
Abstract
BACKGROUND:
Different methods of treatment for preventing knee injuries, enhancing knee strength and minimising post-injury risks have been explored. Among these methods, Kinesio tape (KT) and knee braces (KB) are commonly used.
OBJECTIVE
: To investigate the acute effects of KT and KB on isokinetic knee strength parameters.
METHODS:
A total of 15 healthy sedentary male subjects voluntarily participated in the study. Concentric isokinetic knee extension (EX) and flexion (FLX) strength were measured at three sessions: 1. Baseline 2. with KT (’KT’) 3. with KB (’KB’). Tests were performed at 60, 180 and 240
RESULTS:
‘KT’ and ‘KB’ were associated with increase in PM
CONCLUSION:
In healthy individuals, ‘I’ shape KT and KB positively affect EX and FLX strengths and HQR, especially at low angular velocity.
Introduction
Physically active individuals who participate in recreational, amateur, or professional level activities continually look for recourses or new methods to enhance their muscle strength and prevent injuries [1]. Knee injuries are known to account for up to 60% of all sport injuries, while anterior cruciate ligament (ACL) accounts for almost 50% of knee injuries not excluding others such as meniscal injuries and patello-femoral pain [2, 3]. One of the primary causes of knee injury is the knee joint taking a position contrary to its structure during movement because of strength imbalance in the muscles affecting knee strength [4, 5].
Different methods and treatments are being tested by researchers to prevent knee injuries, enhance knee strength and minimise post-injury risks. Among these methods, Kinesio tape (KT) and knee braces (KB) are the widely applied methods [3, 6, 7, 8]. At present, KT is being extensively used by athletes, physiotherapists and researchers because it has been shown to influence inflammation by increasing blood and lymph circulation, thus stimulating movement as a result of intense contraction in the muscle, reducing pain by decreasing the pressure on subcutaneous nociceptors and facilitating movement in joint and muscle functions by muscle alignment and activation [9, 10, 11, 12, 13]. KT is highly elastic (up to 75% of its original length) depending on the contraction and direction of movement of the muscle group to which it is applied [9, 14]. However, KB has been available for the last 40 years and has been used to help individuals with knee injuries, specifically ACL-reconstructed knees [15, 16, 17]. Moreover, studies have been conducted on KB in relation to physical performance and knee injuries, but these studies generally focused on soccer players. These studies examined the effects of KB on the tendency, severity and incidence of knee injury during physical performance, but they did not indicate any positive finding [18, 19]. Teitz et al. [19] reported that the group using KB was more disabiled than the non-users. In addition, researchers who have examined the effect of KB on neuromuscular activities of the knee joint reported that the use of KB reduced such activity, especially in the quadriceps muscles, but did not reduce the strength by providing a mechanical support to the patellofemoral joint [16, 17].
However, there is still no consensus on whether KT and KB have positive effects in terms of performance [6, 13, 15]. In terms of KT, the reason for this may be that although there are different taping methods, subjects are tested by applying only one taping method to different muscles, especially to the quadriceps (Q) and the hamstring (H) while in terms of KB, it may be attributed to the limited number of studies conducted and the different brands and structures of KB [3, 6, 8, 10, 14, 15, 16, 17, 18, 19, 20, 21, 22].
Therefore this study aimed at investigating the acute effects of ‘I’ shape KT on Rectus Femoris (RF) and the application of KB on isokinetic knee strength, the HQR and the angle of peak moment (JAPM).
