
Abstract
BACKGROUND:
The ratio of hamstring to quadriceps strength (H/Q), from isokinetic testing, is often used to guide training or rehabilitation.
OBJECTIVES:
The primary objective was to develop an assessment protocol that produces reproducible H/Q data in a single testing session.
METHODS:
Twenty-four healthy subjects, 16 women and 8 men, were tested using a reliability study design (2 sessions, 5 repetitions). The main outcome measure was the dynamic control ratio at 60
RESULTS:
Single-session DCR60 data were reproducible (
CONCLUSIONS:
Reproducible DCR60 values may be derived from a single testing session of the hamstrings (in eccentric mode) and the quadriceps (in concentric mode). We recommend collecting five repetitions, and averaging the data for repetitions 2–5.
Introduction
Strength and power of both the hamstrings and quadriceps muscle groups is often a target of rehabilitation following knee injuries or muscle strain injuries [1, 2]. One of the rehabilitation goals may be to normalize the ratio of hamstring-to-quadriceps strength (HQR), derived through isokinetic testing. It has been suggested, however, that the dynamic control ratio (DCR), which is obtained by dividing the peak eccentric moment of the hamstrings by the peak concentric moment of the quadriceps, has a unique differentiating role [3], and may provide the best reflection of the functional, antagonistic actions of these muscles [4]. From a clinical perspective, therefore, having an assessment protocol that can provide reproducible data for the DCR with a realistic minimal detectable change (MDC), using the fewest number of isokinetic measures, would allow the clinician to monitor an individual patient’s progress over time in an efficient way.
Several previous studies have shown that isokinetic testing of the quadriceps and hamstrings can produce reproducible data [1, 4, 5]. Impellizzeri et al. [4], for example, found that peak moment (PM) measurements during isokinetic testing of the hamstrings and quadriceps are highly reproducible over a range of velocities (ICC
While isokinetic measurements at the knee are commonly performed with participants in a seated position (hip flexion 70–85
While the DCR is useful as a primary measure to guide rehabilitation, it is likely not reflective of the full functional capacity of these muscle groups. In addition to the position of the hip (discussed above), the velocity of the movement (including, but not limited to differences between concentric and eccentric movements) and the position of the knee (which affects the length of the muscles and their moment arms at the knee) are also likely to affect the expression of muscular force [11]. Traditional isokinetic testing looks at the PM generated at a specific joint angular velocity [12], but typically does not account for the position at which that PM was generated [13]. Representing muscle function at the knee across multiple joint angular velocities and joint positions, therefore, would add to the information provided by the DCR.
The primary objective of this study, therefore, was to develop a clinical assessment protocol that allows for the acquisition of reproducible DCR data at 60
Methods
Participants
A sample of 28 healthy participants (mean age: 25 yrs; SD: 3 yrs; range: 19–35 yrs) were recruited via social media. Four of the participants withdrew from the study – two due to knee pain experienced during the first testing session, and two due to an inability to attend their second testing session within the prescribed time frame (see procedures, below) – leaving 24 participants, 16 women and 8 men. Based on the method described by Shoukri et al. [14], it was determined that only 15 participants were required to target a reliability coefficient
Subject demographic and anthropometric information (N
24)
Subject demographic and anthropometric information (N
*N
Eligible participants were required to be between the ages 18–35 years, and to understand verbal and written English or French. Exclusion criteria were as follows: any history of injury or surgery affecting the knee; a history of hamstrings or quadriceps injury; any lower extremity injury or surgery that affected daily function within the last 12 months; any cardiovascular, neurological, cognitive, systemic disease, or impairment that may have interfered with isokinetic testing of the knee.
Participants were asked to complete the International Physical Activity Questionnaire long form – past 7 days (IPAQ-L7S) prior to the first testing session. The IPAQ-L7S measures the level of physical activity over the previous week, and has been shown to have acceptable measurement properties for both clinical and research purposes [15, 16]. Participants were also instructed to maintain their regular physical activity between the two testing sessions, but not to take part in any new vigorous physical activity for the duration of the study period. We were not able to collect the IPAQ-L7S data from one participant due to time constraints during the testing sessions.
