
Abstract
Background:
Objectively measuring auditory functions has been proposed as an avenue in differentiating normal age-related cognitive dysfunction from Alzheimer’s disease (AD) and its prodromal states. Previous research has suggested auditory event-related potentials (AERPs) to be non-invasive, cost-effective, and efficient biomarkers for the diagnosis of AD.
Objective:
The objective of this paper is to review the published literature on AERPs measures in older adults diagnosed with AD and those at higher risk of developing AD, i.e., mild cognitive impairment (MCI) and subjective cognitive decline.
Methods:
The search was performed on six major electronic databases (Ovid MEDLINE, OVID EMBASE, PsycINFO, PubMed, Scopus, and CINAHL Plus). Articles identified prior to 7 May 2019 were considered for this review. A random effects meta-analysis and analysis of between study heterogeneity was conducted using the Comprehensive Meta-Analysis software.
Results:
The search identified 1,076 articles; 74 articles met the full inclusion criteria and were included in the systematic review, and 47 articles were included into the analyses. Pooled analysis suggests that AD participants can be differentiated from controls due to significant delays in ABR, N100, P200, N200, and P300 latencies. P300 amplitude was significantly smaller in AD participants compared to controls. P300 latencies differed significantly between MCI participants and controls based on the pooled analysis.
Conclusion:
The findings of this review indicate that some AERPs may be valuable biomarkers of AD. In conjunction with currently available clinical and neuropsychological assessments, AERPs can aid in screening and diagnosis of prodromal AD.
Keywords
INTRODUCTION
Dementia due to Alzheimer’s disease (AD) accounts for 60–80%of all dementia cases [1] and is characterized by impairment in episodic memory as well as other cognitive functions [2]. Neurodegenerative changes that lead to AD begin to accumulate approximately 20 years prior to the appearance of clinical symptoms [3, 4]. Extracellular plaques of amyloid-β (Aβ) are one of the primary AD biomarkers closely associated with neural atrophy and synaptic damage, which are associated with gradual neuronal death [3, 5]. Tau protein accumulation and hyperphosphorylation is another histopathological hallmark of AD. It results in the formation of neurofibrillary tangles (NFTs) inside neural cell bodies, ultimately resulting in synaptic loss and neuronal death [6]. Biomarker abnormalities result in substantial brain injury, neural death, and the degeneration of cortical and subcortical structures. Over time, these changes lead to memory loss, further cognitive impairment, and changes in daily living activities representing the clinical symptoms of AD [5].
Biomarkers of AD have been identified using a number of techniques, including positron emission tomography (PET) for amyloid plaques and more recently for NFTs and glucose metabolism, magnetic resonance imaging (MRI) for volumetric and structural changes, and lumbar puncture for cerebrospinal fluid (CSF) biomarkers (e.g., tau and Aβ) of AD [7, 8]. However, both CSF and PET are not available for mass screening of high risk individuals in many remote areas of high-income countries and in many mid to low-income countries due to the expertise, facilities and infrastructure required to conduct these tests [9]. Additionally, the neuronal death that must occur in order to be detectable by MRI or hypometabolism on FDG-PET is substantial and the change, at least for now, are irreversible. Such difficulties limit the applications of these techniques in preclinical early stages of AD, that is, prior to significant brain damage and the appearance of the clinical symptoms [5, 10]. Other limiting factors for these diagnostic methods include their invasive nature and the high cost associated with conducting these tests, which limits their use in routine clinical practice [11–13].
In addition, commonly utilized cognitive impairment screening tests, such as the Montreal Cognitive Assessment (MoCA) and Mini-Mental State Examination (MMSE), have varied sensitivity and specificity [14], resulting in the possibility that some individuals meet the screening criteria for cognitive impairment on one test but not on the other [15]. Furthermore, even comprehensive neuropsychological measures are not specific or sensitive enough to detect very early and preclinical changes in episodic memory, as the primary clinical manifestations of AD [15].
Considering current challenges associated with identification of those at risk (pre-clinical AD) and diagnosing AD and its prodromal stages as well as the availability of disease-altering interventions, it has become imperative to identify other early diagnostic tool(s) and/or diagnostic strategies for preclinical AD [16]. The identified stages that are associated with higher risk of developing AD, i.e., subjective cognitive decline (SCD) and amnestic mild cognitive impairment (MCI), have the potential to define a target population for early AD intervention. This is important as treatments at later stages of the disease show no promise in altering the disease course due to substantial neuronal injury and cognitive impairment already present [17].
In addition to current biomarkers of AD, measuring the brain’s electrical activity using electroencephalo-graphy (EEG) has been proposed as an avenue to detect early brain changes associated with AD and its prodromal stages [18–21]. Neural responses to specific sensory, cognitive and motor processes can be elicited by combining EEG with particular tasks [22]. These responses, also known as event-related potentials (ERP), are a result of the brain’s adjustment from a discorded (high entropy) to an ordered (low entropy) state in response to synchronization to a particular task [23]. In other words, ERPs reflect the changes in the state of electrical brain activity in response to different tasks. ERPs can be analyzed with respect to the intensity of the response (amplitude) as well as the time the response occurs (latency) in relation to the stimulus [22, 24]. ERPs reflect brain activity that is phase and time locked to a presented stimulus, which has been suggested to be an objective tool for the assessment of cognitive status and other brain functions [22, 25].
Cognitive decline has been shown to be strongly associated with hearing loss with the probability of incident dementia log-linearly increasing with the severity of hearing loss [26]. In addition, results from a number of longitudinal studies suggest that changes in central auditory processing skills, even in the absence of severe peripheral hearing loss, are associated with high incidence of cognitive decline and AD [27, 28]. Objectively measuring auditory functions has been proposed as an avenue in differentiating normal age-related cognitive dysfunction from AD and its prodromal states [29–31].
The peaks of distinct auditory event-related potentials (AERP), measured using surface skin electrodes, that present at different latencies are thought to represent neural activity from different anatomical areas along the auditory pathway and associated structures [32]. For this reason, AERPs have been used to objectively evaluate central auditory function, hearing thresholds, and sensory processing [25, 33–35]. Additionally, AERPs have also been suggested to reflect auditory memory, working memory, attention, language comprehension, discrimination and decision-making [36–39]. These AERP components can be characterized into one of three groups: 1) short latency AERPs, 2) middle latency AERPs and, 3) long latency AERPs. Evoked potentials that appear within 12 milliseconds (ms) of an auditory stimulus are considered short latency AERPs and these include: electrocochleography (ECochG), auditory brainstem response (ABR), and frequency following response (FFR). Middle latency AERPs appear between 12 and 50 ms following a stimulus and these include: middle latency responses (MLR), generally labelled Na, Pa and Nb, and Auditory Steady-State Response (ASSR). Finally, AERPs that occur 50 ms or later following an auditory stimulus are considered late latency AERPs. These responses are divided into exogenous (P50 (P1 or Pb), N100, P200 and N200) or endogenous (P300, N400, P600, Mismatch Negativity (MMN), and contingent negative variation (CNV)). Previous research suggested AERPs to be non-invasive, cost- effective and efficient biomarkers for the diagnosis of AD [40–44]. AERPs alone may not provide the required diagnostic specificity as pathophysiological biomarkers (i.e., Aβ and NFTs); however, AERPs can contribute to the first-line screening to identify high-risk individuals that would otherwise be investigated using expensive (PET or volumetric MRI) or invasive (lumber puncture for CSF) methods. Reducing the number of AD related cases that require second-line or further investigation will reduce cost from both a financial and organizational perspective.
