
Abstract
BACKGROUND:
Familiarization is a fundamental step for a proper maximum strength testing. However, there is a lack of evidence regarding familiarization protocols suitable for isokinetic assessment in men with spinal cord injury (SCI).
OBJECTIVE:
The aim was to compare different familiarization protocols (sessions and sets) and their influences on a maximum isokinetic strength test in individuals with SCI.
METHODS:
Thirty-six men with SCI were enrolled and were randomly assigned to one of three groups that performed one (F1set), two (F2set) or three (F3set) sets of familiarization on an isokinetic dynamometer. Each group repeated familiarization and maximum strength tests on three different days (D1, D2 and D3) with 48 to 72-hour intervals. Multiple one-way analysis of variance was performed to compare the familiarization protocols. For measurement agreement, the intraclass correlation coefficient (ICC) with Bland-Altman plots were used.
RESULTS:
F2set had no statistically difference in peak torque between testing days, or between F1set and F3set. F1set and F3set differed between days for shoulder abduction and extension. ICC was significant and high (ICC
CONCLUSIONS:
One familiarization session composed by 2 sets of submaximal exercise could be adopted as a suitable protocol prior to a maximal strength testing in men with SCI.
Familiarization groups demographics. Each familiarization group was formed by 4 tetraplegics, 4 high paraplegics and 4 low paraplegics men. The variables are exhibited by median (percentiles 25 and 75). Height is show by mean (standard deviation) and etiology is expressed in absolute values (frequency at each group)
Familiarization groups demographics. Each familiarization group was formed by 4 tetraplegics, 4 high paraplegics and 4 low paraplegics men. The variables are exhibited by median (percentiles 25 and 75). Height is show by mean (standard deviation) and etiology is expressed in absolute values (frequency at each group)
No significant difference between familiarization groups. Demographic outcomes were not significant different between males with tetraplegia, high paraplegia and low paraplegia and between familiarization groups. BMI: body mass index; CG: control group; F1set: 1 familiarization set; F2set: 2 familiarization sets; F3set: 3 familiarization sets; TSI: time since injury.
A spinal cord injury (SCI) leads to substantial lifestyle changes, including loss of independence for activities of daily living [1, 2]. The upper limbs must be strong enough to provide self-care, mobility, transfers and activities at work [3]. Hence, strength training is one of the most common interventions adopted to increase functional independence during rehabilitation of patients with SCI [4, 5], and considered by Warburton et al. [6] an essential intervention for this population. Previous studies have demonstrated that strength training improves functional independence and is associated with increased cardiovascular conditioning [2, 7, 8], exercise tolerance [8], muscular endurance [8], reduction of shoulder pain [9] and improved health status [5]. In this context, for proper recommendations of neuromuscular rehabilitation in this population, there is a need for a reliable and accurate assessment of muscular performance parameters to determine the capabilities and potential limitations of men with SCI.
Several studies have reported strength measurements in men with SCI using isokinetic devices. The isokinetic dynamometer has been considered the gold standard for muscle strength assessment [10]. This equipment is often used to assess muscle function and provides detailed and accurate information on torque, position, and limb velocity [11] in different populations. It is well recognized that individuals with SCI present trunk stabilization deficits, which imposes difficulties for upper body strength measurements [12, 13, 14]. Furthermore, proper dynamometer positioning is influenced by an absence of lower body strength. However, there is a lack of information regarding suitable familiarization protocols to be adopted prior to isokinetic strength assessment in this population [2, 12, 15, 16, 17, 18, 19, 20, 21].
Isokinetic testing familiarization in men with SCI is currently performed with different methodologies. Previous studies have adopted dynamic strength testing familiarization composed of two [15, 17] or three [8, 22] submaximal repetitions while other studies have performed two minutes of concentric contractions at 180
Methods
Participants
Thirty-six men with SCI were enrolled in the study (Table 1). They were recruited in the rehabilitation program of a Network Centre of Rehabilitation Hospital. Inclusion criteria were: 1) male sex (over 18 years), 2) diagnosis of traumatic SCI, 3) complete motor lesion (ASIA Impairment Scale, AIS A or B) [13, 14], 4) a wheelchair user and 5) have no prior knowledge or have never performed isokinetic testing. Individuals were excluded if they presented a history of metabolic disorders; or cardiovascular or orthopaedic surgery that could impose restrictions during the performance of the tests.
