
Abstract
Background:
Fatigue is a common complaint in spinal muscular atrophy (SMA). Fatigability is well described in ambulatory SMA but the relationship to perceived fatigue has not been evaluated. Understanding this relationship has proven challenging for most disorders.
Objective:
To assess the relationship of perceived fatigue to fatigability, function, and quality of life in SMA.
Methods:
Thirty-two participants with SMA (21.9% type 2, 78.1% type 3) were recruited. Perceived fatigue and fatigability, function, and quality of life were assessed using standardized questionnaires and assessments. Associations were analyzed using Pearson correlation coefficients (p = 0.05). Also, the effects of age, type, and ambulatory status were determined on perceived fatigue.
Results:
All SMA participants reported fatigue. Perceived fatigue was not associated with function, quality of life, or fatigability in ambulatory SMA patients. Neither age, type, nor ambulatory status influenced perceived fatigue.
Conclusions:
Perceived fatigue can be quantified in SMA. Interestingly, perceived fatigue did not correlate with fatigability or function, suggesting that cognitive, homeostatic, or psychologic factors may be more relevant as co-morbid factors. Clinical trials targeting perceived fatigue in SMA should focus on these patient-reported assessments. A multilevel approach is required to separate the various mechanisms involved in perceived fatigue.
Keywords
ABBREVIAIONS
Spinal Muscular Atrophy
Six-Minute Walk Test
Institutional Review Board
Multidimensional Fatigue Scale
Fatigue Severity Scale
Hammersmith Functional Motor Scale Expanded
Upper Limb Module
Neuromuscular Module
Short-form 36
American Thoracic Society
SMA Functional Composite Score
Physical Health Component Score
Mental Health Component Score
Neuromuscular Junction
INTRODUCTION
Spinal muscular atrophy (SMA) is an autosomal recessive motor neuron disorder with a reported incidence of 1/11,000 live births [1]. Progressive, proximal muscle weakness result from degeneration of spinal cord and brainstem motor neurons. SMA has a broad phenotypic spectrum of severity with a clinical classification based on age of onset and maximal functional status achieved. Patients with the intermediate form, type 2, achieve the ability to sit but never walk. Patients with the mildest form, type 3, achieve the ability to walk independently but have varying degrees of disability [1]. Lower motor neuron involvement in neuromuscular diseases, similar to SMA, results in muscle weakness and can exhibit fatigue. Fatigue is a primary, disabling symptom and is prominent in more than 60% of patients with neuromuscular diseases [2–4]. It often results in low levels of physical activity and decreased social participation in combination with muscle weakness and enhanced fall risk [5].
Fatigue is a complex phenomenon including both psychological and physiological components. The two domains of fatigue include perceptions of fatigue (subjective) and performance fatigability (objective) [6]. Perceived fatigue and fatigability are not only different but potentially independent of each other [6]. Understanding this relationship has been a key objective for clinical research, but has proven challenging for most disorders [6]. Perceived or experienced fatigue is described as an overwhelming sense of tiredness, increasing sense of effort, lack of energy and motivation, and a feeling of exhaustion [7] encompassing a multifactorial approach. Perceived fatigue is different from fatigability which can be measured through objective changes in performance. Fatigability is also described as the magnitude or rate of change in performance criterion relative to a reference value over a given time of task performance or measure of mechanical output [6].
Perceived fatigue is a common, persistent symptom and a recognized clinical phenomenon in SMA [8, 9]. These clinical complaints may impair function and endurance. Perceived fatigue is reported to be greater in patients with SMA type 3 than in patients with more severe phenotypes, as assessed through questionnaires as a vast complaint/physical problem [9]. Previous studies demonstrated fatigability in ambulatory SMA type 3 patients using the six-minute walk test (6MWT), a functional measure, which was shown to be sensitive to fatigue-related changes [10]. Fatigability was also captured using repetitive nerve stimulation in SMA types 2 and 3 [11] and in ambulatory patients where the decrement was related to fatigability on the 6MWT [12]. On the other hand, only a few studies examined perceived fatigue in SMA. Werlauff et al. found perceived fatigue was rare in adult SMA type 2 patients with only 10% reporting abnormal fatigue concluding it did not seem to impact daily life [13]. In contrast, adults with SMA and spinal and bulbar muscular atrophy were found to report disabling perceived fatigue frequently (81%) compared to healthy controls [14].
