
Abstract
BACKGROUND:
The neuromuscular efficiency index (NME) is defined as the individual ability to generate force in relation to the muscle activation level and might be useful to the assessment of individuals with spinal cord injury (SCI) and might elucidate the modifications in strength after an SCI compared to non-disabled subjects (CG).
OBJECTIVE:
Verify if the NME of fully and partially preserved muscles discriminate men with low and high levels of SCI and a matched non-disabled CG.
METHODS:
Fifty-four men with SCI were stratified into the high (HP), and low (LP) paraplegia groups and twenty-seven non-disabled individuals were selected (CG). All subjects performed maximum strength tests in the isokinetic dynamometer for shoulder abduction/adduction (isokinetic) and trunk flexion/extension (isometric). Surface electromyography was measured to calculate the NME, and discriminant analysis was carried out to identify which NME variables would be able to discriminate HP, LP, and CG.
RESULTS:
There were no NME significant differences between groups for the primary muscles of the shoulder abduction/adduction. All NME data failed at discriminant tolerance test to compare HP from LP. The latissimus dorsi NME during trunk extension discriminated CG from HP and LP.
CONCLUSIONS:
The latissimus dorsi NME during trunk extension might be used as an assessment tool to compare SCI individuals and the non-disabled-matched controls. The authors recommend using the NME index for the analysis or comparisons between the same SCI levels.
Keywords
Introduction
Neuromuscular efficiency (NME) is defined as the individual ability to generate force in relation to the muscle activation level [1, 2, 3], and evaluates a muscle’s functional status responsiveness [2], and neural excitability [1, 2]. The NME is an index that assesses the relation of the progressive increase of the electrical activity during continuous muscle contractions [4]. The ratio is based on the force (assessed by isokinetic dynamometer, for example) divided by the measured electrical activity (e.g., root mean square measured by surface electromyography) [1, 4]. For instance, improvements in NME are explained by a greater strength associated with a lower/equal neural recruitment after an intervention [1, 3].
Muscle strength and efficiency are essential for individuals with spinal cord injury (SCI) because they are positively associated with cardiovascular capacity [5, 6], exercise tolerance [6] and muscle strength [6] and, consequently, functional independence. The NME is an important screening tool that can allow health professionals to evaluate the muscle responsiveness and functional performance arising from specific sports training programs and specific rehabilitation processes [1, 3]. The NME could be more sensitive to the neural aspects [1] and might be useful to the assessment of SCI. Therefore, the NME could play an important role in the discrimination of injury levels, as strength and neural stimulus are altered after SCI [7]. The NME might describe strength changes arising from different SCI levels. Consequently, strength variables (e.g., the absolute and relative strength to body mass) that present distinct behavior compared to non-disabled participants or could impact important outcomes as functional independence are also affected and influenced by muscle function and efficiency [8].
Recent studies showed that individuals with high paraplegia and low paraplegia have similar strength and functional independence [9], and individuals with paraplegia presented no significant differences in strength compared to non-disabled individuals [10]. However, in clinical practice, the SCI classification reveals relevant differences in sports performance, wheelchair speed, and overall functional independence, although some assessment scales are not sensitive to detect these differences [11, 12]. Therefore, SCI studies stratify the individuals with paraplegia in high (HP; T1 to T6) and low paraplegia (LP; T7 to L2) [12, 13, 14, 15, 16]. The groups differ in cardiovascular dysfunctions due to autonomic nervous system alterations and trunk instability. Likewise, functional classifications commonly used on Paralympic sports have problems in differentiating athletes, which affects the desired fair and equal competition.
Despite the utility of the NME, to the best of our knowledge, there is a lack of studies addressing the NME in the assessment of individuals with different SCI levels and comparing with control participants. The NME may properly discriminate the SCI levels and explain strength variations after the injury or due to training effects. In addition, the NME might be useful to support the functional classifications of Paralympic sports. The functional classification is in constant improvement [17, 18, 19], and an index that assesses both muscle strength and neural component might contribute to this field. Fully preserved muscles of individuals with paraplegia have already been used to establish a positive relationship between strength and functional independence [20, 21]. Nevertheless, sports performance and the optimal level of functional independence might also be influenced by partially compromised muscles (e.g., trunk muscles) [22, 23].
