
Abstract
Background:
Notwithstanding the amount of deliberate exercise, the daily patterns of active versus sedentary behavior have a major influence on health outcomes [1]. Patterns of habitual active and sedentary behavior in Myasthenia Gravis (MG) patients, as well as their possible relations to disease activity, are not known.
Objective:
To evaluate baseline patterns of physical and sedentary behavior in MG patients.
Methods:
Activity patterns of twenty-seven MG patients were assessed by a Dynaport MoveMonitor (McRoberts) accelerometer, worn for seven consecutive days. The amount of time spent in moderate and vigorous intensity activities, physical activity level (PAL), number of steps/day and sedentary time were assessed and correlations to disease severity were analyzed. The results were compared to general recommendations and published data of healthy individuals and to data of patients with the chronic disorders chronic obstructive pulmonary disease (COPD) and mitochondrial myopathy.
Results:
MG patients had sedentary behavior during 78±7% of the day. There was neither a correlation between disease severity and number of steps/day (R = –0.15; p = 0.56) nor between disease severity and PAL (R = 0.33; p = 0.26). Nevertheless, the MG patients met the recommendations of daily deliberate exercise (181±158 MET min/day). PAL was lower in MG patients (1.5±0.138) than in healthy individuals (1.67±0.145, p < 0.00001).
Conclusion:
Although a majority of MG patients meet the recommendations of deliberate exercise, their baseline physical activity levels are dominated by sedentary behavior. In comparison with a healthy population, MG patients are less physically active, but the reason for this remains unclear with no correlations between disease severity and physical activity patterns.
INTRODUCTION
The health benefits of physical exercise are well established. Furthermore, there is a growing body of evidence that not only deliberate exercise itself, but also patterns of active and sedentary time, are vital to improve health outcomes. A recent meta-analysis demonstrated that, after statistical adjustment for physical activity, sedentary time was independently associated with a greater risk for all-cause mortality, cardiovascular disease, cancer and type 2 diabetes in adults, although less prominent in those who participated in higher levels of physical activity [1, 2].
The autoimmune neuromuscular disorder Myasthenia Gravis (MG) causes skeletal muscle weakness that worsens with exercise. However, it is not known whether the reduced exercise tolerance associated with MG is associated with reduced daily physical activity and there is no existing knowledge regarding the patterns of habitual physical exercise and sedentary behavior of MG patients. Consequently, there is also no evidence on how the activity levels in MG patients compare to healthy populations or patients with other chronic disorders. As in many neuromuscular disorders, general fatigue and cardiovascular deconditioning are more prevalent in MG patients [3]. Nevertheless, most MG patients do not experience fixed muscular weakness. In case of physical inactivity, there could be a “vicious cycle” in which physical deconditioning discourages patients from exercising, which in turn worsens overall conditioning [4]. The traditional advice regarding physical exercise to MG patients has been to restrict, or even completely discourage exercise, mainly based on theoretical assumptions and lack of knowledge [3]. Recently though, a pilot study proposed that general recommendations regarding physical exercise could be applied safely to well-regulated MG patients [5].
In this study, we aimed to document the baseline habitual patterns of physical and sedentary activity, as well as energy consumption in Swedish MG patients. Furthermore, we wanted to correlate these parameters with the disease severity and to compare them to existing data on healthy individuals [6] with regards to the American College of Sports Medicine (ACSM) guidelines for exercise [7]. Additionally, we examined how patterns of physical activity compared with published data on two other chronic disease populations; chronic obstructive pulmonary disease (COPD) and mitochondrial myopathy [8, 9].
METHODS
Subjects and ethical considerations
One hundred-and-forty-three adult MG patients from the outpatient Neurology clinics in the regions of Jönköping County and Uppsala University Hospital in Sweden and with a confirmed diagnosis of MG according to the Myasthenia Gravis Foundation of America (MGFA) [10] were invited to participate in two separate training intervention studies, one in Jönköping County [5] and one in the region of Uppsala [11]. The physical activity habits of 27 patients (13 female, mean age 62±16 years) initially included in these studies were assessed by an accelerometer as described below. Current disease severity was evaluated by patient examination according to the MG Composite Scale (MGC), performed by a board-certified neurologist (EW).
