
Abstract
In this paper, a small antenna is proposed to diagnose skin sarcoma at an embryonic stage. The antenna has an area of 30.54 × 15.27 mm2 and resonates at 1429 MHz with a reflection coefficient of −17.64 dB. The structure consists of a 35 μm copper sheet etched on a 1.6 mm FR-4 substrate. The diagnosis is based on the resonance frequency shift, and the SAR (Specific Absorption Rate) variation when the antenna is positioned on malignant tissue. For the simulations, a three-layer body phantom (skin, fat, muscle), and a half-sphere tumor phantom were considered. Simulations of the antenna performances showed that for a tumor of 100 μm, the resonant frequency, and the SAR decrease by 2 MHz, and 1.09 mW/Kg, respectively. In addition to sarcoma detection, the antenna’s 3.6 dBi gain allows for 124.47 m biomedical communication links in a complex environment.
Keywords
Introduction
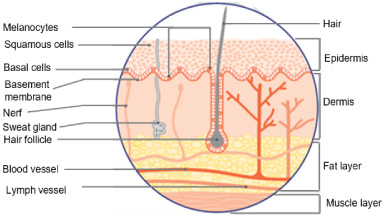
The skin is the organ that covers the entire human body and protects other organs against all forms of external aggression. To ensure this role, it is constantly renewed by rejecting dead cells toward the superficial surface. The structure of skin includes several sub-layers whose thicknesses vary depending on the organ it covers. According to [1], healthy skin (1–4 mm) mainly includes three parts: the epidermis, the dermis, and the hypodermis. Figures 1 and 2 illustrate the different parts of healthy skin.
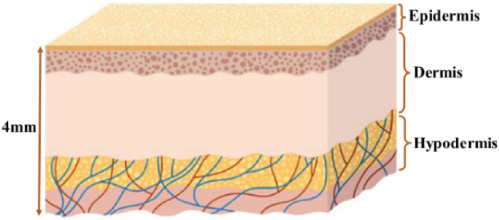
Simplified skin structure.
In addition to abrasions, cancer is the main skin disease. Skin cancer occurs when the cells of a tissue are deeply altered due to an external shock (smoking, alcoholism, solar radiation, virus attack, electromagnetic radiation) or a genetic predisposition. The proliferation of diseased cells then causes the formation of a tumor.
Skin cancer is a form of cancer that is developing more and more due to the emergence of factors such as the aging of the population, the change of leisure habits and the fashion of tanned skin [3]. According to [4], skin cancer is on the rise in recent years. In fifteen years, the annual number of new cases in Belgium has risen by almost 400% between 2004 and 2018.
Depending on their location in the skin, there are several types of cancer.
Basal cell carcinomas represent 70% of skin cancers. They develop when the keratinocytes located in the deepest layer of the epidermis (stratum basale) are altered. Basal cell carcinomas can occur on almost any part of the body including the face, head, neck, trunk, limbs, feet and even the genitals [1]. The size of the carcinomas may approach 20 mm at their metastasis stage.
Melanoma and squamous cell carcinoma constitute about 20% of skin cancers. Skin melanomas develop from melanocytes and are the least frequent but most serious form of epidermis cancer.
Skin sarcoma is a kind of cancer that develops in the dermis and hypodermis. It accounts for 2% of all cases of skin cancer. The diagnosis of skin sarcoma is overly complex, so it is recommended to have at least two expert opinions. The most used diagnosis to detect a skin sarcoma is histology which allows to characterize the tumor by taking and analyzing a fragment of tissue (anatomopathology).
Whatever the type of skin cancer, early diagnosis helps to avoid proliferation through metastasis or invasive disease. It can also increase the patient’s chances of recovery.
Several methods are used to diagnose skin cancers:
Visual inspection of the lesion is the best-known ancestral method [1].
Biopsy [5], dermoscopy [6], HD imaging, and confocal microscopy [7] are techniques based on microscopic observation and imaging. Electrical impedance spectroscopy and electrical impedance tomography focus on variations in cell conductivity. New diagnostic methods based on the analysis of the dielectric characteristics (permittivity, conductivity, and tangent loss) of tissues [8].
In most cases, these new diagnostic methods exploit the impact of dielectric characteristics on antenna resonance or variations in the Specific Absorption Rate of tissues [9,10]. They are not capable of detecting tumors in the embryonic stage. On the other side, traditional methods are often costly and complex to implement, so they are either abandoned or rarely used [1].
