: Sarcopenia is a component of frailty, which is a common geriatric syndrome for which the quantification of muscle strength is important.
OBJECTIVE:
Describe studies that have used isokinetic testing for detecting sarcopenia and determine whether there is an isokinetic strength level that can best detect sarcopenia.
METHODS
: A systematic review was performed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses. Our literature search involved the following key words: (isokinet*) AND ((sarcopenia) OR (frailty) OR (muscle weakness). Sarcopenia reference values for isokinetic knee flexion and extension at 60/s were determined using summary data from relevant articles.
RESULTS:
A total of 19 studies that were relevant and lacked major methodological flaws were included. Most measured peak torque of the knee extensors and/or flexors. The measurements were found to be valid and responsive. The net moment weighted averages for knee extension torques were 83 3 Nm for males and 60 7 Nm for females in sarcopenia population. For knee flexion, the weighted averages for knee extension torque were 47 6 Nm for males and 36 5 Nm for females in sarcopenia population. All weighted averages were significantly lower than the reference values for the healthy population aged 60–70 ( 0.001).
CONCLUSIONS:
The isokinetic strength values reported herein can be used to identify sarcopenia in older men and women.
Numerous studies have described muscle strength as decreasing with age. Such decreases are a highlight of geriatric syndromes such as sarcopenia and frailty. As both sarcopenia and frailty typically lead to mobility limitations and a loss of overall self-sufficiency in the later stages; the identification of muscle weakness is important for both mentioned conditions. The identification of sarcopenia and frailty is typically evaluated by handgrip strength in clinical practice [1]. Handgrip strength has practical advantages, as it is easy to measure and interpret relative to available reference values [1, 2]. On the other hand, handgrip strength has disadvantages; it does not focus on muscles underlying mobility limitations [3] or untoward events such as falls [4, 5]. Although research studies on sarcopenia sometimes include isokinetic strength measurements, there is still a lack of consensus as to the what level of isokinetic strength best differentiates individuals who are versus are not sarcopenic. The purposes of this systematic review, therefore were to summarize studies in which isokinetic measures have been used for detecting sarcopenia and to determine an isokinetic strength cut-point for its designation.
Methods
The present systematic review is reported in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) [6]. The following electronic bibliographic databases were searched: Web of Science, Scopus, and PubMed. Potentially relevant articles were identified on February 10, 2019. We used the same search string in all the databases (Table 1). After deleting duplicates, article titles and abstracts were examined to determine whether the articles identified by the searches addressed the isokinetic testing of muscle strength and focused on patients/participants aged 65. We selected potentially relevant articles and then examined the full texts. Finally, we selected appropriate articles for the purposes of this review. Additionally, we hand-searched the reference lists of eligible articles and of several recently published reviews for additional studies.
Search results in electronic databases
Database
Key
Number
Web of Science
TOPIC: (isokinet*) AND TOPIC: (sarcopenia) OR TOPIC: (frailty) OR TOPIC: (muscle weakness)
580
Scopus
(TITLE-ABS-KEY (isokinet*)) AND ((TITLE-ABS-KEY(sarcopenia) OR TITLE-ABS-KEY (frailty) OR TITLE-ABS-KEY (muscle AND weakness)))
766
PubMed
Search (((isokinet*) AND ((sarcopenia) OR (frailty) OR (muscle weakness)))
575
We included all the articles from cross-sectional studies, validation studies, and randomized controlled trials in which isokinetic dynamometry was used for diagnosing participants aged 65 with sarcopenia, frailty or decreased muscle function. Articles were excluded if they failed to provide procedural specifics. Review articles and articles in languages other than English were excluded. Included articles were examined for study specifics (e.g., design, participants and aims), isokinetic testing specifics, descriptions of how sarcopenia or frailty were described, and key findings. Of particular interest in regard to key findings were the validity, responsiveness, and magnitude of isokinetic measures.