The primary objective of this study is to assess the feasibility of measuring perceived fatigue in children and adults with SMA and their caregivers and to assess the relationship of perceived fatigue to fatigability, function, and quality of life in SMA. We will examine if perceived fatigue is related to age, severity and ambulatory status. We hypothesize that higher functioning SMA patients will experience greater perceived fatigue and the relationship to fatigability will be limited.
MATERIALS AND METHODS
Subjects
Thirty-two participants with SMA type 2 (21.9%) and type 3 (78.1%) (mean age, 20.5 years [SD 13.5]; range 5 to 49 years; 23 men/boys; 53.1% ambulatory) were recruited consecutively through their participation in a natural history study from the SMA Clinical Research Center at Columbia University Medical Center. All participants spoke English and gave informed consent or assent for the Columbia University Institutional Review Board (IRB)-approved study. This study is in accord with the Helsinki Declaration of 1975.
Procedures
Perceived fatigue, function, and quality of life were assessed using standardized questionnaires and assessments. Fatigability was assessed in ambulatory patients. Clinical assessments of perceived fatigue included the PedsQL™ Multidimensional Fatigue Scale (MFS) and the Fatigue Severity Scale (FSS). Fatigability was determined using the 6MWT. Functional measures included the Hammersmith Functional Motor Scale Expanded (HFMSE) and Upper Limb Module (ULM). Quality of life was assessed using the PedsQL™ Neuromuscular Module (NM) and the Short-form 36 (SF-36).
PedsQL™ MFS
The PedsQL™ MFS was designed to measure perceived fatigue in pediatric patients ages 2–18 and later expanded to include greater than age 18 years. The 18-item scale is comprised of 3 subscales: general fatigue (6 items), sleep/rest fatigue (6 items), and cognitive fatigue (6 items). It is a generic symptom-specific instrument that includes a child self-report and parent proxy-report [15, 16]. The instructions ask how much of a problem each item has been during the past 1 month. A five-point Likert response scale is utilized (0 = never a problem; 1 = almost never a problem; 2 = sometimes a problem; 3 = often a problem; 4 = almost always a problem). Items are reverse scored and linearly transformed to a 0–100 scale (0 = 100, 1 = 75, 2 = 50, 3 = 25, 4 = 0); so that higher scores indicated better health-related quality of life (lower fatigue symptoms). Scale scores are computed as the sum of the items divided by the number of items answered [15].
FSS
The FSS is a unidimensional scale which focuses on the physical aspects of fatigue. It is a self-reported questionnaire developed to measure the impact of disabling fatigue on daily functioning and can be applied to patients with neuromuscular diseases [17]. It covers several areas including physical, social, and cognitive effects. It is composed of 9-items with scores ranging from 1 = “strongly disagree” to 7 = “strongly agree”. A higher score represents greater fatigue. A global score is a mean score of individual item scores. A score of >4 indicates abnormal fatigue and a score of >5 indicates severe fatigue [18]. Perceived fatigue in patients with SMA type 2 and congenital myopathies have recently been shown to be captured using the FSS [13]. Test-rest for FSS in SMA was highly consistent [13].
6MWT
The 6MWT has been shown to be a valid and reliable test for the evaluation of fatigability, endurance, motor function, and exercise capacity in SMA [19]. Procedures for the 6MWT were adapted from the American Thoracic Society (ATS) guidelines [20] and were previously described by us for use in SMA [19, 21]. Participants walked up and down a straight corridor along a 25-meter linear walking course and were instructed to walk as far as possible without jogging or running, turn around the cone, and come back and repeat this loop as often as possible for 6 minutes. Distance walked over the entire 6-minute time period, distance covered each minute, and the time to complete each 25 meter interval was recorded. Fatigability was determined as the difference in the distance walked during the first and last minute expressed as a percent change, where a positive value represents fatigue [22].
HFMSE
The HFMSE is a disease-specific scale consisting of 33-items measuring gross motor function in SMA types 2 and 3. It has demonstrated good reliability and validity in patients with SMA, [23, 24] requires standard equipment, has minimal participant burden, and takes less than 15 minutes, on average to complete [23].
ULM
The ULM is a disease-specific scale consisting of 9-items measuring arm function to capture performance on activities of daily living in non-ambulant SMA types 2 and 3. It has demonstrated reliable performance in children as young as 30 months and takes on average less than 10 minutes to complete [25].