All subjects gave written informed consent to participate in the study, which was approved by the Regional Ethical Review Board, Linkoping, Sweden (Dnr 2014/459–31) and Ethical Review Board, Uppsala, Sweden (Dnr 2016/144).
Measures of physical activity
Patterns of physical activity were measured using an accelerometer (DynaPort Move- Monitor, McRoberts, The Hague, The Netherlands) worn at the lower back for seven consecutive days. Four measures of different physical activity qualities were conducted: amount of moderate and vigorous intensity activity measured in metabolic equivalent of task minutes (METmin), physical activity level (PAL), number of steps/day and sedentary time. The measures were correlated to current disease severity as measured by the MGC score, which was obtained at one occasion for each patient during the week of activity measurement. We obtained total MGC score [ranging from 0 (no muscle fatigue) to 50 (worst possible muscle fatigue)] and also the subdomain of proximal leg weakness [ranging from 0 (no fatigue) to 5 (severe fatigue)].
The number of patients fulfilling general recommendations of the different measures was calculated. Further, the amounts of different intensity activities were assessed in totals of uninterrupted >10-minute-bouts of moderate and vigorous activity during the day separately and in combination, and expressed in METmin/day, which is a measure of energy expenditure during an activity, incorporating both its intensity and duration. This measure is defined as the ratio of metabolic rate during different physical tasks to rest, where 1 MET is an individual’s energy expenditure while sitting quietly, and is recommended by The American College of Sports Medicine (ACSM) [7]. Moderate intensity activity was defined as >3METs and vigorous intensity activity was defined as >6METs. The total time durations of moderate and vigorous intensity activity per day were noted. The amount of moderate and vigorous intensity activities was correlated to disease severity (MGC). The numbers of patients fulfilling ACSM recommendations for daily physical activity in METs, as well as in common time were calculated. Sedentary time was defined as minutes of awake activity with an energy expenditure≤1.5 METs, while in a sitting, reclining or lying position in accordance with existing definitions [1]. Patterns of time spent sedentary were evaluated and described in the MG cohort.
PAL, the total energy expenditure in kcal/kg divided by the basal metabolic rate (BMR) in kcal/kg [6], was calculated. PAL includes all activity types (i.e. not only moderate/vigorous intensity) and therefore, with a single number [ranging from <1.4 (extremely inactive) to >2.4 (extremely active)], describes a holistic perspective of the physical activity pattern [12] over a set period of time. A chair- or bed-bound lifestyle corresponds to an average PAL value of 1.2, while a lifestyle of strenuous work or highly active leisure corresponds to a PAL value of 2.0–2.4 [6].
The mean number of steps per day was assessed and correlated to MGC score. The number of patients achieving the general recommendations of 10 000 steps/day [13, 14] was assessed.
Comparison cohorts
Comparisons were done with published data on PALs in healthy adult individuals from a WHO cohort [6], divided into gender, age decades and weight. Comparisons were also done with published data on total METs/day and number of steps/day in a cohort of 177 COPD patients (11 women, mean age 71±8 years) [8] as well as in a cohort of 100 patients with mitochondrial myopathies (50±12 years) [9].
Statistical methods
D’Agostino & Pearson normality test indicated that most of the data were not normally distributed and therefore these non-parametric data were presented as median (95% confidence interval, CI). For parametric variables, mean±SD was given. For the power calculation, we set the confidence level to 90% and the power to 80%. Further, we assumed a difference between healthy control and patients in most activity measures of 35% and thus the calculated sample size needed was 23 patients. Spearman Rank correlation analysis was performed to correlate non-parametric measures and Pearson correlation was used for parametric data. Kruskal-Wallis test was applied for comparison of two or more independent samples (between MG patients and patients with other chronic diseases). The Wilcoxon signed rank test was used to compare non-parametric measures and two-way ANOVA was used for comparison of parametric measures for the MG patients with matched healthy controls from the WHO cohort. A p-value < 0.05 was considered significant. All statistical analyses were performed in GraphPad Prism version 6.07 for Windows (Graphpad software, La Jolla, CA, USA, www.graphpad.com).