Many studies have been conducted on AERPs in people with cognitive decline due to AD. In order to evaluate the currently available literature and identify any gaps in the knowledge, this paper aims to systematically review the published literature currently available on auditory event-related potentials that have been used to assess the auditory functions in older adults diagnosed with AD and its clinical and pre-clinical stages, including those with MCI and SCD. This review and meta-analysis aims to: 1) determine the magnitude of AERP latency and amplitude abnormalities present in SCD, MCI, and AD participants compared to controls, 2) determine which AERPs can differentiate between the subject groups (normal healthy controls, SCD, MCI, and AD), and 3) determine which AERPs can yield a possible biomarker for pre-clinical and early clinical AD, i.e., SCD and MCI.
METHODS
All full-length peer-reviewed publications of original data that measured AERPs in people with AD, MCI, SCD, and age-matched controls available on electronic databases prior to 7 May 2019 were considered for this review. The search was performed on major electronic databases (Ovid MEDLINE, OVID EMBASE, PsycINFO, PubMed, Scopus, and CINAHL Plus) using keywords alone or in combination with Medical Subject Headings divided into two domains: 1) auditory tests and 2) AD. Only studies with specified aMCI participants were included in the meta-analyses; MCI studies that did not specify aMCI, however, still fit the remaining inclusion criteria were included in the summary table for descriptive purposes. A random effects meta-analysis and analysis of between study heterogeneity was conducted using the Comprehensive Meta-Analysis software, version 3. Methods were informed by Cochrane guidelines for systematic reviews [45] and the methodological approach is outlined in detail in the review protocol [46].
RESULTS
Search result
As shown in Fig. 1, a total of 1,076 titles and abstracts were screened against the eligibility criteria. Of the screened articles, 852 were excluded based on the information provided in the title and abstract, and 224 articles were selected for full text review. A total of 74 articles met the full inclusion criteria and were included in the systematic review, and 47 were added into the various meta-analyses. Articles were excluded from the meta-analysis for one or more of the following reasons: 1) mean values were not reported and/or could not be obtained, 2) standard deviation (SD) and/or standard error values were not reported and could not be obtained, and 3) one or more of the participant group(s) results were reported in multiple articles. In the latter case only the data from most recent article were included in the meta-analysis. Meta-analyses were not conducted for AERPs if: 1) there were less than two studies using the same testing paradigm in the same participant groups (e.g., Three-tone active oddball paradigm, Active vowel discrimination task), and 2) there were less than three articles on the same AERP.
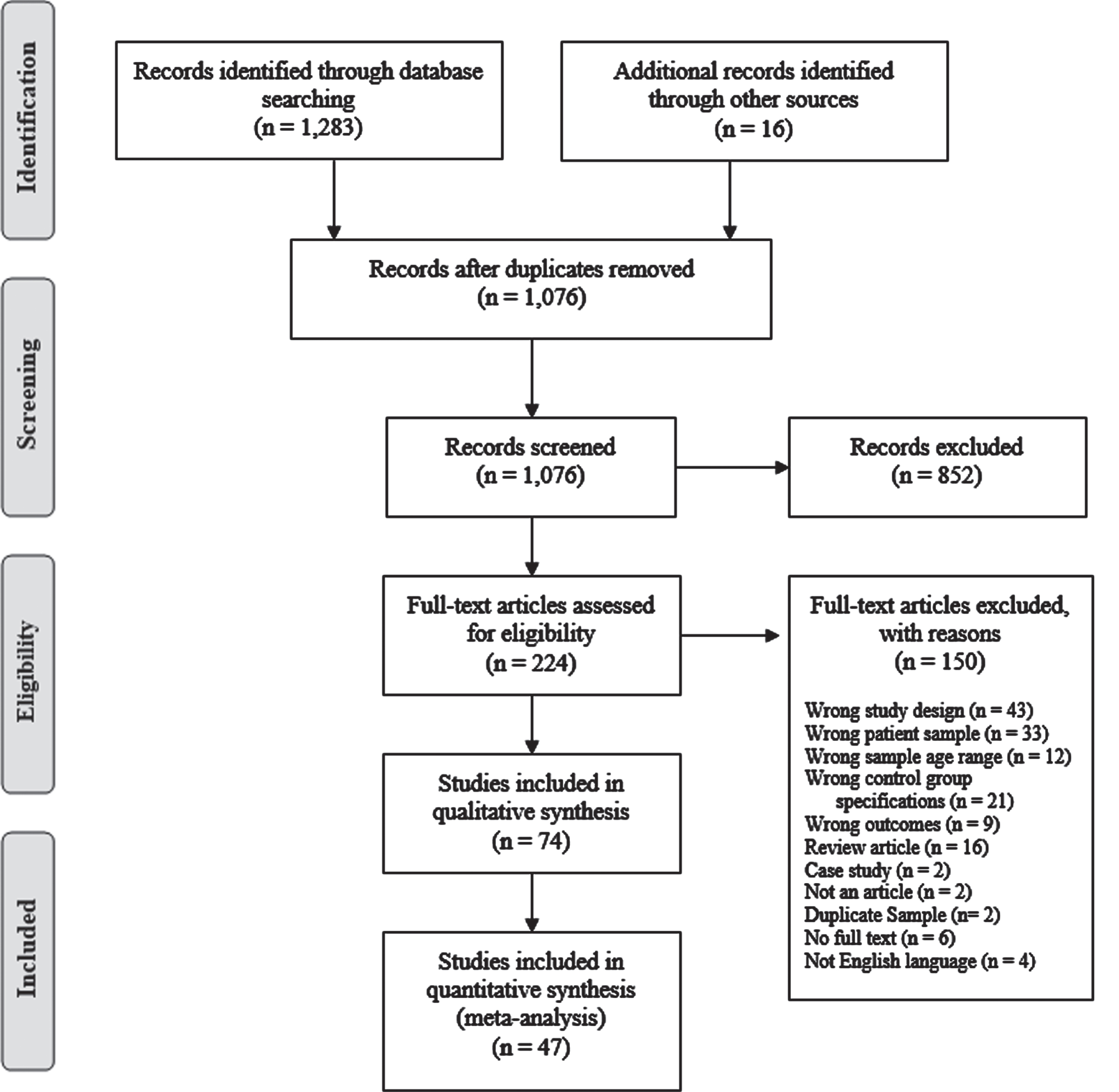
PRISMA flow diagram of search result.
