
Abstract
Objective:
To study the clinical features of interstitial lung disease (ILD) in patients with dermatomyositis and factors related to its development.
Methods:
Clinical records for patients with dermatomyositis were reviewed retrospectively.
Results:
Records were analysed for 230 patients (mean follow-up period, 18 months). The prevalence of ILD was 49.6%. The presence of ILD correlated positively with the presence of arthralgia, myoasthenia and cough, but negatively with the presence of Gottron’s papules. Patients with ILD had poorer pulmonary function and more frequent positivity for anti-Jo1 antibodies than those without ILD. Patients with ILD characteristically showed linear, patchy, ground-glass opacities and reticular computed tomography (CT) patterns, usually at the bottom or apex of the lung.
Conclusions:
Dermatomyositis patients presenting with heliotrope rash, arthralgia, myoasthenia, cough, dysphagia, anti-Jo1 positivity or abnormal lung function were more likely, whereas those presenting with Gottron’s papules were less likely, to develop ILD. Characteristic CT patterns in dermatomyositis patients with ILD were lines, patches, ground-glass opacities and reticulation.
Introduction
The inflammatory myopathies are a group of acquired skeletal muscle diseases that include polymyositis, dermatomyositis and inclusion body myositis. Dermatomyositis is an inflammatory idiopathic myopathy that is characterized by proximal muscle weakness and cutaneous eruptions. Patients eventually have problems with activities of daily living and may develop pulmonary disease, cardiac disease and other autoimmune disorders.1–3 Lung involvement in dermatomyositis may appear as inflammatory interstitial lung disease (ILD) and/or as a complication of muscle weakness, with consequences that may include aspiration pneumonia or ventilatory insufficiency. Studies report a prevalence of ILD ranging between 10% and >50%. 4 ILD is a negative prognostic factor associated with increased morbidity and mortality in patients with polymyositis/dermatomyositis.5–7 However, the clinical profile of ILD in polymyositis/dermatomyositis remains to be clarified. Unanswered questions about the prevalence or dermatomyositis–ILD in China, factors that may be related to its occurrence and development and its characteristic computed tomography (CT) imaging findings prompted us to conduct the present study. We hoped to establish whether CT scanning should be added to the routine examinations undertaken in future, in patients with dermatomyositis presenting to hospital.
Patients and methods
Study population
In a retrospective study based on information in patients’ medical records, we identified patients admitted to the Department of Dermatology at Huashan Hospital, Shanghai, China, between January 2005 and March 2011, who had dermatomyositis based on the criteria of Bohan and Peter.1,2
Screening for ILD had comprised of questioning about pulmonary complaints, lung auscultation, pulmonary function testing and lung radiological examinations. In the event of suggestive findings in the screening examinations, lung CT had been performed for verification. ILD was diagnosed when the CT findings showed bilateral reticular opacities, with or without honeycombing, or extensive ground-glass opacities. Patients with other substantial pulmonary diseases (such as severe emphysema), and those with a history of other lung diseases that could develop into fibrosing alveolitis were excluded, as were patients who had evidence of chronic congestive heart failure. 4
The study protocol was approved by the Ethics Committee of Huashan Hospital, Fudan University. All investigations in this study were conducted in accordance with the Declaration of Helsinki. Personal identifiers were removed from the data set before analyses were undertaken. Written consent was obtained from each participant included in the retrospective analysis.
Data retrieval
Clinical data retrieved from records made at the time of dermatomyositis diagnosis included each patient’s clinical history, physical examination results, laboratory findings, CT findings, pulmonary function test results and any moderate or severe electromyographic findings. Because only 25 patients had been willing to undergo muscle biopsy, no biopsy results were collected. However, all the results were consistent with the diagnostic criteria for dermatomyositis. Particular attention was paid to information that recorded signs and symptoms. Information on treatment was collected from medical records at the time when patients were discharged from hospital.
Laboratory tests
Serum samples were obtained from patients on admission, using standard techniques, and were immediately sent to the Clinical Immunology Department of Huashan Hospital for analyses of aspartate aminotransferase, lactic dehydrogenase, α-hydroxybutyrate dehydrogenase, erythrocyte sedimentation rate, creatine kinase, creatine kinase isoenzyme MB, antinuclear antibodies and antibodies against histidyl-transfer RNA synthetase (Jo1). The Euroline immunoassay system (catalogue numbers DL1590-1601 8G and DL1530-1601 3G; Euroimmun® US, Morris Plains, NJ, USA) was used for the parallel detection of different autoantibodies. All assays were performed according to the manufacturer’s instructions.
