
Abstract
BACKGROUND:
Lifting heavy objects can induce postural stress and low back pain.
OBJECTIVE:
This study aimed to examine the effect of object weight expectations on trunk muscle activity and assess trunk muscle activity in people with chronic low back pain.
METHODS:
Twenty-two male college students (11 healthy and 11 participants with chronic low back pain) were recruited. The procedure was performed in three settings: lifting an expected 5-kg object, lifting an unexpected 10-kg object, and lifting an expected 10-kg object. Lifting was divided into five phases, and the muscle activity in each phase was compared between groups (chronic low back pain/control), object weight predictions, and phases.
RESULTS:
Compared to the control group, the chronic low back pain group had higher erector spinae muscle activity, regardless of weight or prediction, and significantly higher rectus femoris muscle activity in the early lifting phase of the expected 10-kg object (
CONCLUSIONS:
Healthy individuals and individuals with chronic low back pain had different recruitment strategies for lifting objects heavier than predicted.
Introduction
Low back pain (LBP) is highly prevalent regardless of age [1] and causes a reduction in daily activities and work ability [2]. More specifically, LBP persisting for more than 3 months requires a long recovery time and is defined as chronic LBP (CLBP) [3]. Lifting is one of the many factors that induce LBP [4], and a higher frequency of LBP has been reported in individuals who lift and carry heavy loads at work [5]. For example, frequently lifting and carrying a low-load mass with a forward-bent back doubled the risk of developing chronic LBP among healthcare workers [6].
Trunk muscle activity is essential for controlling trunk stability [7] and lifting. Moreover, lifting tasks require trunk flexion and extension, which can overload the lower back and erector spinae (ES) muscles. Accordingly, trunk muscle activity during lifting has been investigated to clarify the mechanism of lifting-induced LBP.
Lifting-induced LBP may be related to object weight prediction [8, 9], and differences in trunk muscle activity with and without weight prediction have been investigated. Studies on healthy men have shown that back muscle activity increases when lifting without weight prediction compared with when weight is predicted, leading to LBP [8, 9]. For example, lifting without predicting the weight of an object increases muscle activity in the ES [8]. Furthermore, lifting a heavier-than-expected object produces eccentric contraction of the trunk extensors early in the lifting phase [10] and an overload of the back muscles. Moreover, the activity of the back muscles is higher in the latter half of the lifting motion [9].
A comparison of normal subjects and those with a history of low back pain has shown that the EMG amplitude of the ES during lifting is higher in those with two or more episodes of LBP than in normal subjects [11], suggesting that the ES muscles may be involved in LBP during lifting. However, it is unclear whether trunk muscle activity differs between individuals with chronic low back pain (CLBP) and healthy subjects when holding a heavier-than-expected object. Understanding the differences in muscle activity between these two groups may reveal the mechanisms underlying trunk muscle dysfunction in individuals with LBP. Therefore, this study aimed to examine whether the trunk muscle activity of subjects with CLBP differs from that of healthy subjects when holding a heavier-than-expected object.
Methods
Participants
A total of 22 male college students (age, 20.5
Experimental task
Experimental procedure
Experimental procedure
Participants were asked to lift boxes of different weights (5 and 10 kg) from a platform; the weights were based on previous studies [11, 14]. Each box was made of plastic, had a black body with a green lid, and was 29.5 cm
Muscle activity was measured using a wireless surface EMG system (DELSYS Trigno Wireless EMG System; DELSYS, Natick, MA, USA) that had a sampling frequency of 2000 Hz. The activity of the right-sided muscles was measured. The skin was rubbed with alcohol to reduce skin impedance, and the surface electrodes were positioned on the rectus abdominis (RA), internal oblique (IO), external oblique (EO), ES, gluteus maximus (GMa), rectus femoris (RF), biceps femoris (BF), and biceps brachii (BB) based on previous studies [15, 16, 17, 18]. Surface electrodes were attached parallel to the muscle fibers. A digital video camera (Exilim EX-FH20; Casio Computer Co., Ltd., Tokyo, Japan) was set up perpendicular to the plane of motion 3 m to the right of the platform, and recordings were made at a frequency of 210 Hz. To obtain kinematic data, reflective markers (QPM190, Qualisys AB, Gothenburg, Sweden) were attached to the right side of the object, right acromion, and middle fingertip. The digital video camera was synchronized with the electromyography (EMG) system.
