
Abstract
BACKGROUND:
Interstitial lung disease is characterized by exertion dyspnea, exercise limitation and reduced quality of life. The role of exercise training in this diverse patient group is unclear. The growth differentiation factor 15 (GDF15) is a stress-sensitive circulating factor that regulates systemic energy balance and could be a possible biomarker in interstitial lung disease.
OBJECTIVE:
To evaluate the effect of supervised exercise (endurance and resistance) training (SET) on exercise capacity, pulmonary function parameters and GDF15 levels in patients with interstitial lung disease (PwILD).
METHODS:
In this non-randomized case-control trial, the experimental group comprised of 10 PwILD (7 women and 3 men) while the control group consisted of of 18 apparently healthy participants s 11 women and 7 men). All subjects completed an 8-week supervised exercise training program, at a rate of twice a week. Dyspnea was evaluated using the Shortness of Breath Respiratory Questionnaire. Exercise capacity was measured using the 6-min walk test while the heart rate (HR) was monitored before and after the exercise training. GDF15 levels were measured by Enzyme-Linked Immunosorbent Assay (ELISA).
RESULTS:
PwILD had significantly shorter 6-min walk distance than the control subjects at both the 1
CONCLUSION:
Supervised exercise training did not affect GDF15 levels in both patient and control groups but its values in PwILD were significantly higher compared to those of controls (
Keywords
Introduction
Physical exercise improves the quality of life and decreases the risk of several diseases [1]. Exercise training is an essential constituent of evidence based management programs for many chronic cardiac and respiratory conditions. Interstitial lung disease (ILD) is a group of disabling chronic lung conditions consisting of more than 200 different disease entities [2]. They are normally associated with interstitial inflammation, [3] and fibrosis. Stressful dyspnea, insightful exhaustion and reduced exercise tolerance are common [4] with subsequent decline in health associated quality of life. Therapeutic choices are often restricted and patients go through cumulative exercise control as their condition advances. There are few well described studies reported on the importance of exercise training in interstitial lung disease (ILD) [5]. The respiratory imbalance noticed in ILD patients is more apparent during exercise. Pathophysiological mechanisms responsible for exertional dyspnea and reduced exercise tolearnce include changed respiratory mechanics, compromised gas exchange, cardiovascular abnormalities and peripheral muscle dysfunction [6].
Exercise training rules in chronic respiratory diseases are same as defined for healthy individuals, including personalized exercise recommendation and evolution of training load [7]. There is a significant indication that a minimum of 8 weeks of exercise training bring considerable improvement in exercise tolerance and clinically important changes in exercise capacity and quality of life [8]. Physical exercise is potentially useful as a treatment for subjects with ILD, [9] with advancements in six-minute walk distance (6MWD), dyspnea, and exercise capacity [5].
Several studies reported positive results of exercise training on fortitude and quality of life [10]. However, very few explored the effect of exercise training on exercise capacity and pulmonary function in patients with ILD [11, 12, 13, 14]. Recently our group assessed [15] the impact of supervised exercise training (SET) on pulmonary function Parameters, exercise capacity and Irisin biomarker in ILD patients.
Growth differentiation factor 15 is a distant member of the transforming growth factor-
The biological effects of GDF-15 are condition based and may differ with the phase of the disease [22]. GDF-15 concentrations increase with age in healthy old aged subjects [23]. The circulating levels of GDF-15 are increased in acute pulmonary embolism [24] and in idiopathic pulmonary arterial hypertension provide predictive information about the long-term risk of death or lung transplantation [25].
Growth differentiation factor 15 contributes to the loss of muscle in COPD which elevated levels of this cytokine translate into reduced exercise ability in subjects with COPD. Labaki et al. [26] examined the link between GDF-15 levels and 6MWD and assumed that higher GDF-15 levels are associated with lower six minutes walking distance (6MWD). Yazisiz et al. [27] defined the function of GDF-15 in the development of pulmonary fibrosis and reported serum GDF-15 levels in ILD patients with connective tissue disorders (CTD) and CTD without ILD which were significantly higher than healthy controls. Raised serum GDF-15 level was found [28] to estimate an adverse result individually in subjects with COPD exacerbation, proposing the probability that serum GDF-15 could be used as a predictive biomarker of COPD exacerbation.