The experiments were undertaken with the understanding and written consent of each participant, and that the study conforms with The Code of Ethics of the World Medical Association (Declaration of Helsinki), printed in the British Medical Journal (18 July 1964). Ethics approval for this study was received from the research ethics board of the CRIR and the CIUSSS Centre-Ouest-de-l’Île-de-Montréal (CRIR-1139-0316).
Participants completed two testing sessions within a 7-day interval, with a minimum of 48 hours between sessions to allow for recovery. Isokinetic testing was done for knee flexion (hamstrings) and extension (quadriceps) on the dominant leg (preferred leg to kick a ball), using a CSMI Humac Cybex NORM isokinetic dynamometer (Computer Sports Medicine Inc., Stoughton, MA). The participants were tested in prone, with a pad under the pelvis, placing the hips in
Each session began with a 5-minute warm-up on a stationary bicycle, at a low-moderate intensity. The participant then lay prone on the dynamometer (seatback laid flat), with straps placed around the pelvis and thigh to prevent them from moving during testing. The dynamometer software was set for a knee ROM between 10
The testing protocol followed a standardized, non-randomized protocol for isokinetic testing of the knee. Under each condition, participants had to complete 5 submaximal (
Data analysis
The raw data acquired from the dynamometer software were sampled at 100 Hz, and included all 5 repetitions for the hamstrings and quadriceps at each velocity. As this software ‘zeros’ the moment data at the impact point with the digital stop, to limit impact artifacts, the actual ROM available for each repetition was below the 10
Knee angle, angular velocity and moment data for each individual repetition were filtered using a 4
DCR60 and DCR120
To calculate the DCR60, the main outcome variable for the study, the PM for the hamstrings for each trial of the eccentric 60
DCRROM60 and DCRROM120
As the DCR above do not account for the knee angle at which the PM values occurred, two additional measures were determined. The DCRROM60 represents the DCR at 60
Normalized moment
The moment data for each repetition, under all conditions, were normalized to the PM for the same repetition of the quadriceps under the concentric 60
Statistical analyses
Independent samples t-tests, along with Levene’s test for equality of variances, were used to compare the mean DCR60 and DCR120 between male and female participants, in order to ensure that no significant sex-related differences were present [17], and that these data could be combined for reliability testing.
Generalizability theory was used to address the reproducibility of DCR60. During the first step, the generalizability study (G-study), the reliability coefficient (
where z-score determines the confidence interval of the MDC, based on a normal distribution curve. In this study, a z-score of 1.96 was used, which represents 95% of the data under the normal curve (i.e. a 95% confidence interval). This means that, if the difference between two measures of the DCR60 matches or exceeds this value, the difference is due to real change rather than variability, 19 times out of 20.
During the second step, the decision study (D-study), the
The G-study and D-study were also repeated excluding the first repetitions from each testing session (i.e. using repetitions 2 through 5), and excluding the first two repetitions (i.e. using repetitions 3 through 5). If these analyses produced an improvement in the
Dynamic control ratio means (SD) with comparison for sex-related differences
Dynamic control ratio means (SD) with comparison for sex-related differences
Subscript 2–5 indicates that the first repetition was removed from the data.