Methods
Participants
Fifteen healthy sedentary male subjects (mean age
Descriptive parameters of subjects
Descriptive parameters of subjects
Comparison of PM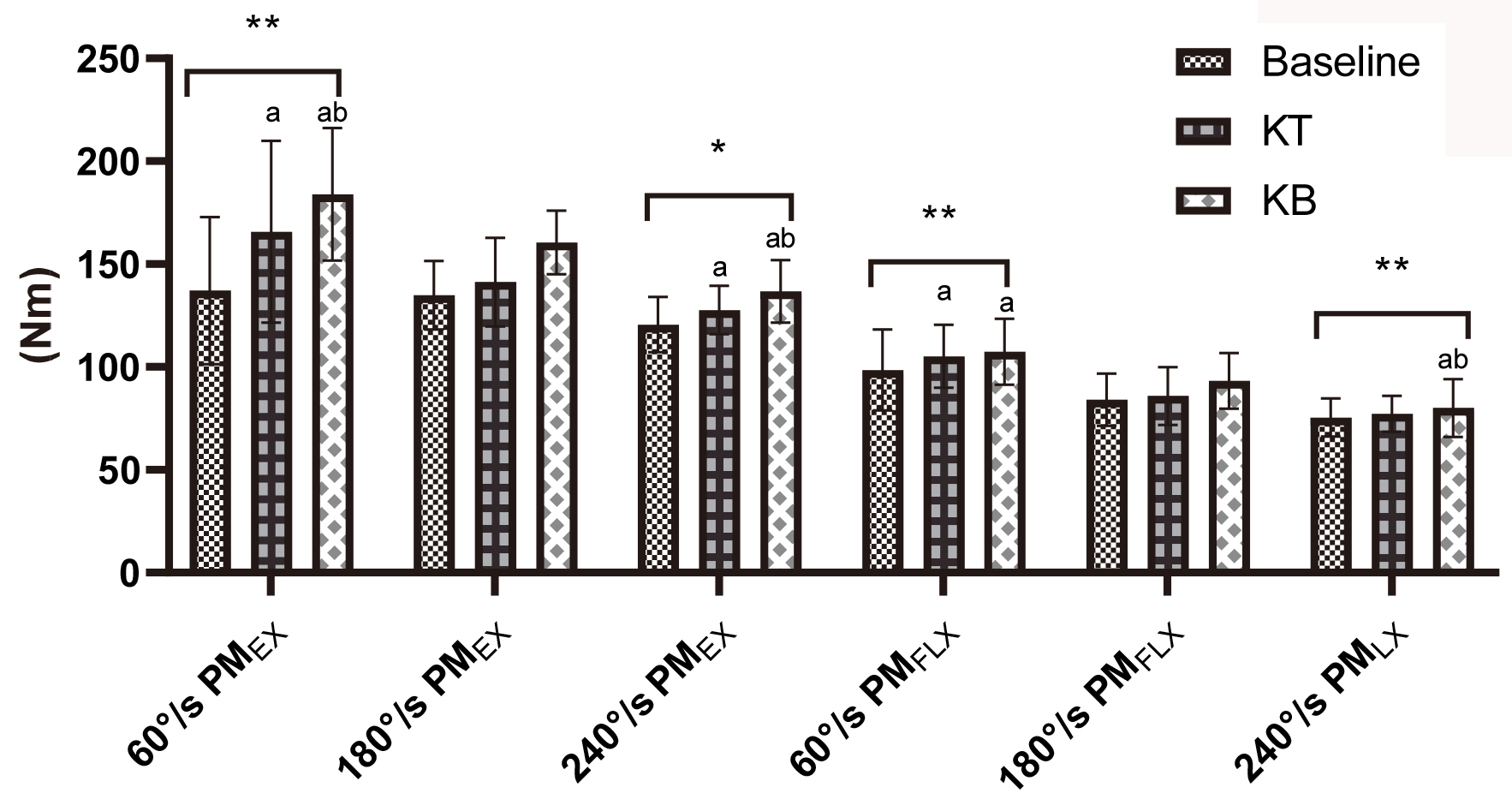
The study was designed as a randomised, double-blind and cross-controlled experiment. The participants visited the laboratory four times comprising one familiarisation session followed by three repeated testing sessions for all subjects. In the first session, the participants were informed about the test protocols and their height, weight and body mass index were measured. After first session, they were randomly assigned to either baseline, ‘KB’ or ‘KT’.
Isokinetic knee strength measurement
A Cybex Humac Norm, USA isokinetic dynamometer was used for testing in the seated position. Dominant limb of the subjects was fixed to an isokinetic seat with belt. Isokinetic tests were performed at three different velocities (60, 180 and 240
Kinesio taping
Kinesio Tex Gold tape, 5-cm wide (Albuquerque, NM, USA), was used in the study and applied with an I-shaped pattern on a clean and dry skin. The KT was applied in a standardised manner (origin to insertion) running from a point 10 cm below the anterior superior iliac spine to superior pole of the patella on RF muscle with 25% tension [9] to ease the RF muscle activation. For consistency of tension the KT was applied by the same investigator to all subjects.
Knee brace
DonJoy Tru-pull Advance System (11-1289/90-X- 06000) was used for this study. This brace features an elastomeric pull device with pull straps above and below the patella. It has a rubber band effect that provides a strong dynamic pull on the patella as the knee extends. The brace was worn on the dominant leg during the test [3].
