
Abstract
Using amyloid PET imaging as a single primary surrogate efficacy measure in Alzheimer’s disease immunotherapy trials, as happened when the FDA granted accelerated approval of aducanumab, is unjustified. In vivo evidence indicates that PET quantification of amyloid deposition is distorted and misrepresents effects of anti-amyloid treatments due to lack of specificity of the PET imaging probe, effects of amyloid-related imaging abnormalities, spill-over from high white matter signals, and questionable quantification models. Before granting approval to other immunotherapy candidates, the FDA should require rigorous evidence of all imaging claims and irrefutable documentation that proposed treatments are clinically effective and harmless to patients.
On June 7, 2021, the FDA granted accelerated approval to aducanumab (marketed as Aduhelm by Biogen) for the treatment of Alzheimer’s disease (AD), against the recommendation of its advisory panel. The Agency indicated that this major decision was solely based on a single primary outcome measure, i.e., a presumed reduction in cerebral amyloid-β (Aβ) deposits implied by amyloid PET images [1], and with an expectation that this would subsequently ‘lead to a reduction in cognitive decline’ [2].
Even though the use of biomarkers as a single primary surrogate efficacy measure can be considered for accelerated approval, this was a surprising move. The FDA guidance for developing drugs for the treatment of early AD [3], explicitly indicates that the Agency does not support their use (February 2013, updated in February 2018 for comments only, current as of 04-21-2020) [4]. No reported new evidence since then indicates that amyloid PET imaging fulfills the critical requirement established in the FDA guidance. Not surprisingly, the FDA’s accelerated approval of aducanumab, an immunotherapy treatment drug, without a documented significant positive clinical effect, has received widespread criticism [5].
Multiple lines of evidence negate support for the use of amyloid PET as a single primary outcome measure for these treatments. Below we point to some of the most important reasons, each of which should make the FDA refrain from using amyloid PET imaging as an endpoint technique.
Firstly, amyloid PET biomarkers for Aβ deposition have insufficient in vivo specificity and, in addition, poor overall agreement of the amyloid PET signals with CERAD neuritic plaque ratings in postmortem determinations [6]. The historical claim that amyloid PET imaging biomarkers label Aβ aggregates [7] has not received consistent support. The literature also present claims that these biomarkers label oligomers and that in many cases the positive brain signals were obtained with no evidence for the presence of Aβ aggregates [8]. Part of the problem resides in the fact that the FDA-approved amyloid PET imaging biomarkers are structurally diverse, have different in vitro affinity for Aβ, and different specificities. The uncharged derivatives of thioflavin-T (11C-PiB and 18F-flutemetamol) have also been shown to be retained nonspecifically by non-amyloid tissue targets, e.g., estrogen sulfotransferase, an enzyme that is elevated in brain inflammation [9, 10]. The other FDA-approved imaging biomarkers from the family of trans-stilbene derivatives (18F-florbetapir and 18F-florbetaben), have received limited in vivo Aβ specificity evaluations. 18F-florbetapir, which has questionably been used to ‘quantify’ brain amyloid removal by aducanumab and related treatments, is a very hydrophobic molecule, the in vivo retention fate of which is attributed to Aβ pathology. However, the signal decrease upon treatment observed in the white matter, an area typically lacking Aβ deposition, is likely due to another process involved in its brain accumulation.
Secondly, the presence of amyloid-related imaging abnormalities (ARIAs) resulting from these anti-amyloid treatments would, among other factors, locally affect blood brain barrier diffusion and diminish tissue accumulation of the PET biomarkers, regardless of presence or absence of Aβ deposition [11]. Therefore, attributing lower brain amyloid PET signals in patients with ARIAs solely to the anti-amyloid treatments, without further analysis, is scientifically indefensible.
Thirdly, the large non-specific white matter signal consistently found in PET images with all Aβ brain imaging agents (e.g., 18F-florbetapir, 18F-florbetaben, and 18F-flutemetamol) results in significant spill-over and partial volume effects over the cortical signals [7]. Moreover, signal quantification in the grey matter is particularly problematic in the presence of cortical atrophy, as observed in the AD brain.