Physical activity level was estimated by the amount of hours expended in any sport and/or physical exercise that were oriented by a Physical Educator or Physiotherapist, according to Janssen et al. [29]: (1) Sedentary (0 hours per week); (2) Moderately active (1 to 3 hours per week); (3) Active (3 to 6 hours per week); (4) Very active/athlete (more than 6 hours per week). This study was approved by the Institutional Ethics Committee (protocol n. 53341616.0.0000.0022) and all individuals signed a written informed consent form.
Procedures
Familiarization protocols
Subjects were randomly assigned to one of three groups that performed one (F1set,
Three days of maximum strength test using isokinetic dynamometer. Familiarization were conducted with a level of “2” by OMNI scale, 60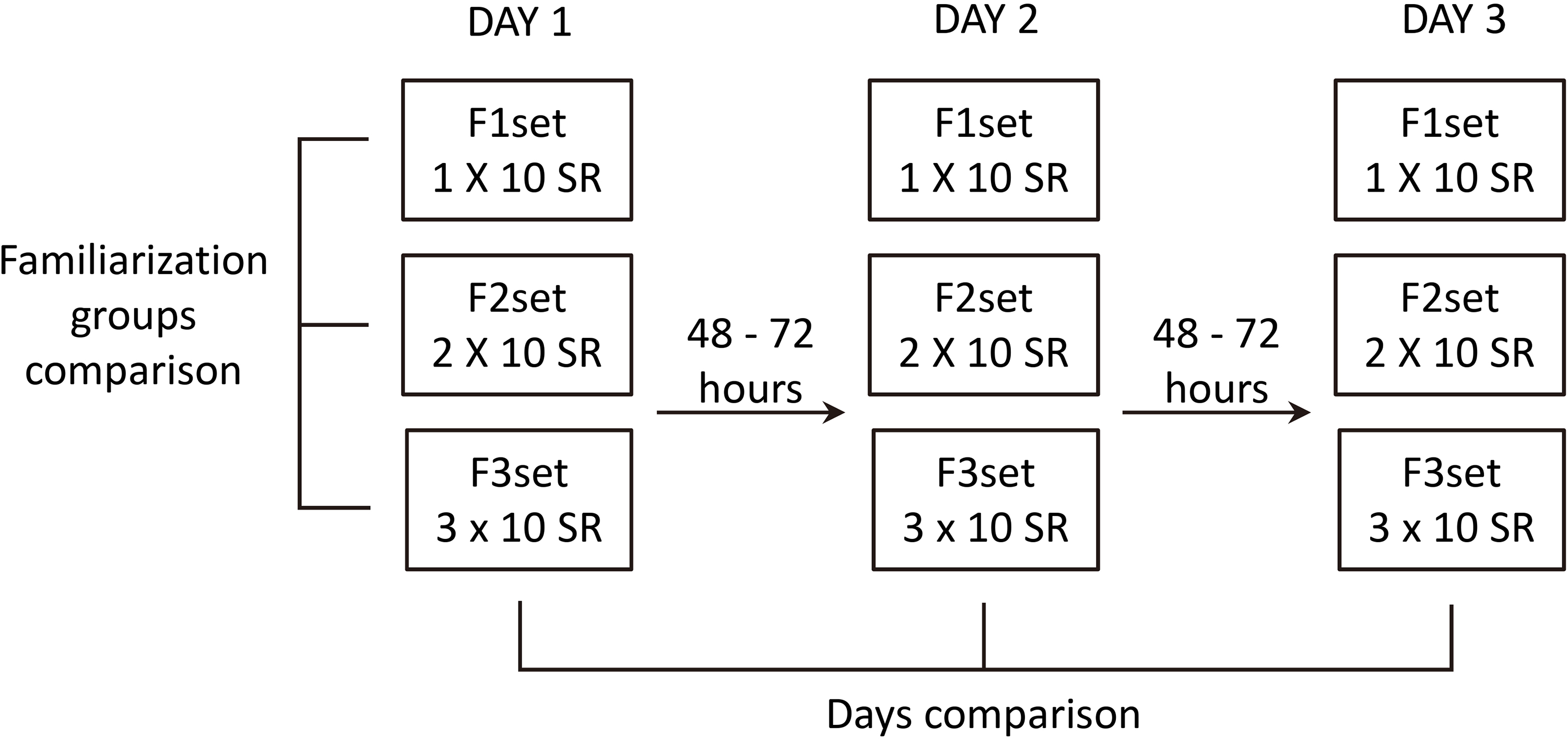
Maximum strength testing of elbow flexion and extension, shoulder abduction and adduction, and shoulder flexion and extension were performed on a Biodex System 4 isokinetic dynamometer (Biodex Medical, Shirley, NY). Calibration was performed according to the manufacturer’s instructions. The dynamometer rotational axis was aligned with the anatomical points of the elbow and shoulder joints. Reference points were the lateral epicondyle, humeral head and humeral tubercle. All points of force application were positioned at the hand. Individuals with tetraplegia had their hands fixed with neoprene strips. These procedures were adapted from Kotajarvi and colleagues [16] and used by previous studies [15, 17]. Strips and belts were used for stabilization of the trunk, pelvis, arm and hands, in order to avoid compensatory movements [35].