Therefore, the aim of the present study is to verify if the NME of fully (shoulder abduction and adduction) and partially (trunk flexion and extension) preserved muscles will be able to discriminate men with low and high levels of SCI and a matched non-disabled control group (CG). It is hypothesized that the NME will be able to discriminate non-disabled CG from individuals with SCI; and will discriminate different levels of SCI.
Materials and methods
Ethics approval
The study was approved by the ethics committee of the Sarah Network of Rehabilitation Hospitals (protocol n. 53341616.0.0000.0022), and all patients provided written informed consent to participate in the study.
Participant demographic data, considering the injury level groups. The variables are presented as median (25
and 75
percentiles). Body mass index (BMI) is shown as mean (standard deviation). Etiology and injury level are expressed in absolute values (frequency at each group)
Participant demographic data, considering the injury level groups. The variables are presented as median (25
A and B: Illustration of EMG electrodes positioning, coupled to the muscle belly of the following muscles: 1) pectoralis major; 2) rectus abdominis; 3) latissimus dorsi; 4) erectors spinae; 5) medial deltoid. C: EVA (Ethyl Vinyl Acetate) adaption made to the back of the isokinetic chair to maintain the back muscles electrodes free of contact.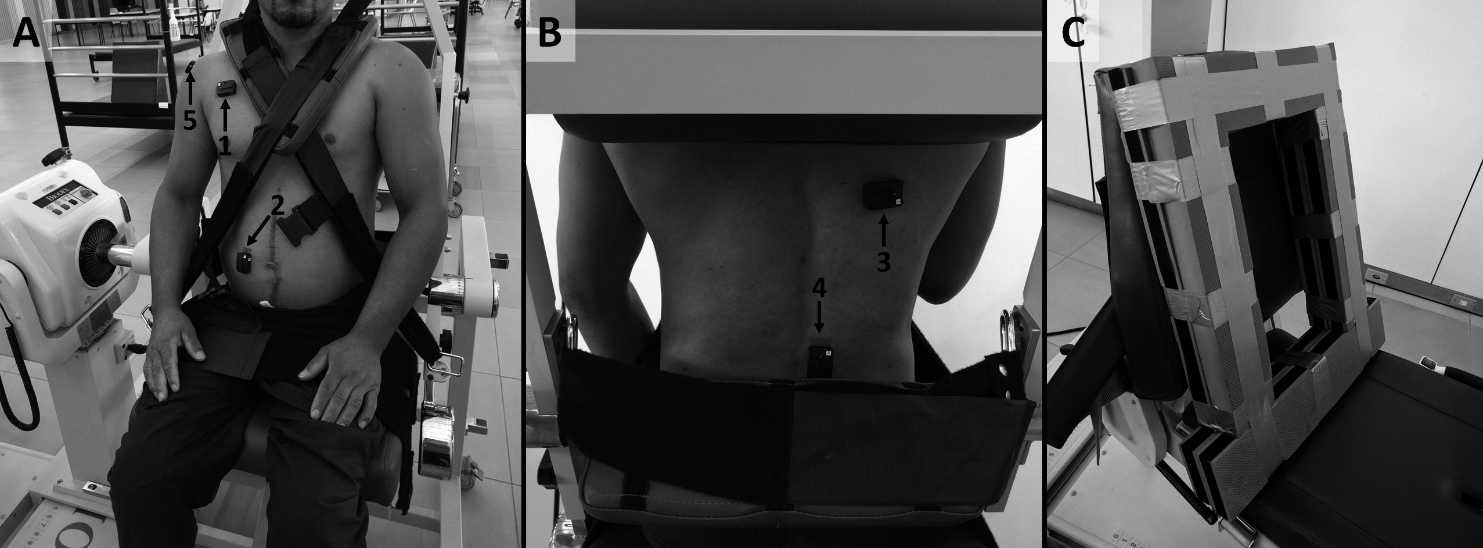
Flow diagram of maximum strength tests in isokinetic dynamometer (isokinetic and isometric test) performed by the groups high paraplegia, low paraplegia, and control. ROM: range of motion; OMNI-RES: perception scale of effort for strength exercise.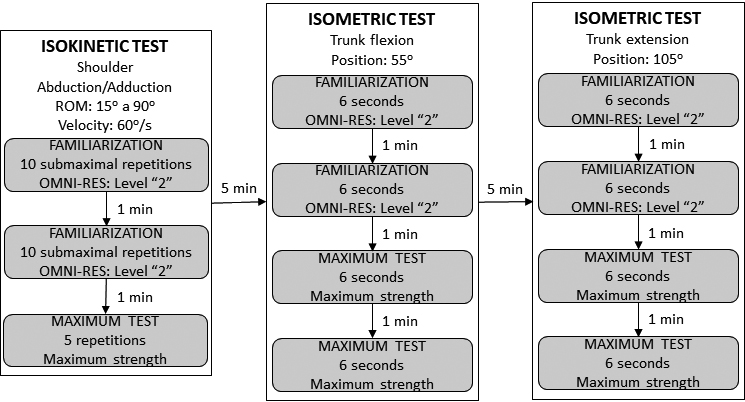
A convenience sample of fifty-four individuals with SCI was recruited from the rehabilitation program of a Network Centre of Rehabilitation Hospitals. Twenty-seven individuals without SCI composed by male adults matched by age, body mass, and height was selected as the CG, thus totaling 81 participants in the present study (Table 1).