SMA Functional Composite (SMA-FC)
The SMA-FC score uses the unweighted averages of the 3 individual percentage scores of the 6MWT, HFMSE, and ULM. The combination of these measures broadens the spectrum of ability captured and may bridge potential gaps in assessment. The SMA-FC score may improve the ability to detect effects of treatment in trials that include participants with SMA types 2 and 3 [26].
PedsQL™ NM
The PedsQL™ NM module is a 25-item scale that encompasses 3 subscales: About My/My Child’s Neuromuscular Disease (17 items), Communication (3 items), and About Our Family Resources (5 items). The format, instructions, Likert response scale, and scoring method for the NM module are identical to the PedsQL™ MFS, with higher scores indicating a better health-related quality of life and it has been shown to be reliable in SMA [27, 28].
SF-36
The SF-36 is a generic health-related quality of life questionnaire composed of 36-items organized in 8 domains; 4 are summarized in the physical health component score (PCS) and 4 for the mental health component score (MCS). Item scores are coded, summed, and transformed into a scale ranging from 0 to 100 for each domain with higher scores indicating a better health-related quality of life. The SF-36 was used recently in SMA adults although validity and reliability has not been investigated formally [29].
Data analysis
Associations between perceived fatigue and other clinical outcomes were analyzed using Pearson correlation coefficients. Separate analyses were performed on the PedsQL™ MFS general fatigue subdomain only as it is supposed to be more related to patient functional status [16, 30]. The effect of age and SMA type on perceived fatigue were examined using one-way analysis of variance (ANOVA). An independent samples t-test was used to determine differences in perceived fatigue for ambulant and non-ambulant participants. An alpha level of p < 0.05 was considered statistically significant for all analyses.
RESULTS
Thirty-two participants with SMA type 2 (21.9%) and type 3 (78.1%) were recruited. Demographic and clinical characteristics are described in Table 1. Seventeen participants were ambulatory, 8 participants had scoliosis surgery and 3 required night time respiratory ventilation using Bilevel Positive Airway Pressure (BiPAP). One of the ambulatory participants did not perform any motor function testing during the clinical evaluation and only completed patient-reported outcome measures.
Demographic and clinical characteristics
SMA-FC, Spinal Muscular Atrophy Functional Composite; HMFSE, Hammersmith Functional Motor Scale Expanded; ULM, Upper Limb Module; 6MWT, Six-Minute Walk Test.
All SMA participants reported perceived fatigue. Perceived fatigue and quality of life scores for participants and caregivers are described in Table 2. The SMA participant report of perceived fatigue was similar to caregivers. Perceived fatigue was similar for SMA type 2 and 3 participants (PedsQL™ MFS: 70.2%, 73.4%). Perceived fatigue was common in adult participants with 78.6% reporting excessive symptomatic or abnormal fatigue (FSS > 4) and 50.0% reporting severe fatigue (FSS≥5). SMA participants reported similar health-related quality of life as did their caregivers.
Mean fatigue and quality of life scores for participants and caregivers
PedsQL™ MFS, PedsQL™ Multidimensional Fatigue Scale; PedsQL™ NM Module, PedsQL™ Neuromuscular Module; FSS, Fatigue Severity Scale; SF-36, Short-form 36.
Perceived fatigue was not associated with function or quality of life in any of the SMA participants, or with fatigability in the ambulatory participants (Table 3). The subdomains of perceived fatigue on the PedsQL™ MFS (general fatigue, sleep/rest fatigue, and cognitive fatigue) had no relationship to function, quality of life, or fatigability. There was no association between age, SMA type, or ambulatory status and perceived fatigue (Fig. 1). All correlations had alpha levels of p > 0.05.