We hypothesized that GDF-15 could play a pathogenic role in interstitial inflammation in patients with ILD (PwILD). These findings have directed us to explore biological markers that may permit prior discovery of ILD. Since plasma levels of GDF-15 in patients with ILD have never been reported previously, the main object of present study was to discover a possible role for GDF-15 in patients with ILD before and after exercise training and also to evaluate the impact of SET on pulmonary function and exercise capacity in ILD patients.
Method
Participants
Interstitial Lung Disease patients (
Study design
This is a non-randomized case control interventional study (single-arm clinical trial (SACT).
Distribution of medical diagnosis for patients who participated in the study.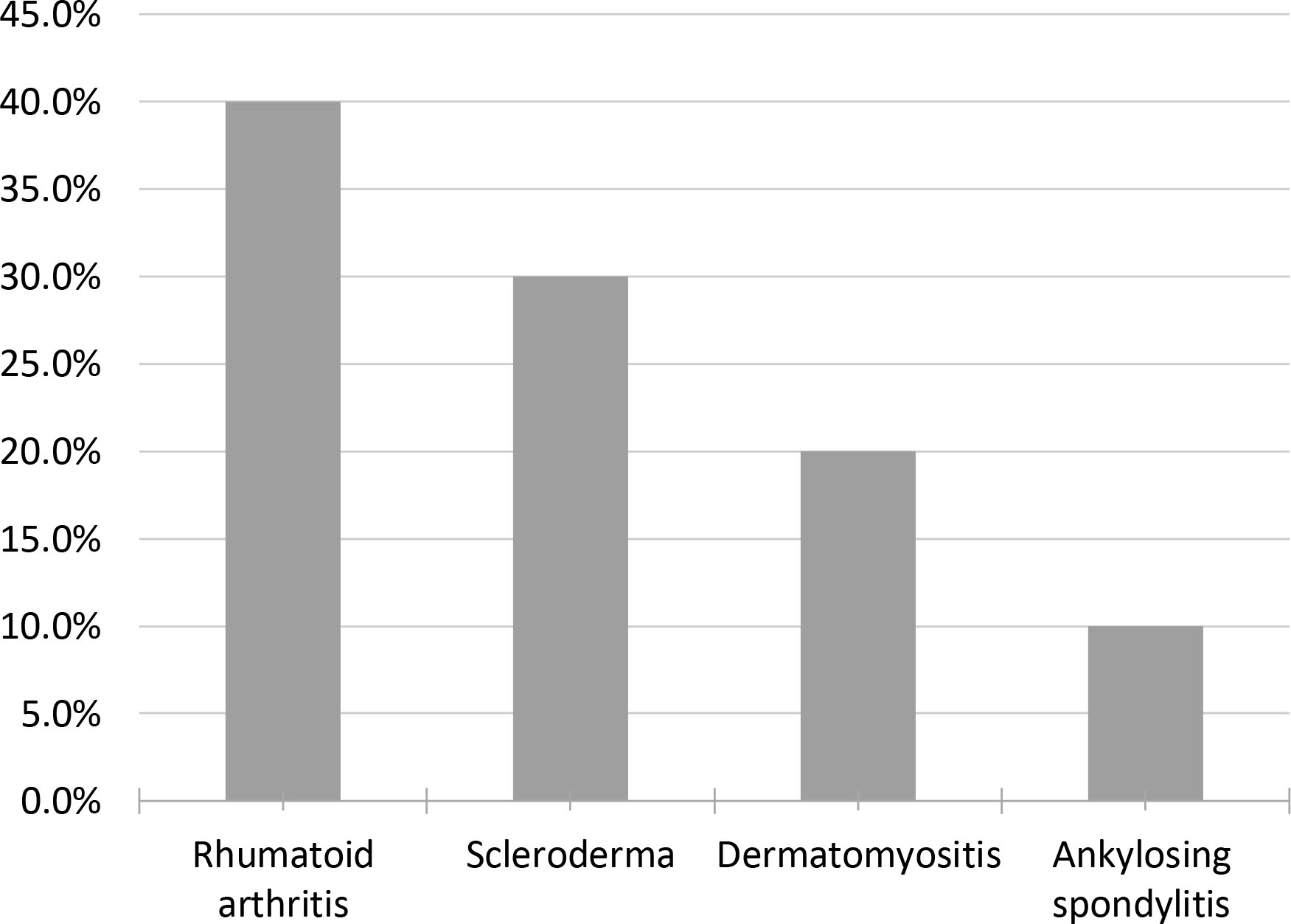
The inclusion criteria for SET program in ILD has been broad and participants have had a wide range of ILD diagnoses (Fig. 1). The patients with stable condition, non-smokers, having dyspnea on exertion, on medical treatment and not involved in any exercise program in the last 12 months were included. All participants were free from any serious risk of exercise training according to the guidelines of ACC/AHA for exercise testing [29]. The control subjects were medically free, non-smokers and their pulmonary function tests were normal. Patients with ILD with long term Oxygen (O
Study protocol
Both patients and healthy subjects received the same exercise training program. All exercise protocol was supervised and performed with oxygen supplementation 2 L/min via intranasal cannula to avoid unwanted shortness of breath (SOB). Full written consent obtained from the participants prior to the study. Adequate level of confidentiality and privacy of subjects was established. The study protocol was approved by the College of Medicine King Saud University Institutional Review Board (Ref. No. 17/0591/IRB, dated Oct. 5, 2017). The pulmonary function test (PFT) was carried out according to previously recommended techniques [30]. Measurements of participant’s body mass composition, blood pressure, oxygen desaturation SpO2, were recorded before and after the exercise.
Supervised exercise training (SET)
Endurance and resistance training are the main applied modalities in typical exercise training programs. Participants attended a SET program twice-weekly for eight weeks which consisted of endurance training (cycle ergometer and arm ergometer) and resistance training (upper and lower limb) exercise training as described previously [29, 31].
Endurance training