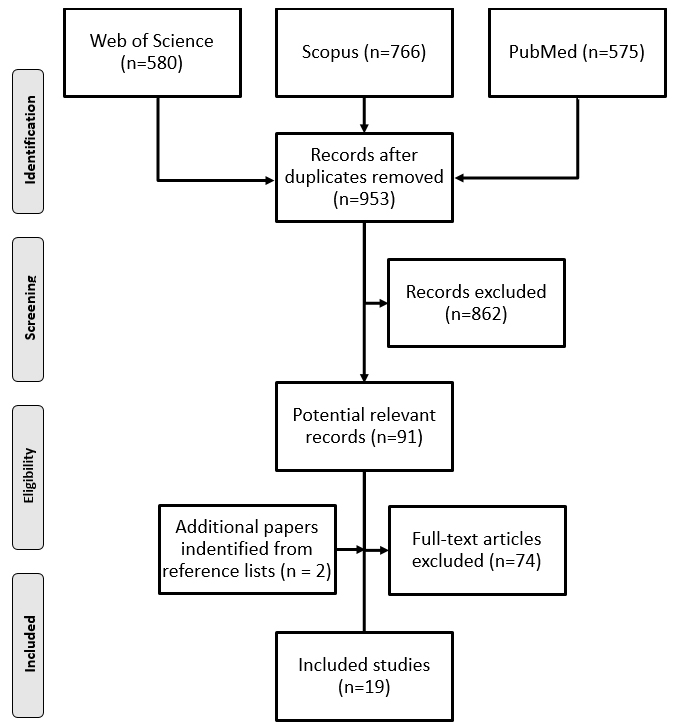
The PRISMA flowchart of the review selection process.
Calculation of weighted averages
To approximate the values of muscle strength, we calculated weighted averages when possible. We used either the baseline values in the RCTs or the values for sarcopenic/frail individuals in cross-sectional studies. The weighted average was calculated by Eq. (1).
where is the weight of each study calculated by Eq. (2).
where is the within-study variance for study (i) and is the mean for study (i). The variance of the weighted average was defined by Eq. (3).
The 95% confidence interval (CI) for the weighted average was computed as the lower limit and upper limit by Eq. (5).
The standard deviation (SD) was calculated by Eq. (6).
Then, we compared the weighted averages with the reference values for healthy older adults by the independent -test.
Results
Out of the 1,921 articles identified by the database search, we included a total of 17. An additional two articles were identified by hand searches. Ultimately, 19 articles that met the inclusion criteria were included in the review (Fig. 1).
There were 12 cross-sectional studies [7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18], four randomized controlled trials [19, 20, 21, 22], one prospective study [23], one multicenter clinical trial [24], and one validation study [25] that were included. Five studies focused on frail people, 10 focused on people with sarcopenia and the other studies focused on people with muscle functioning problems that were defined differently. The randomized controlled trials examined the influence of several physical activity interventions on different muscle-related measures. One validation study tried to establish the validity of a novel portable trunk-muscle torque measuring instrument [25]. The cross-sectional studies tried to explore different relationships among muscle function or muscle mass and several independent variables, such as plasma levels of interleukin, the extent of apoptosis activation, and bone mass density. The main topic of one study was estimating the reference values of isokinetic measures in females with frailty [18] (Table 2).
The most frequently measured isokinetic strength was that of knee extension, followed by knee flexion. Both were measured with participants in a sitting position. The most commonly reported angular velocity was 60/s. Peak torque (Nm) was the most commonly reported measure. Several different diagnostic methods were used to identify muscle problems. The most common method was the sarcopenia algorithm by the European Working Group on Sarcopenia in Older People (EWGSOP) [1]. Validity was demonstrated by a correlation between standardized physical performance tests [7, 11], simple questionnaire to rapidly diagnose sarcopenia (SARC-F) [16], bone mineral density [12], and apoptotic signaling [14], several studies demonstrated that sarcopenic or fragile people were weaker than their healthy peers [9, 8, 13, 15, 17, 18, 23]. One study presented cutoff points for trunk flexion and extension torque [25]. Isokinetic dynamometry was used in 4 intervention studies [19, 20, 21, 22]. Finally, reliability was estimated in 1 study [24]. Summary of the methods in the selected studies is presented in Table 3.