Only the dominant limb was assessed, at a velocity of 60
End ROM of each exercise was measured with a goniometer and based on this value, ROM of each exercise was calculated by the dynamometer. Weight of the upper limb and the dynamometer lever arm was standardized in relation to the starting position of each exercise. For reliability purposes, the chair settings used on the first test day were recorded and replicated on the following sessions. A rest interval of 5 minutes was provided between shoulder and elbow testing (Fig. 2).
Maximum strength test sequence in isokinetic dynamometer for extension/flexion of the elbow, abduction/adduction and extension/flexion of the shoulder. F1set: group with 1 set of familiarization; F2set: group 2 sets of familiarization; F3set: group with of 3 sets of familiarization.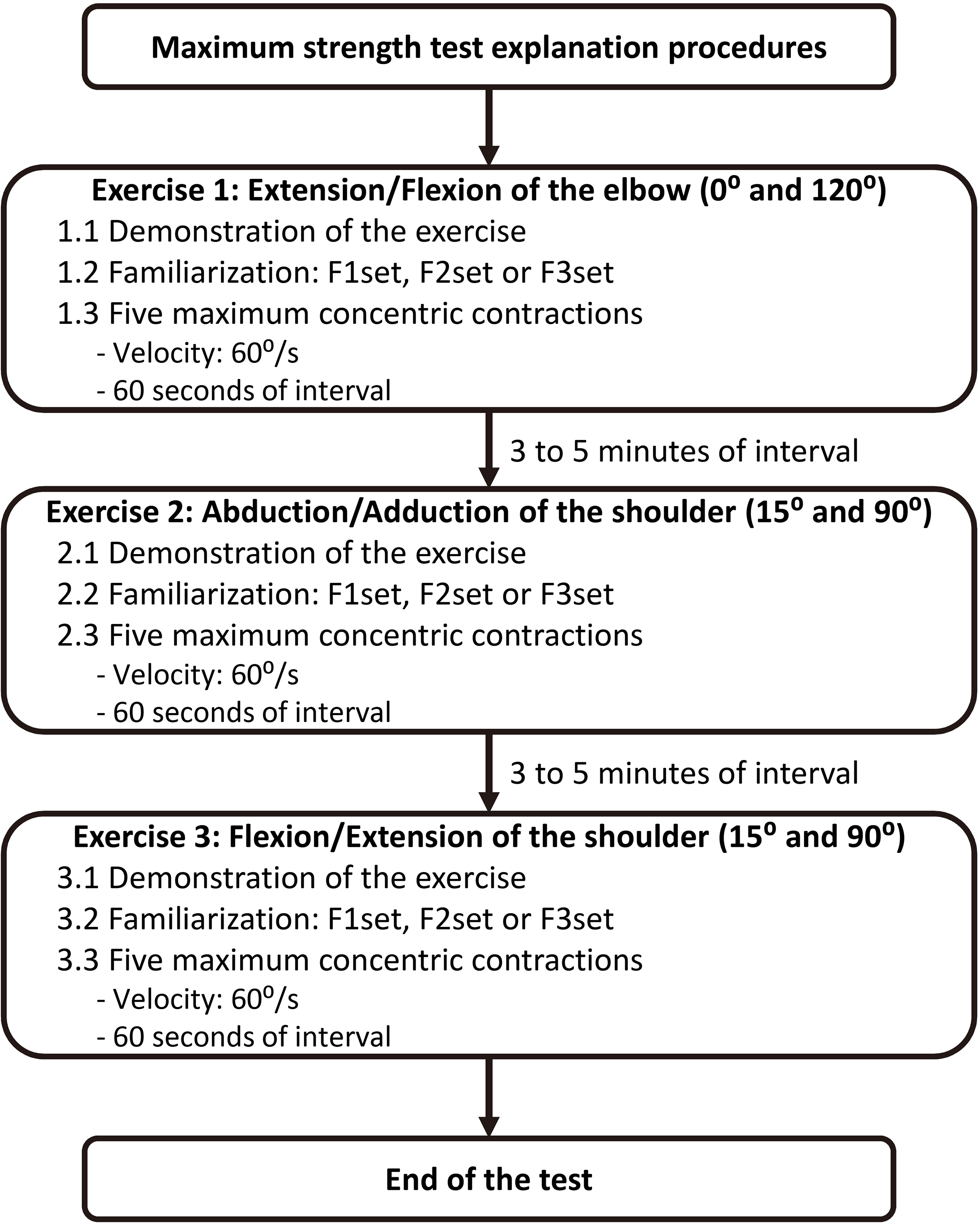
An a priori sample size calculation was performed based on peak torque outcome and considering a three stage by one-way analysis of variance (ANOVA), with a large effect size (0.80),
Peak torque (N.m) of six concentric movements during each familiarization group (F1set: 1 familiarization set; F2set: 2 familiarization sets; F3set: 3 familiarization sets). Values presented in mean (standard deviation)
Peak torque (N.m) of six concentric movements during each familiarization group (F1set: 1 familiarization set; F2set: 2 familiarization sets; F3set: 3 familiarization sets). Values presented in mean (standard deviation)
No significant difference between familiarization groups.