Experimental procedure
To normalize EMG data, maximum voluntary contraction (MVC) was performed for each muscle, and each participant practiced each MVC to learn the position and measurement methods prior to the MVC test. Manual resistance was applied until the participants achieved maximum effort. Participants performed maximum isometric contractions for 3 s. The MVC for the RA was measured in a supine position using a partial sit-up with the knees flexed at 90
Lifting practice was conducted after the MVC test (Table 1). To get familiarized with a 5 kg weight, the participants lifted a 5-kg object for 5 times. After the weight was recognized, the “lifting of the expected 5-kg object” task was performed. Subsequently, participants were told that the electrodes and markers needed to be checked for misalignment and were led behind a partition. The 5-kg object was replaced with a 10-kg one, which went unnoticed by all participants. This was termed as the “lifting the unexpected 10-kg object” task. Although the participants recognized the object as a 5 kg one, its true weight was 10 kg. Finally, to recognize a 10 kg weight, the participants lifted a 10-kg object for 5 times. Following this, the “lifting of the expected 10-kg object” task was performed.
Participants were guided throughout the lifting task using a metronome (ME110SBL; Yamaha Corporation, Shizuoka, Japan); throughout 2-s intervals, participants started lifting from a static standing position and touched the object; the object was lifted until the trunk was upright; the object was returned to the platform; and, finally, the participant returned to a static standing position.
Data analysis
Phases of lifting. Lifting was divided into the following five phases: preparation, early lifting, middle lifting, late lifting, and recovery.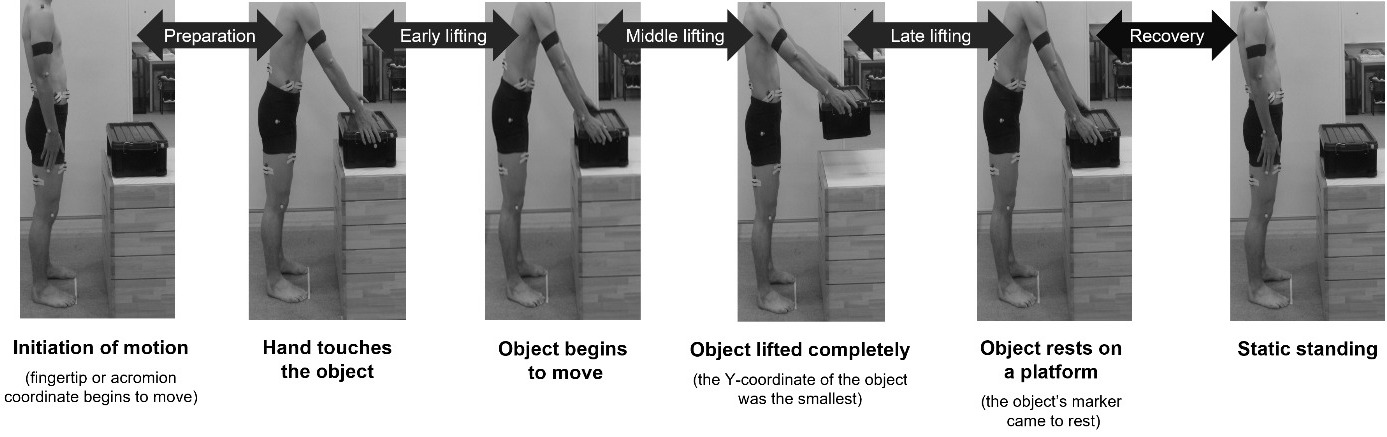
Data analysis software (ImageJ; National Institutes of Health, Bethesda, MD, USA) was used to divide the data into the following five phases: preparation, early lifting, middle lifting, late lifting, and recovery (Fig. 1). The interval between motion initiation and touching the object by hand was defined as the preparation phase. The interval between touching the object by hand and the initiation of the object’s marker coordinate movement was defined as the early lifting phase. The interval between the time of initial movement of the object’s marker coordinate and the point at which the object was completely lifted was defined as the middle lifting phase. The interval between the point of times when the object was completely lifted and when the object was rested on a platform was defined as the late lifting phase. The interval between the point of times when the object was rested on a platform and the end of lifting procedure was defined as the recovery phase.
The raw EMG data were bandpass-filtered between 20 and 450 Hz and full-wave-rectified using an analysis software (LabChart 8; AD Instruments, New Zealand). The root mean square (RMS) during the MVC test was calculated by identifying the compartment with the maximum amplitude in 1 s. The RMS during each phase was normalized as a percentage of the highest RMS obtained during a 1s period in the MVC test (%MVC).