The peak torque (Nm) in knee extension as well as in flexion varied considerably among the studies. In extension, the lowest and highest values in males net moment were 57 24 Nm and 96 25 Nm, respectively; the lowest and highest values in females were 38 14 Nm and 87 18 Nm, respectively. The peak torque in knee flexion also varied; the lowest and highest values in males were 31 Nm (at 95% CI 28–34) and 63 20 Nm, respectively; the lowest and highest values in females were 18 Nm (at 95% CI 16–20) and 50 17 Nm, respectively. The peak torque weighted average in knee extension was 83 23 Nm for males and 60 7 Nm for females. The peak torque weighted average in knee flexion was 47 6 Nm for males and 36 5 Nm for females. All weighted averages were significantly lower than the reference values for the healthy population aged 60–70 ( 0.001). The results of this analysis are presented in Table 4. There was not enough information to calculate weighted averages in the faster velocity condition (180/s). However, the results at 60.s were somewhat consistent (Table 5).
Discussion
Isokinetic dynamometry is a commonly used procedure for measuring muscle strength in athletes of many sports. Nevertheless, its potential is not fully realized in older people with muscle problems. Especially in people with sarcopenia, isokinetic dynamometry can be informative. This method is useful mainly in measuring lower extremity strength, which is essential for locomotion and is one of the most important factors of self-sufficiency in the elderly population. This study clearly documented that sex-specific isokinetic strength of the knee flexors and extensors at 60/s can detect sarcopenia and frailty in individuals; the sarcopenic values (males: knee extension 83 23 Nm, females: knee extension 60 7 Nm, males: knee flexion 47 6 Nm, females: knee flexion 36 5 Nm) are lower than the normative values of a healthy population [26, 27]. On the other hand, we found that isokinetic strength measurements are not consistent across studies; therefore, procedures should be standardized in measuring isokinetic muscle group strength, selecting contraction speeds and reporting values, just as they have been for handgrip strength.
Summary of studies evaluating isokinetic strength in the sarcopenia population
American community-dwelling sedentary males and females ( 107), 71.9% frail
Examine the relationships between multiple physical factors believed to be associated with frailty, including isometric and dynamic strength, range of motion, sensation, coordination, balance, and reaction time, and the physical performance test.
Spanish, Swiss, English older people ( 368), 70.9% sarcopenic and malnourished
Quantify systematic variability and intraindividual variability among three consecutive repetitions of concentric isokinetic knee extension and knee flexion muscle actions to determine velocity-related differences in peak torque and mean power in healthy elderly older adults versus sarcopenic and malnourished older adults
Spanish, Swiss, English older people ( 257), 100% sarcopenic, malnourished
Determine the test – retest reliability and minimum detectable change scores for 7 common clinical measurements of muscle strength and physical function
Examine the association between FFM & muscle strength with bone mineral density sites and to compare the bone mineral density values between sarcopenic and nonsarcopenic older females
Compare the performance of the knee extensors test (by isokinetic dynamometer) and plasma levels of interleukin-6 & soluble receptors of tumor necrosis factor alpha between sarcopenic & nonsarcopenic community-dwelling elderly females
American community-dwelling older adults ( 20), 35.0% low-functioning
Explore the relationship between the extent of apoptosis activation in the skeletal muscle & measures of muscle mass & physical performance in older persons
American community-dwelling older adults ( 154), 49.0% sarcopenic
Classify individuals using two common sarcopenic indices: appendicular lean mass.height & skeletal muscle index, & to determine each indices value as indicators of lower extremity strength & physical function
Frailty: 1) modified PPT score between 18–32 2) peak aerobic power between 10–18 ml.kgmin 3) self-report of difficulty or assistance with two instrumental activities of daily living or one basic activity of daily living.
Responsiveness: No SGNF in knee strength after intervention.
Frailty: 1) modified PPT score between 18–32 2) peak aerobic power between 10–18 ml.kgmin 3) self-report of difficulty or assistance with two instrumental activities of daily living or one basic activity of daily living.
Responsiveness: Exercise intervention had a SGNF larger effect on the study group than on the control group in terms of maximum voluntary knee extensor & flexor torque.
Dominant extremity concentric knee extension & flexion; PT & mean power @ 60/s 7 180/s.