Study characteristics
All studies included in the review compared auditory electrophysiological assessments in a group of participants with cognitive impairment or cognitive complaints with a healthy (non-complainers) age-matched control group. Fifty-four studies compared participants with AD to healthy controls, 11 compared participants with MCI to healthy controls, 9 compared both participants with MCI and AD to healthy controls, while none were found which compared participants with SCD to healthy controls. The studies included a total of 3,740 participants (1,455 AD, 615 MCI, 0 SCD and 1,670 controls) from 25 countries. The majority of the studies used the National Institute of Neurological and Communicative Disorders and Stroke and the Alzheimer’s disease and Related Disorders Association (NINCDS-ADRDA) and/or Diagnostic and Statistical Manual of Mental Disorders (DSM) criteria to diagnose AD (52 out of 62 studies), one study used neuropsychological assessments by certified neurologist coupled with the Mini-Mental State Examination (MMSE) and Wechsler Memory Scale, one study used the Clinical Dementia Rating (CDR) and 8 studies used other neuropsychological evaluations and/or medical imaging (see Table 1). MCI was diagnosed using the Petersen’s criteria [47] and/or DSM criteria in most studies (15 out of 20 studies) included in the review, Smith’s 1996 criteria was used in two studies [48], Winbald’s criteria [49] was used in one study, and 2 studies used other neuropsychological evaluations to diagnose MCI, as described in Table 1.
Characteristics of auditory event-related potential cohort studies included in the systematic review
AERP, Auditory event-related potential; AD, Alzheimer’s group; MCI, Mild cognitive impairment group; SCD, Subjective cognitive decline group; HC, Healthy controls (aged matched); CDR, Clinical dementia rating; NINCDS-ADRDA, National Institute of Neurological and Communicative Disorders and Stroke and the Alzheimer’s disease and Related Disorders Association; DSM, Diagnostic and Statistical Manual of Mental Disorders; MoCA, Montreal Cognitive Assessment; MMSE, Mini-Mental State Examination; DRSS, Dementia Rating Severity Scale; B-RDS, Blessed-Roth Dementia Scale; BADLS, Bristol Activity of Daily Living Scale; TS-P300, Temporo-superior P300 component; TB-P300, Temporo-basal P300 component; IPL, Interpeak latency; L, Left ear; R, Right ear; MCI-SD, Single domain amnestic mild cognitive impairment; MCI-MD, Multiple domain amnestic mild cognitive impairment; MCI-P, Mild cognitive impairment patients with progressive decline; MCI-S, Stable mild cognitive impairment; AD-N, Treatment naïve; AD-T, Treatment group (10 mg/day donepezil); APOE E4+, Apolipoprotein E4 alleles positive; APOE E4-, Apolipoprotein E4 alleles negative; MMN, Mismatch negativity; FFR, Frequency-following response; ABR, Auditory brain response; ASSR, Auditory steady-state response; MLR, Middle latency response.
Studies included in the review assessed most AERPs including: ABR, ASSR, FFR, MLR, MMN, positive late latency AERPs (P50, P200, and P300), and negative late latency AERPs (N100, N200, N400). These AERPs were elicited using varying cognitive tasks, including passive double (paired) click paradigm, active (two-tone and three-tone) oddball paradigm, passive oddball paradigm, active vowel discrimination task, passive (rarefaction clicks) hearing task, semantic activation task and spoken word paradigm. The studies included in the systematic review are summarized in Table 1.
Meta-analysis
The results of the meta-analyses are reported as standard difference in mean (SMD) with 95%confidence intervals (CI) as the synthesized measure of effect size. The meta-analyses results are reported under the random effects model, which accounts for any variations between study methodologies. An effect size between 0.2 and 0.5 is considered a small effect, between 0.5 and 0.8 is considered a medium effect, while an effect size 0.8 or higher is considered a large effect [50]. The Cochrane’s Q-Value statistic was performed to test heterogeneity of the studies and the I-squared (I2) statistic was performed to indicate heterogeneity as a percentage. Heterogeneity analysis results are presented as part of the “summary” on the meta-analyses forest plots.
Auditory brainstem responses and mismatch negativity
Compared to the control group, AD participants had significantly prolonged ABR Wave V latencies, pooled SMD: 0.46 (n = 4, 95%CI: 0.10 to 0.82, p = 0.01; Fig. 2A). Although the effect size would be considered small (< 0.5) [50], the variation in ABR wave V latency between participants with AD and healthy controls was significant when using a passive rarefaction click paradigm. No significant difference in SMD between controls and AD participants was seen in ABR waves I and III; pooled SMD: –0.06 (n = 3, 95%CI: –0.42 to 0.31, p = 0.76; Supplementary Figure 1A) and 0.25 (n = 3, 95%CI: –0.11 to 0.62, p = 0.18; Supplementary Figure 1B), respectively. A statistically significant difference in pooled SMD between controls and AD participants was present in interpeak I-V and interpeak I-III latencies; SMD 0.47 (n = 6, 95%CI: 0.16 to 0.77, p = 0.00; Fig. 2B), and 0.34 (n = 4, 95%CI: 0.03 to 0.64, p = 0.03; Fig. 2 C), respectively. There was no significant difference in interpeak III-V latencies between AD participants and controls in the reviewed studies, pooled SMD: 0.31 (n = 5, 95%CI: –0.17 to 0.80, p = 0.21; Supplementary Figure 1 C). MMN amplitude did not differ significantly between AD and control participants when elicited using the passive oddball paradigm and pooled analysis revealed no effect (effect size < 0.2 [51]), SMD: –0.06 (n = 3, 95%CI: –0.46 to 0.34, p = 0.76; Supplementary Figure 2).
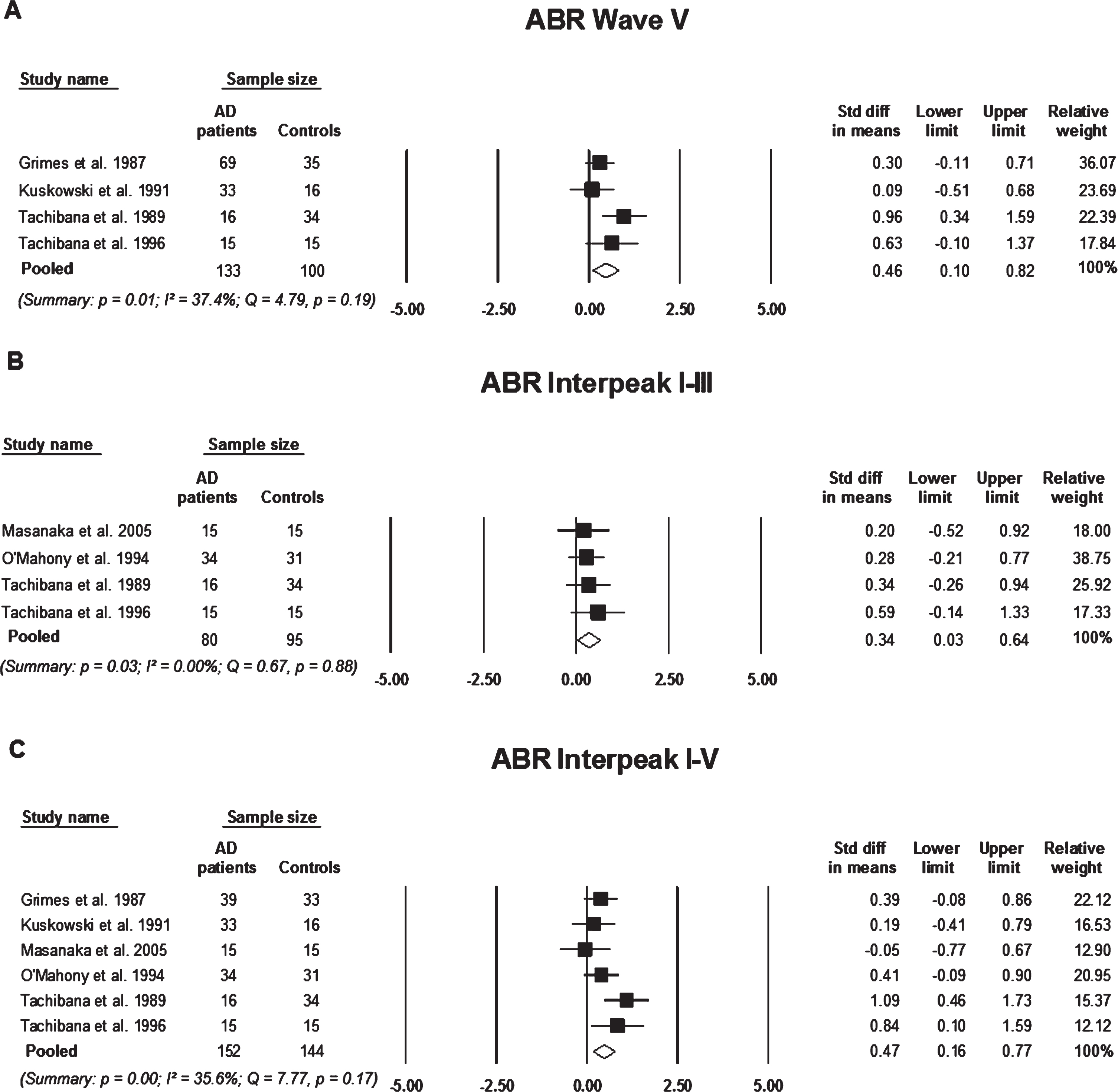
Standard mean difference and pooled estimated of each study included in the meta-analyses of auditory brainstem responses (ABR) elicited using the passive rarefaction click paradigm. All the analyses compare participants with Alzheimer’s disease (AD) to controls A) analysis of ABR wave V latency, B) analysis of ABR interpeak wave I-III, and C) analysis of ABR interpeak wave I-V. Summary includes: p = significance level; I2 = percentage of heterogeneity; Q = Cochrane’s Q. The horizontal lines represent the 95%confidence interval for each computed standard mean difference. Note: weights are from random effects analysis.