RESULTS
Patient characteristics
Patient characteristics are summarized in Table 1. Of the 27 patients, 14 had early onset MG (EOMG) and 13 had late onset MG (LOMG). The mean BMI was 27±4.3; 10 patients (37%, 7 women) had a normal BMI (18.5–25 kg/m2), 10 patients (37%, 3 women) were overweight (BMI 25–29.9 kg/m2) and 7 patients (26%, 2 women) were obese (BMI ≥30 kg/m2).
Clinical data on participating MG patients. MGC, myasthenia gravis composite score (1–50); PAL, physical activity level
Moderate and vigorous intensity activity
The mean of total uninterrupted >10-minute-bouts of moderate and vigorous intensity activity during the day was 181±158 MET min/day. There was no significant correlation between MGC score and moderate and vigorous intensity activities (MET min/day) over the week (R = –0.39 p = 0.17). There was a wide distribution, where some of the patients with the highest MGC scores still managed to achieve >104 MET min/day. Twenty-one (78%, 13 women) MG patients achieved above the recommended minimum average of 64 MET min/day. When moderate and vigorous intensity activities were analyzed separately, three patients (11%) met the recommended daily goal of moderate intensity exercise≥30 min/day for at least 5 days a week (mean 2±1.8 days) and another three patients (11%) met the recommended daily goal of vigorous intensity exercise≥20 min/day for at least three days a week (mean 0.7±1.4 days). Comparison of total METs per day between MG patients, COPD patients and patients with mitochondrial myopathy revealed no significant difference, p = 0.93.
