
Abstract
BACKGROUND AND OBJECTIVE:
Muscle weakness is among the most common and obvious impairments in older adults and individuals with neurologic disorders. Although impairments in muscle strength are typically characterized using performance measures, the impairments have also been described using patient or observer-report. The objective of this review was to summarize literature describing use of a patient-report instrument, the Strength Domain (SD) of the Stroke Impact Scale (SIS), to grade strength impairments.
METHODS:
Peer-reviewed literature reporting SD scores for the SIS was identified using computerized searches of the CINAHL, PubMed, and Scopus databases followed by hand searches. Potentially relevant articles were then mined for data on the participants tested, the SIS version used, scores documented, and clinimetric properties reported.
RESULTS:
Sixty-five articles were judged appropriate based on inclusion and exclusion criteria. The articles involved more than 7000 residents of 22 countries. All articles focused on individuals with stroke (usually chronic), although one also included community-dwelling adults without stroke. The SIS version used was frequently unreported, but 3.0 was version most often specified. For articles reporting SD scale scores the mean ranged from 19.7 to 85.5. Construct (known groups, convergent, and discriminant) validity of the SD was supported by the literature as was its internal consistency and test-retest reliability. Responsiveness of the SD was evinced by numerous studies showing increases in SD scores with time or accompanying effective interventions. However, only one study indicated responsiveness using an anchor-based statistic.
CONCLUSIONS:
The SD of the SIS is a well-established and mostly clinimetrically sound patient-report measure of paretic limb strength among individuals with stroke. Its use with individuals with weakness accompanying aging or diagnoses other than stroke remains to be substantiated.
Introduction
Muscle strength, a muscle power function according to the International Classification of Functioning, Disability and Health (ICF), is well established as an important body function [1]. Numerous options for measuring muscle strength have been described in the literature. Although performance measures are by far the most commonly employed, patient- and observer-report measures have also been used. Bohannon recently reviewed the scores and clinimetric properties of several different patient-report measures of strength [2]. Intentionally, his review did not address what may be the most widely used patient-report measure of strength, that is, the strength domain (SD) of the Stoke Impact Scale (SIS).
The SD of the SIS requires patients to rate their strength over the past week in the: a) arm that was most affected by their stroke, b) hand grip that was most affected by their stroke, c) leg that was most affected by their stroke, and d) foot/ankle that was most affected by their stroke. The strength of each of the 4 aforementioned body regions is rated as: 5 (a lot of strength), 4 (quite a bit of strength), 3 (some strength), 2 (a little strength), and 1 (no strength at all). The total SD score (range 4 to 20) is often converted to a scale score which can range from 0 to 100 [3].
As no critical review of the SD of the SIS exists to guide clinicians in decisions regarding its use, the current review was undertaken to summarize the literature reporting use of the SD of the SIS to describe strength impairments. Of particular interest were the specifics of use, scores reported, and the clinimetric properties of the SD.
Methods
Peer-reviewed articles providing information on the SD of the SIS were sought by the author via computerized searches of 3 bibliographic databases (CINAHL, PubMed, and Scopus) as well as hand-searches on September 17, 2020. The search start date was January 1, 1990. The search string employed in all searches was ““Stroke Impact Scale” AND “Strength.”” Only articles including information specific to the SD of the SIS were included. Articles were excluded if they were reviews, case studies, protocols, meeting abstracts, or written in a language other than English (unless adequately translatable by Google Translate). Articles were also excluded if they did not include descriptive statistics for scores of the SD.
Potentially relevant articles addressing the SD of the SIS were mined for information on populations tested, the SIS version used, and findings regarding the SD of the SIS. Findings regarding the SD focused on SD scores and specifics relevant to clinimetrics of the SD (i.e., validity, reliability, and responsiveness).
Results
Figure 1 illustrates how the final sample of 65 experimental and non-experimental studies was derived from the 147 non-duplicative potentially relevant articles identified by the searches. The 65 summarized articles included greater than 7000 participants from 22 countries, with the United States, Taiwan, and Sweden contributing the largest number. All articles focused on individuals with stroke (usually chronic), although one also included community-dwelling adults without stroke [38]. The specific SIS version used was often unreported. When stipulated, the most common version was 3.0. Thirteen studies denoted non-English language versions of the SIS [10, 11, 13, 15, 16, 17, 20, 22, 44, 46, 47, 49, 50]. All studies reported SD scores based on patient-report, but 2 studies included SD scores obtained from proxy-report [15, 24] as well. Per design, all included studies reported descriptive statistics for SD scores. However, scores in 2 studies were limited to the “arm” and “hand” items of the SD [9, 19]. Most studies reported SD scale scores- the mean of which ranged from 19.7 to 85.5. One study presented only the standard deviation (19.3) of SD scale scores [43].