The aim of this study is therefore to propose a modern method capable of diagnosing cutaneous sarcoma at an early stage with a high degree of accuracy and at low frequency bands.
To achieve this objective, in this paper, a wearable loop antenna structure is investigated and designed for the early diagnosis of skin sarcomas. The proposed antenna consists of a small meander structure fed by a discrete port. It has been dimensioned to resonate in the Wireless Medical Telemetry Service band (WMTS).
Beyond the introductory part, the remainder of this paper consists of three parts: Section 2 presents the structure and performance of the proposed antenna. Section 3 compares the performances of the proposed antenna with those described in the related literature. Finally, Section 4 presents a conclusion of the study. It also gives the future direction of this work.
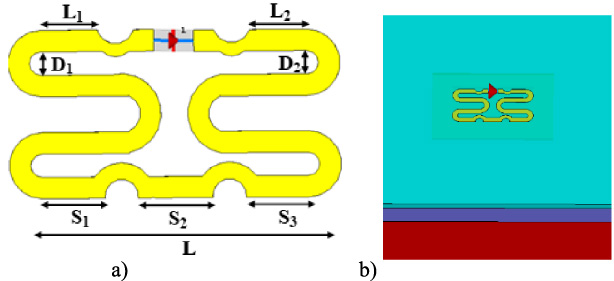
Antenna geometry: (a) spread antenna, (b) profile view of the antenna on the 3-layer phantom (light blue, dark blue, red).
Antenna structure
In this study, we propose an antenna for the early diagnosis of skin sarcoma, a rare but dangerous type of cancer. The antenna structure is the same as the one presented in the paper [11]. To adapt the characteristics of the proposed antenna to the application requirements, we have used FR-4 as the substrate, and superstrate instead of polyimide then we have optimized its dimensions. The use of the proposed antenna involves placing it on the skin of the area under investigation and measuring the resonance frequency and the Specific Absorption Rate. The stage of the tumor is finally defined from the scale of the cancer tumor stage (Table 3) and the SAR variation (Table 5).
To simulate the antenna parameters in the presence of the human body, a three-layer phantom was used. This model was used because it is considered in several studies to be the closest to the reality of the human body [12,13]. The phantom consists of a thick layer of muscle on which is placed a thin layer of fat. The skin, the superficial layer of this model, is thinner than the others. In this study, we considered the muscle, the fat, and the skin, with thicknesses of 27.5 mm, 8.5 mm, and 2.5 mm respectively.
Figure 3 shows the geometry of the antenna spread out and placed on the 3-layer model.
Table 1 presents the dimensions of the proposed antenna.
Free space simulation
To verify that the antenna will have radiation directed towards the experimented tissues, we simulated the reflection coefficient and the gain of the antenna in free space.
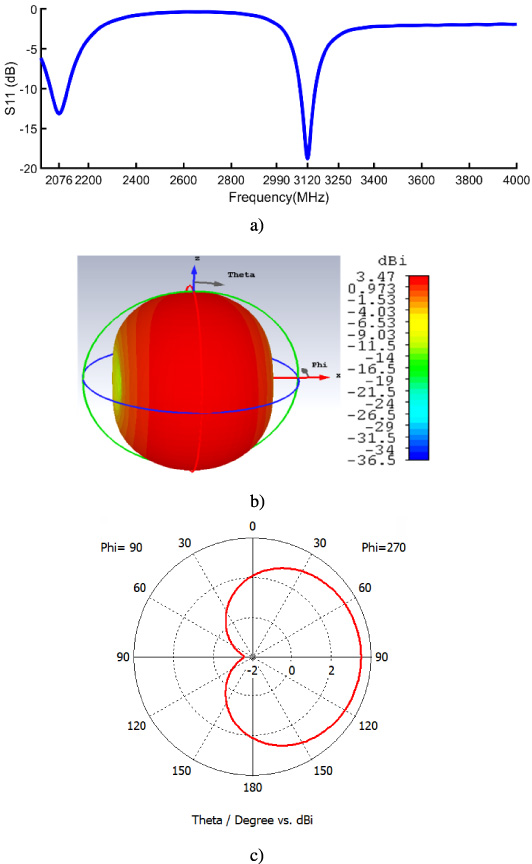
Free space antenna performances a) reflection coefficient b) antenna 3D directivity at 1st resonance, c) Co-polarization.