Pulmonary investigations
Pulmonary function had been tested by measuring vital capacity (VC, a surrogate measure of pulmonary muscle strength), total lung capacity (TLC, measured to detect restrictive lung defects) and carbon monoxide diffusion capacity (DLCO, measured by spirometry, using the single-breath method). Test results were expressed as percentages of predicted values for age and height.8,9 Pulmonary muscle strength was considered to be reduced if VC or total lung capacity was ≤ 80% of the predicted value. Values ≤ 80% for TLC and DLCO were considered abnormal.
Lung CT
Computed tomography scanning results were obtained for each dermatomyositis inpatient who had undergone a lung CT scan during the study period. Each lung CT was performed using a Somatom® scanner (Siemens, Erlangen, Germany). Slice thickness was 2 mm every 20 mm, including the entire lung. Typical CT findings in ILD include linear opacities (thickened inter- and intralobular septa), consolidation (areas with increased attenuation, and obscuration of bronchial walls and vessels) and ground-glass opacities (hyperattenuated areas in which the bronchi and vessels remained visible). Honeycombing (areas of small cystic spaces with thickened walls) and traction bronchiectasis (bronchial dilatation due to traction by fibrous tissue) were considered to be consistent with fibrosis. 10
Statistical analyses
Mean data are presented ±SD. The paired t-test was used to compare continuous variables (age and laboratory values) between the groups with and without ILD. The χ2-test was used for discrete variables (sex, symptoms and altered lung function). P-values < 0.05 were considered significant. All tests were performed using Stata® software, version 9.0 (Stata Corp., College Station, TX, USA), except for multifactorial logistic regression analysis, which was performed using SPSS® software, version 15.1 (SPSS Inc., Chicaco, IL, USA). Such analyses were undertaken to reveal more about the link between clinical findings and the development of ILD in dermatomyositis patients.
Results
Patient characteristics
A total of 230 dermatomyositis patients were identified during the study period, 91 of whom were men and 139 were women; their mean age was 51.97 ± 15.48 years (range, 17–84 years). The mean duration of dermatomyositis from symptom onset was 18 ± 27.99 months (range, 2 weeks to 10 years). Of the 230 patients, 114 (49.6%) were diagnosed with ILD; 63 of the 114 patients with ILD were females and 51 were males. The mean age of the dermatomyositis patients with ILD was 54.82 ± 13.27 years (range, 17–83 years). Of the 116 dermatomyositis patients not diagnosed with ILD (50.4%), 76 were females and 40 were males: the mean age of these patients was 49.16 ± 16.98 years (range, 21–84 years). Distributions of age and sex did not differ significantly between the groups with or without ILD. The median course of dermatomyositis in patients with ILD was 13 months (range, 1–57 months), which did not differ significantly from the 23 months (range, 2–120 months) observed in patients without ILD. Seven cases were complicated with malignant tumours: four with lung cancer, two with breast cancer and one with nasopharyngeal carcinoma.
Disease manifestations
Cutaneous manifestations in 230 dermatomyositis patients with or without interstitial lung disease (ILD.

Data presented as n (%) of patients.
Statistical analysis performed using the χ2-test.
NS, no statistically significant between-group difference (P ≥ 0.05).
Other clinical manifestations in dermatomyositis patients with or without interstitial lung disease (ILD.

Data presented as n (%) of patients.
Statistical analysis performed using the χ2-test.
NS, no statistically significant between-group difference (P ≥ 0.05).
Laboratory findings
Laboratory findings in dermatomyositis patients with or without interstitial lung disease (ILD.

Data presented as mean ± SD or n (%) of patients.
Statistical analysis was performed with the paired t-test (continuous variables) or χ2-test (discrete variables).
ILD, interstitial lung disease; NS, no statistically significant between-group difference (P ≥ 0.05).
Electromyographic and pulmonary investigations
Electromyographic and pulmonary function test findings in dermatomyositis patients with or without interstitial lung disease (ILD.

Data presented as n (%) of patients.
Statistical analysis performed using the χ2-test.
DLCO, carbon monoxide diffusion capacity; NS, no statistically significant between-group difference (P ≥ 0.05).
Pulmonary function test results were available in 99 patients with, and 83 without, ILD. Tests were not performed in 48 patients because they were not clinically indicated or because the patient had declined the test. For all three tests (VC, TLC and DLCO), there were significantly greater percentages of patients with reduced values in the group with ILD than in the group without ILD (all P = 0.000, Table 4). The greatest difference was in the number of patients with reduced VC, i.e. reduced pulmonary muscle strength (82 [82.8%] and nine [10.8%] of the patients with or without ILD, respectively).
Lung CT findings
Lung computed tomography findings in dermatomyositis patients with or without interstitial lung disease (ILD.