Sarcopenia: EWGSOP algorithm
Responsiveness: In individuals with mild-moderate sarcopenia, but not severe sarcopenia, consumption of the high-protein oral nutritional supplements SGNF leg muscle strength & quality compared with the standard diet.
Dominant extremity concentric knee extension & flexion; PT & mean power (W) @ 60 & 180/s
Sarcopenia: EWGSOP algorithm
Validity: 1) repetition with the highest PT value may be the best indicator of maximal strength, while the average may indicate strength maintenance in sarcopenic elderly individuals 2) intraindividual variability among repetitions reflected functional decrements in sarcopenic elderly individuals compared with healthy elderly individuals 3) decreases in PT from 60/s to 180/s may reflect large losses in fast-twitch (type II) fiber function.
Dominant extremity concentric knee extension; peak torque & PT relative to body weight @ 60/s
Sarcopenia: AFFMI below 5.45 kg/m
Validity: 1) both absolute & relative PT were SGNF lower in the sarcopenic group than in the control group 2) quadriceps strength was SGNF related to aerobic capacity indices in older females.
Validity: 1) PT in the sarcopenic groups SGNF in healthy females 2) the simultaneous presence of reduced muscle mass, strength, & function is a major risk factor for falls.
Muscle weakness: using cutoff values equal to the 25th percentile PT in males & females separately
Validity: Muscle mass was not SGNF associated with physical performance in weak older adults. Measures of muscle strength may be of greater clinical importance in weak older adults than muscle mass alone.
Validity: Obesity measured by BMI, the percentage of fat mass & the abdominal fat area is not SGNF associated with functional limitations in older adults.
Bilateral concentric knee extension; PT, mean power & work normalized by body @ 60 & 180/s
Sarcopenia: EWGSOP algorithm
Validity: Sarcopenic elderly females showed low levels of performance in the lower limbs, predisposing them to greater vulnerability in functional activities that require agility & postural stability.
Sarcopenia: 1) AFFMI below 5.45 kg/m for females & 7.23 kg/m for males; 2) SMI the cutoff value scores above 37% for males & above 28% for females were considered nonsarcopenic
Validity: 1) together, nonsarcopenic group SGNF PT for the knee extensors 2) females, the nonsarcopenic SGNF PT in the knee extensors & ankle dorsiflexors 3) males, no SGNF differences in PT 4) SGNF correlation between PT & sarcopenic indices (AFFMI & SMI) in females but not in males.
Trunk flexion & extension; PT in 10 flexion. For normalization, PT was divided by body weight
–
Validity: The cutoff points for flexion & extension torque were 2.0 Nm/kg & 3.0 Nm/kg, respectively, in males, & the cutoff points for flexion & extension torque were 0.8 Nm/kg & 1.7 Nm/kg, respectively, in females.
Concentric knee extension & flexion; PT relative to body weight @ 90/s, & 180/s
Sarcopenia: EWGSOP algorithm
Responsiveness: Group-based compared to home-based exercise yielded SGNF ( 0.05) in muscle strength after 12 weeks. No SGNF changes in the control group.
Right leg concentric knee extension & ankle plantarflexion; PT @ 60/s
Frailty: using the 9-item, modified PPT
Validity: Individuals with diabesity & peripheral neuropathy are particularly likely to be classified as frail. Early identification & interventions aimed at improving lower-extremity function may be important to mitigate the early onset of functional decline.
Validity: 1) normalized PT SGNF differed between frailty groups & not frail group 2) SGNF correlation between normalized PT & PPT score ( 0.61) 3) the cutoff value was 1.46 Nm/kg.
PT peak torque, PPT Physical fitness test, SGNF significant/significantly, EWGSOP European Working Group on Sarcopenia in Older People, AFFMI Appendicular fat free mass index, SMI Skeletal muscle index, SARC-F: A simple questionnaire to rapidly diagnose sarcopenia.
Reported values of knee extension and flexion peak torque in sarcopenic and non-sarcopenic populations
Note: values in Nm are expressed as the mean SD, median [25th, 75th IQR] or mean (95% CI); $only 1 participant; *significantly different than the reference value at level 0.001.