P50 (Pb or P1)
P50 elicited using the paired-click paradigm varied significantly in amplitude and latency between AD participants and controls. AD participants had larger P50 amplitudes and prolonged P50 latencies in comparison to controls, pooled SMD: 0.67 (n = 4, 95%CI: 0.33 to 1.01, p = 0.00; Fig. 3A) and 0.33 (n = 4, 95%CI: –0.01 to 0.66, p = 0.05; Fig. 3B), respectively. The pooled effect size suggests that the average P50 amplitude for a participant in the AD group is 0.67 SD above that of a participant in the control group, hence the average AD participant would have larger P50 amplitude than over 73%of the participants in the control group. On the other hand, pooled analysis of P50 elicited using the rarefaction click paradigm showed no significant difference in P50 amplitudes or latencies between controls and AD participants (n = 2; Supplementary Figure 3).
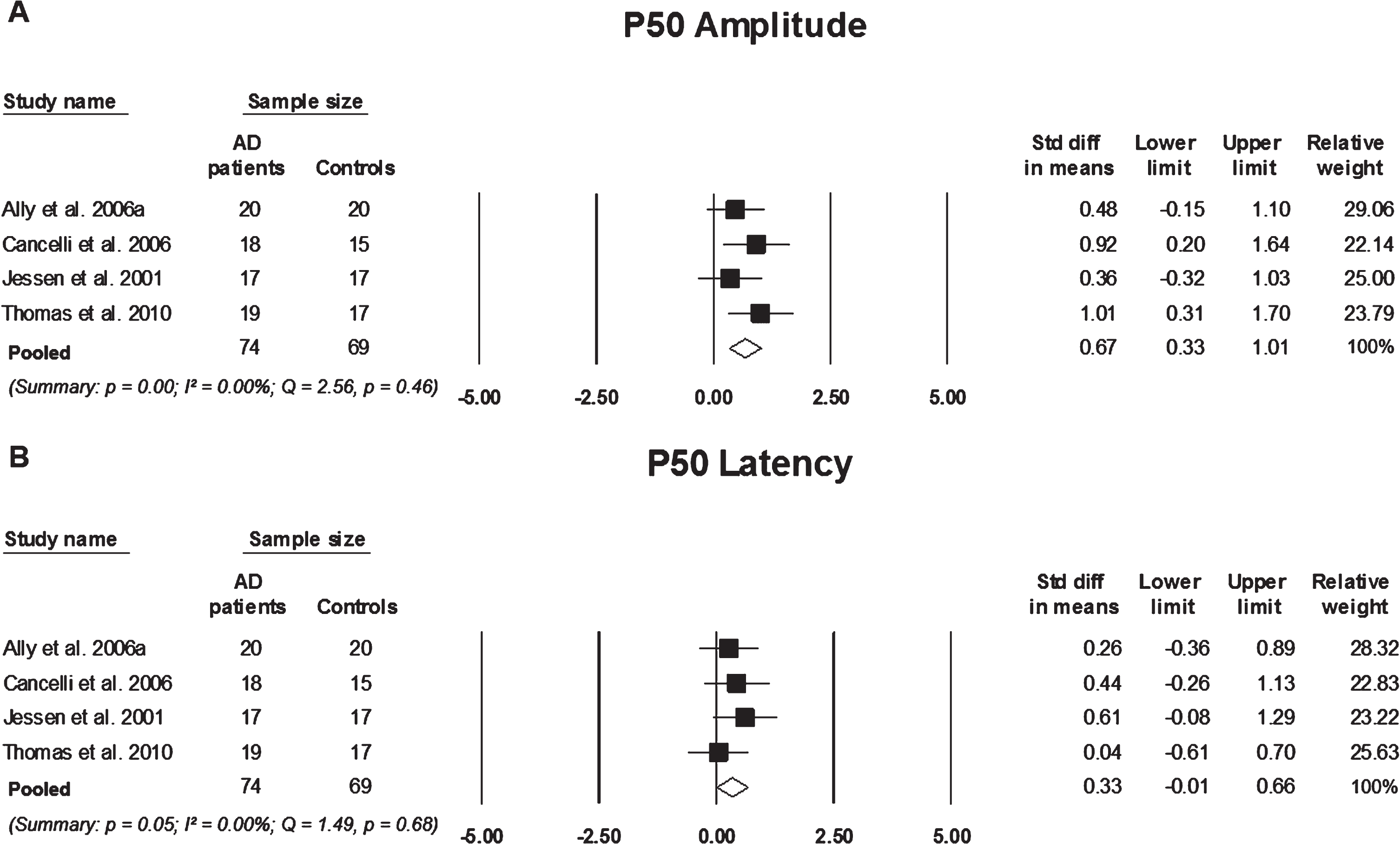
Standard mean difference and pooled estimated of each study included in the meta-analyses of P50 elicited using the paired-click paradigm. A) comparing P50 amplitude between participants with Alzheimer’s disease AD to controls, B) comparing P50 latency between participants with AD and controls, Summary includes: p = significance level; I2 = = percentage of heterogeneity; Q = Cochrane’s Q. The horizontal lines represent the 95%confidence interval for each computed standard mean difference. Note: weights are from random effects analysis.