DCR60 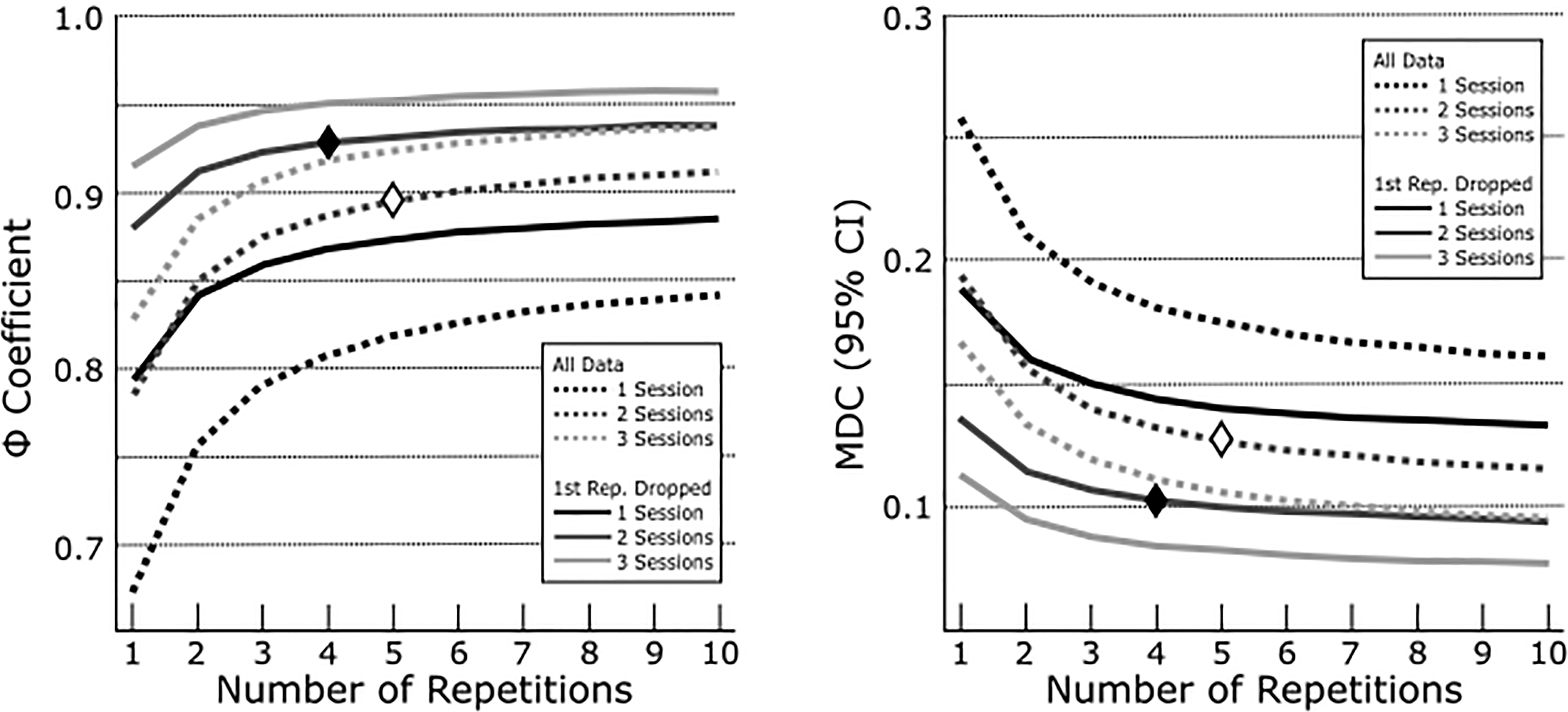
No significant difference were found between male and female participants for DCR60 or DCR120 (Table 2). As such, all further analyzes were done using data from the entire study population (N
DCR60
The mean DCR60 for the experimental data (2 testing sessions, 5 repetitions per session) was 0.421 (SD 0.141). These data produced a
The D-study indicated that using data from only one testing session, excluding the first repetition, the
All data from the D-study, for DCR60, are presented in Fig. 1.