Reported values of knee extension and flexion peak torque muscle strength in sarcopenic and non-sarcopenic populations
Note: values in Nm are expressed as the mean SD or mean (95% CI); R right leg; L left leg.
Normative values for the healthy elderly population have been presented for isometric and isokinetic knee flexion and extension and for other muscle groups [26, 27, 28], where the strength of the knee extensors and flexors decreases with age by 2% or more per year [29]. Therefore, it is difficult to determine cutoff points and reference values for multifactorial syndromes such as sarcopenia. However, our reported sarcopenia values (Table 4) are similar to the isokinetic knee extension cutoff points (94.5 Nm in males and 62.3 Nm in females), which have been reported for predicting slow gait speeds [30]. This finding suggests that these cutoff points are useful in forecasting sarcopenia because decreases in muscle strength start to lead to a slower gait speed when there is a clear sign of sarcopenia progression. One of the main limitations of our reported reference values is the absence of isokinetic strength values relative to participants’ body mass; 2 studies [18, 25] successfully found sarcopenia cutoff values (Table 3) for females in knee extension (1.46 Nm/kg) and for both sexes in trunk flexion and extension. This finding shows that body mass-related strength values might be more informative than the commonly reported raw maximal strength values in representing valid sarcopenia cutoff points.
Selecting muscle groups or muscle chains to test is an important issue in the diagnosis of sarcopenia. We found that most studies focused on the knee extensors and flexors as relevant muscle groups. This selection seems to be justified by knowledge from the rehabilitation field; the knee extensors are the first group of muscles to lose strength with any form of hypokinesis, and knee flexors decrease in strength when knee stability is disrupted. Only one study reported trunk flexion and extension strength [25], two studies reported ankle dorsiflexion and ankle plantarflexion strength [7, 15] and no studies reported hip abduction strength. Although trunk flexion and extension strength have been used to estimate sarcopenia cutoff points [25], we must mention that this test probably has lower validity than the other tests because the complex movements involved in this test are difficult and require more familiarization with the test and because trunk flexors and extensors are often shortened. Regarding ankle muscle groups, we recommend ankle dorsiflexion due to its relationship with physical performance and reported differences between healthy and sarcopenic populations [7, 15]; however, we do not recommend ankle plantarflexion, as its relations and differences have not been reported [7, 15]. The lack of evaluations of the hip abductors is quite surprising because of its relation to falls in the elderly population [31] and the relation between functional muscle activity and the strength ratios of the hip abductor muscles to the knee extensor and flexor muscles [32]. Therefore, we recommend testing of the knee extensors and flexors, which are the most frequently reported muscle groups, and suggest performing a verification study focused on the hip abductors for estimating strength in individuals with sarcopenia.
Seven studies considered multiple speeds of contraction in their approach, where most studies used 60/s as the basic speed in reporting strength. Since a higher speed of contraction (180/s) showed larger differences between sarcopenic and healthy females [13], the age-related strength decrease is larger in fast contractions than in slow contractions (60/s) [29], and the strength decrement in peak torque at 180/s may reflect greater losses in type II fiber function [8], we suggest that testing at a higher speed (180/s) might provide better reference values that have better relations with functional performance and muscle mass quality. On the other hand, we were not able to find a sufficient number of studies to estimate the cutoff points or reference values for males and females, such as the normative values for isokinetic knee extension and flexion strength at 180/s. Therefore, higher contraction speeds during isokinetic testing should be performed in future studies for identifying sarcopenia.
Another finding is that many previous studies reported isokinetic strength in groups of individuals of both sexes, which makes interpretation of the results impossible because the decreases in muscle strength are dramatically larger in males than in females; additionally, females are reported to have less muscle strength than males [27, 33, 34]. Therefore, we strongly recommend reporting isokinetic values by sex.
Conclusion
The isokinetic knee extension strength values at 60/s that can identify sarcopenia are 83 23 Nm in males and 60 7 Nm in females; in knee flexion, the values are 47 6 Nm and 36 5 Nm, respectively. Therefore, prevention interventions should be applied in potential sarcopenic populations if their strength levels are close to or below these reference values. Future studies should determine the sex-specific sarcopenia cutoff points for hip abductor, knee extensor and knee flexor isokinetic strength in relation to body mass and evaluate whether such values alone can be used as sarcopenia evaluation by itself.