Although there was a small pooled effect size, participants with AD showed prolonged N100 latencies in comparison to control participants, pooled SMD: 0.32 (n = 14, 95%CI: 0.13 to 0.51, p = 0.00; Fig. 4B). MCI participants did not significantly differ in N100 latency from control participants, pooled SMD 0.20 (n = 2, 95%CI: –0.58 to 0.93, p = 0.59; Supplementary Figure 4A). The SMD between AD, MCI, and control participants were not significant for N100 amplitude (Supplementary Figure 4B,C). Similarly, P200 latencies differed significantly between AD participants and controls, SMD: 0.34 (n = 10, 95%CI: 0.04 to 0.65, p = 0.03; Fig. 4A), however, did not differ significantly between MCI and control participants. Also, there was no significant difference present in P200 amplitude in participants with AD or MCI in comparison to controls (n = 2, p > 0.05; Supplementary Figure 5).
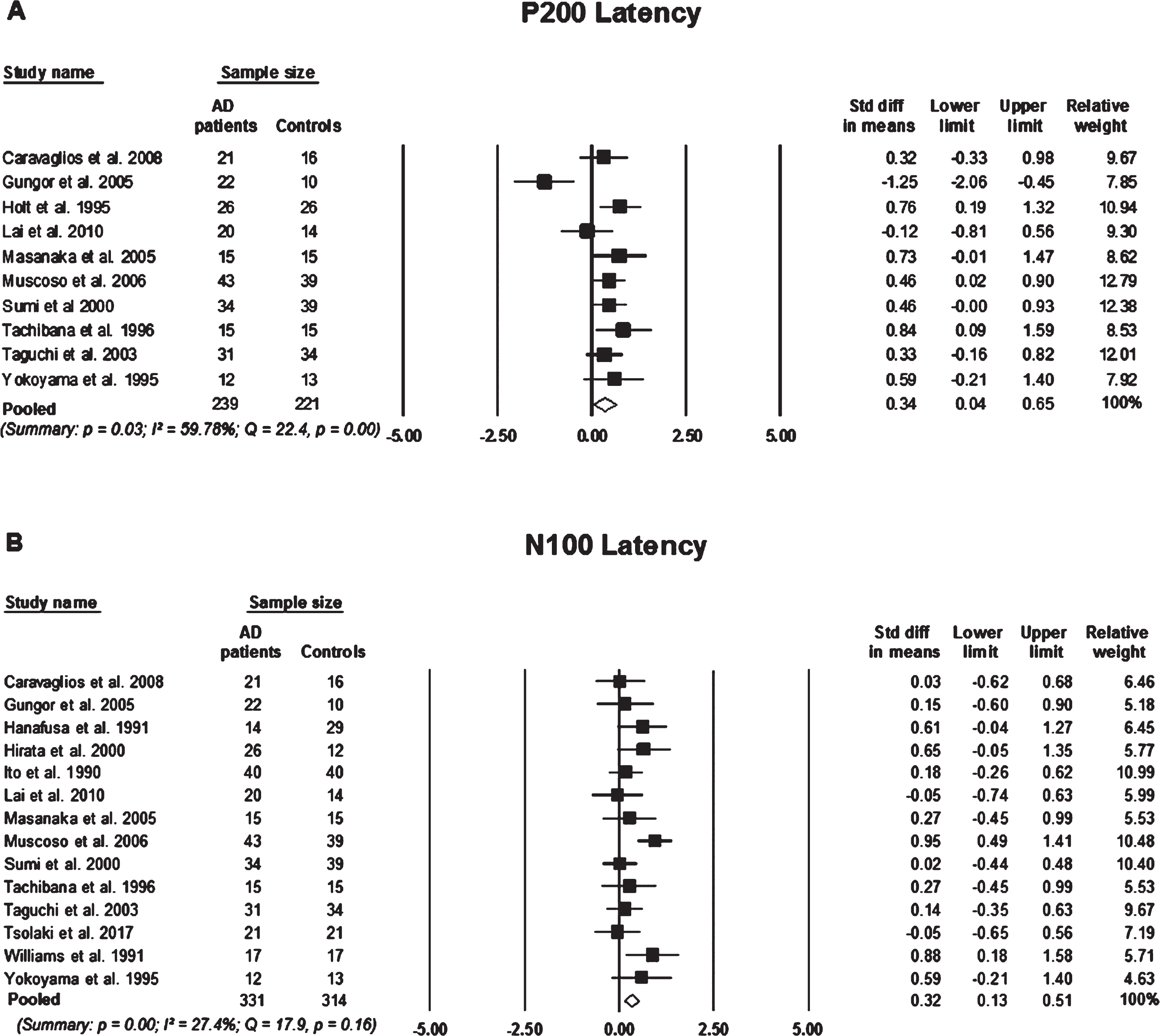
Standard mean difference and pooled estimated of each study included in the meta-analyses of P200 and N100 elicited using an active two-tone oddball paradigm. A) Comparing P200 latency between participants with Alzheimer’s disease (AD) and controls, B) comparing N100 latency between participants with AD and controls. Summary includes: p = significance level; I2 = percentage of heterogeneity; Q = Cochrane’s Q. The horizontal lines represent the 95%confidence interval for each computed standard mean difference. Note: weights are from random effects analysis.
N200
N200 latencies, elicited using an active two-tone paradigm, were significantly prolonged in AD in comparison with controls, pooled SMD: 0.73 (n = 17, 95%CI: 0.35 to 1.10, p = 0.00; Fig. 5A). However, N200 latency was not significantly different between MCI participants in comparison to controls, pooled SMD: 0.33 (n = 5, 95%CI: –0.14 to 0.81, p = 0.17; Fig. 5B). Indicating that the average AD participant would have a significantly more delayed N200 latency than over 76%of control participants. To a slightly lesser extent, a participant in the MCI group would have a longer N200 latency than over 62%of control participants. However, there was no statistically significant difference in N200 mean latencies between AD participants and MCI participants, pooled SMD: –0.17 (n = 2, 95%CI: –0.60 to 0.26, p = 0.43; Supplementary Figure 6A). There was no significant difference present in N200 amplitudes between any of the participant groups (Supplementary Figure 6B, C).