Bland and Altman method and intraclass correlation coefficient (ICC) comparing isokinetic exercises between testing days (D1, D2 and D3) for familiarization groups (F1set, F2set and F3set). Confidence interval was set on 95% (95% CI)
The Shapiro-Wilks normality test was used to assess the distribution of variables. One-way analysis of variance (ANOVA) was performed to compare familiarization protocols. When the F test was significant, a Bonferroni test for multiple comparisons was used (height, peak torque and agonist/antagonist concentric ratios). The Bartlett test of homogeneity of variances was used while the Kruskal Wallis test with Mann-Whitney post hoc was used for non-parametric variables (age, physical activity level, time since injury, body mass and body mass index). A General Linear Model for repeated measures ANOVA with the Bonferroni post hoc test was used to compare strength between days.
With the purpose of analyzing the measurement agreement between the familiarization protocols, the intraclass correlation coefficient (ICC) with Bland Altman plot was used to compare the first (D1), second (D2) and third (D3) days of familiarization. The ICC was classified based on Cicchetti standards: below 0.40 – level of clinical significance is poor; 0.40 to 0.59 – fair; 0.60 to 0.74 – good; 0.75 to 1.00 – excellent [36]. Confidence intervals of 95% (95% CI) was used between comparisons.
The Outlier Labeling Rule was used to detect outliers and discrepant results [37, 38]. The outlier’s values were calculated by the difference between percentiles 25 and 75 multiplied by a factor (2.2). This result is subtracted from percentile 25 and added to percentile 75.