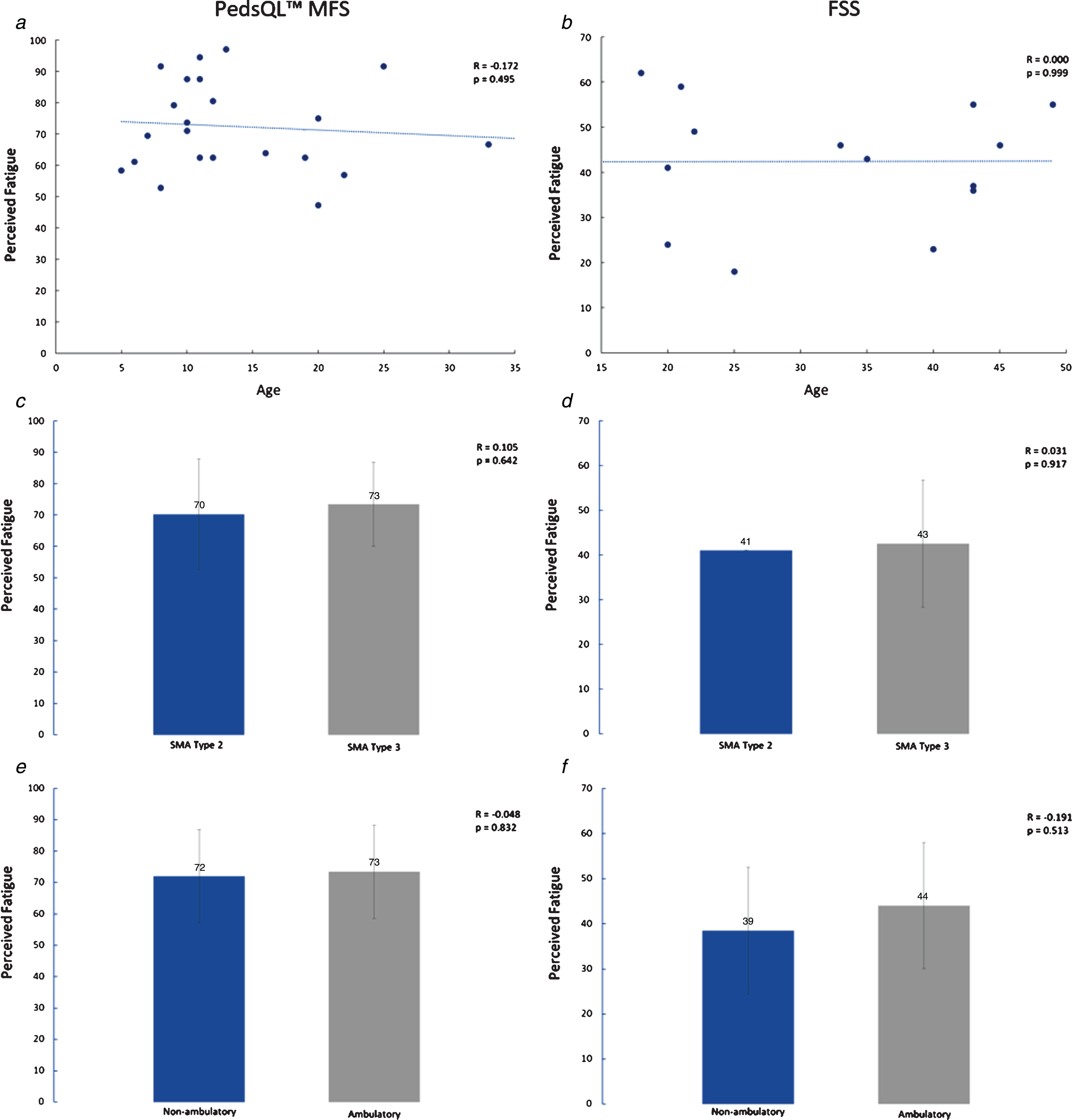
Associations of perceived fatigue to age, SMA type, and ambulatory status. a) PedsQL™ MFS and age, b) FSS and age, c) PedsQL™ MFS and SMA type, d) FSS and SMA type, e) PedsQL™ MFS and ambulatory status, f) FSS and ambulatory status.
Correlation coefficients of perceived fatigue, fatigability, function, and quality of life measures
PedsQL™ MFS, PedsQL™ Multidimensional Fatigue Scale; FSS, Fatigue Severity Scale; PedsQL™ NM Module, PedsQL™ Neuromuscular Module; SF-36, Short-form 36; PCS, Physical health Component Score; MCS, Mental health Component Score; 6MWT, Six-Minute Walk Test; HMFSE, Hammersmith Functional Motor Scale Expanded.