The endurance training program involved flexibility and aerobic exercises. We relied on the Rating of perceived exertion (PRE) scale and complemented by HR monitor (polar watch 430) for monitoring the training intensity. In the initial visit, exercise intensities for endurance training were targeted to the level that patients could exercise at. This meant just lower than the Borg breathlessness rating based on RPE (12–13/20 progressing to 14–15/20, moderate to vigorous, respectively which depended on the ability of subjects and symptom of Borg RPE scale. The target HR was calculated using the HR reserve method such that during the activity the HR was kept below 60% of HR reserve.
Training in cycle ergometer
Participants had performed exercise training in cycle ergometer (ergoline GmbH – Type: ergoselect 200 p mit BD) at an intensity which was initially equivalent to 60% of baseline HR reserve with 20 seconds work interspersed with 20 seconds rest for a maximum time 15 min. The workload was increased according to the subject’s ability and exercise intensity (RPE and HR) for about (5 to 10) watts at each exercise session.
Training in arm-ergometer
Participants have performed exercise training in arm ergometer at interval training. (ergoline GmbH – Type: ergoselect 400 p) at an intensity which was initially equivalent to 60% of baseline HR reserve with 20 seconds work interspersed with 20 seconds rest for a maximum time 15 min. The workload was increased according to the subject’s ability and exercise intensity (RPE and HR) for about 5 watts at each exercise session.
The resistance training
The resistance training session comprised three sets of leg extension and front raise. The intensity-based on one repetition maximum (1RM) (40% to 50%) for one to three sets with 10 to 15 repetitions per set with one min of rest between the sets. The progression of resistance training was expressed by the weight in kgf, that participant worked against in each visit. Most of the subjects trained with 5–20 kgf, depending on their individual ability and symptoms of RPE.
All outcome measures were determined at baseline (visit 1) and after completion of eight weeks of the exercise intervention (visit 15). The following variable indicators were measured before and after SET.
Outcome measures
Shortness of breath questionnaire (SOBQ)
Both patients and healthy subjects were asked to fill the SOBQ. It is a multi-dimensional instrument to measure the three factors of dyspnea (intensity, quality and emotional responses to this sensation). It is a valid and reliable tool used to indicate severity of shortness of breath previously [32]. The (SOBQ) involves twelve descriptor items on a scale of none (0), mild (1), moderate (2), or severe (3). Total scores from the (SOBQ) range from 0 to 36, with higher scores showing greater severity.