Footnotes
Acknowledgments
This review was supported by the research grants of Charles University, Czech Republic (PRIMUS/19/HUM /012 and the project Q41).
Conflict of interest
The authors have no conflicts of interest to declare.
References
1.
Cruz-JentoftAJBaeyensJPBauerJMBoirieYCederholmTLandiF, et al. Sarcopenia: European consensus on definition and diagnosis. Age Ageing. 2010; 39(4): 412-423.
2.
ChenL-KLiuL-KWooJAssantachaiPAuyeungT-WBahyahKS, et al. Sarcopenia in Asia: consensus report of the Asian Working Group for Sarcopenia. J Am Med Dir Assoc. 2014; 15(2): 95-101.
3.
CawthonPM. Assessment of lean mass and physical performance in sarcopenia. J Clin Densitom. 2015; 18(4): 467-471.
4.
LloydRSOliverJLHughesMGWilliamsCA. Reliability and validity of field-based measures of leg stiffness and reactive strength index in youths. J Sports Sci. 2009; 27(14): 1565-1573.
5.
BuchnerDMCressMEDe LateurBJEsselmanPCMargheritaAJPriceR, et al. The effect of strength and endurance training on gait, balance, fall risk, and health services use in community-living older adults. J Gerontol A Biol Sci Med Sci. 1997; 52(4): M218-224.
6.
MoherDLiberatiATetzlaffJAltmanDG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann Intern Med. 2009; 151(4): 264-269.
7.
BrownMSinacoreDRBinderEFKohrtWM. Physical and performance measures for the identification of mild to moderate frailty. J Gerontol A Biol Sci Med Sci. 2000; 55(6): M350-355.
8.
CramerJTJenkinsNDMMustadVAWeirJP. Isokinetic dynamometry in healthy versus sarcopenic and malnourished elderly: beyond simple measurements of muscle strength. J Appl Gerontol. 2017; 36(6): 709-732.
9.
de OliveiraRJBottaroMMotaAM, et al. Association between sarcopenia-related phenotypes and aerobic capacity indexes of older women. J Sports Sci Med. 2009; 8(3): 337-343.
10.
KimJHChoiSHLimS, et al. Sarcopenia and obesity: gender-different relationship with functional limitation in older persons. J Korean Med Sci. 2013; 28(7): 1041-1047.
11.
KimKEJangSSLimS, et al. Relationship between muscle mass and physical performance: Is it the same in older adults with weak muscle strength? Age Ageing. 2012; 41(6): 799-803.
12.
LimaRMBezerraLMARabeloHT, et al. Fat-free mass, strength, and sarcopenia are related to bone mineral density in older women. J Clin Densitom. 2009; 12(1): 35-41.
13.
LustosaLPBatistaPPPereiraDSPereiraLSMScianniARibeiro-SamoraGA. Comparison between parameters of muscle performance and inflammatory biomarkers of non-sarcopenic and sarcopenic elderly women. Clin Interv Aging. 2017; 12: 1183-1191.
14.
MarzettiELeesHAManiniTM, et al. Skeletal muscle apoptotic signaling predicts thigh muscle volume and gait speed in community-dwelling older persons: An exploratory study. PLoS ONE. 2012; 7(2): e32829.
15.
MerriwetherENHostHHSinacoreDR. Sarcopenic indices in community-dwelling older adults. J Geriatr Phys Ther. 2012; 35(3): 118-125.
16.
Parra-RodríguezLSzlejfCGarcía-GonzálezAIMalmstromTKCruz-ArenasERosas-CarrascoO. Cross-cultural adaptation and validation of the Spanish-language version of the sarc-f to assess sarcopenia in Mexican community-dwelling older adults. J Am Med Dir Assoc. 2016; 17(12): 1142-1146.
17.
TuttleLJBittelDCBittelAJSinacoreDR. Early-onset physical frailty in adults with diabesity and peripheral neuropathy. Can J Diabetes. 2018; 42(5): 478-483.