The Results in Fig. 4(a) show that the antenna has two resonant modes. The first mode is realized at frequency of 2076 MHz and the second is obtained at 3120 MHz. Figure 4(b) shows that the gain of the antenna at 3120 MHz frequency is 3.47 dBi. It also proves that the radiation is directed in the direction of the axis (ox) i.e., in the plane orthogonal to the tissues.
Proposed antenna dimensions
We also simulated the performances of the antenna when it is in direct contact with the skin. As shows in Fig. 5 antenna presents a frequency resonance at 1429 MHz with a reflection coefficient of −17.64 dB. It has a bandwidth of 284 MHz extended from 1278 MHz to 1562 MHz and a gain of 3.6 dBi.
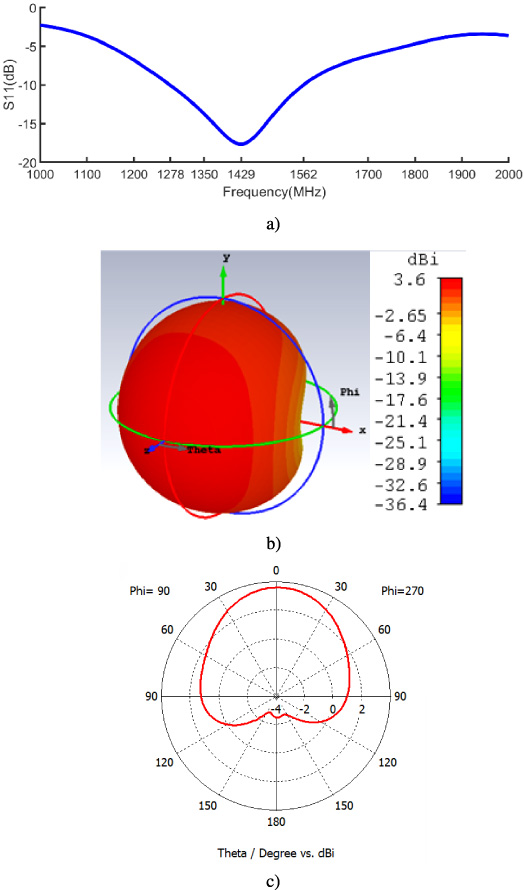
Performance of the antenna on the phantom (a) simulated reflection coefficient (b) antenna 3D directivity at 1st resonance, (c) Co-polarization.
Besides its performances, our proposed antenna can be used to establish a link in IB2OB (In-Body to On-Body) communications in the WMTS (Wireless Medical Telemetry Systems) bands of 1395–1400 MHz and 1427–1432 MHz.
However, our goal is to use the antenna to diagnose cancers of the skin sarcoma at early stages. Today, cutaneous sarcomas are often diagnosed in advanced stages and the diagnosis is overly complex as stated in the introductory section. We therefore considered the characteristics of the three tissues (Skin, Fat, Muscle) at the 1.5 GHz frequency available in the database of dielectric characteristics of healthy tissues [14]. Table 2 summarizes the essential characteristics of those tissues.
Characteristics of the tissues
Scale to determine the cancer tumor stage
The cancerous tumor was modeled as a half-sphere with its center at the lower boundary of the hypodermis. Figures 6a and 6b show the tumor in the tissue.
The reflection coefficient of the antenna was simulated from the embryonic stage of the tumor to a stage where it could be invasive. At the embryonic stage, the tumor has a dimension of 100 μm. It has a relative permittivity (𝜀 r ) and conductivity (𝜎) of 51.02 and 4.84 S/m, respectively. The tumor is considered invasive if its size reaches 4/5 of the skin thickness. This corresponds to a tumor radius of 2 mm since we took an average skin size of 2.5 mm.
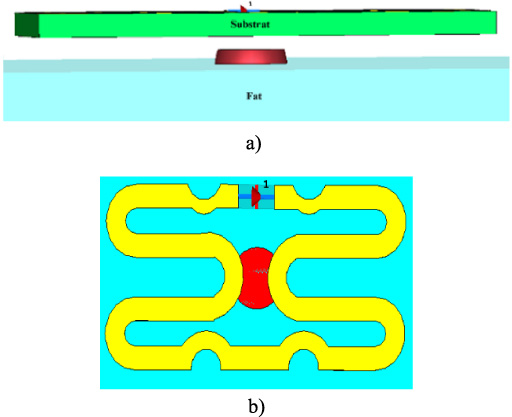
Tissues with tumor: (a) Longitudinal view of the tumor modeled in the embryonic state (the skin is transparent), (b) antenna large section on the tumor.