DCR120
The data for DCR120 followed a similar pattern to the DCR60 data, but with slightly larger ratios (higher relative hamstring moment-of-force), slightly lower
The D-study indicated that using data from only one testing session, excluding the first repetition, the
DCRROM60 and DCRROM120
The mean values for DCRROM60 and DCRROM-120 are illustrated in Fig. 2. H
DCRROM60 (black) and DCRROM120 (grey) over the ROM. Values are illustrated for knee joint angles for which data was available for at least 15 subjects.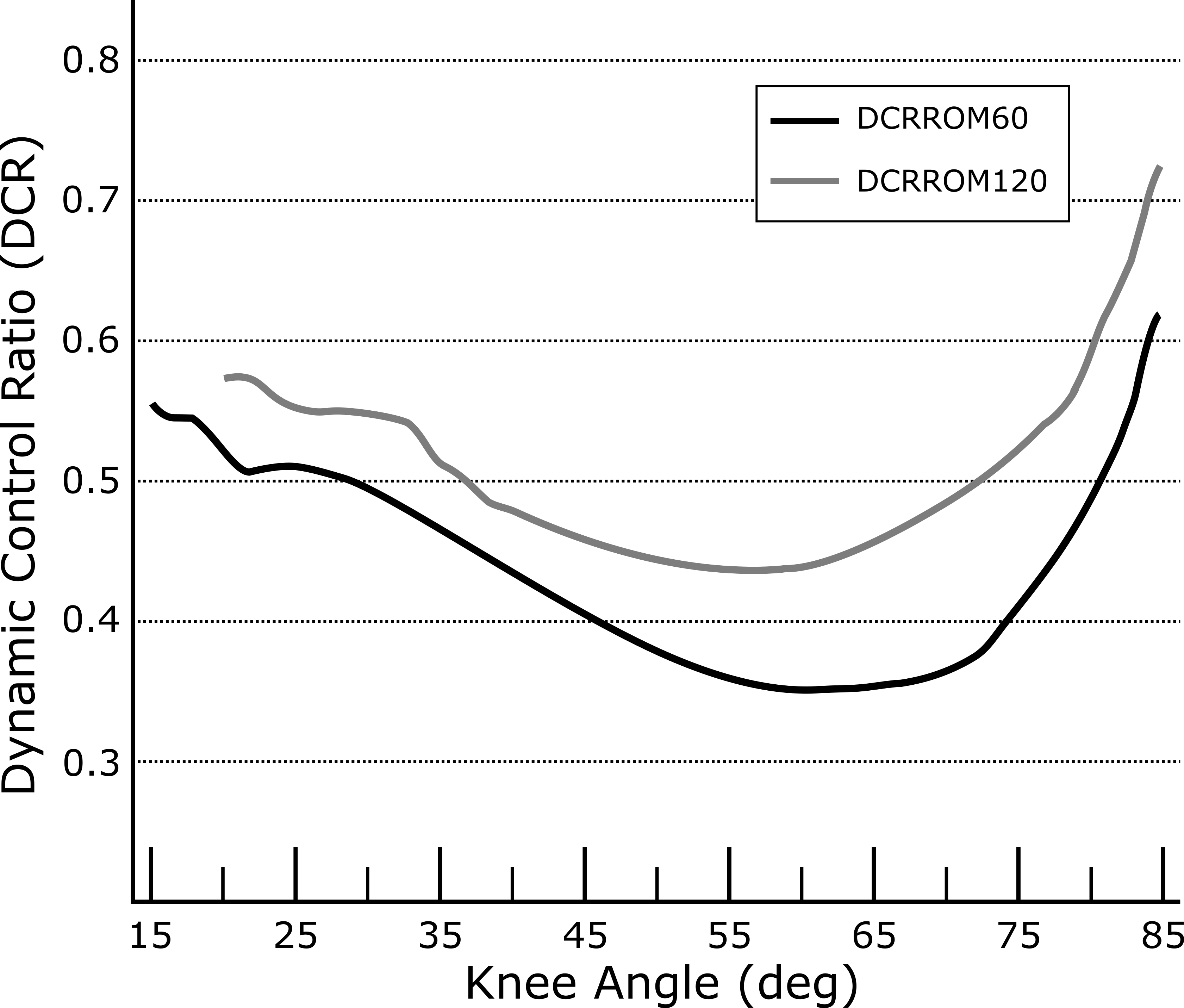
The mean, normalized (to the peak quadriceps moment at 60
Discussion
The primary objective of our study was to develop a clinical assessment protocol for the DCR60 that produces reproducible data, and a realistic MDC. We found that this could be achieved using a single-session protocol, collecting 5 repetitions but excluding the first repetition from the average. The same was found for the DCR120, although with a slightly lower
Mean quadriceps and hamstrings moment-of-force data (from data normalized to the individual subject’s peak quadriceps moment-of-force at Concentric 60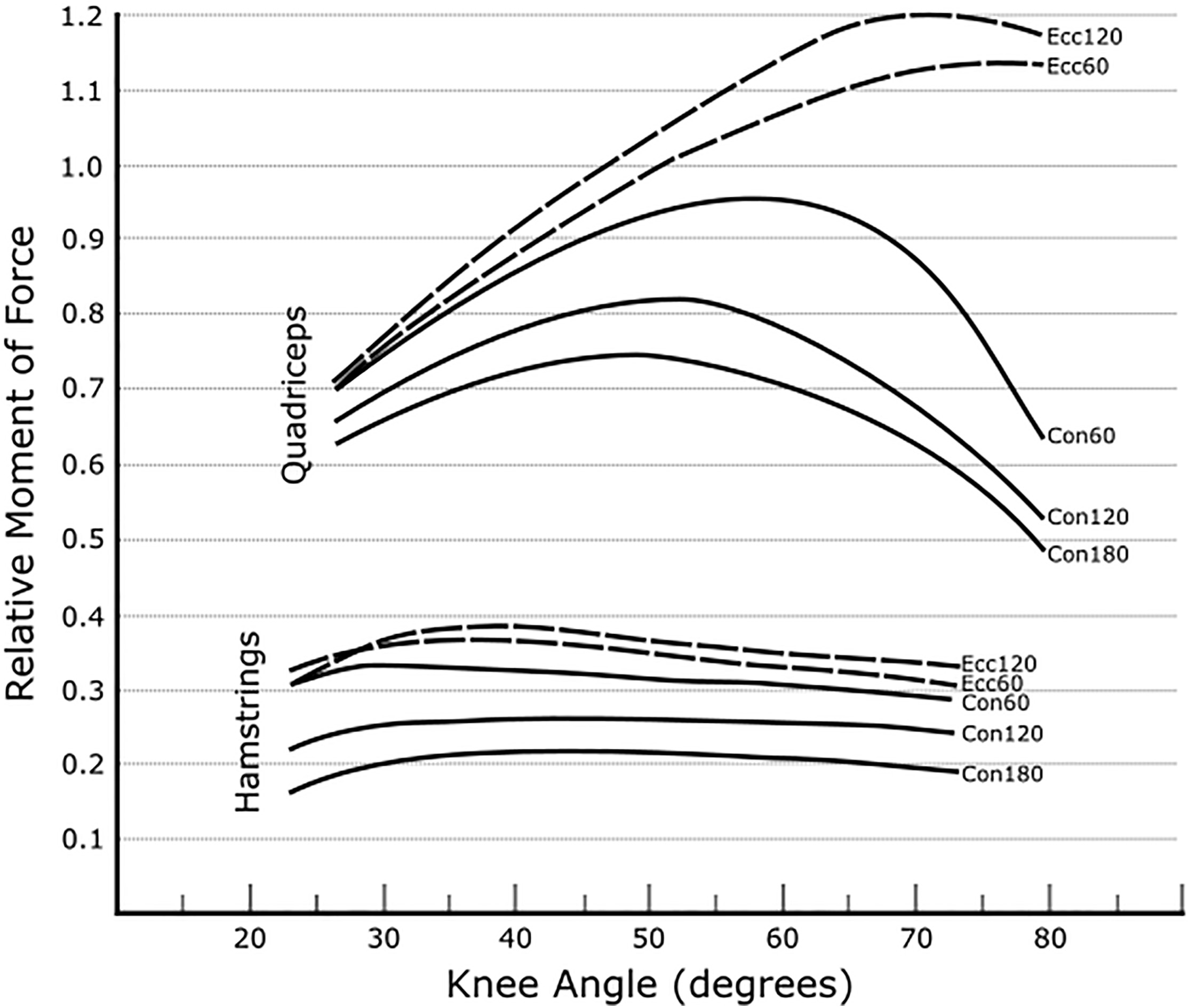
Our findings indicate that isokinetic testing of the hamstrings and quadriceps produces highly reproducible data, which is in line with the findings of previous studies, despite methodological differences. Impellizzeri et al. [4], for example, tested the H/Q ratio in sitting, using data collected over three sessions, and based their analysis on the intra-class correlation coefficient (ICC) model (2,1) [19]. This previous study reported a reproducibility coefficient for the DCR60 of 0.87 for the right leg, and 0.80 for the left, with a MDC of 0.124 and 0.123 respectively. The mean DCR60 reported in this previous study (0.71), however, was quite different