18.
Van RoieEVerschuerenSMBoonenS, et al. Force-velocity characteristics of the knee extensors: an indication of the risk for physical frailty in elderly women. Arch Phys Med Rehabil. 2011; 92(11): 1827-1832.
19.
BinderEFSchechtmanKBEhsaniAA, et al. Effects of exercise training on frailty in community-dwelling older adults: results of a randomized, controlled trial. J Am Geriatr Soc. 2002; 50(12): 1921-198.
20.
BinderEFYarasheskiKESteger-MayK, et al. Effects of progressive resistance training on body composition in frail older adults: results of a randomized, controlled trial. J Gerontol A Biol Sci Med Sci. 2005; 60(11): 1425-1431.
21.
CramerJTCruz-JentoftAJLandiF, et al. Impacts of high-protein oral nutritional supplements among malnourished men and women with sarcopenia: a multicenter, randomized, double-blinded, controlled trial. J Am Med Dir Assoc. 2016; 17(11): 1044-1055.
22.
TsekouraMBillisETsepisE, et al. The effects of group and home-based exercise programs in elderly with sarcopenia: a randomized controlled trial. J Clin Med. 2018; 7(12): pii: E480.
23.
GadelhaABVainshelboimBFerreiraAPNeriSGRBottaroMLimaRM. Stages of sarcopenia and the incidence of falls in older women: A prospective study. Arch Gerontol Geriatr. 2018; 79: 151-157.
24.
JenkinsNDMCramerJT. Reliability and minimum detectable change for common clinical physical function tests in sarcopenic men and women. J Am Geriatr Soc. 2017; 65(4): 839-846.
25.
SasakiESasakiSChibaD, et al. Age-related reduction of trunk muscle torque and prevalence of trunk sarcopenia in community-dwelling elderly: Validity of a portable trunk muscle torque measurement instrument and its application to a large sample cohort study. PLoS ONE. 2018; 13(2): e0192687.
26.
HarboTBrincksJAndersenH. Maximal isokinetic and isometric muscle strength of major muscle groups related to age, body mass, height, and sex in 178 healthy subjects. Eur J Appl Physiol. 2012; 112(1): 267-275.
27.
NederJANeryLEShinzatoGTAndradeMSPeresCSilvaAC. Reference values for concentric knee isokinetic strength and power in nonathletic men and women from 20 to 80 years old. J Orthop Sports Phys Ther. 1999; 29(2): 116-126.
28.
BohannonRW. Reference values for extremity muscle strength obtained by hand-held dynamometry from adults aged 20 to 79 years. Arch Phys Med Rehabil. 1997; 78(1): 26-32.
29.
FronteraWRHughesVAFieldingRAFiataroneMAEvansWJRoubenoffR. Aging of skeletal muscle: a 12-yr longitudinal study. J Appl Physiol (1985). 2000; 88(4): 1321-1326.
30.
FragalaMSAlleyDEShardellMDHarrisTBMcLeanRRKielDP, et al. Comparison of handgrip and leg extension strength in predicting slow gait speed in older adults. J Am Geriatr Soc. 2016; 64(1): 144-150.
31.
LloydBDWilliamsonDASinghNAHansenRDDiamondTHFinneganTP, et al. Recurrent and injurious falls in the year following hip fracture: a prospective study of incidence and risk factors from the Sarcopenia and Hip Fracture study. J Gerontol A Biol Sci Med Sci. 2009; 64(5): 599-609.
32.
StastnyPTufanoJJLehnertMGolasAZaatarAXaverovaZ, et al. Hip abductors and thigh muscles strength ratios and their relation to electromyography amplitude during split squat and walking lunge exercises. Acta Gymnica. 2015; 45(2): 51-59.
33.
HughesVAFronteraWRWoodMEvansWJDallalGERoubenoffR, et al. Longitudinal muscle strength changes in older adults: influence of muscle mass, physical activity, and health. J Gerontol A Biol Sci Med Sci. 2001; 56(5): B209-217.
34.
FronteraWRBigardX. The benefits of strength training in the elderly. Sci Sports. 2002; 17(3): 109-116.