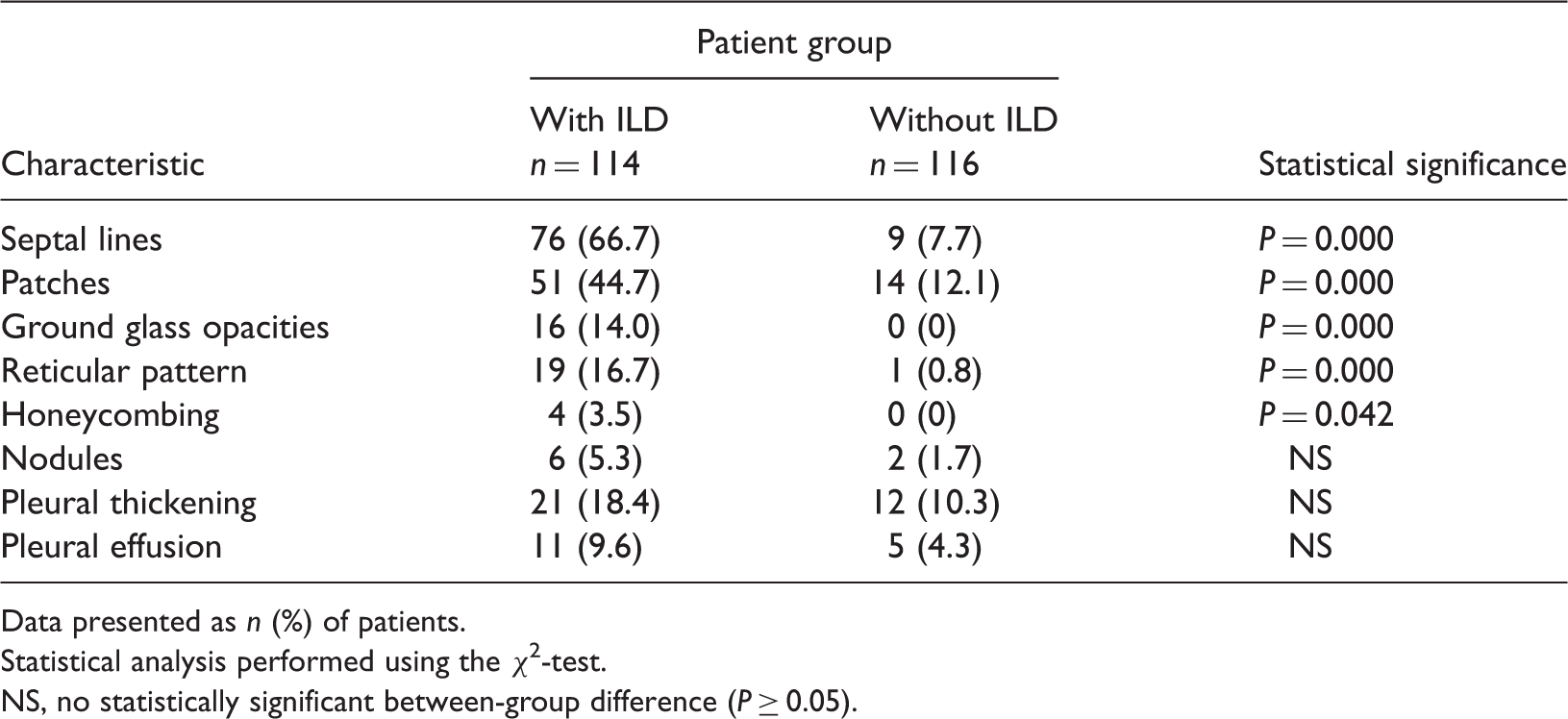
Data presented as n (%) of patients.
Statistical analysis performed using the χ2-test.
NS, no statistically significant between-group difference (P ≥ 0.05).
Multifactorial logistic regression analysis
Multifactorial logistic regression analysis of the s between clinical manifestations and interstitial lung disease in dermatomyositis patient.

Treatment
Corticosteroids were the mainstay of treatment for the dermatomyositis patients included in this study. In most cases, improvement was seen during the first 4 weeks of such treatment. Subsequently, dosages of oral steroids were gradually reduced and changed to alternate-day regimens. Monitoring patients for the adverse effects of steroids and prophylactic use of agents to offer gastrointestinal protection were routinely undertaken.
Discussion
The mechanism underlying the development of ILD in patients with dermatomyositis remains unclear. In most studies, ILD has been thought to be an antibiotic-resistant pneumonitis. Alveolitis appears in the early stages of collagen vascular diseases that are associated with ILD and may eventually develop into pulmonary fibrosis.