Six minutes walk test (6MWT)
The 6MWT was used for estimating exercise capacity in both ILD patients and controls. The reproducibility of the 6MWD has been confirmed in ILD [33]. Participants were trained to walk from one end to the other of long uncrowded 50 m long hallway at their own speed, while trying to cover as much as possible f a distance in 6 min. Finally covering distance was recorded at the end of six-minute waking before and after SET program.
Heart rate (HR)
Polar heart rate monitor was used to assess the heart rate (HR) of all participants before and after exercise session.
Blood sample collection and analysis
Blood samples from the 10 ILD patients and 18 matched healthy controls were drawn after overnight fasting. Blood was taken into 3 mL EDTA containing tubes for blood collection. The samples were centrifuged directly after the blood sampling for 20 min at 4
Statistical analysis
Data were analysed by using the statistical software package SPSS, version 21 and it will presented as mean
Results
Demographic characteristics of study groups
The demographic characteristics of the sampled study groups are presented in Table 1.
0pt 0pt
Personal characteristics and Body mass index of the sampled study groups
Personal characteristics and Body mass index of the sampled study groups
The findings of the 6MWT are outlined in Table 2. The PwILD had significantly lower 6MWD values than control group at 1st visit (395
Six minutes walk test (6MWT) of the sampled study groups
Six minutes walk test (6MWT) of the sampled study groups
The overall change in SOBQ score of Dyspnea-12 using questionnaire (D-12) before and after SET program is presented in Table 3 and Fig. 2 for both PwILD and controls. Patients had higher D-12 score at baseline than the controls and the score was reduced significantly (
Overall change in shortness of breath respiratory questionnaire (D-12) items before and after SET according to the study groups
Overall change in shortness of breath respiratory questionnaire (D-12) items before and after SET according to the study groups
Change in GDF15 levels before and after intervention among the study groups
Change in overall shortness of breath respiratory questionnaire (SOBQ) score before and after intervention among the study groups.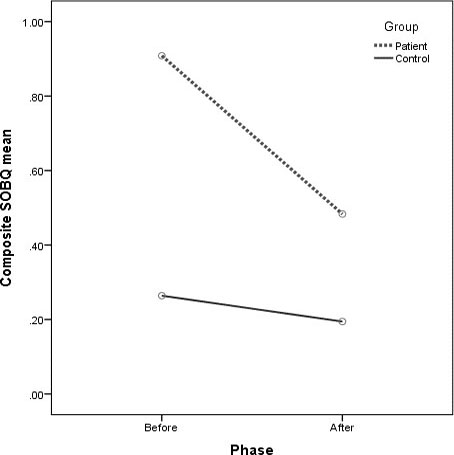
Trends in HR before and after SET were recorded at each visit among the study groups. The patients comparatively had higher HR than the controls before starting SET and after completing the SET. Figure 3 shows the overall change (difference between pre and post SET) in heart rate (HR) of patients (30–35 bpm) compared to controls (40–45 bpm) at each visit.