from ours (0.421). This may be due to the effect of the test position (sitting vs. prone lying, respectively) on this measure. Changing the hip position may have a similar effect to that of the knee joint angle on the maximum moment produced by the quadriceps (rectus femoris), and to a lesser extent the hamstrings (Fig. 3, discussed below). It may also, however, reflect the fact that 2/3 of the participants in our study were female, who tend to have a lower H/Q ratio than males [17]. This sex-related difference, however, was not significant in the present study (Table 2), nor was the DCR for the male participants as high as previous reports. This effect also cannot be fully considered, as Impellizzeri et al. did not report the sex of their participants.
The effects of joint angular velocity and joint angle on the hamstring and quadriceps moment (Figs 2 and 3) reflect differences in muscle architecture. Lieber and Friden (2001) provide a comprehensive review of the direct relationship between muscle physiological cross-sectional area and force production, and of the effect of muscle fiber length on the rate of force decline at higher velocities (longer muscles show less force decline with increasing velocity of shortening). The greater physiological cross-sectional area of the quadriceps muscles [11, 20], along with the larger moment arm of the quadriceps due to the fulcrum provided by the patella [21, 22], explains the larger moment produced by the quadriceps, relative to the hamstrings, throughout the ROM (Fig. 3). Each of the muscles that comprise the quadriceps muscle group, however, have similar muscle fiber lengths, which are comparable to those of the semimembranosus, but shorter than those of the biceps femoris and semitendinosus [11, 20]. This accounts for the much larger relative drop in moment for the