Although the outcome for patients with polymyositis/dermatomyositis has substantially improved, at least one-third of patients are left with mild to severe disability.13–15 Older age and association with severe internal diseases (such as diabetes mellitus, arrhythmia and severe pulmonary infection) are factors associated with poor prognosis.13–15 Consequently, the survival of dermatomyositis patients with severe ILD is poor. 16
In this retrospective study of dermatomyositis patients, we found a high prevalence of ILD (49.6%), which is within the range of 10–50% reported by Fathi et al. 17 Because ILD is a key factor relating to organ involvement and prognosis, and because of its high prevalence, it is important that dermatologists pay close attention to the early diagnosis and prompt treatment of ILD in dermatomyositis patients.
The presence of cough at disease onset was the most common pulmonary symptom in dermatomyositis patients with ILD (30 patients, 26.3%). Clinical manifestations such as myoasthenia, myalgia, difficulty in combing the hair/climbing stairs, arthralgia and dysphagia occurred significantly more frequently in dermatomyositis patients with ILD than in those without ILD. However, cutaneous manifestations were less closely related to the occurrence of ILD. Both heliotrope rash and Gottron’s papules are specific for dermatomyositis. In the present study, heliotrope rash was significantly more prevalent in the dermatomyositis patient group with ILD than in the group without ILD, while the reverse was observed for Gottron’s papules. As cutaneous manifestations might fluctuate with time, the presence of either Gottron’s papules or heliotrope rash determined at a single timepoint may not correlate with ILD. In the present study, most patients’ cutaneous manifestations were recorded at the onset of dermatomyositis. We consider that it is important to follow these dermatomyositis patients and evaluate cutaneous manifestations on future occasions, if a reliable conclusion is to be reached.
Several laboratory markers can be used to predict the development of ILD, such as the presence of antiaminoacyl tRNA synthetase antibodies; of these, the antihistidyl tRNA synthetase antibody anti-Jo1 is the strongest predictive factor for ILD in patients with myositis. 18 The reported frequency of ILD in patients with anti-Jo1 antibodies is >70%. 19 In our study, the frequency of ILD in patients with anti-Jo1 antibodies was much lower than this (seven patients, 6.1%), although all seven of these patients had ILD. Thus, the presence of anti-Jo1 antibody was highly associated with ILD, in dermatomyositis patients. We suggest that routine testing for anti-Jo1 antibodies is undertaken in dermatomyositis patients who present with cough, myoasthenia, myalgia and difficulty in combing hair/climbing stairs, arthralgia or dysphagia, especially in those without Gottron’s papules.
Clinical and laboratory abnormalities suggestive of muscle disease are characteristic features of dermatomyositis. The myopathies primarily affect the proximal muscles, are usually symmetrical and are slowly progressive over a period of weeks to months. 20 In the present study, the myopathies in most of the dermatomyositis patients with ILD affected the proximal muscles. The prevalence of myopathies in patients with ILD was 55.3%) was greater than that in those without ILD (43.1%), though this difference was not statistically significant.
Interstitial lung disease is associated with restrictive lung-function impairment, which is defined as reduced TLC. Pulmonary function test results in our study showed that patients with ILD had significantly poorer function than those without ILD. However, in some myositis patients, low TLC can also be a consequence of respiratory muscle weakness.3,11 Thus, we cannot exclude the influence of muscle weakness on leading to reduced lung volume in some patients. In most of our cases, restrictive lung function impairment was accompanied by reduced DLCO. Reduced DLCO did not occur in the absence of restrictive lung function impairment in the present study.
Lung CT is essential for the evaluation of ILD. Lines, ground-glass opacities and peribronchovascular thickening have been identified as the most common lung CT abnormalities observed at the initial imaging.11,12 In the present study, the main lung CT abnormalities in dermatomyositis patients with ILD were septal lines (66.7%), patches (44.7%), ground-glass opacities (14.0%), reticulation (16.7%) and pleural thickening (18.4%): full data appear in Table 5. Because lung CT has been found to be a sensitive method of detecting early changes in the pulmonary system, and is an ideal means of evaluating the prognosis of dermatomyositis patients with ILD,21,22 lung CT scanning should be included in the routine examination of dermatomyositis patients and those who have ILD in addition to other diseases.
In conclusion, this study revealed that the presence of arthralgia, myoasthenia and cough were positively related to the presence of ILD in dermatomyositis patients, whereas the presence of Gottron’s papules was negatively related to ILD. Positivity for anti-Jo1 antibody was significantly associated with ILD, in dermatomyositis patients.
Footnotes
Declaration of conflicting interest
The Authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.