The inclusion criteria were: 1) male, 2) diagnosed with traumatic SCI paraplegia, 3) at least 6 months since the injury, 4) complete motor lesion (ASIA Impairment Scale, AIS A or B) [24], 5) clinical stability (patients evaluated by medical staff to participate in the rehabilitation program) and 6) manual wheelchair user. Participants were excluded if they had a history of metabolic disorders, cardiovascular, cardiac, or orthopedic surgery that would hamper performance in functional tests or an adequate exercise technique. The data was achieved in the participant’s medical records. Subjects were sequentially assigned to a high (HP, T1 to T6) or low paraplegia group (LP, T7 to L3) until reaching the estimated sample size.
Procedures
Muscle strength assessment
Three maximum strength tests were carried out in a fixed order on an isokinetic dynamometer (Biodex System 4, Biodex Medical, Shirley, NY). The device was calibrated according to the manufacturer’s instructions and the rotational axis aligned with the anatomical points of the shoulder and hip. Straps and belts were used to stabilize the trunk, pelvis, arm, and hands to prevent compensatory movements (Fig. 1A). Before testing, each exercise was demonstrated and executed to establish the range of motion (ROM) and for proper positioning of the participant relative to the dynamometer.
The maximum tests were performed on a fixed order and with a 5-minute rest interval between them, and a standardized verbal encouragement was adopted by the same assessor. For analysis purposes, the highest peak torque in each movement was considered for the comparison between groups and expressed in Newton-meters (N.m).
The participants performed three maximum strength tests (Fig. 2):
Concentric shoulder abduction and adduction at 60 Two tests of Maximum voluntary isometric contraction (MVIC): trunk flexion and trunk extension: strength assessment consisted of 2 familiarization sets and two 6-second MVIC sets separated by 1-minute intervals. The familiarization sets were submaximal (level 2 on the OMNI-RES) [25]. For the two MVIC sets, participants were instructed to execute a continuous maximum contraction and avoid bouncing movements. The highest peak torque between the two MVIC sets was used for analysis. Participants performed the trunk flexion test with their arms relaxed, and for trunk extension was instructed to rest their hands on the belts stabilizing the trunk. These adjustments were made to prevent participants from using the upper limb during the movement.