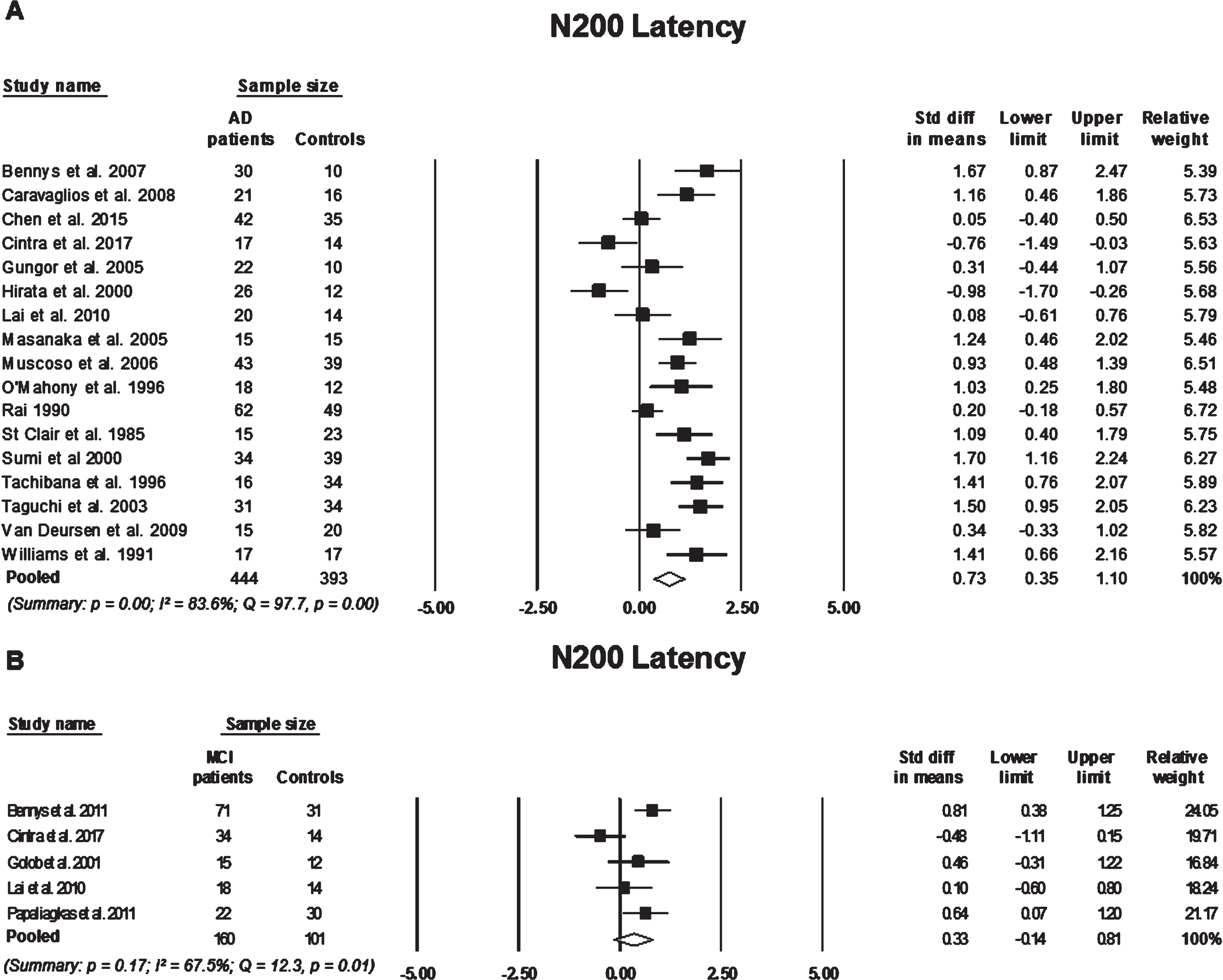
Standard mean difference and pooled estimated of each study included in the meta-analyses of N200 elicited using an active two-tone oddball paradigm. A) comparing N200 latency between participants with Alzheimer’s disease (AD) and controls, B) comparing N200 latency between participants with mild cognitive impairment (MCI) to controls. Summary includes: p = significance level; I2 = percentage of heterogeneity; Q = Cochrane’s Q. The horizontal lines represent the 95%confidence interval for each computed standard mean difference. Note: weights are from random effects analysis.
P300
Compared to controls, participants with AD had significantly prolonged P300 latencies with a large effect size (effect size > 0.8), pooled SMD: 1.08 (n = 28, 95%CI: 0.78 to 1.38, p = 0.00; Fig. 6A). MCI participants also had prolonged P300 latencies in comparison to controls with a medium effect size (effect size between 05–0.8), pooled SMD: 0.59 (n = 6, 95%CI: 0.03 to 1.14, p = 0.00; Fig. 6B), suggesting that an AD participant has a P300 latency on average 1.08 standard deviations above a control participant, which exceeds over 84%of the P300 latency measures for control participants. Similarly, P300 latencies in MCI participants are on average 0.59 standard deviations above control subjects, which exceeds over 69%of the P300 latency measures for control participants. Although the cognitively impaired groups (i.e., AD and MCI) differed significantly from the controls, their P300 latencies did not differ significantly from each other, SMD: 0.09 (n = 2, 95%CI: 0.09 to 0.52, p = 0.88; Supplementary Figure 7A). Participants with AD also showed smaller P300 amplitudes when compared to controls, SMD: –0.70 (95%CI: –0.92 to –0.48, p = 0.00; Fig. 6C). P300 amplitudes did not differ significantly when comparing MCI participants with controls and AD participants (Supplementary Figure 7B,C).
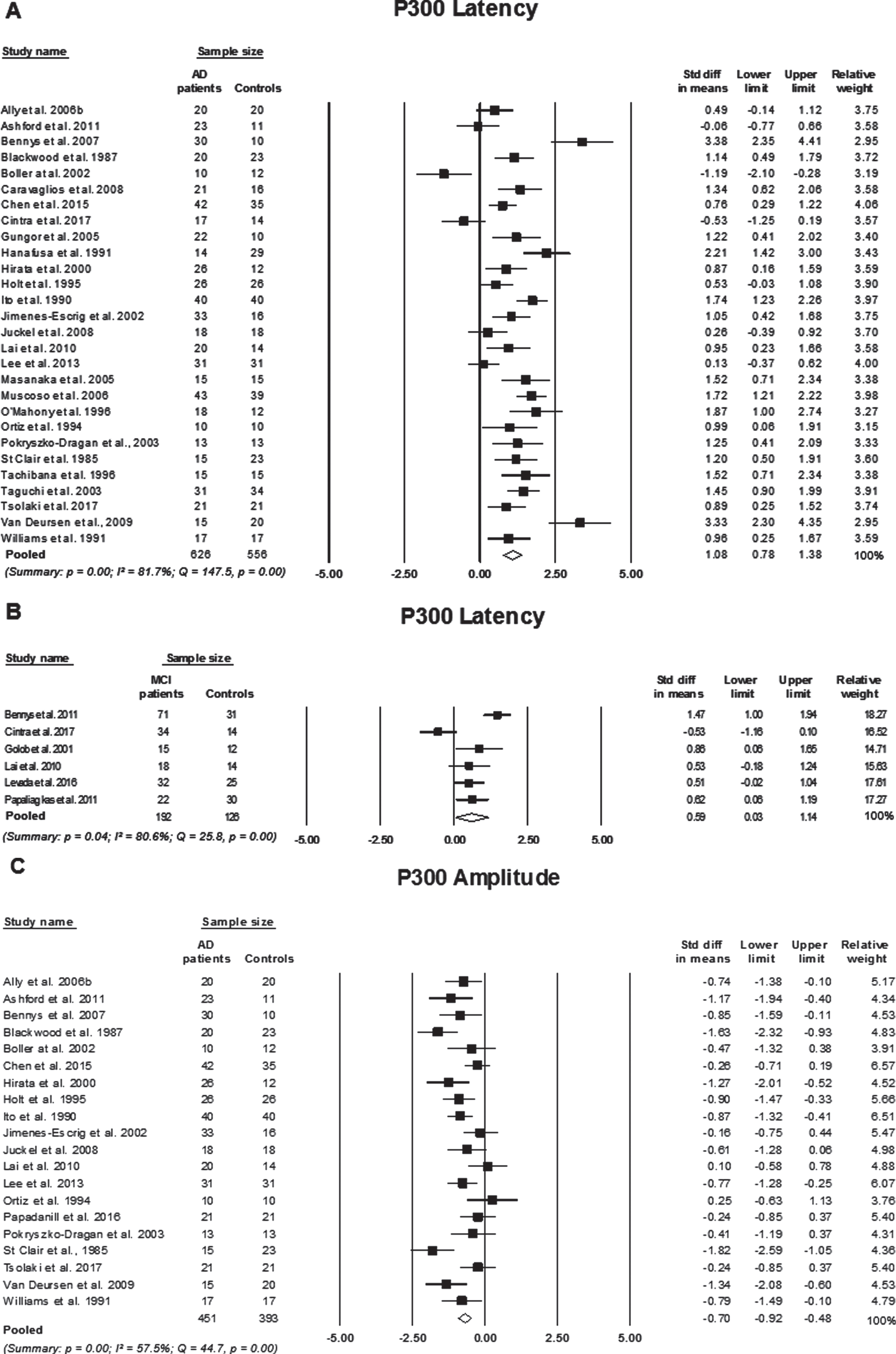
Standard mean difference and pooled estimated of each study included in the meta-analyses of P300 elicited using an active two-tone oddball paradigm. A) comparing P300 latency between participants with Alzheimer’s disease (AD) and controls, B) comparing P300 latency between participants with mild cognitive impairment (MCI) to controls, and C) comparing P300 amplitude between participants with AD to controls. Summary includes: p = significance level; I2 = percentage of heterogeneity; Q = Cochrane’s Q. The horizontal lines represent the 95%confidence interval for each computed standard mean difference. Note: weights are from random effects analysis.