Trend in HR change (difference between pre and post SET) at each visit among the study groups.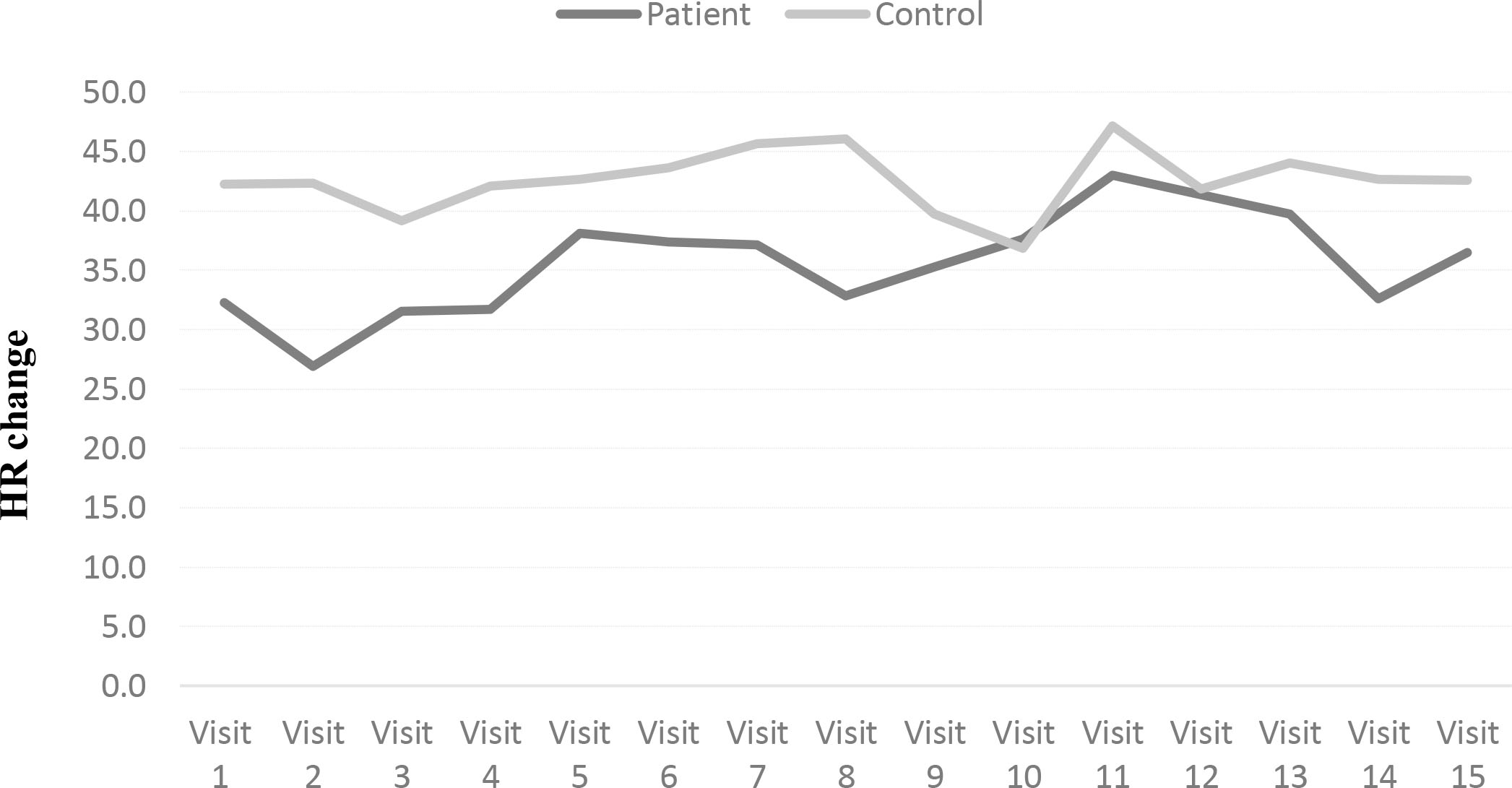
The mean pre exercise and post exercise training GDF15 levels are presented in Table 4. Pre and post mean GDF15 values of ILD patients (120.9
Discussion
Recently, there is increasing evidence that exercise training is a vital element of pulmonary rehabilitation (PR), and efficient intervention to improve dyspnea, exercise capacity and functional status in PwILD. In the present case-control interventional design study we evaluated the effect of SET on exercise capacity, dyspnea and GDF-15 plasma levels in PwILD and normal healthy subjects.
This study demonstrate that all Pw ILD improved the 6MWD significantly which is consistent with earlier reports [34]. Our results indicate an overall mean improvement of 64 meters in 6MWD which was greater than the minimal clinically important difference (MCID) (30–33 m) [5] previously reported for PwILD [13, 35, 36, 37, 38]. Though increases in 6MWD beyond the MCID has been described [34] after exercise training (ET) in PwILD the mechanism by which this increase was arbitrated was not unfolded. The smaller improvement by the controls (44 m) may be due to the latter having achieved long distances at baseline with limited capacity for further improvement.