A portable electromyograph with a wireless system (Trigno
The same assessor positioned the electrodes on the participant’s dominant side, in the following muscles: pectoralis major, rectus abdominis, medial deltoid, latissimus dorsi, and erector spinae muscles. The guidelines of SENIAM (Surface Electromyography for the Noninvasive Assessment of Muscles) [26] and standards proposed by Criswell [27] (Fig. 1A and B) were adopted. An adapted Ethyl Vinyl Acetate support was developed and positioned in the backrest of the dynamometer’s chair, in order to avoid the contact of the sEMG electrodes positioned in the latissimus dorsi and erector spinae muscles with the chair (Fig. 1C).
The sEMG and the dynamometer were synchronized by an analog adapter (Delsys, Inc). For each muscle, root mean square (RMS, in V) values were calculated in a 70%-time window centered on the peak torque. The RMS was used to estimate the NME, according to the following equation [7]:
where, peak torque in N.m and RMS in V.
The primary muscles responsible for each movement were selected for the NME calculation, as follow: (1) shoulder abduction: medial deltoid; (2) shoulder adduction: pectoralis major and latissimus dorsi; (3) trunk flexion: rectus abdominis; (4) trunk extension: latissimus dorsi and erector spinae.
Statistical analysis
Sample size was calculated (G*Power software version 3.1.9.2) considering a multivariate analysis of variance (MANOVA), with effect size of 0.12,
The Shapiro-Wilk test was used to assess the data normality assumptions. To compare groups means, the ANOVA with the Bonferroni post hoc test (
Discriminant analysis was carried out using the Wilk’s Lambda method in order to identify which of the six NME indices (medial deltoid for shoulder abduction; pectoralis major and latissimus dorsi for shoulder adduction; rectus abdominis for trunk flexion; latissimus dorsi and erector spinae for trunk extension) would be able to discriminate the SCI groups (HP and LP) and the CG. The matrices of homogeneity were tested using the Box’s M test of equality of covariance. The canonical correlation was applied to measure the association between the discriminant function and the variables. Subsequently, a classificatory analysis and cross-validation demonstrated the allocation accuracy for each discriminant analysis.
The IBM SPSS statistical package (version 22.0; SPSS Inc, Armonk, NY) and Matlab (R2014.A, The MathWorks Inc, Natick, MA, US) were used. Statistical significance was set at 5% (
Results
The CG presented significantly higher body mass and height compared to HP and LP. HP and LP did not differ in the main demographic data (
Peak torque and normalized RMS
The peak torque of shoulder abduction and adduction were significantly lower in the HP compared to the LP and CG (58.2 N.m vs. 71.3 N.m and 68.7 N.m, respectively;
Descriptive data of absolute muscle strength (N.m) for high paraplegia (HP), low paraplegia (LP) and control (CG) groups. Shoulder adduction peak moment is presented as mean (standard deviation). The other variables are shown as median (25
and 75
percentiles)
Descriptive data of absolute muscle strength (N.m) for high paraplegia (HP), low paraplegia (LP) and control (CG) groups. Shoulder adduction peak moment is presented as mean (standard deviation). The other variables are shown as median (25
There were no significant differences between groups on sEMG activity (RMS) of the primary muscles (shoulder abduction and adduction;
Normalized Root Mean Square (RMS, V) and Neuromuscular Efficiency (NME, N.m/V) of the high paraplegia (HP), low paraplegia (LP) and control (CG) groups. Data are presented as median (25
There were no significant differences on NME between the HP, LP, and CG for the primary muscles of the shoulder abduction (medial deltoid) and adduction (pectoralis major and latissimus dorsi). Likewise, there were no significant differences on NME between HP and LP for trunk flexion (rectus abdominis) and extension (latissimus dorsi;
All NME data did not meet the discriminant tolerance test in the comparison between HP and LP. The NME of medial deltoid (shoulder abduction), pectoralis major and latissimus dorsi (shoulder adduction), rectus abdominis (trunk flexion) and erector spinae (trunk extension) also did not meet the discriminant tolerance test in the comparison between groups. The NME of the latissimus dorsi during trunk extension discriminated the CG from the HP and LP (function coefficient
Discussion
The aim was to compare the NME of men with different levels of SCI with non-disabled-matched controls and to verify whether the NME would be able to discriminate these groups. The rectus abdominis NME during trunk flexion, and the latissimus dorsi NME during trunk extension were different between CG and SCI groups. In addition, the latissimus dorsi NME during trunk extension was the best discriminator between SCI groups and between individuals with SCI and the CG. However, contrary to our hypothesis, the muscle efficiency of the targeted muscles was the same for individuals with high and low paraplegia since the NME did not discriminate the groups.