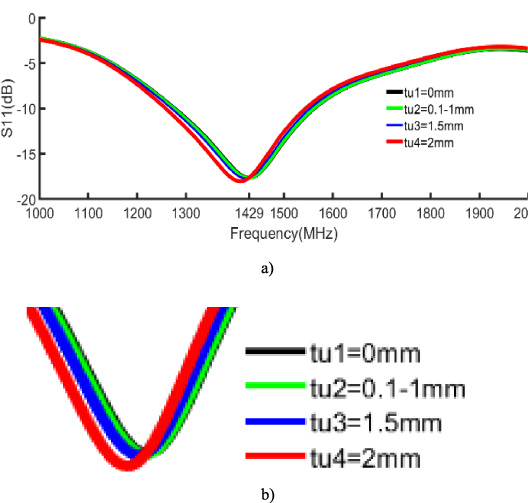
Simulated reflection coefficient (a) normal view (b) enlarged section.
The simulation results have been depicted in Fig. 7.
The curve analysis in Fig. 7 clearly shows that for a skin with fixed characteristics and fixed tumor permittivity, the increase in tumor volume drops the resonant frequency. The variation reaches 18 MHz for flared tumors (2 mm radius). This variation represents a 1.2% shift in resonance due to a higher permittivity of the tumor. The result is consistent with the 3.5% and 2.2% observed by Zahra Katbay [11] at 1005 MHz and 2247 MHz. In addition, the difference is due to the 5 mm tumor size she used in her study.
In consideration of these results, we have established Table 3 to serve as a scale in determining the stage of a cancerous tumor.
The cells of the stem tumor can multiply to spread in the hypodermis tissue (invasive tumor) or reach tissues of other organs (metastasis).
To simulate the antenna reflection coefficient at an invasive tumor stage, a pattern of 5 identical tumors were used. The simulation showed that the resonance dropped by 7 MHz compared to that of a single tumor in the invasive state. Furthermore, for tumors in the embryonic state, the difference is very minor. This proves that the antenna should be used to detect tumors that are still localized, i.e., in the embryonic state.
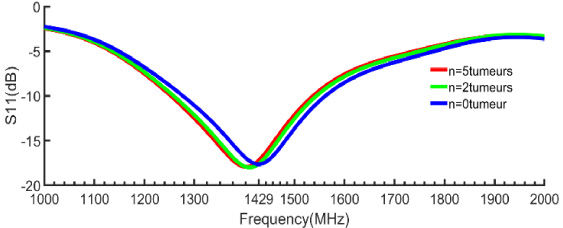
Resonance mode shift in the invasive state.
The antenna has been observed under conditions of varying skin thickness, permittivity, and conductivity.
It observed that the thickness of the skin has an influence on the resonance frequency. We observed that for the same size of fixed tumor, as the thickness of the skin increases, the resonance is towards the low frequencies. Moreover, its capacity to distinguish a malignant tissue from a benign tissue remains the same. This proves that a single antenna cannot detect tumors in all parts of the body, especially since some parts are not of the same thickness. The dimensions of the proposed antenna have been adjusted for an average thickness of 2.5 mm. Figure 9 shows the variation of the simulated reflection coefficient when varying the thickness of the skin.
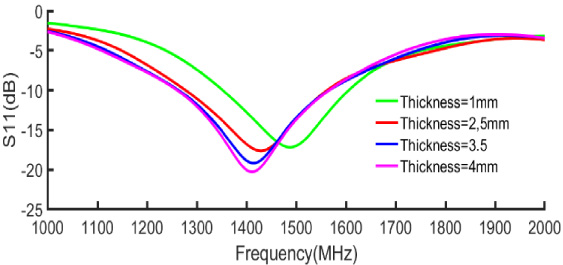
Simulated reflection coefficient for different skin thicknesses.
By varying the permittivity of the skin from 42 to 47, simulations showed that the resonant frequency shifted only by 1 MHz. So, the proposed antenna can be used at 1429 MHz with both dry and wet skins.
When also varying the conductivity from 0.7 to 1.2 S/m, changes in the resonant frequency were observed only for the two extremes where it had moved from 1429 to 1433 MHz. For the other discrete values used between 0.7 S/m and 1.2 S/m, the resonant frequency remained at 1429 MHz. The antenna can therefore be used with various fabrics of conductivities.