DISCUSSION
Perceived fatigue can be quantified using the PedsQL™ MFS and FSS in children and adults with SMA and their caregivers. More than half of SMA patients report having abnormal/severe fatigue with little difference between SMA subtypes. Interestingly, perceived fatigue was not related to function in SMA type 2 or 3 patients or fatigability in ambulatory patients, possibly suggesting that covariates such as cognitive, homeostatic, or psychologic factors were more relevant. Assessments of perceived fatigue may add value as an outcome measure for clinical trials that target symptomatic treatment of fatigue in SMA.
Relationships between perceived fatigue and fatigability have been difficult to demonstrate in other neurological disorders including multiple sclerosis, [31] idiopathic inflammatory myopathies, [32] fascioscapulohumeral dystrophy, [33–35] Guillain–Barre syndrome, [36] myotonic dystrophy, [34, 35] and hereditary motor and sensory neuropathy type I [34, 35]. Studies have suggested the missing link between perceived fatigue and fatigability may be due to the actual construct that multidimensional fatigue scales measure or suggest that numerous factors such as psychological parameters, sleep disturbance, pain, and motivation, may account for higher levels of perceived fatigue rather than disease activity and damage [4, 38]. Therefore, it is possible that in SMA, psychological factors may have greater significance in determining the degree of perceived fatigue than peripheral factors of fatigability, related to the motor unit, and captured by the 6MWT.
Similar to our findings, perceived fatigue was not correlated with fatigability in patients with myasthenia gravis using the 6MWT as a measure of fatigability [39]. Similar to myasthenia gravis, SMA patients exhibit evidence of a synaptopathy with related dysfunction in the neuromuscular junction (NMJ). The lack of association found in myasthenia gravis of perceived fatigue to fatigability supports the multidimensional fatigue model and may be similar to perceived fatigue in SMA.
Fatigability is consistently detected during performance of the 6MWT [10, 22] which, among neuromuscular disorders, is unique to SMA patients [21]. Transmission defects are common in patients with SMA and can be caused by NMJ dysfunction, which may be one possible explanation of this fatigability or sensory-motor circuit dysfunction [41]. Fatigability may also be related to mitochondrial dysfunction in the NMJ [42] or in the muscle tissue itself [43].
In this study, we were unable to find a relationship between function (6MWT performance) and perceived fatigue. In contrast, in Duchenne muscular dystrophy, perceived fatigue was associated with baseline function and 12 month changes with 6MWT distance in patients aged 5–13 years old [16]. This finding could be a reflection of the rapidly progressive disease course and progressive worsening in Duchenne muscular dystrophy, whereas SMA is a relatively stable disease and the perception of worsening is attenuated.
Perceived fatigue has been reported to be more evident in patients with SMA type 3 than in patients with more severe phenotypes [9]. Two studies examined differences between SMA types and found 64% of SMA type 3 described perceived fatigue in contrast with 34% in SMA type 1–2, [17] and only 10% of SMA type 2 patients had FSS > 4 [13]. It is believed that perceived fatigue is not prominent in SMA type 2 because patients with SMA are dependent on others for activities of daily living and require assistance [13]. As a result, they implement coping strategies from an early age [13]. In contrast, our study found that SMA type 2 and type 3 participants had similar amounts of perceived fatigue. While age did not associate with perceived fatigue in this cohort, its effect on type 2 and type 3 patients may be impacted based on age-related daily routines (i.e., an older, full-time employed type 3 patient may perceive more fatigue than a type 2 patient who is being homeschooled). The type 2 and 3 population in this study had a mean age of 12.3 and 22.7 years respectively. Moreover, SMA type 2 patients can experience pain secondary to spinal deformity, require hospitalizations due to illnesses, and suffer periods of deterioration in strength. Although not formally assessed in this study, increased pain, frequent hospitalizations, and strength deterioration may have contributed to our patients’ experience of higher fatigue scores given the typical disease characteristics of SMA type 2. Additionally, natural history reports patients between 5 and 15 years have the largest negative changes and the highest risk of losing function likely due to weight gain, increased contractures and scoliosis during the years leading to and throughout puberty [44]. These factors could contribute to perceptions of experienced fatigue as well.
In this study, the majority of SMA adults (78.6%) reported excessive perceived fatigue and half experienced severe fatigue. This is similar to previous reports of adults with neuromuscular diseases as the majority of patients with fascioscapulohumeral dystrophy (61%), hereditary motor and sensory neuropathy type 1 (67%), and myotonic dystrophy type 1 (74%) experienced severe perceived fatigue, which was associated with severe impairment in daily life activities [3].