Heterogeneity
The percentage of variation across studies (I2 statistic) due to heterogeneity as well as Cohran’s Q-value and level of significance are presented on each fort plot for each meta-analysis (refer to Figs. 2–6 and Supplementary Figure 1–7). I2 less than or equal to 25%is considered low heterogeneity, I2 between 26–50%is considered moderate heterogeneity and substantial heterogeneity is I2 = 75%or greater [42]. Higher percentage of variation (I2) across studies is indicative of greater variation in study outcomes and/or between study variations in clinical heterogeneity, that is, differences between participant characteristics, timing of outcome measures and characteristics of the intervention [52]. Despite efforts to reduce clinical heterogeneity using a strict inclusion criteria and only pooling studies with similar designs, there was still significant heterogeneity across studies on; P300 latency (I2 > 80%, p < 0.01), P300 amplitude comparing AD to controls only (I2 = 57.5%, p = 0.00), N200 latency (I2 > 64%, p < 0.05), N200 amplitude comparing MCI to controls only (I2 = 85%, p = 0.00), P200 latency comparing AD to controls only (I2 = 59.8%, p = 0.00), N100 amplitude comparing AD and MCI to controls (I2 = 90.5%and 93.9%, p = 0.00, respectively), P50 amplitude elicited using rarefaction clicks (I2 = 91.6%, p = 0.00), and studies on ABR measuring interpeak wave III-V (I2 = 67.1%, p = 0.02). Controlling for factors such as the severity and duration of the disease, could reduce between study heterogeneity, however, this can be difficult to achieve as a limited number of studies report or measure for these factors. As higher heterogeneity dilutes confidence in the pooled effect, it is therefore important to take this into account when interpreting the final outcomes. It is also noteworthy that all other between study heterogeneity analyses were insignificant.
Methodological quality assessment
Studies included in this review were assessed based on their methodological quality using a quantitative quality assessment tool (EPHPP, 1998). The studies were rated as either “strong”, “moderate” or “weak” based on the overall outcomes of the eight core components of the EPHPP instrument. These components are: 1) selection bias, 2) study design, 3) confounders, 4) blinding, 5) data collection methods, 6) withdraws and dropout, 7) intervention integrity, and 8) analysis, refer to Table 2. A majority of the included studies were rated as “moderate” (n = 47, 63.5%), 5/74 (6.7%) studies were rated as “strong” and 22/74 (29.7%) were rated as “weak”. None of the included studies were described as a randomized trial, however, the “strong” studies (n = 5) indicated blinding in the study design. One study had a double-blind study design [52], and 4 studies were a single blind [53–56]. The studies that were rated as “moderate” or “weak” did not met all the core components of the quality assessment, which is attributed to one or more of the following reasons: 1) absence of information (e.g., recruitment procedure), 2) lack of a randomized control trial study design, 3) no use of blinding, and 4) lack of clarity.
Qualitative assessment results for quantitative studies included in the review (n = 74)
Fifty-four (72.9%) studies selected participants that were “very likely” to represent the target population, while 19 studies did not clearly describe their recruitment procedure, resulting in a “weak” rating in the selection bias component of the quality assessment. Most studies (86%) controlled for confounding factors in their study design (e.g., recruitment) and/or in statistical analysis, therefore, there were no differences in age, gender ratio, and education level between study groups. All studies (n = 74; 100%) utilized valid data collection tools and appropriate statistical methods for data analysis (see Table 2). All the studies included in this systematic review were case-control studies, therefore, the level of recommendation for all individual studies was level 4 based on American Society of Plastic Surgeons’ Evidence Rating Scale for diagnostic studies [57].
DISCUSSION
This systematic review and meta-analysis aimed to investigate whether AERPs differ in amplitude and/or latency between participants with cognitive impairment (MCI and AD) or subjective cognitive decline (SCD) to age-matched controls based on the analysis of currently available literature. Some AERPs (i.e., ASSR, FFR P30, N400, and slow wave) were not meta-analyzed as there was only a limited number of studies with similar designs reporting their findings, however, the majority of the AERPs were meta-analyzed (ABR, MMN, P50, N100, P200, N200, and P300). Findings from this investigation suggest that the AERPs analyzed in the review (except for MMN) vary significantly, in mean latency and/or amplitude, between participants with AD and controls. No significant variation in AERP mean latencies or amplitudes between AD participants and MCI participants were observed; however, this could be due to the low number of studies comparing these two groups. Only P300 differed significantly between MCI participants and controls based on the pooled analysis, but again this could be attributed to the low number of studies with similar designs investigating AERPs in MCI participants. Notably, due to the lack of studies investigating AERPs in SCD in comparison to non-SCD participants, a meta-analysis on this group could not be performed.
Auditory event-related potentials and cognitive decline
Although there are conflicting reports regarding ABRs in participants with AD, this meta-analysis suggests that there are significant delays in the appearance of ABR wave V, interpeak I-V wave and interpeak I-III wave in patients with AD in comparison to controls. There are multiple neural generators of ABRs which are sequentially activated throughout the brainstem auditory pathway. Therefore, ABRs have been frequently used to evaluate the function and integrity of the central and peripheral auditory pathway [35]. The findings of this meta-analysis are consistent with suggestions of brainstem and midbrain structure abnormalities in people with AD [58, 59]. Variations in disease severity and duration have been proposed as explanations for conflicting results across ABR studies [43], but nevertheless pooled analysis of the studies is supportive of significant abnormalities in ABRs in AD participants when compared to controls.