We demonstrated significant differences in trunk strength (flexion and extension) between HP vs. LP vs. CG. Trunk flexion/extension MVIC on an isokinetic dynamometer was a useful assessment, as previous studies did not find differences between the strength of preserved muscles in individuals with SCI compared with individuals without SCI [20, 21, 28, 29, 30]. The responsiveness for detect trunk flexion/extension strength difference between SCI injury level and non-disabled individuals allows using this test to assess interventions (e.g., training or rehabilitation) or to predict outcomes (e.g., functional independence cutoff points). The abdominal muscles are innervated by the intercostal nerves (T7 to T11) and the erector spinae by spinal nerves, with both muscles determinant to trunk balance. The paraplegia groups were stratified considering these characteristics and, thus, significant differences between groups on peak trunk flexion/extension torque were expected.
The rectus abdominis (during trunk flexion) and latissimus dorsi NME (during trunk extension) were significantly different only between CG and paraplegia groups. Moreover, the latissimus dorsi during the trunk extension was the best variable to discriminate paraplegia and CG. The higher latissimus dorsi is fully preserved in HP and LP. Hence, this muscle presents a higher innervation (thoracodorsal nerve, C6 to C8) compared to the erector spinae and rectus abdominis, this aspect might explain the equivalent RMS values between groups. However, the trunk extension peak torque was significantly higher (around six times) in CG compared to the paraplegia groups. Prime movers of hip extension (e.g., hamstrings and biceps femoris) might have influenced the greater peak torque in the CG. Consequently, latissimus dorsi during trunk extension presented a higher NME and, might have influenced the discrimination analysis.
Although NME was not a discriminate outcome able to differentiate the SCI levels, the erector spinae NME during trunk extension was higher in the HP compared to the LP. The erector spinae RMS was two times higher in the LP compared to the HP. However, the peak torque produced by the LP was only 33% higher and, consequently, the erector spinae NME during trunk extension was lower in the LP (NME equal peak torque divided by RMS). Since the absolute muscle strength is deemed to be important for trunk balance and functional activities [21, 23, 31, 32], we speculate that this outcome might be prioritized for functional independence analysis, regardless of the reduced NME and the amount of muscle activation found in lower SCI levels.
Regarding shoulder abduction/adduction, the NME of the primary muscles was not different between groups, although LP and CG presented higher peak torques compared to the HP. The muscles involved in the shoulder abduction/adduction are fully preserved in individuals with paraplegia, as their innervations are originated above the compromised SCI levels [33]. NME assesses the neural and muscular adaptations of a specific muscle group [2] and changes in the deltoid fiber types have been reported in different SCI levels [34]. Our findings demonstrated that RMS of abduction/adduction muscles were not different between groups, but peak torque differences between groups were not expected. Previous studies have demonstrated similar shoulder strength between this injury levels [9, 10, 21], and participants of the present manuscript were assessed with their trunk stabilized, minimizing the support function of the trunk muscles. These muscles provide adequate support of the shoulder girdle, and, probably, could help to improve the shoulder peak torque of individuals with paraplegia in the shoulder strength test [29, 30].