Physical activity level (PAL) and sedentary versus active time in MG patients
Mean PAL for the MG patients was 1.5±0.14, which is in the range of a sedentary behavior. The MG patients had on average 78±7% of sedentary (lying or sitting) time, 20±6% of standing/locomotion/shuffling activities and 2% of not wearing the device per 24 hours. The mean daily active time (time in activities >3 METs for at least 10 min, max interruption 1 min) was 35±29 min (Table 1). There was no correlation between disease severity (MGC) with neither PAL (Fig. 1a, p > 0.05) nor with sedentary or active time (Fig. 1b, p > 0.05 for all).
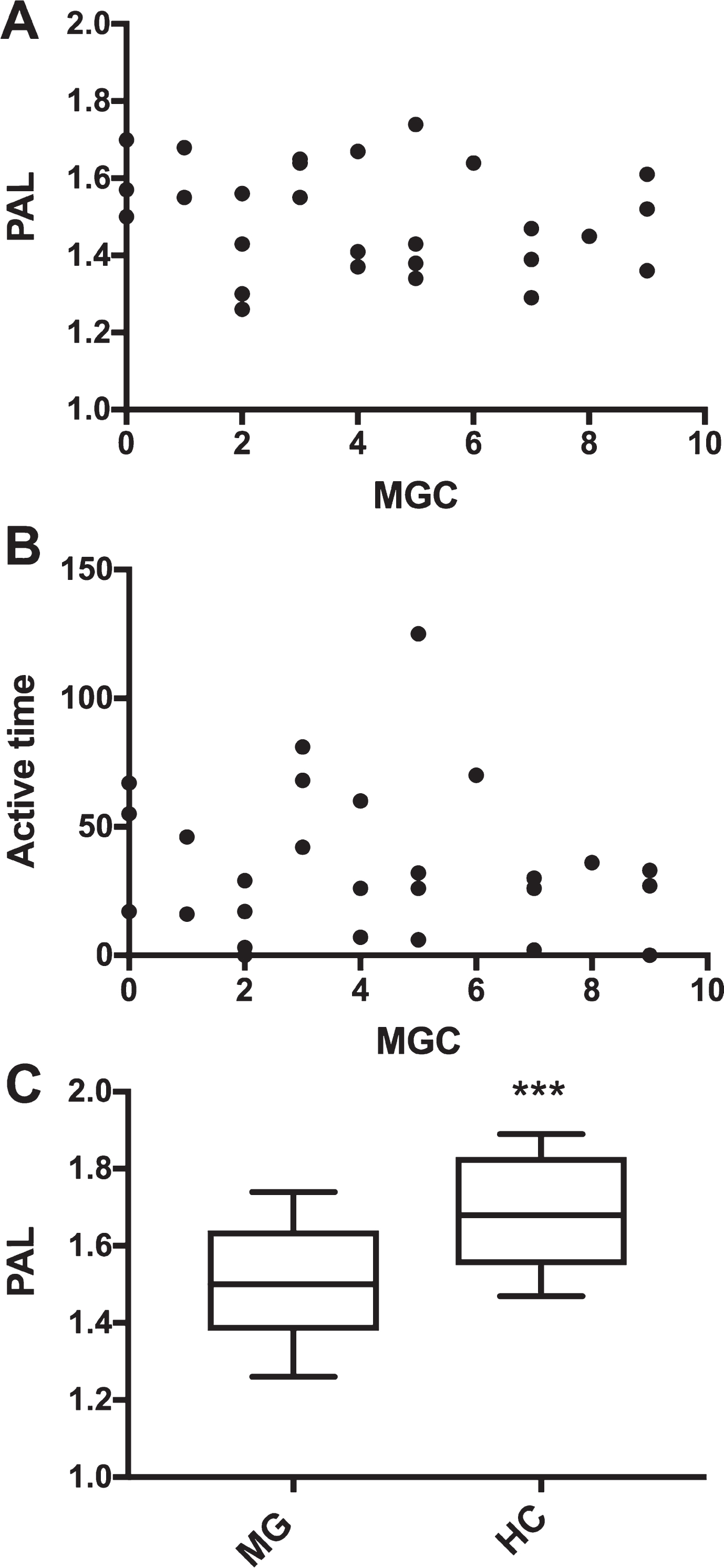
A and B) No correlation between MG composite score (MGC) and A) physical activity level (PAL) or B) active time (minutes/day) among MG patients (N = 27) using Spearman Rank correlation. C) Amount of PAL in the group of MG patients and healthy controls (HC). Whiskers indicate minimum and maximum PALs, the line in the box indicates mean. ***p < 0.0001.
Additionally, there was a significant difference in PALs between MG patients and the WHO data on age-corresponding healthy individuals (1.67±0.15, p = <0.0001, Fig. 1c).
There was a negative correlation between age and PAL (R = –0.48, p = 0.010; Fig. 2a). However, no significant correlations were found between age and disease severity (MGC; R = –0.09 p = 0.65) or disease severity (MGC; MGC legs) and PAL (R = –0.25 p 0.20; R = –0.0052, p = 0.98). There was also no correlation between BMI and PAL (R = –0.356 p = 0.0683).