Flow chart summarizing how the ultimate sample of articles was determined.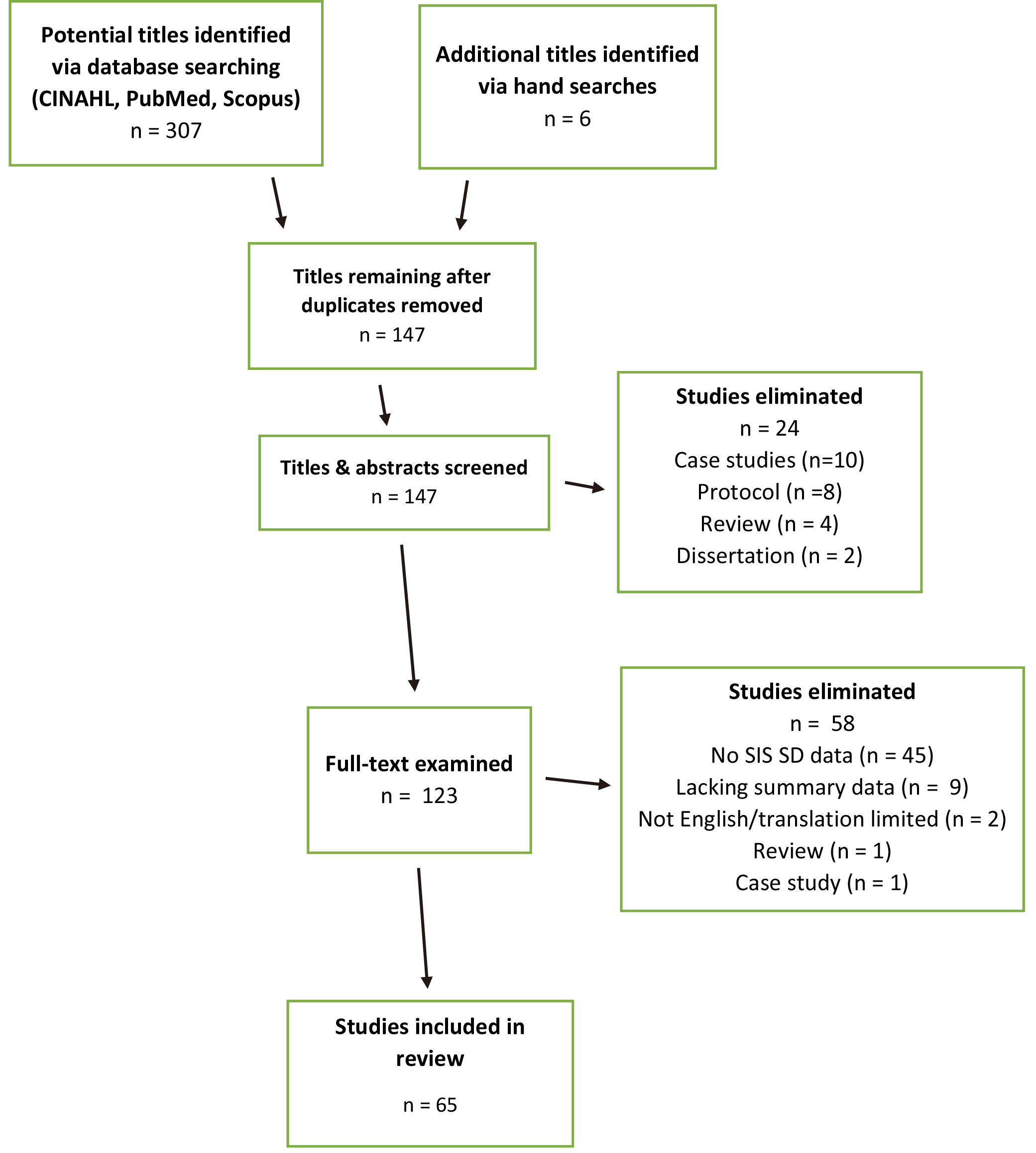
Clinimetric support for the SD of the SIS was found to be mostly supportive. This support incorporates construct validity, reliability, and responsiveness.