Statistical analyses were performed using SPSS version 28.0 (IBM Corp.; Armonk, NY, USA). Height, weight, and age were compared between both groups. We conducted the Kolmogorov-Smirnov test to confirm the normality of the data. Nonparametric tests were used to assess age. Each muscle activity was analyzed using a three-way repeated measures analysis of variance (ANOVA) (GROUP [control/CLBP]
Results
Characteristics of the chronic low back pain group and control group
Characteristics of the chronic low back pain group and control group
Group characteristics are expressed as the mean
There were no significant differences in age, height, weight, and body mass index between both groups (Table 2). In the CLBP group, the VAS score at the time of the experiment was 2.2
Erector Spinae and Rectus Femoris muscle activity in each group with and without weight prediction
Muscle activity data are expressed as the mean
Comparison of muscle activity with and without low back pain. Mean and standard deviation for the electromyographic activity of the erector spinae (a, expected 5 kg; b, unexpected 10 kg; c, expected 10 kg) and rectus femoris (d, expected 10 kg). 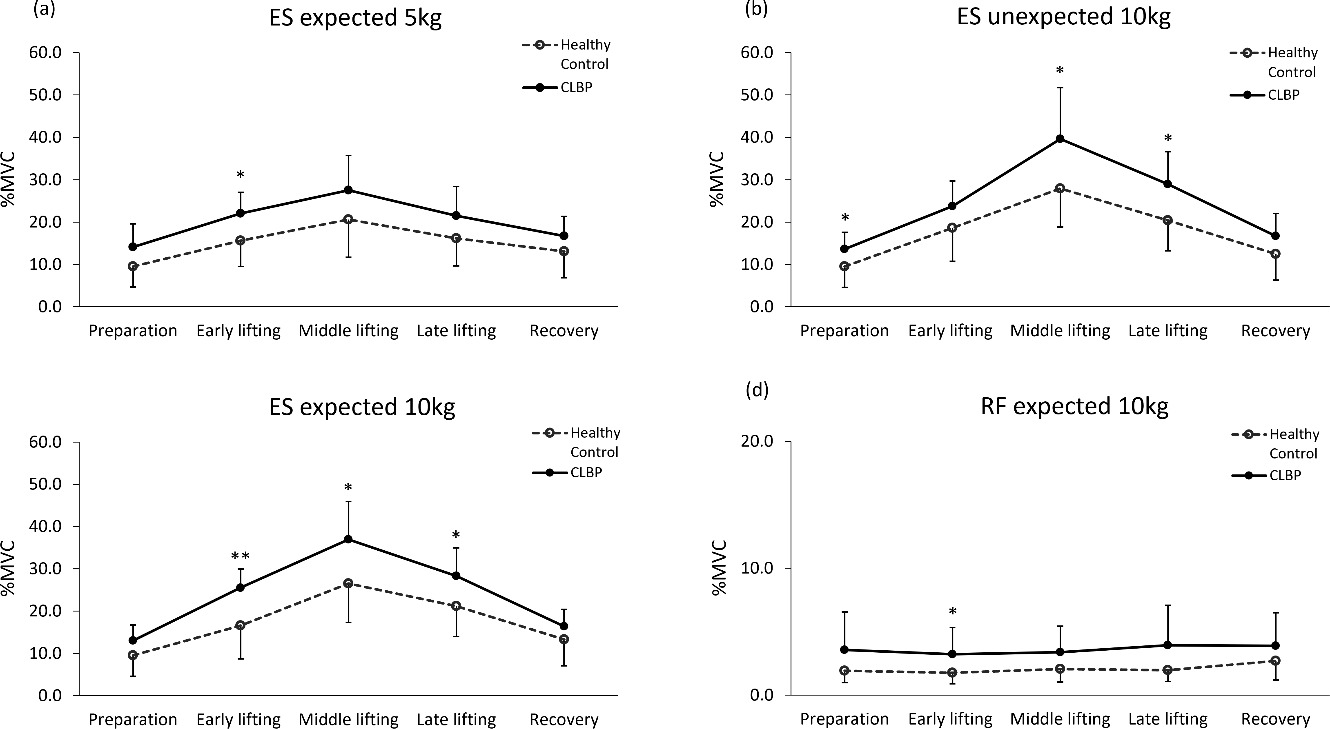