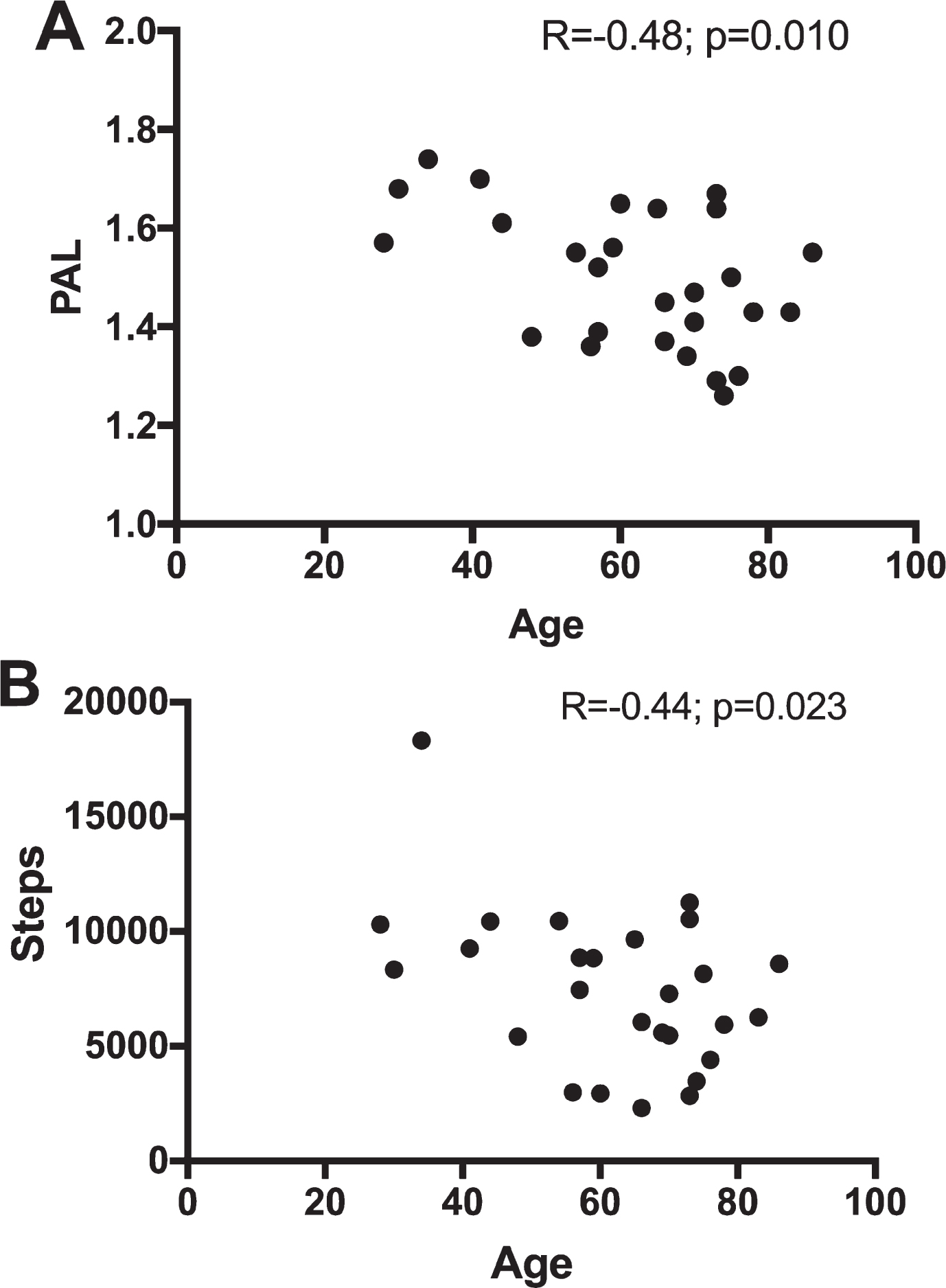
A and B) Significant correlation between A) age and physical activity level (PAL) and B) between age and number of steps. R, Pearson correlation coefficient.
Steps
There was a mean number of 7462±3471 steps/day in the MG cohort. Neither did number of steps correlate with MGC (R = –0.10; p = 0.63), nor with the leg subdomain of MGC (R = 0.083; p = 0.68). Again, there was a negative correlation between age and number of steps/day, (R = –0.44 p = 0.023; Fig. 2b). Merely six patients (22%, 6 women) achieved the internationally recommended level of 10 000 steps/day [12].
Mean number of steps per day was comparable between MG patients and patients with mitochondrial myopathies (6883±3944; p = 0.14) and comparison of steps per day between MG patients, COPD patients and patients with mitochondrial myopathy revealed no significant difference (p = 0.533).