The Specific Absorption Rate (SAR)
To evaluate the risk of ionization of the tissues, we have analyzed the Specific Absorption Rate (SAR). The permissible values of the SAR for 1 g and 10 g of tissue are set by the ANSI (American National Standard Institute) at 1.6 W/Kg and 2 W/Kg respectively [15]. The SAR was determined theoretically and then by electromagnetic simulation considering a 3-layer model with a volume of 90 × 90 × 38.5 mm3. Equation (1) [12] was used for the computations.
For a simulation power of 0.5 W, a proportion of 0.437 W was absorbed by the 3 tissues (skin, fat, muscle).
The calculated SAR at 10 g of tissue is 1.38 W/Kg and the simulated value is 1.26 W/Kg according to the simulation sheet Table 4.
Simulated results of the SAR
SAR variation
These theoretical results agree with those of the simulation. These SAR values are both well below the maximum value of 1.6 W/g authorized by the American National Standard Institute (ANSI).
To illustrate the low level of SAR, we generated the distribution of the power lost in the tissues (Fig. 10).
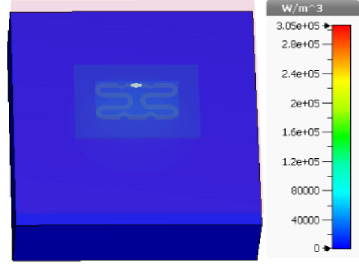
Distribution of the power loss in tissues.
The blue color of the distribution in Fig. 10 shows that the power absorbed is indeed very low. The use of the proposed antenna will therefore have no adverse electromagnetic effects on the tissues.
SAR variation has been exploited in several [10,15] papers to detect the presence of a cancerous tumor. This approach is also exploited here to diagnose cutaneous sarcoma at an early stage. We varied the size of the cancer tumor, and we analyzed the impact on SAR. Table 5 shows the results of this simulation.
Two statements result from those results. The SAR of the normal tissue is higher than that of the diseased tissue. Furthermore, as the tumor size increases, the SAR decreases. This is since the tumor absorbs liquids, and this increases the density of the tissue.
The results of this study corroborate those obtained by K. Brinda and his group in the paper [16] where they observed a decrease in SAR of 1/1000 W/Kg.
We can therefore state that any variation in the SAR of a tissue compared to that of the healthy tissue would prove that the tissue is affected by a tumor. The difference between the two values of SAR depends on the size of the tumor.
Link budget
As mentioned in part 2.3., the antenna can be used to establish IB2OB communication. It can be integrated for example in a sensor of an IoMT (Internet of Medical Things) network to transmit the measurements directly to a connected Gatway. To ensure this capability, we have evaluated the range of the signal generated by the antenna when it is excited with a Gaussian voltage of 1 V. When the antenna is well matched, the range of the signal can be estimated with Eq. (3) and Eq. (4) from the article [17].
P t is the transmitted power, G t and G r are the transmitted and the received antenna gains, L is the path loss, n is the propagation exponent which is 3 in NLOS (None-Line-Of-Sight) situation. G t is our proposed antenna gain at the resonance and G r is the gain of an IoT node.
NLOS propagation is the mode of wave propagation in media with obstacles. Obstacles can cause losses in the signal level due to propagation mechanisms (reflection, refraction, diffraction, and absorption). The direct consequence of the loss of the signal level is the decrease of the range of the radio waves. From Eq. (3) and Eq. (4) we can derive Eq. (5).
This shows that the antenna can equip sensors communicating with an IoT gateway in a large hospital. This antenna is therefore a good candidate for the vulgarization of IoMT.
Table of link budget parameters
From the Table 7, we can assert that the suggested antenna is the only one able to detect tumors in the depth of the skin at an embryonic stage (100 μm).
Performances comparison table of the proposed antenna with other antennas
Performances comparison table of the proposed antenna with other antennas
In this work, an antenna of 30.54 × 15.27 × 1.6 mm3 resonating at the frequency of 1429 MHz was proposed. The antenna allows the detection of skin sarcomas at a rather early stage. The diagnostic of this dangerous type of cancer is based on both the interpretation of the variations of the resonance frequency and the SAR. The characteristics of the antenna were simulated with healthy skin and then with skin affected by a cancerous tumor of the hypodermis (skin sarcoma). The simulation with the malignant tissue shows that the resonant frequency, and the SAR decrease by 1.2%, and 1/1000 W/Kg respectively, compared to the healthy tissue. The antenna can also establish IB2OB communication links of 124.47 m. Based on the good performances of the proposed antenna, it could be a good candidate for skin cancer detection and other biomedical applications. The next step in this study is to build a prototype of the antenna with a view of comparing the simulated performances with the measured ones.