In spite of the limited improvement in PwILD, some symptomatic benefit was attained with variations in SOBQ and HR symptoms beyond the MCID. Generally, the SOBQ and HR score improved after exercise. The overall score of D-12 questionnaire at baseline was high and then declined post-SET, while minimum changes in the score of overall D-12 questionnaire were found in the control group having low scores at baseline. This significant improvement in dyspnea was associated with the observed gains in exercise capacity in the PwILD. Similar improvements in dyspnea were obtained in other studies [11, 13, 34] using Chronic Respiratory Disease Questionnaire (CRDQ) that achieved the minimum important difference (MID). To our knowledge, no previous study adopted the D-12 Questionnaire to evaluate the effect of an exercise training program in dyspnea improvement for these patients. Further investigation is necessary to explain the usefulness of the SOBQ in determining change in dyspnea in PwILD. These facts have important clinical significance and practical associations, since proven and effective therapies for ILD are restricted.
Numerous mechanisms may explaine the effect of exercise training on the physiological and clinical outcomes in PwILD. It is possible that frequent stimuli of high ventilation required during exercise sessions, stretching of the thoracic muscles and chest expansion during deep breathing exercises resulted in a more effective breathing pattern, enhance pulmonary compliance and pleural elasticity within the lung tissue, increased strength of respiratory muscles and decreased dyspnea perception following exercise training [39].
Since no suitable biomarker for the diagnosis of ILD exists the main object of our study was to evaluate the effect of SET on GDF15 biomarker in patients with ILD. Our results show significantly higher GDF15 levels as compared to controls both pre and post SET. However, no significant change in GDF15 values has been observed within PwILD and controls after SET innervation. Similar trend in increase of GDF15 levels were reported after playing different sports [40, 41]. So far no single study reported the effect of exercise on GDF15 concentration in these patients. However, previously increased GDF15 levels associated with both COPD [42] and lung injury [43] have been reported. Since GDF15 is not lung specific it is difficult to tell whether the source of GDF15 is from lung tissue or other organ systems.
This study has some limitations. First, the small sample size prevents generalization. Additional confirmation of the findings in a larger, extensive group of PwILD is necessary. Second, the sample was heterogeneous with respect to enclosure of patients with numerous ILD etiologies. The sample size was inadequate for subgroup analyses based on etiology. This again may obstruct the ability to generalize data over the entire ILD group.
This study hints that the SET program may be effective for patients with ILD, providing significant clinical improvements in exercise capacity, dyspnea and functional status for these patients. This strengthens the recommendation for the role of exercise training as part of a standard comprehensive treatment for ILD patients. The described SET seems to be safe and well tolerated by the patients. However, the exact underlying mechanisms of training adaptation, long-term impact, the ideal program modalities, and other issues still need to be elaborated in further studies.
Conclusions
This study provided evidence that patients with ILD completing SET program established progress in exercise capacity (6MWT) and dyspnea. The results also indicate that SET does not affect circulating GDF-15 levels in PwILD although their GDF15 values were significantly greater than the control group’s before and after SET. Moreover, these values may be considered clinically significant. Our results provide preliminary support for introducing SET programs to increase pulmonary function and exercise capacity in patients with PwILD, but maintenance strategies are warranted to preserve the outcomes. From a clinical perception, the results of this study offer evidence that exercise training is safe and well tolerated by PwILD and that participation may improve their exercise performance.
Author contributions
CONCEPTION: Abdulrahman Mohammed Alhwoikan
PERFORMANCE OF WORK: Rahmah Mohammad Alyami
INTERPRETATION OR ANALYSIS OF DATA: Rahmah Mohammad Alyami
PREPARATION OF THE MANUSCRIPT: Rahmah Mohammad Alyami
REVISION FOR IMPORTANT INTELLECTUAL CONTENT: Abdulrahman Mohammed Alhwoikan
SUPERVISION: Abdulrahman Mohammed Alhwoikan
Ethical considerations
Institutional Review Board approval number; E-17-2630 Dated: 5
Funding
National Plan for Science and Technology and Innovation (MAARIFAH), and Vice Deanship of Research Chairs, at King Saud University, Kingdom of Saudi Arabia for financial support.
Footnotes
Acknowledgments
We thank National Plan for Science and Technology and Innovation (MAARIFAH), and Vice Deanship of Research Chairs, at King Saud University, Kingdom of Saudi Arabia for financial support.
Conflict of interest
The authors have no conflicts of interest to report.