Thus, due to these unavoidable factors any quantitative or visual qualitative reading would be an unreliable marker of changes in grey matter Aβ deposition, a fact that no arbitrary regional quantification SUVR model with suboptimal regional specificity can possibly correct [12]. Therefore, FDA’s current consideration of further applications for accelerated approval of similar immunotherapeutic AD drugs, e.g., donanemab (Eli Lilly) and lecanemab (Eisai Inc.), using amyloid imaging as a single primary surrogate efficacy measure, without strict consideration of its value is startling. In the donanemab and lecanemab clinical trials, a persuasive description of the amyloid PET imaging methods employed, and their interpretation are woefully inadequate. Without any PET image documentation to support imaging signal decreases with an apparent dose-dependent decrease in amyloid deposits, therapeutic results would be inconclusive and unconvincing [13, 14].
A new example of misleading image documentation is the PET interim analysis of a sub-study designed to evaluate the effect of gantenerumab (Hoffmann-La Roche) on Aβ plaque deposition using 18F-florbetapir PET imaging in patients with prodromal to moderate AD [15]. Similar to what was observed with other treatments, significant decreases are reported with 18F-florbetapir brain white matter signals (Fig. 1). These images, demonstrating white matter labeling and decline with treatment, are by no means confident evidence of the stipulation stated in the FDA guidance for a reduction in cerebral gray matter Aβ deposits that may create any realistic expectations ‘of a reduction in cognitive decline’.
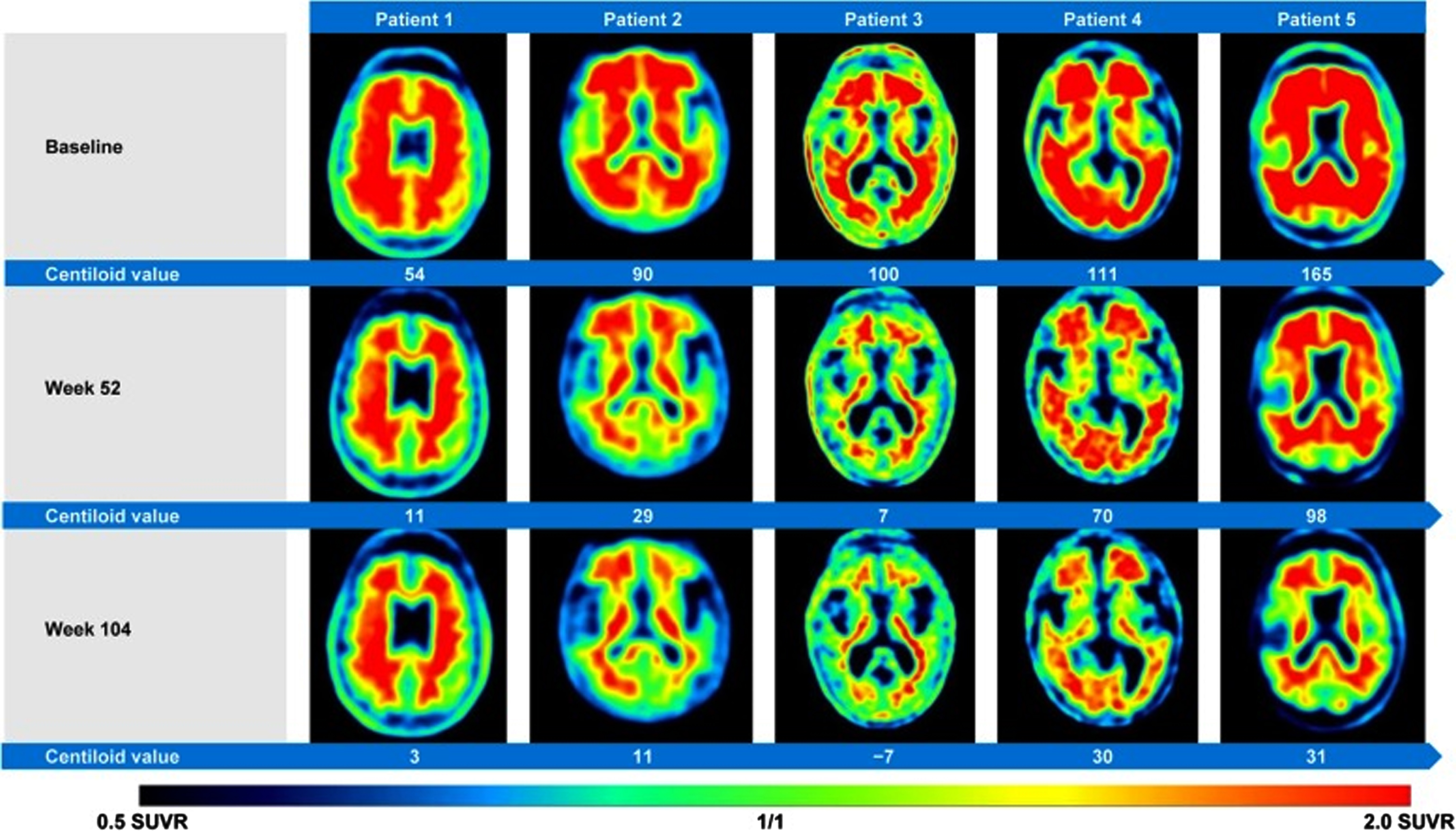
Figure 2 as it appeared in reference [15] with the following legend: “Amyloid-β plaque reduction with Gantenerumab. Axial Florbetapir brain PET images from five patients displaying reduction of amyloid-β plaques from OLE baseline to OLE week 52 and OLE week 104. Axial slices are at the level of the basal ganglia. PET images were obtained 50 min post-injection, SUVR data with the cerebellar cortex as the reference region.” OLE, open label extension. This image is reproduced under the terms of Creative Commons Attribution 4.0 International License.
So far, anti-amyloid immunotherapy treatments, involving many thousands of participants, have shown no appreciable clinical benefits, but instead displayed very concerning immunotherapy-induced brain damage. It is, therefore, incumbent upon the FDA to carefully examine the methodical profile of severe adverse effects, in the context of the questionable efficacy of these treatments, before doing anything else. The functional effect of these immunotherapy treatments can easily be determined by examining a representative, randomly selected, cohort of deliberately treated AD patients with quantitative 18F-fluorodeoxyglucose (FDG) PET imaging to assess their global and regional cerebral gray matter glucose metabolism. Any significant reduction in regional or global FDG PET signals, in a cohort of patients compared with a placebo group, should be tantamount to a failure of the trial with that particular anti-amyloid immunotherapy in AD.