Comparison of muscle activity with and without weight prediction. Mean and standard deviation for the electromyographic activity of the (a) erector spinae, (b) rectus femoris, (c) biceps femoris, and (d) biceps brachii muscles. 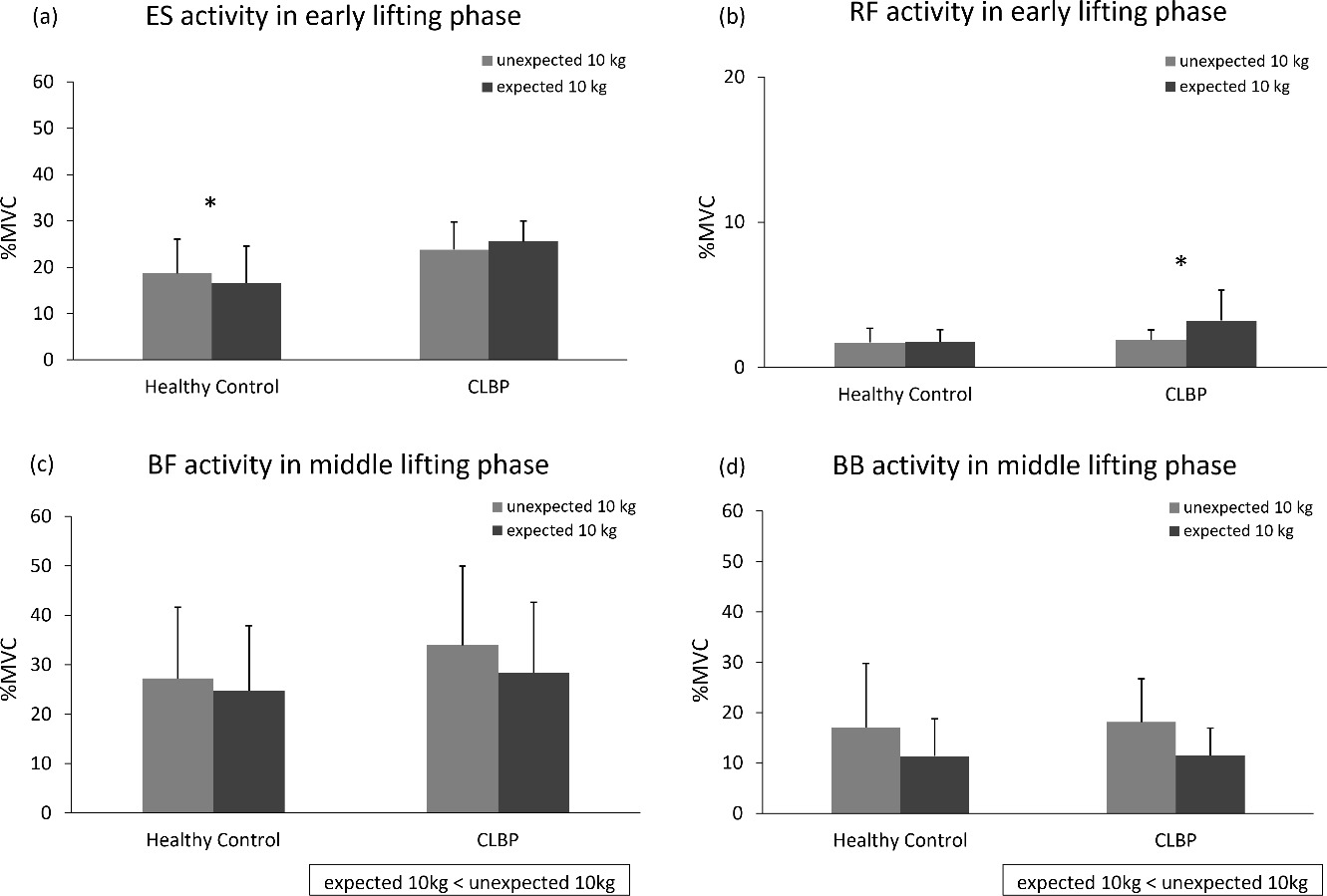
EMG data are expressed as %MVC. Three-way repeated measure ANOVA revealed a significant three-way interaction for the ES muscle (
Three-way repeated measure ANOVA revealed a significant three-way interaction for the RF muscle (
Three-way repeated measure ANOVA showed no three-way interaction but a significant two-way interaction of TRIAL
Three-way repeated measure ANOVA showed no three-way interaction but a significant two-way interaction of TRIAL
This study investigated muscle activity during 3 different lifting tests. The control and CLBP groups differed in their recruitment patterns when lifting objects heavier than expected.
The ES muscle activity was higher in the CLBP group than in the control group during lifting, regardless of the weight or prediction. It has been reported that repetitive lifting induces measurable fatigue in the ES muscles [19]. Thus, it can be hypothesized that muscle fatigue and overloading may occur during repeated lifting.