Data analysis
Data were analysed using the SPSS and expressed as the mean and standard deviation. The Shapiro–Wilk test was used for assessing normality of data. Repeated measures one-way analysis of variance and LSD correction were used for analysing differences between the trials. Partial ETA was used to calculate effect size (ETA) between the trials. According to ETA (
Comparison of HQR values between trials. *significant differences between trials in 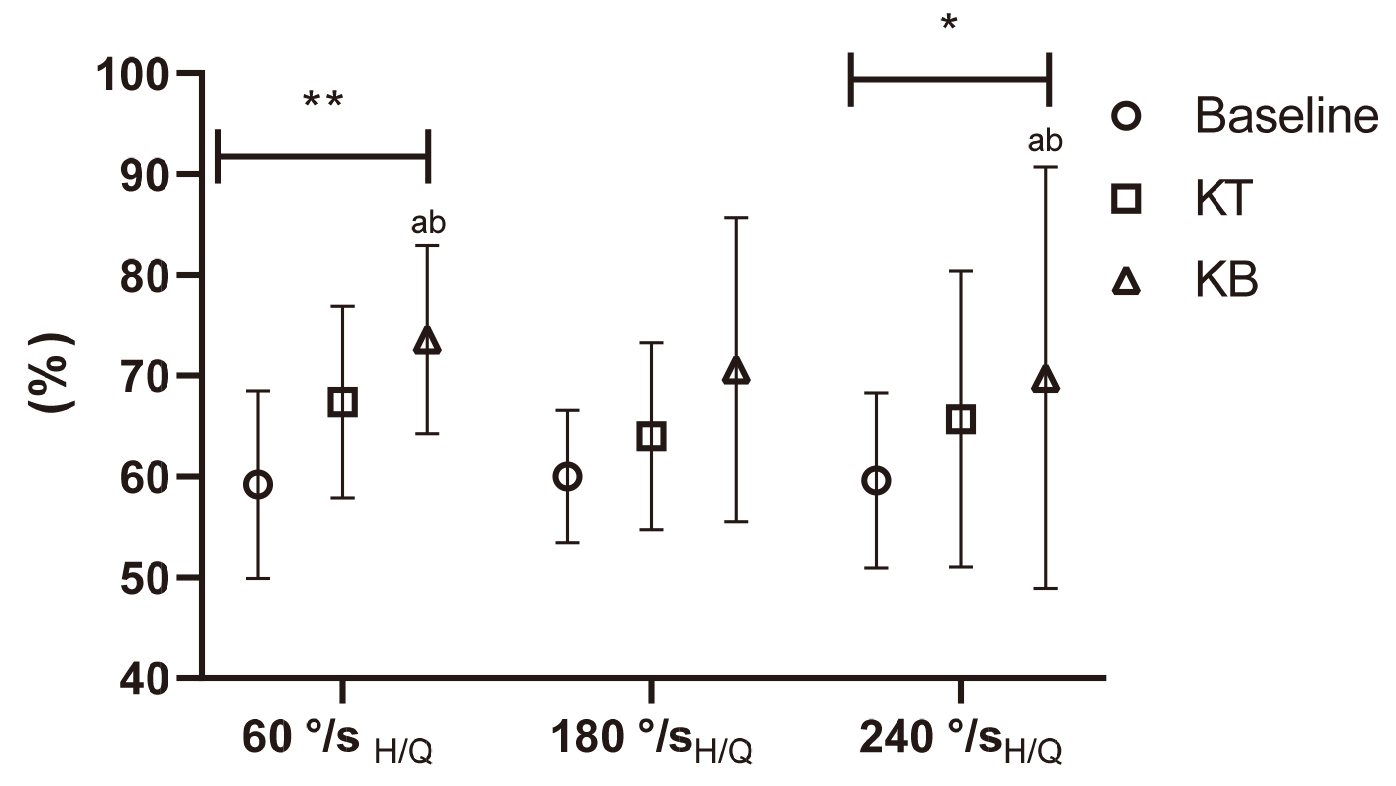
For tests at 60
Comparison of JAPM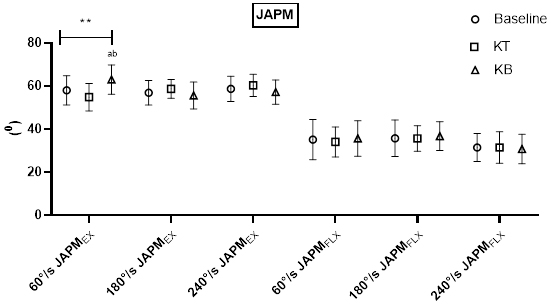
For JAPM
This main finding of this study is that for both 60 and 240
Previous studies reported that KT had no acute effect on muscle strength in different contractions and velocities [1, 8, 22, 23, 24, 25, 26]. Similarly, researchers have reported that KT applied to muscle groups in different joints did not have an acute effect on isokinetic strength [13, 27, 28]. However, others have shown that acute KT application improved isokinetic muscle strength and activation [6, 8, 10, 24]. Researchers have also stated that, in addition to effects of the training (especially in athletes), the increase in PM caused by KT application to the quadriceps could affect neural activation and regeneration of muscle fibres [29, 30]. In summary, there is a diversity of findings relating to the acute strength effects of KT and KB which could be attributed to the differences in training history, injury history and cutaneous afferent applications of subject groups in which KT and KB were applied. It brings to mind the idea that muscle groups, which are already developed especially in athletes, will not be significantly affected compared to the situation in sedentary individuals and individuals with a history of injury.
Studies investigating the effects of KB on isokinetic knee strength are limited. Aktaş and Baltaci [3] reported that KT and KB application increased isokinetic knee strength at 60
In this study, the increase in knee isokinetic strength in both EX and FLX phases of KT measurements is considered to be due to the ‘I’ shape technique, which is specifically aimed at increasing muscle strength in the EX phase. This result can be supported by the following theories of researchers. KT may affect the functions of muscle and myofasia by increasing blood circulation in the region where it is taped [33]. According to Ridding et al. [34], activity in both the central and peripheral nervous system may be augmented by cutaneous afferent applications, increasing motor unit stimuli and motor activation by the intense