Some characteristics must be considered in the NME analysis of subjects with SCI. The order of motor unit’s recruitment of a given muscle is the same as before the SCI [35]. However, the recruitment does not appear to be as precise and as predictable as before the injury since selective changes in the electrophysiological properties of a given motoneuron can partially disrupt this order [35]. The frequency of motor unit firing and the amplitude of motor unit potentials might also influence the sEMG signal. Although there is scarce information on how these variables are affected by duration or time of SCI, [35] it is suggested that the frequency of motor unit’s firing ratio is lower after the SCI [36, 37]. The literature data for the amplitude of motor unit potentials are mixed, as the amplitude increase over time in some units, but remain relatively constant or slightly declined in other units [35]. Finally, the Golgi tendon organ was previously linked to reductions in the RMS due to a mechanism of neural inhibition [38, 39]. Individuals with a higher level of SCI are expected to have cutaneous hyperreflexia, spasms activity and clonus, influenced by proprioceptive receptors [40, 41] and, consequently, these aspects might affect the EMG data.
It is probable that due to the aforementioned factors, studies adopting the NME as an outcome are scarce [42]. Nevertheless, NME is important to ascertain the functional status of different muscle groups (EMG-torque ratio) [2]. However, the index has not been responsive enough to detect neural and strength changes between groups in our study. The strength of individuals with SCI is dependent on the neural stimulus preserved above the injury level, and depending on the injury level, the restrictions on the amount of motoneuron activation can be proportionally different compared to those on muscle strength. Our findings evidenced that NME may not explain these alterations between different SCI levels, considering that muscle efficiency is dependent on a greater force production with less neural activation [42]. We would recommend that this index might be used as an evaluation measure of performance after a period of training to compare subjects with the same injury level. Future studies may also use the NME index as a predictor outcome for functional independence.
Study limitations
During trunk flexion/extension strength test, other muscles involved in the hip flexion/extension were probably recruited and could have influenced the peak torque differences between CG and paraplegia groups. We adopted a strength testing composed by concentric contractions and a single velocity (60
Conclusions
Our findings demonstrated that NME of the rectus abdominis during trunk flexion, and of the latissimus dorsi during trunk extension were different between CG and SCI groups. However, the latissimus dorsi NME during trunk extension was the best discriminator between SCI individuals and the non-disabled matched controls and might be used as an assessment tool to compare these groups. In addition, the NME of fully and partially preserved assessed muscles was not a discrimination variable to discriminate high and low paraplegia, demonstrating that muscle efficiency is the same regarding different injury levels. Consequently, regarding SCI, we would recommend using NME to assess only the subjects in which present the same injury level.
Author contributions
CONCEPTION: Frederico Ribeiro Neto and Rodrigo L. Carregaro.
PERFORMANCE OF WORK: Frederico Ribeiro Neto and Rodrigo R. G. Costa.
INTERPRETATION OR ANALYSIS OF DATA: Frederico Ribeiro Neto and Rodrigo L. Carregaro.
PREPARATION OF THE MANUSCRIPT: Frederico Ribeiro Neto, Rodrigo R. G. Costa, Ricardo A. Tanhoffer, Josevan C. Leal, Martin Bottaro and Rodrigo L. Carregaro.
REVISION FOR IMPORTANT INTELLECTUAL CONTENT: Frederico Ribeiro Neto, Rodrigo R. G. Costa, Ricardo A. Tanhoffer, Josevan C. Leal, Martin Bottaro and Rodrigo L. Carregaro.
SUPERVISION: Frederico Ribeiro Neto and Rodrigo L. Carregaro.
Ethical considerations
The study was approved by the ethics committee of the Sarah Network of Rehabilitation Hospitals (protocol n. 53341616.0.0000.0022), and all patients provided written informed consent to participate in the study.
Funding
The authors report no funding.
Footnotes
Acknowledgments
The authors have no acknowledgments.
Conflict of interest
We certify that no party has a direct interest in the results of the research supporting this article or has or will confer benefit on us or on any organization with which we are associated.