The IBM SPSS statistical package (version 22.0) and G*Power statistical power software (version 3.1.9.2; Universität Kiel, Germany) were used. Statistical significance was set at 5% (
Comparison between protocols
There were no significant differences in peak torque between groups for each tested day (Table 2).
Comparison between testing days
For the F1set group, peak torque was significantly lower on the first day when compared to the second and third days for shoulder abduction (
Means and SDs of three agonist/antagonist concentric movements ratios of peak torque for familiarization groups on three days
Means and SDs of three agonist/antagonist concentric movements ratios of peak torque for familiarization groups on three days
No significant difference between familiarization groups.
For the F2set group, no significant differences were found for peak torque or agonist/antagonist ratio between exercises and testing days (
For the F3set group, significantly lower peak torque was produced on D1 compared to D3 for shoulder abduction (52.0 vs 56.9 N.m,
ICC values were significant and were classified as excellent for all three familiarization protocols, for all tested days (Table 3). Additionally, the Bland Altman plot demonstrated that both the difference between the means and the intervals around these differences (
The present study demonstrated that a familiarization session consisting of two sets of shoulder abduction/adduction, flexion/extension or elbow flexion/extension did not influence muscle strength testing on subsequent days. Moreover, the agonist/antagonist ratio did not differ between familiarization protocols. Thus, our findings demonstrated that one single day of familiarization composed of two sets could be suitable and applied prior to a maximum strength tests of men with different levels of SCI on an isokinetic dynamometer. Moreover, one session with two sets presented better results as a familiarization procedure compared to the other familiarization protocols analyzed, demonstrating that an extensive familiarization is not needed.
The F2set presented no peak torque differences between days. In contrast, the F1set and F3set presented lower peak torques for shoulder abduction and extension on the first day when compared to D2 and D3. The F2set intraclass correlation coefficient was high (over 0.84, classified as excellent) between days one and three, for all exercises, indicating that the non-significant difference between days and the consistency and agreement of the results were not influenced by the variability of the strength measurements [39]. The Bland Altman plot also confirmed the agreement between measurements of the familiarization protocol for the F2set. Hence, it is possible to assume that a difference between the means and the intervals around these differences were small. Therefore, the adoption of two sets prior to a strength test on a single day may be sufficient as a familiarization process for this population.
Investigations on the number of testing days for familiarization is not only important to understand learning effects and adaptations to muscle testing procedures, but also to exclude the possibility of an underestimation of muscle performance or overestimation of strength gains. Although Moritani and de Vries [40] showed a prevalence of neural factors responsible for strength gains up to four weeks of training, recent studies [41, 42] have reported earlier involvement of hypertrophic components. In the present study, the maximum interval for each familiarization group was one week, minimizing the potential for strength gains due to these factors.
We found no significant peak torque differences between testing days when F1set, F2set or F3set were compared. It is worthy to note that most previous studies have adopted lower familiarization exercise volumes. For instance, two [15, 17] and three [8, 22] submaximal repetitions have been reported as familiarization. However, previous studies did not report the protocol intensity. Therefore, it is important to control intensity in order to avoid deleterious effects such as fatigue, before beginning a maximum strength test. The present study standardized intensity based on the OMNI scale for perceived exertion during strength exercises [30]. We assumed that a pre-determined submaximal intensity was important to minimize the occurrence of fatigue, especially in a SCI population who present strength deficits influenced by trauma.
The velocity adopted in the present study for familiarization was the same as the maximum strength test. Previous studies have reported that 60
Study limitations
The standardized intensity based on the OMNI imposed some limitations. The individuals had never used this scale during strength training or testing, thus, it is possible that the association of perceived exertion with a strength exercise could have influenced our intensity control.
Conclusion
The present study demonstrated that one session, composed of 2 sets of submaximal resistance exercise performed with a level “2” on the OMNI scale can be used as a familiarization protocol prior to a maximal isokinetic strength testing of the elbow and shoulder of men with SCI. These findings have important practical implications for allied health professionals with the aim to assess muscle strength or prescribe strength training to men with SCI.
Footnotes
Conflict of interest
The authors report no declarations of interest.