RF muscle activity was also higher in the CLBP group than in the control group during the early lifting phase (i.e., the interval between the participant’s hand touching the object and the object beginning to move) of the expected 10-kg object lifting task. There was no difference in ES and RF muscle activity between both groups during the early lifting phase of the unexpected 10-kg object lifting task. These findings indicate that, when lifting an object of predictable weight, the CLBP group prepared for the lifting task by increasing ES and RF muscle activity before the object moved. However, these strategies were not applied when lifting an object heavier than expected. A previous study reported that vastus lateralis muscle activity was higher in healthy individuals than in patients with CLBP when lifting an object from the ground with both hands [14]. However, RF muscle activity was higher in the CLBP group than in the control group in the present study. Perhaps, the differences in quadricep muscle activation between both studies is owing to differences in height when lifting from the floor or from a platform [14]. In the current study, participants were instructed to maintain knee extension during lifting. Compared to the control group, the CLBP group demonstrated increased RF activity and knee extension immobilization, indicating that compensation for the trunk muscle dysfunction may have occurred.
This study focused on differences in muscle activity with and without prediction. In the control group, ES muscle activity during the early lifting phase was higher when lifting the unexpected 10-kg object than when lifting the expected 10-kg object. There was no difference in muscle activity between groups, but BB and BF activity were higher when lifting the unexpected 10-kg object than when lifting the expected 10-kg object. Thus, when lifting an object that was heavier than expected, BB and BF activity increased regardless of the group, whereas, in the control group, ES activity increased before the object was moved. In previous studies using healthy participants, ES muscle activity was higher when the weight of an object was unexpected than when it was expected [8, 20]. Similarly, when participants could not predict the object’s weight, ES activity increased only in the control group in the present study. Muscle activity was also previously measured in healthy participants during unilateral upper limb raising, and ipsilateral ES and BF muscle activation was found to precede the deltoid muscle before the upper limb moved [21]. Accordingly, ES and BF may function as postural control muscles. Moreover, delayed ES feedforward has been reported in patients with lumbar spine instability [22]. Given the results of this study, healthy participants could use strategies to recruit the ES muscle earlier and control posture when lifting objects that are heavier than expected. In contrast, it was suggested that the ES muscle does not control posture before object movement in the CLBP group.
Overall, this study showed that the CLBP group had higher ES muscle activity than the control group, regardless of an object’s weight or predicted weight. Individuals with CLBP were unable to recruit their trunk muscles appropriately when lifting objects that were heavier than predicted, suggesting trunk muscle dysfunction. This may lead to worsening or prolongation of LBP, but it was not investigated in this study and requires further research.
This study had several limitations. First, the sample size was small. In this study, it was difficult to recruit large number of individuals with CLBP. Further studies with more participants will be needed in the future. Each participant’s motion during lifting was not analyzed. Although the participant’s movements were standardized in this study, differences in motion caused by the presence or absence of predictions may have occurred. In future studies, it would be worth considering the participant’s motion, as well as trunk muscle EMG. Moreover, although this study was conducted with specific weights (5 and 10 kg), the type of object weight is not specified in actual situations. Therefore, it is necessary to increase the variation in object weights in further studies.
In conclusion, the CLBP group had significantly higher ES muscle activity during lifting than the control group. When lifting an object that was heavier than expected, BB and BF activity increased regardless of LBP. Moreover, ES activity also increased before the object was moved, but only in the control group. These findings suggest that healthy individuals and individuals with CLBP had different muscle recruitments for lifting objects heavier than predicted.
Author contributions
CONCEPTION: C.S. and M.E.
PERFORMANCE OF WORK: C.S., H.H., K.S.
INTERPRETATION OR ANALYSIS OF DATA: C.S., H.H. and M.E.
PREPARATION OF THE MANUSCRIPT: C.S., H.H., R.H., H.Y., K.S., T.T. and M.E.
REVISION FOR IMPORTANT INTELLECTUAL CONTENT: C.S., H.H., R.H., H.Y., K.S., T.T. and M.E.
SUPERVISION: C.S. and M.E.
Ethical considerations
All participants were informed of the study’s aims and procedures before participation, and written informed consent for participation was obtained from all participants. The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Review Committee of the authors’ affiliated institutions (Approval number: 18581-210218, Approval date: 2/18/2021).
Funding
This study was supported by a Grant-in-Aid program from Niigata University of Health and Welfare.
Footnotes
Acknowledgments
Not applicable.
Conflict of interest
The authors declare that they have no competing interests.