8, cyclophosphamide = 7, intravenous immunoglobulin (IVIg) = 7, methotrexate = 4 and rituximab = 2). Treatment with steroids as monotherapy was more frequent in patients with NSVN (47% vs.10%; p = 0.01). There were no statistically significant differences between groups regarding type of immunosuppression prescribed, although treatment duration was longer in patients with SVN than NSVN (34 vs. 9 months, p = 0.008).
Minimum follow-up duration was 6 months (range: 6–195 months), and longer in SVN patients (40 vs. 24 months; p = 0.03). All patients presented therapeutic response showing improvement of at least 1 point in the MRC-Sum score or related to chronic pain, without significant differences between groups. Only 3 patients with SVN suffered relapses before the sixth month, with a sustained improvement at the last control. No other diseases were recorded during follow-up. (Table 2).
Treatment and follow up
NS = not significant.
Biopsy findings before and after treatment
NS = not significant.
DISCUSSION
Diagnosis of VPN can be challenging in daily neurological practice, often causing important diagnostic delays or leading to inappropriate treatments. In this study we describe results from a Latin American cohort of patients with VPN, comparing those presenting inflammation restricted to peripheral nerves, to those experiencing vasculitis secondary to a systemic condition.
No significant differences in demographic features or gender distribution were found between groups. Neuropathic pain and walking impairment were the most frequent symptoms, in line with observations from previous studies [10–14]. Neurological exam findings, baseline muscle strength and degree of disability did not contribute to differentiate SVN from NSVN [15–17].
Interestingly, SVN showed significantly higher ESR values, coinciding with an increased systemic inflammatory response. As reported by Collins et al. [7], erythrocyte sedimentation rates (ESR) of over 100 mm/h seem to exclude NSVN, making this an important tool to help distinguish between both conditions. Although our results showed a trend in this regard, differences between groups for ESR over 100 mm/h were not statistically significant in this cohort.
It is important to highlight that presence of active lesions on histopathology was significantly more common in untreated patients at time of nerve biopsy, a finding which supports indication of nerve biopsy in untreated patients. This, together with greater clinical awareness, hopefully will improve diagnostic accuracy of definite vasculitis, help avoid misdiagnosis and prompt earlier effective treatment. In contrast to Dyck et al. [2], who describe that NSVN tends to affect smaller epineurial arterioles than in SVN, we found no significant differences in the size of the vessels involved in our cohort. Surprisingly, combined nerve and muscle biopsies did not increase diagnostic yield in this study. This may have been due to small sample size and/or the muscles selected for biopsy. While in most other series, distal muscles such as the peroneus brevis or gastrocnemius were selected for biopsy [11, 18], we chose proximal muscles (vastus lateralis). Although it has been previously suggested that VPN preferentially affects distal muscles [17], this has never been studied specifically.
The wide treatment spectrum used in this series precludes precise analysis of patient response. However, severe phenotypes should probably be treated with more aggressive and sustained immunosuppressive treatment strategies [19], especially those patients with rapidly progressive presentation or refractory to CS monotherapy [7].
Our study has several limitations, including the fact that it is a retrospective analysis from a single tertiary center and therefore does not represent the population at large; that it lacked a standardized protocol; and that patients analyzed corresponded to a small sample studied in different time periods, therefore, valid standardized outcome measures were not used to assess motor response as well as for pain assessment.
In summary, neuropathies presenting as mononeuritis multiplex should make us suspect VPN, although this is not the only form of presentation. Elevated ESR and specific systemic antibodies associated with rheumatologic diseases, when present, should orient towards SVN etiology. Considering the effect of corticosteroids on active vasculitic lesions, peripheral nerve biopsy should be performed as early as possible to avoid misdiagnosis. Due to the aggressiveness of the pathology and high recurrence rate, an accurate diagnosis and sustained treatment are essential to prevent permanent disability and potential neurological sequelae.
VPN is an infrequent disease and multicenter studies will be necessary to put together a more comprehensive clinical picture and establish evidence-based treatment guidelines.
CONFLICTS OF INTEREST
The auhors have no conflict of interest to report.
Footnotes
ACKNOWLEDGMENTS
Teaching and Research Committee, Raúl Carrea Institute for Neurological Research (FLENI).
The authors received no financial support for the research, author-ship, and/or publication of this article.