MMN has been proposed to reveal deficits in echoic memory storage and automatic mismatch detection essential for attention [60]. An impaired MMN response in AD participants suggests difficulty in automatic information processing that is required for sensorial storage [61]. However, in this meta-analysis no significant difference was observed between AD participants and controls. It should, however, be noted that only three studies were included in the pooled analysis of standard mean differences of MMN amplitude between AD participants and controls, meaning that these results should be interpreted with caution. Individually, two studies suggest that MMN is significantly impaired in participants with AD in comparison to healthy controls [42, 61], while one study report no difference in MMN measures between the two groups [52]. There is evidence that suggests that MMN latency is significantly longer in MCI participants in comparison to controls, again, indicating that automated auditory information processing is impaired at this stage of cognitive decline [62]. Some, non-AD related, studies have suggested that reduced MMN amplitude could be used as an index for cognitive decline, as it correlates with increased severity of negative symptoms (including, attention difficulties, memory problems, social withdrawal, and apathy) [63–65]. However, limited research has compared MMN measures at different stages of AD, making it difficult to establish if MMN can be applied to staging cognitive decline associated with AD.
The meta-analyses of late latency (P50, N100, P200, N200, and P300) AERPs indicate that these components are significantly abnormal in AD participants when compared to controls. Pooled analysis of the studies suggests that using an active two-tone oddball paradigm AD participants can be differentiated from controls due to significant delays in N100, P200, N200, and P300 latencies. The strength of the response was not significantly affected by the presence of AD in any of the AERPs except for P300 amplitude, which was significantly smaller in AD participants compared to controls when elicited using an active oddball task. Inter-subject variability in amplitude may have led to inconsistent findings within each study as well as in the pooled analysis. Abnormalities in these AERPs in people with cognitive decline have been linked to their proposed roles in cognitive processes such as attention, memory and executive functions [66–69].
A small number of studies have investigated P50 amplitude and latency differences between AD participants and controls. Pooled analysis indicates that P50 amplitude and latency differ significantly between the groups. Variations in the pooled analysis of P50 measures between AD participants and controls were only observed when P50 was elicited using a paired-click paradigm, which is thought to reflect sensory gating. This is supportive of the hypothesis that P50 may be an index of attention and inhibitory processing, which is altered due to progressive cognitive decline observed in AD [53, 70].
Both N100 and P200 have been suggested to be generated by the primary and secondary auditory cortex, therefore, these AERP components are thought to reflect the higher processing of sensory information [71, 72]. Although previous studies reported that N100 and P200 components do not discriminate between healthy aging and AD [70, 73–75], pooled analysis suggests that latency measures of these components may differentiate normal controls from people with AD. This contradicts previous assumptions that people with AD may not have measurable impairments in perceiving and processing changes in an auditory stimulus [76].
Multiple neural regions have been implicated in the generation of the N200 response, these include the brainstem, thalamic region, and the auditory cortex [77, 78]. The N200 peak is suggested to reflect the discrimination, perception, and classification of auditory information [79]. Results from this analysis imply that AD participants have impaired central auditory processing as reflected by longer N200 latency when compared to controls. Behavioral studies have also shown that AD and MCI participants have impaired central auditory processing. Reduced performance in the Synthetic Sentence Identification-Ipsilateral Competing Message (SSI-ICM) task, which is used to test central auditory function, has been seen in participants with MCI and AD [27, 80]. There has also been a strong association between SSI-ICM performance and cortical thickness of the primary auditory cortex [81], further supporting that association between cortical degeneration and impaired auditory processing seen in cognitively impaired participants. A previous meta-analysis on N200 latency in participants with AD and MCI reported significant standard mean differences between AD and MCI subjects when compared to controls, but not when compared to one another [82]. However, in this study pooled analysis of N200 latency did not indicate that this AERP can differentiate between MCI and healthy aging, or between MCI and AD participants.
The neural generators of the P300 response are thought to include: the frontal lobe, temporal-parietal junction, medical temporal lobe, posterior cingulate gyrus, and the parietal cortex [83–85]. Regions that are known to be involved in sensory processing, memory storage, cognitive function, and executive functions. It is therefore suggested that P300 reflects cortical activity as it relies on functions such as memory, attention, and discrimination to be elicited. AD participants’ exhibit increased P300 latency, which is an indication of diminished classification speed in processing tasks and dysfunctional attention-driven discrimination processing, which is suggested to evaluate the representation of previous events in working memory [86, 87]. Additionally, P300 amplitude has been proposed to be an index of the amount of cognitive resources allocated by a participant to a cognitive process or task [88]. Pooled analysis suggests that AD participants have reduced P300 amplitude, which in turn reflects altered cognitive resource allocation to an attention-driven discrimination task.
P300 latency abnormalities in MCI participants are relatively similar to that of AD participants, which is further supported by the insignificant standard mean difference in the analysis comparing these components in participants with AD and MCI. Similar to the findings of this meta-analysis, a previous meta-analysis reported that P300 latency did not differ significantly between MCI and AD participants [89]. Interestingly, however, a longitudinal study evaluating patients at risk of developing AD, found that MCI participants that progressed to probable AD after a 5-year follow-up, had longer P300 latency at baseline when compared to MCI participants that did not progress to AD [90]. This in turn implies that latency measures of some AERPs may provide an avenue in discriminating between those at higher risk of AD from healthy individuals.
Study limitations
For the analysis of some AERPs, such as MMN, P50 and ABR, and the analysis of MCI studies, the low number of studies with similar methodological design investigating these AERPs poses as the strongest limitation. Meta-analysis studies are unable to overcome the limitations presented in individual studies, therefore, more data would be required to make final conclusions. Slight variations in diagnostic criteria used within the studies in combination with differences in factors such as gender ratio, MMSE scores, and testing paradigm modality may affect heterogeneity between the studies and the significance of the effect size.
Conclusions and gaps in knowledge
The findings of this review indicate that some AERP measures may be valuable biomarkers of AD. In conjunction with currently available clinical and neuropsychological assessments, AERPs may aid in detecting cognitive impairment associated with AD. The use of AERPs for measuring differences between AD patients and healthy older adults show great promise, particularly the use of P50, N100, P200, N200, and P300 latency measures. P300 also shows promise in differentiating between MCI patients and healthy age matched controls, which could aid in early detection of individuals at prodromal stages of AD. However, based on the pooled analysis, none of the AERPs showed significant sensitivity in differentiating between AD and MCI patients. These findings suggest that although AERPs have inadequate sensitivity for staging cognitive decline or differentiating between AD and MCI, they have adequate specificity to discriminate between those with cognitive impairment from healthy older adults. Also, this review highlights the need for research on AERPs in participants with SCD. AERPs were not analyzed for the SCD group as there were no studies on this group. Two studies were identified outside this review to have investigated AERPs in a group with subjective memory complaints or cognitive decline [91, 92]. However, both studies lacked a control group of individuals without SCD, therefore the AERP measures reported would not indicate differences between these participants and non-SCDs. Investigating AERPs in SCD participants could provide more information on the possible application of these measures in identifying cognitive impairment at earlier stages prior to the appearance of cognitive decline on neuropsychological assessments. In addition, there are a limited number of studies that investigate certain AERP components, such as ASSR, FFR, N400, and P600, which again highlights the need for more research in order to fully elucidate the usefulness and effectiveness of AERP measures as a biomarker of cognitive decline associated with AD.
DISCLOSURE STATEMENT
Authors’ disclosures available online (https://www.j-alz.com/manuscript-disclosures/21-0556r1).