DISCUSSION
To our knowledge, this is the first study to objectively describe patterns of physical activity and sedentary behavior in MG patients. It showed a tendency of an overall sedentary behavior among MG patients regarding physical activity level and number of steps/day as well as sedentary time. MG patients in average were spending 78% of their time in sedentary activities and reached a mean number of 7462 steps/day, with only 22% (all women) achieving a recommended level of 10 000 steps/day. Still 78% achieved the recommended minimum average of 64 MET min/day when all types of moderate and vigorous activities of at least 10 minutes duration were counted for. This is much in line with what has been described in the general population, with unfavorable high sedentary time in spite of high levels of deliberate exercise. In comparison to data on healthy individuals the MG patients were less physically active and were more often sedentary.
Sedentary time is an emerging measure shown to be of importance to overall health, as prolonged sedentary time has been independently associated with negative health outcomes regardless of physical activity [1, 2]. A sedentary lifestyle might have an even higher impact in subgroups of MG, due to disadvantageous patterns of other lifestyle-related risk factors [15]. There is no gold standard for prescribing reduced sedentary time, rather heterogeneity of methods for doing so [16]. Regarding recommendations on physical activity, varied approaches seem to be necessary to reduce sedentary behaviors in different societies and cultures [17]. This implies that tailored recommendations to reduce sedentary time in MG patients is needed.
Intriguingly, MG disease severity did not correlate with any of the different measures of physical activity. This suggest that the sedentary behavior in MG patients with mild-moderate disease activity has other implications than the disease related muscle fatigue itself. Instead, disease perception, expectations and attitudes in both patients and caregivers can play important roles on how MG patients develop substantially sedentary behaviors. In this study we chose MGC to represent the current level of MG disease severity, since it also considers fatigue issues in the everyday life. Nevertheless, as MGC represent a summary of different symptoms the impact of specific separate symptoms other than leg fatigue was not evaluated and cannot be ruled out.
The patterns of physical activity of MG patients did not differ significantly in comparison with the published data on patients with COPD and patients with mitochondrial myopathies. Since the compared cohorts differed in gender and age distributions the results are unreliable, but still could be argued to indicate possible mutual mechanisms to an increased sedentary behavior among patients with different chronic disorders.
Limitations include the relatively small number of MG patients, which in turn reflects the fact that it was difficult to recruit MG patients for the exercise studies [5, 11], as well as for activity measurements. Also, we used large sets of control data from healthy control subjects, since including age and gender matched healthy controls can also be an obstacle; considering the differences in amount of daily activity among different healthy individuals. Further, the measurements were carried out before the patients were to take part in a training intervention, which might have led to a participation bias, with mainly training motivated patients participating and thereby a less sedentary pattern than representative for all MG patients. Furthermore, the measurements were conducted in summertime in Sweden, which is a time when people are much more likely to be active, given the longer daylight hours and favorable weather. Therefore, it could be assumed that wintertime activity patterns would be even more sedentary.
There is an urgent need for well-documented recommendations for physical activity in MG patients. To establish such recommendations, it is crucial to understand the existing patterns of physical activity and sedentary behavior in MG patients. This study contributes important findings on such behavior in the everyday life of MG patients and implies a need to promote physical activity on all levels. As general exercise recommendations for healthy adults have proven safe to MG patients with mild-moderate disease, this should already be recommended strongly while waiting for more tailored recommendations where strategies to reduce sedentary time must not be forgotten.
CONCLUSION
Although a majority of MG patients meet the recommendations for weekly deliberate moderate and/or intense exercise, baseline physical activity levels of MG patients are dominated by a sedentary behavior. In comparison with a healthy population, MG patients are less physically active, but the reason for this remains unclear as there are no correlations between disease severity and different measures of physical activity patterns.
CONFLICT OF INTEREST
The authors have no conflict of interest to report.
Footnotes
ACKNOWLEDGMENTS
The study was funded by Futurum (FUTURUM-520281 and FUTURUM-520411), Palle Ferbs Memorial Foundation and Neuroforbundet (NEURO Sweden) to EW. Study funding was also provided by the Swedish Society of Medicine (SLS-499271) and the Swedish Research Council (VR-523-2014-2048) to ARP.