To date, only one report has provided preliminary information on the validity of the FSS to assess the effect of salbutamol on perceived fatigue by patients with SMA. The FSS proved to be sensitive and reliable to quantitatively reveal patients’ experiences after starting salbutamol treatment; and all patients reported improvement in their condition, including reduced fatigue, and increased energy and strength [45].
Perceived fatigue can have many contributing factors that could go into the equation to distinguish it. Distinguishing perceived fatigue from related sensations can be done by including measures of mood and sleepiness as covariates [6]. A study examining perceived fatigue in mitochondrial disease suggested that anxiety, depression, and daytime sleepiness may be confounding factors of perceived fatigue, although, in the absence of clinically relevant anxiety or depression in this cohort, it is unlikely that the primary cause of fatigue is related to a mood disorder [46].
Patient-reported questionnaires vary greatly in how they measure perceived fatigue. They can include questions regarding momentary (state) perceptions, chronic characteristics (trait perceptions), the impact of fatigue on function, ratings of related constructs (e.g., tiredness), dimensions of fatigue (e.g., mental vs physical), and severity [6] highlighting why capturing perceived fatigue is complex and complicated. Studies examining perceived fatigue should account for these important covariates, such as depression, pain, weakness, and sleepiness [6].
We did not systematically explore other possible contributing aspects of perceived fatigue such as mood, depression, sleep disorder, pain, or a central nervous system evaluation. In this study, a retrospective review found two participants (6.3%) were receiving medication for a history of depression or anxiety. Additional potential contributors to perceived fatigue may include weight gain and hospitalizations which were not formally examined in this study. To further understand the impact of perceived fatigue on patients with SMA, an in depth neuropsychological evaluation will be necessary to evaluate mental fatigue (central factors). Future studies could assess causal factors that could help direct pharmacological and non-pharmacological symptomatic treatments. A greater understanding of what contributes to perceived fatigue would help to optimize rehabilitation programs.
Another limitation is that a unidimensional scale (FSS) was used to assess perceived fatigue for adults while a multidimensional scale (PedsQL™ MFS) was used for children, although no correlation was found with the general fatigue subdomain of the PedsQL™ MFS when looked at separately to mimic a unidimensional scale. In our population, only one adult participant with SMA type 2 was administered the FSS. Exclusion of the first 2 items should be taken into consideration to improve the properties and content validity of the FSS during administration to the SMA type 2 population to assess perceived fatigue in future studies [13].
Our study was limited by a relatively small convenience sample of 32 participants. No additional fatigability measurements were performed such as electrophysiological evaluations to measure decline in muscle force after exercise (peripheral fatigue) or to measure central activation failure (central fatigue). In addition, fatigability was only assessed in ambulatory participants. Future studies are needed to develop assessments to measure fatigability for non-ambulatory SMA patients. While fatigability tests are currently in development, [47] potential assessments may include nine-hole peg test [48] and 6-minute cycling test [49].
Perceived fatigue in SMA is a relevant problem that needs attention for clinical management and care. Treatment strategies should be focused on other potential cofactors contributing to fatigue. Currently, the optimal treatment strategies for fatigue in neuromuscular disease included symptomatic treatment of the underlying disease, pharmacotherapeutics directed at treating fatigue, rehabilitation or exercise, educational interventions (guidance and advice for daily activities with special attention for overuse), cognitive behavioral therapy, or a combination of these [17, 51].
Perceived fatigue in SMA is common, frequently severe, and similar in magnitude to that reported in other chronic neurological disorders [6, 16]. Our findings highlight the complexity of the relationship between perceived fatigue and fatigability, requiring a multilevel approach to separate the various mechanisms involved in this debilitating symptom. The PedsQL™ MFS and FSS are patient-reported outcome measures currently available to assess the extent of perceived fatigue and may add value for clinical trials that target symptomatic treatment of fatigue in SMA.
CONFLICT OF INTEREST
The authors have no conflicts of interest to report.
Footnotes
ACKNOWLEDGMENTS
This study is supported by the Department of Defense; USAMRAA Grant/Cooperative award number: 09131005(W81XWH-10-1-0127) and the SMA Foundation. We would like to thank the patients and families who participated in this study.