In the best of all circumstances, amyloid PET scans as the sole efficacy measure are only part the story. There are other indicators that might deserve worthwhile consideration. For instance, quantification of plasma Aβ42, as well as the ratio between the two forms (Aβ42/Aβ40) may be used to characterize more efficiently patients with brain amyloidosis [16]. Brain amyloid PET scans with, i.e., 11C-PiB, 18F-florbetaben, or 18F-florbetapir [17, 18], do not offer any discrimination as to the proposed pathogenic forms of brain amyloid deposition.
We are not in a position to point to any specific reasons as to why the amyloid hypothesis has failed so far [19]. We, however, have noted its paradoxical survival for well over 30 years without any proof of its validity and despite multiple indications on the contrary, including the many failed treatment attempts, which should be clear evidence to move in new directions in the search for effective treatments [20].
Amyloid PET imaging has no diagnostic value and presents serious limitations as a single primary surrogate marker of efficacy. Therefore, the recent petition by the “imaging community” to the Center of Medicare and Medicaid Services (CMS) to reconsider its previous National Coverage Determination (NCD), allowing for only one PET Aβ scan per AD patient undergoing monoclonal antibody treatment [21], is without merit. Acceptance by CMS will lead to a large number of superfluous PET Aβ scans, the misleading results of which can only create significant anxiety and unnecessarily disturb patients and their families and impose an additional unnecessary financial burden on the health care system.
Amyloid PET imaging is inappropriate as a single endpoint technique for the FDA approval of immunotherapy in AD. The significant brain damage observed with anti-amyloid immunotherapy treatments, coupled with the absence of documented clinical efficacy, should give the FDA a necessary respite to conduct an obligatory and in-depth review of the immunotreatment side effects and of the PET imaging methods used. This should be done before the Agency even considers processing new applications for approval of immunotherapy in AD. The use of a PET Aβ scans of questionable validity for patient selection and as an endpoint technique of anti-amyloid treatments that have repeatedly been demonstrated not to work, is an extraordinarily disconcerting approach for treating a disease that affects millions worldwide and needs discerning solutions.
DISCLOSURE STATEMENT
Authors’ disclosures available online (https://www.j-alz.com/manuscript-disclosures/22-0841r1).