stimulation of the motor cortex. Moreover, it was suggested that motor units were stimulated more quickly and easily by reducing neuron threshold with cutaneous applications and that the increase in muscle activations increased tension in the muscle applied with KT and the muscle reflex and activation [35, 36]. Unlike the results of this study and other theories, some researchers have reported that cutaneous application of KT could increase motor activations by changing motor neuron stimuli; however, the stimuli were not strong enough to affect strength [8].
As for the asymmetry issue, asymmetric strength for the lower limb can be defined as inability of the right and left Q and H muscles to produce equal amounts of similar contraction types and may thus expose the knee [37, 38]. In this study, KT and KB applications increased HQRs and this increase was significant at 60
Our results support the idea that KT stimulates cutaneous mechanoreceptors in the taped region and that this stimulation may affect the range of motion in the lower extremity [34, 42, 43, 44]. It is suggested that in the higher angular velocities, the application of KT meant reaching the JAPM in lower angles (compared to KB) due to a possible inhibitory effect on the cutaneous mechanoreceptors.
In terms of limitations of this study, the most important is the bilateral application of KT on the RF only. Another limitation concerns the fact that we tested isokinetically in the concentric fashion only, which reveals only part of the full effect on the muscular performance.
Conclusion
In view of the foregoing findings and analysis we suggest that both interventions may be beneficial. Investigating further the effects of different KT taping techniques and different KB types on isokinetic variables and ultimately on the athletic performance is thus warranted.
Author contributions
CONCEPTION: Mustafa Özdal and Mehmet Vural.
PERFORMANCE OF WORK: Mustafa Özdal and Mehmet Vural.
INTERPRETATION OR ANALYSIS OF DATA: Mustafa Özdal and Mehmet Vural.
PREPARATION OF THE MANUSCRIPT: Ali Kerim Yılmaz and Menderes Kabadayı.
REVISION FOR IMPORTANT INTELLECTUAL CONTENT: Ali Kerim Yılmaz and Menderes Kabadayı.
SUPERVISION: Ali Kerim Yılmaz and Mustafa Özdal.
Ethical considerations
The study was approved by the Clinical Research Ethics Committee of Gaziantep University (2019/392).
Funding
The authors report no funding.
Footnotes
Acknowledgments
We would like to thank all of the subjects who volunteered their time to participate in the study.
Conflict of interest
The authors have no conflict of interest to report.