quadriceps at higher velocities, as well as the tendency of the quadriceps to show a more parabolic curve over the knee ROM, with a flatter curve for the hamstrings (Fig. 3). This is also reflected in the DCRROM variables (Fig. 2), as well as in previously reported findings in sitting [13].
It is important for clinicians to keep this effect of muscle architecture in mind when interpreting the DCR. These differences make it unrealistic to expect the DCR60, in particular, to be high (approaching or exceeding 1). The range of DCR60 in our study, based on our recommended single-session assessment protocol, was 0.188 to 0.807. As such, clinicians may only want to target an increase in the DCR if this value is felt to be too low.
As with all studies, the interpretation of our data is subject to certain limitations. When assessing the value of the DCR60 or DCR120 to guide training, it is important to recognize that knee angular velocities during activities such as sprinting may far exceed 120
Our findings indicate that reproducible data for the DCR60 and DCR120 can be acquired in a single testing session with 5 repetitions, excluding the first repetition from the average. While the exact MDC values in our study will likely change for different patient populations, the MDC produced using this protocol were clinically achievable for individuals with a low DCR. It must, however, be kept in mind that joint angular velocity and joint angle both have an impact on the moment at the knee. As such, the DCR alone (based on the PM over the ROM) does not fully capture the functional capacity of these muscles.
Conflict of interest
The authors have no conflicts of interest, financial or otherwise, to report.
Footnotes
Acknowledgments
Funding for the equipment used in this project was received from the Canada Foundation for Innovation.