Three subtypes of construct validity were supported by the literature reviewed. The first subtype of validity supported was known groups validity; herein, defined as the ability of the SD scores to distinguish between groups expected to differ in limb strength. Among the articles summarized in this review, significant differences in SD scores were found between hierarchical categories (groups) of the Modified Rankin Scale (disability) [15, 16, 17, 61], Barthel Index (activities of daily living) [13, 15, 17, 67], National Institutes of Health Stroke Severity Scale (NIHSS) [13], Stroke Upper Limb Capacity Scale (upper limb mobility) [10], gait speed [35], and Activity Card Sort (physical activity participation) [63]. The second subtype of validity supported by the literature was convergent validity; herein defined as the degree to which SD scores of the SIS were related to other measures with which they theoretically should be related. SD scores would certainly be expected to be, and were, correlated significantly with other measures of muscle strength. Specifically, SD scores were found to correlate significantly and strongly with NIHSS Arm and Hand Motor Scores (
The third subtype of validity supported was discriminant validity; that is, the extent to which SD scores of the SIS were unrelated to other measures to which they would not, in theory, be expected to be related. In this review, measures classified as theoretically unrelated were those clearly nonphysical in nature. The measures and their mostly very weak and insignificant correlations with the SD were the Memory (
Summary of studies included in review
Anxiety and Depression Scale scores (
Three primary aspects of relative reliability have been addressed in the literature: internal consistency, test-retest reliability, and inter-tester reliability. Internal consistency of SD item scores has been documented in 7 studies (
Responsiveness, or the sensitivity of a measurement to changes in strength over time, found considerable support in studies showing SD scores to increase, often significantly, over time or concomitant with interventions [3, 4, 5, 6, 7, 8, 13, 14, 15, 22, 23, 28, 29, 30, 31, 32, 33, 36, 37, 38, 39, 40, 41, 42, 43, 44, 49, 50, 51, 52, 56, 60, 62, 64, 65, 66]. These increases could vary depending on the intervention applied, the severity of stroke, or the chronicity of stroke [3, 28, 29, 39, 51, 52, 56, 60, 64, 65, 66]. In regard to chronicity, the SD of the SIS actually decreased significantly between 1 and 5 years in one study [54] and between 1 and 6 years in another study [67]. Formal statistical summaries of responsiveness over time in the review were scarce. With 1 exception, they involved distribution-based statistics including effect size [39], standardized response mean [13], standard error of measurement [15, 43], and smallest real difference/minimal detectable change [15, 43]. The exception was the purported minimal clinically important difference of 9.2 points referred to by Lewthwaite et al. [40].
This review focused on literature addressing use of the SD of the SIS as a self- or proxy-report measure of limb muscle strength. The large number of individuals in different settings whose diverse limb strength has been measured with different versions of the SD of the SIS studies provides support for its use. Nevertheless, use of the SD of the SIS almost exclusively with patients with stroke limits its generalizability. While known groups and convergent validity of the SD of the SIS is well established in this review, its relationship with other self-report measures of limb muscle strength remains unexplored [2]. Discriminant validity is mostly supported, but whether strength should be or not be related to specific nonphysical variables is debatable. Also unaddressed is self-report of trunk muscle strength.
The reliability of SD measures of the SIS, whether test-retest or inter-tester, is generally acceptable in this study. However, ICCs less than 0.80 are not uncommon. Moreover, the SD of the SIS is a essentially ordinal measure not best addressed by the ICC. So the reliability of the SD of the SIS would appear to warrant further scrutiny. The same applies to information on responsiveness. This review has several limitations beyond those already noted. First, a single examiner was engaged in the selection and review of articles. Second, by intent, no quality rating was conducted.
Conclusions
Use of the SD of the SIS is supported by considerable evidence. However, further research Is required, particularly in its use with nonstroke populations.
Ethical considerations
This study, as a literature review, was exempt of Institutional Review Board approval.
Funding
The author reports no funding.
Footnotes
Acknowledgments
The author has no acknowledgments.
Conflict of interest
The author claims no conflict of interest.